Frenum
4,332 words · 14 min read
Quick Definition
A small fold of tissue that connects the lips, cheeks, or tongue to the jawbone. An abnormally tight or short frenum can restrict movement and may require surgical correction (frenectomy).
Frenum: The Definitive Guide to Understanding This Oral Tissue and Its Impact on Dental Health
The human mouth is a marvel of intricate structures, each playing a vital role in our ability to speak, eat, and maintain overall oral health. Among these often-overlooked components are the frena (plural of frenum), small yet significant folds of connective tissue that can profoundly influence everything from a baby's ability to nurse to an adult's gum health and orthodontic stability. If you've ever heard terms like "tongue-tie" or "lip-tie," you're already familiar with conditions related to the frenum. Understanding what a frenum is, its various types, and when it might require attention is crucial for comprehensive dental care.

A frenum is essentially a small band of fibrous tissue that serves as an anchor, connecting more movable parts of the mouth, such as the lips, cheeks, or tongue, to the less movable jawbone or gingiva (gums). While typically unobtrusive and functional, an abnormally tight, thick, or short frenum can restrict movement, leading to a cascade of dental, speech, and even feeding difficulties. When such restrictions occur, a minor surgical procedure called a frenectomy may be recommended to alleviate the tension and restore proper function. This in-depth guide will explore every facet of the frenum, offering clarity for anyone seeking to understand its impact on oral health.
Key Takeaways:
- What it is: A frenum is a small fold of tissue connecting movable oral structures (lips, tongue) to less movable ones (gums, jaw).
- Types: The most common are the lingual frenum (under the tongue) and labial frenum (under the upper/lower lips).
- Issues: An abnormally tight or short frenum can cause feeding problems in infants, speech impediments, gum recession, and orthodontic issues like gaps between teeth.
- Diagnosis: Dentists diagnose frenum issues through visual examination, palpation, and functional assessment of oral movements.
- Treatment: The primary treatment is a frenectomy, a minor surgical procedure to release the frenum, often performed with a scalpel or laser.
- Impact: Correcting frenum issues can significantly improve feeding, speech, oral hygiene, and overall dental health.
Detailed Explanation
The term "frenum" (from the Latin fraenum, meaning "bridle" or "rein") perfectly describes its function: to tether or restrain. In the mouth, these seemingly minor tissue bands can, when abnormal, exert a significant "bridling" effect on crucial oral functions.
Types and Classifications of Frenum
There are several frena located throughout the mouth, each with a specific name based on its location:
-
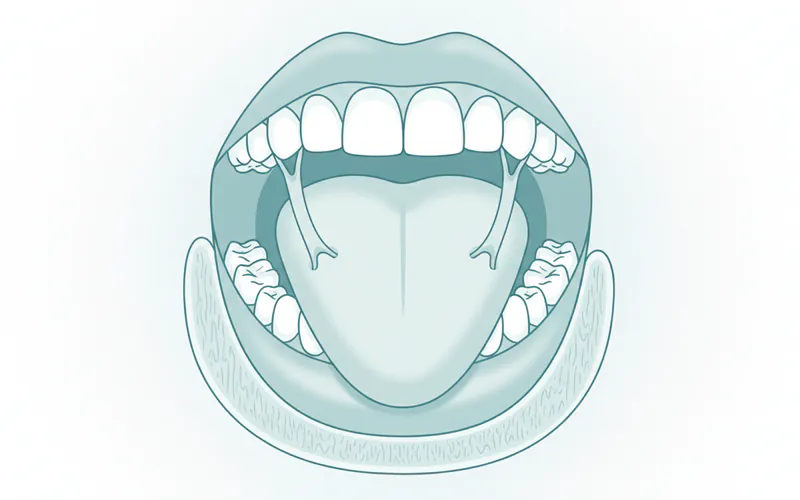
Lingual Frenum:
- Location: This is the band of tissue located under the tongue, connecting the underside of the tongue to the floor of the mouth.
- Significance: When the lingual frenum is unusually short or tight, it restricts the tongue's movement, a condition known as ankyloglossia, more commonly called "tongue-tie." This is perhaps the most well-known frenum-related issue due to its profound impact on infants.
- Classification (for ankyloglossia): Often classified by its attachment point and restriction level. A common system, like the Kotlow Classification, categorizes tongue-ties based on how close the frenum attaches to the tongue tip, ranging from Class 1 (attaching close to the tip) to Class 4 (attaching near the base, considered a posterior tongue-tie, which can be harder to visually identify but equally restrictive).
-
Labial Frenum (Maxillary and Mandibular):
- Location: These are the bands of tissue connecting the inside of the upper lip (maxillary labial frenum) and the lower lip (mandibular labial frenum) to the gingiva above the two front teeth and below the lower front teeth, respectively.
- Significance:
- Maxillary Labial Frenum: An overly thick or low-inserting maxillary labial frenum can create a persistent gap between the two upper front teeth, known as a diastema. This can be an aesthetic concern and may interfere with orthodontic treatment, potentially causing relapse if not addressed. It can also pull on the gum tissue, leading to gingival recession or preventing proper tooth brushing in the area.
- Mandibular Labial Frenum: While less commonly problematic than its upper counterpart, an unusually thick or tight mandibular labial frenum can also contribute to gum recession around the lower front teeth and interfere with the fit of dentures.
- Classification (for labial frenum): Often classified by its attachment point relative to the gingival margin (where the gum meets the tooth) and the width of the attached gingiva.
-
Buccal Frenum:
- Location: These frena are found on the sides of the mouth, connecting the cheeks to the gum tissue, typically near the premolars or molars.
- Significance: Buccal frena are less frequently problematic but can sometimes interfere with denture retention or contribute to discomfort if they are exceptionally tight.
Causes and Risk Factors
The development of an abnormally tight or short frenum is almost universally congenital, meaning it is present at birth. It is primarily considered a developmental anomaly.
- Genetic Predisposition: While specific genes aren't always identified, there appears to be a genetic component, as frenum issues can run in families. If one child has a tongue-tie, there's a higher chance subsequent children may also have one.
- Embryonic Development: During fetal development, the tongue and lips typically separate from the floor of the mouth and the jawbone, respectively, allowing for increased mobility. When this separation process is incomplete or restricted, an abnormally short or thick frenum forms.
- No Known Preventative Measures: As these conditions are developmental, there are no known preventative measures parents can take during pregnancy. The focus is entirely on early identification and appropriate intervention.
Signs and Symptoms to Watch For
The symptoms associated with a problematic frenum can vary significantly depending on the type of frenum involved and the individual's age.
In Infants (primarily Lingual and Maxillary Labial Frenum):
- Difficulty Breastfeeding: This is the most common and often the first recognized symptom of ankyloglossia or a tight labial frenum.
- Poor latch, shallow latch.
- Clicking sounds during feeding.
- Inadequate weight gain for the baby.
- Prolonged feeding times.
- Gumming or chewing the nipple.
- For the mother: Nipple pain, damage, mastitis, low milk supply due to inefficient milk transfer.
- Difficulty Bottle Feeding: Though less common, a restricted tongue can make bottle feeding difficult for some infants, affecting their ability to create proper suction.
- Reflux and Colic Symptoms: Due to swallowing excessive air during inefficient feeding.
- Poor Oral Hygiene: A tight labial frenum can make it challenging to adequately clean under the upper lip, increasing the risk of early childhood caries (cavities) on the front teeth.
- Open Mouth Posture: Sometimes seen with severe tongue-tie, as the tongue cannot rest properly on the roof of the mouth.
In Children and Adults (Lingual and Labial Frenum):
- Speech Impediments:
- Lingual Frenum (Tongue-tie): Difficulty pronouncing sounds requiring tongue elevation or precise articulation, such as "r," "l," "t," "d," "n," "th," and "s" sounds (often manifesting as a lisp).
- Labial Frenum: Less direct impact on speech, but can affect the ability to form certain lip shapes.
- Eating Difficulties:
- Lingual Frenum: Trouble licking an ice cream cone, clearing food from the molars, or moving food efficiently around the mouth.
- Labial Frenum: Difficulty fully opening the mouth for certain foods.
- Dental and Periodontal Issues:
- Maxillary Labial Frenum: Persistent diastema (gap between upper front teeth) that may not close completely with orthodontic treatment or may relapse after braces are removed. Gum recession (gingiva) and inflammation due to the frenum pulling on the gum tissue.
- Mandibular Labial Frenum: Can pull the gum tissue away from the lower front teeth, leading to gum recession and potentially root exposure.
- Discomfort or Pain: The frenum tissue can be stretched or irritated during normal oral functions, leading to discomfort.
- Difficulty with Oral Hygiene: Making it hard to brush effectively in certain areas, particularly under the upper lip if the labial frenum is tight.
- Impact on Denture Wearers: An excessively thick or high frenum can interfere with the proper fit and retention of removable partial or full dentures.
Diagnosis Process — What Your Dentist Does
Diagnosing frenum issues typically involves a comprehensive evaluation by a dental professional, pediatrician, or lactation consultant.
- Clinical Examination: The dentist will visually inspect the frenum, noting its thickness, length, and attachment point. They will also assess the surrounding gingiva and teeth for any signs of recession or spacing issues.
- Palpation: Gently feeling the frenum and the surrounding tissues can help assess its elasticity and identify any unusual fibrous bands.
- Functional Assessment: This is critical. The dentist will observe the patient's oral movements to determine the extent of restriction:
- For Lingual Frenum: Asking the patient (or observing the infant) to lift their tongue to the roof of the mouth, stick it out, and move it from side to side. The ability to touch the roof of the mouth with the tongue while the mouth is wide open is a good indicator of mobility. For infants, assessing the quality of their suck and latch is paramount.
- For Labial Frenum: Gently pulling the lip away from the gums to see how much it restricts movement and if it causes blanching (whitening) of the gum tissue, indicating tension.
- Symptom Review: A detailed discussion of symptoms, including feeding difficulties, speech issues, discomfort, or aesthetic concerns, provides crucial context for diagnosis.
- Referrals: In cases of complex feeding issues, a lactation consultant might be involved. For speech problems, a speech-language pathologist may provide a more detailed assessment and therapy recommendations. Orthodontists are often involved when a labial frenum contributes to a diastema or gum recession.
Treatment Options with Pros, Cons, and Costs
The primary treatment for an problematic frenum is a surgical procedure to release or remove the restrictive tissue. This procedure is generally known as a frenectomy, though variations exist.
-
Frenotomy (for infants):
- Description: Often used for infants with tongue-tie, this is a simpler procedure involving a quick incision to snip the frenum. It's less invasive than a full frenectomy.
- Pros: Quick, minimal discomfort, often performed without anesthesia (or topical anesthetic), immediate improvement in feeding.
- Cons: Only suitable for very thin, superficial frena. May not fully release thicker or more complex ties.
- Cost: Often covered by medical insurance if deemed medically necessary for feeding issues. Out-of-pocket can range from $150 - $500.
-
Frenectomy:
- Description: A more complete removal or revision of the frenum. Can be performed using various techniques:
- Scalpel Frenectomy (Traditional): Surgical blade is used to precisely cut and remove the restrictive tissue. Sutures (stitches) are often used to close the wound.
- Laser Frenectomy: A dental laser (e.g., CO2 laser, diode laser) is used to ablate (vaporize) or cut the frenum.
- Pros of Scalpel: Well-established technique, relatively low cost.
- Cons of Scalpel: May involve more bleeding, requires sutures, longer healing time compared to laser.
- Pros of Laser: Minimal bleeding (laser cauterizes as it cuts), often no sutures needed, reduced post-operative pain and swelling, faster healing, reduced risk of infection, often quicker procedure time.
- Cons of Laser: Higher equipment cost can translate to a slightly higher procedure fee, not all dental offices have laser technology.
- Cost of Frenectomy (Scalpel or Laser) in the US:
- Without insurance: $250 - $1,500 per frenum.
- With insurance: Typically covered partially or fully if deemed medically or dentally necessary (e.g., impacting speech, eating, causing gum recession, or preventing successful orthodontics). Co-pays and deductibles will apply. Laser procedures may sometimes be billed slightly higher or require prior authorization.
- Description: A more complete removal or revision of the frenum. Can be performed using various techniques:
-
Frenuloplasty:
- Description: A more complex revision of the frenum, often involving Z-plasty or W-plasty techniques to reconfigure the tissue and increase mobility. This is usually reserved for very thick, wide, or fibrous frena, or cases where significant scar tissue has formed.
- Pros: Provides maximal release and improved long-term results for severe cases.
- Cons: More invasive, requires sutures, longer recovery, typically performed by an oral surgeon.
- Cost: $1,000 - $3,000+, depending on complexity and location. More likely to require general anesthesia for children.
Step-by-Step: What to Expect During Treatment
The process typically involves several stages:
- Consultation and Diagnosis: Your dentist or oral surgeon will examine the frenum, discuss your symptoms, and explain the recommended procedure.
- Preparation:
- For infants: Often no specific preparation beyond ensuring the baby is fed and comfortable.
- For older children/adults: Local anesthetic (numbing injection) will be administered to ensure you feel no pain during the procedure. For very anxious children or complex cases, sedation (e.g., nitrous oxide, oral sedation, or even general anesthesia) may be discussed.
- The Procedure (Frenectomy/Frenotomy):
- The area is isolated, and the frenum is carefully released.
- Scalpel: A small incision is made to release the frenum. Any bleeding is controlled, and sutures (dissolvable stitches are common) may be placed to help the tissue heal and prevent reattachment.
- Laser: The laser energy precisely cuts and cauterizes the tissue simultaneously, minimizing bleeding and often eliminating the need for sutures. The process is very quick, often lasting only a few minutes.
- Immediate Aftercare: Once the procedure is complete, you'll receive specific instructions for post-operative care.
Recovery Timeline and Aftercare
Recovery from a frenum release procedure is generally straightforward, but adherence to aftercare instructions is vital to prevent complications and ensure optimal healing.
- Pain Management:
- Infants: Often only require comfort nursing/feeding immediately after. Over-the-counter infant acetaminophen may be recommended by your pediatrician.
- Older Children/Adults: Mild discomfort is common for 1-3 days. Over-the-counter pain relievers (e.g., ibuprofen or acetaminophen) are usually sufficient.
- Wound Care:
- Keep the area clean. Gentle rinsing with warm salt water several times a day (for older children/adults) helps keep the site clean and promotes healing.
- Avoid vigorous brushing directly on the wound for a few days.
- Stretching Exercises (Crucial!): This is arguably the most important part of aftercare, especially for lingual frenectomy. Your dentist will provide specific exercises to perform several times a day for several weeks. These exercises aim to prevent the tissue from reattaching and ensure maximum mobility. Without these, the frenum can heal back tightly.
- Diet: Stick to soft, non-acidic foods for the first few days to avoid irritating the healing site.
- Healing Time:
- Frenotomy (infants): Often appears healed within a few days to a week.
- Frenectomy (scalpel or laser): The initial healing of the wound surface usually takes 1-2 weeks. Full tissue maturation and complete resolution of discomfort can take several weeks to a month.
- Follow-up: A follow-up appointment is typically scheduled within 1-2 weeks to ensure proper healing and address any concerns.
- Potential Complications: While rare, potential complications include infection (though minimized with laser), excessive bleeding, pain, or scar tissue formation leading to reattachment (preventable with stretching).
Prevention Strategies
As frenum issues are congenital, there are no specific prevention strategies to avoid their occurrence. The focus, therefore, shifts to early detection and intervention. Regular dental check-ups from infancy are crucial. For new parents, being aware of feeding difficulties and consulting with pediatricians or lactation consultants early can lead to a timely diagnosis and treatment.
Cost Ranges in the US (with/without insurance)
The cost of frenum release procedures in the United States can vary based on the type of procedure, the dentist's or specialist's fees, geographic location, and whether a laser or scalpel is used.
| Procedure Type | Without Insurance (Estimate) | With Insurance (Estimate) | Notes |
|---|---|---|---|
| Frenotomy (Infant) | $150 - $500 | Often covered under medical insurance if documented feeding issues; co-pay/deductible applies. | Simpler, quicker procedure; sometimes performed by pediatricians, ENTs, or specialized dentists. |
| Scalpel Frenectomy | $250 - $1,000 | Varies widely based on dental vs. medical policy; typically 50-80% coverage after deductible. | Traditional surgical approach, may include costs for sutures and follow-up. |
| Laser Frenectomy | $400 - $1,500 | Similar to scalpel, but some insurers may require prior authorization for laser, or consider it "elective" depending on the reason. | May have slightly higher upfront cost due to technology, but often less discomfort and faster healing. |
| Frenuloplasty | $1,000 - $3,000+ | More likely to be covered by medical insurance if deemed reconstructive or necessary for function. | More complex, often performed by oral surgeons; may include anesthesia fees. |
Insurance Considerations:
- Medical vs. Dental: For infants, a frenotomy due to feeding difficulties is often considered a medical procedure and may be covered by your medical insurance. For older children and adults, frenectomies performed for dental reasons (e.g., gum recession, facilitating orthodontics, speech) might fall under dental insurance.
- Documentation is Key: Thorough documentation from your dentist, pediatrician, or lactation consultant explaining the medical or dental necessity of the procedure is crucial for insurance reimbursement.
- CPT Codes: Procedures are billed using specific CPT (Current Procedural Terminology) codes. Your provider can help clarify which codes will be used for pre-authorization.
- Out-of-Network: Costs can be significantly higher if you see an out-of-network provider.
Treatment Options Comparison Table
| Feature | Frenotomy (Infant) | Scalpel Frenectomy | Laser Frenectomy | Frenuloplasty |
|---|---|---|---|---|
| Primary Use | Thin, superficial lingual ties in infants | General lingual or labial frenum release | General lingual or labial frenum release | Complex, thick, or fibrous frena; scar tissue revision |
| Invasiveness | Least invasive (simple snip) | Moderately invasive (cutting) | Minimally invasive (vaporization/cutting) | Most invasive (reconstructive surgery) |
| Anesthesia | Topical or none (infants) | Local anesthetic | Local anesthetic (sometimes topical only for infants) | Local anesthetic, possibly sedation or general anesthesia |
| Bleeding | Minimal | Moderate | Minimal (laser cauterizes) | Moderate |
| Sutures | Rarely needed | Often needed | Rarely needed | Always needed |
| Procedure Time | Very quick (minutes) | 10-20 minutes | 5-15 minutes | 30-60+ minutes |
| Post-op Pain | Minimal | Mild to moderate | Minimal to mild | Moderate to significant |
| Healing Time | Days to 1 week | 1-2 weeks (initial); several weeks (full) | 3-7 days (initial); 1-2 weeks (full) | Several weeks to months |
| Risk of Reattachment | Low with proper aftercare | Moderate without diligent stretching | Lowest with diligent stretching | Low with diligent stretching and careful surgical technique |
| Cost Range (US) | $150 - $500 | $250 - $1,000 | $400 - $1,500 | $1,000 - $3,000+ |
For Parents / Pediatric Considerations
For parents, understanding the impact of frenum issues on infants and young children is paramount.

- Infant Feeding: A tight lingual frenum (tongue-tie) or maxillary labial frenum (lip-tie) can be a significant barrier to successful breastfeeding. It's not just about the baby's ability to latch, but also the mother's comfort and milk supply. If a baby isn't gaining weight adequately or the mother experiences persistent pain, a frenum assessment should be a priority.
- Early Intervention: Addressing frenum issues early in life can prevent a cascade of problems. Correcting a tongue-tie in infancy can drastically improve feeding, potentially reducing issues like reflux, colic, and even improving sleep.
- Speech Development: While not all speech impediments are due to a tongue-tie, a severe restriction can certainly contribute. If your child struggles with specific sounds or their speech clarity is consistently behind peers, a dental evaluation, in conjunction with a speech-language pathologist, is advisable.
- Oral Hygiene: A tight labial frenum can make it very difficult for parents to lift a baby's lip to clean the front teeth, increasing the risk of early childhood caries. Correcting this can significantly improve a child's ability to maintain good oral hygiene.
- Holistic Approach: Many parents find success by collaborating with a team of professionals, including pediatricians, dentists, oral surgeons, lactation consultants, and speech therapists, to ensure comprehensive care for their child.
Frequently Asked Questions
How much does a frenectomy cost?
The cost of a frenectomy in the US typically ranges from $250 to $1,500, depending on whether a scalpel or laser is used, the complexity of the frenum, the location of the practice, and the practitioner's fees. A simple frenotomy for an infant might be on the lower end ($150-$500), while a laser frenectomy for an adult could be higher. Most dental and medical insurance plans offer partial or full coverage if the procedure is deemed medically or dentally necessary, but co-pays and deductibles will apply. It's crucial to get a detailed estimate from your provider and check with your insurance company beforehand.

Is a frenectomy painful?
During the procedure, local anesthetic is used, so you should not feel any pain. For infants, a topical numbing gel or no anesthetic might be used for quick frenotomies. After the procedure, mild discomfort, soreness, or a burning sensation (especially with laser) is common for a few days. This can usually be managed effectively with over-the-counter pain relievers like ibuprofen or acetaminophen. Infants typically recover quickly and may only require comfort feeding.
How long does a frenectomy take?
The actual frenectomy procedure is very quick, often lasting only 5 to 20 minutes, depending on the technique (scalpel vs. laser) and the complexity of the frenum. The overall appointment, including consultation, anesthesia, and post-operative instructions, will naturally be longer, perhaps 30 minutes to an hour. Recovery involves diligent aftercare, including stretching exercises, for several weeks.
Are there alternatives to frenectomy?
For some very mild cases, especially if symptoms are not severe, a "watch and wait" approach might be considered, particularly for older children where the frenum might naturally stretch or where minor speech issues can be managed with speech therapy alone. However, for significant feeding difficulties, speech impediments, gum recession, or orthodontic concerns, a frenectomy is generally considered the most effective and often the only definitive solution to fully release the restriction. Speech therapy can be a valuable adjunct post-frenectomy to help retrain muscles and consolidate new movement patterns.
Does insurance cover frenectomy?
Yes, many insurance plans cover frenectomy, but coverage can vary significantly between medical and dental policies and based on the reason for the procedure. For infants, if the procedure is performed due to medically documented feeding difficulties (e.g., poor weight gain, maternal pain), it is often covered under medical insurance. For older individuals, if it's for issues like speech, gum recession, or to facilitate orthodontics, it may fall under dental insurance. Pre-authorization from your insurance company is highly recommended to understand your specific benefits and potential out-of-pocket costs.
What's the difference between a frenotomy and a frenectomy?
A frenotomy is a simpler, less invasive procedure, essentially a quick "snip" of a thin frenum, often performed on infants for tongue-tie. It primarily involves cutting the restricting tissue. A frenectomy, on the other hand, is a more involved surgical procedure that involves the more complete removal or revision of the frenum, often including surrounding tissues. It may involve sutures and is typically used for thicker, more fibrous frena in older children or adults. While the terms are sometimes used interchangeably, frenectomy generally implies a more definitive and extensive release.
Will my child's speech improve after a frenectomy?
For children whose speech impediments are directly caused by a restricted lingual frenum (tongue-tie), a frenectomy can significantly improve their ability to articulate certain sounds. However, the improvement is not always immediate or automatic. Many children benefit from post-operative speech therapy to retrain their tongue muscles and learn new patterns of articulation, as they may have compensated for the restriction for years. The earlier the intervention, often the more rapid and complete the speech improvement.
What are the risks of a frenectomy?
Frenectomy is considered a safe, minor surgical procedure with a low risk of complications. Potential risks include:
- Bleeding: Usually minimal, especially with laser, but can occur.
- Infection: Rare, as the mouth heals well, but possible.
- Pain or Swelling: Typically mild and managed with over-the-counter medication.
- Scarring: Minimal, but can occur.
- Reattachment: The most significant risk, especially if post-operative stretching exercises are not diligently followed. The tissue can heal back to a restrictive state.
- Nerve damage: Extremely rare due to the superficial nature of the procedure, but a theoretical risk.
``
When to See a Dentist
It's important to consult with a dental professional if you suspect a frenum issue, regardless of age.
See a dentist or pediatrician for infants if:
- Your baby has persistent difficulty latching or feeding, resulting in poor weight gain.
- You experience significant nipple pain or damage during breastfeeding.
- Your baby makes clicking sounds while feeding.
- Your baby shows signs of reflux or colic that might be related to feeding difficulties.
- You notice difficulty cleaning under your baby's upper lip.
See a dentist for children and adults if:
- You or your child have persistent speech difficulties, especially with sounds requiring tongue elevation.
- You notice a significant gap between the upper front teeth (diastema) that may be caused by a thick maxillary labial frenum.
- There are signs of gum recession (gingiva) around the front teeth.
- You experience discomfort or restricted movement of your tongue or lips.
- Orthodontic treatment is being considered or has been completed, and a frenum is impacting tooth movement or stability.
- Denture retention is an issue due to an interfering frenum.
A consultation with a knowledgeable dentist or oral surgeon can help accurately diagnose the issue and recommend the most appropriate course of action, ensuring optimal oral health and function.
``
``
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.