Orthodontics
5,235 words · 17 min read
Quick Definition
The dental specialty focused on diagnosing, preventing, and treating misaligned teeth and jaws (malocclusion) using braces, clear aligners, and other appliances.
Term: Orthodontics Short Definition: The dental specialty focused on diagnosing, preventing, and treating misaligned teeth and jaws (malocclusion) using braces, clear aligners, and other appliances. Related Terms: Braces, Invisalign, Malocclusion, Retainer SEO Keywords: orthodontics, orthodontics dental, what is orthodontics
What is Orthodontics? Your Definitive Guide to a Healthier Smile
Orthodontics is a specialized branch of dentistry dedicated to correcting teeth and jaws that are positioned improperly. More than just cosmetic enhancements, orthodontic treatment aims to improve oral health, restore proper function, and enhance facial aesthetics. When teeth are misaligned or jaws don't meet correctly, it can lead to a host of problems, from difficulty chewing and speaking to excessive wear on tooth enamel and increased risk of cavities and gum disease.
The field of orthodontics is surprisingly common. According to the American Association of Orthodontists (AAO), over 5 million people in the U.S. and Canada are receiving care from AAO orthodontists, and nearly 2 million of those are adults. This highlights that while many people associate orthodontics with teenagers, it’s a vital treatment option for individuals of all ages seeking to optimize their dental health and achieve a confident, functional smile. Understanding "what is orthodontics" is the first step toward appreciating its profound impact on overall well-being.
Key Takeaways:
- Orthodontics is a dental specialty focused on correcting misaligned teeth and jaws.
- Treatment extends beyond aesthetics, addressing critical functional and health issues like chewing, speaking, and preventing tooth wear.
- Malocclusion, or a "bad bite," is the primary condition treated by orthodontists.
- Common treatment options include braces (metal, ceramic, lingual) and clear aligners like Invisalign.
- Orthodontic care is for both children and adults, with increasing numbers of adults seeking treatment.
- Retainers are essential after treatment to maintain results long-term.
Detailed Explanation
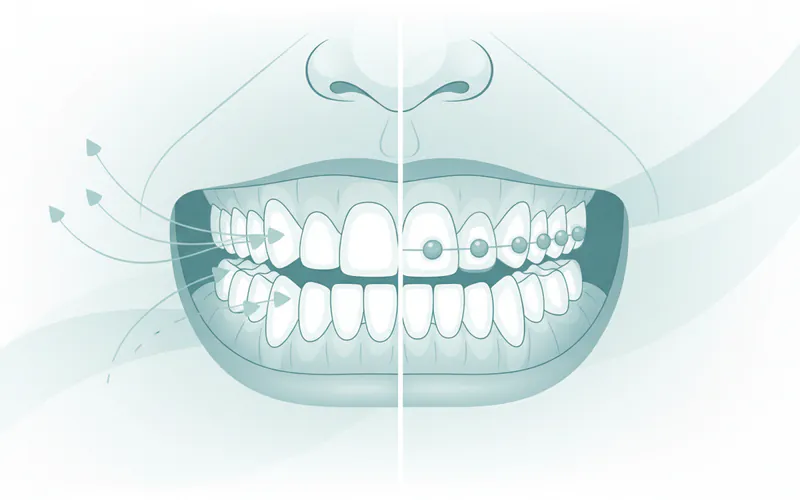
Types and Classifications of Malocclusion
Malocclusion is the technical term for misaligned teeth or an improper bite. Orthodontists classify malocclusion into several types, each requiring a specific approach to treatment.
I. Angle's Classification of Malocclusion:
- Class I Malocclusion: This is the most common type. The bite is generally correct, meaning the upper first molar's mesiobuccal cusp aligns with the lower first molar's buccal groove. However, there may be crowding, spacing, or other localized issues with the teeth.
- Class II Malocclusion (Overbite/Overjet): Occurs when the upper jaw and teeth protrude excessively forward relative to the lower jaw and teeth. This can manifest as:
- Overjet: When the upper front teeth stick out significantly past the lower front teeth horizontally.
- Deep Bite (or Overbite): When the upper front teeth significantly overlap the lower front teeth vertically, sometimes completely covering them.
- Class III Malocclusion (Underbite): Characterized by the lower jaw and teeth protruding excessively forward relative to the upper jaw and teeth. This can give the appearance of a prominent chin.
II. Specific Types of Malocclusion:
- Crowding: When there isn't enough space in the jaw for all teeth to erupt properly, causing them to overlap, rotate, or push against each other. This is one of the most frequent reasons people seek orthodontic treatment.
- Spacing (Diastema): Gaps between teeth, often due to missing teeth, small teeth, or a large jaw. A common type is a gap between the two upper front teeth.
- Crossbite: Occurs when one or more upper teeth bite on the inside of the lower teeth. This can affect a single tooth, a group of teeth, or even the entire arch. It can lead to asymmetrical jaw growth if not treated.
- Open Bite: When the upper and lower front teeth do not overlap at all, leaving a gap between them even when the mouth is closed. This can make biting into certain foods difficult. An open bite can also occur in the back teeth.
- Protrusion: Upper front teeth that stick out, often associated with a Class II malocclusion.
- Impacted Teeth: Teeth that are unable to erupt through the gum line into their proper position, often due to obstruction from other teeth or bone. Wisdom teeth are frequently impacted, but canines are also commonly affected.
Causes and Risk Factors
Malocclusion is often a complex issue with multiple contributing factors. Understanding these can help in both prevention and treatment planning.
I. Genetic and Hereditary Factors:
- Jaw Size and Shape: The size and shape of the jaws, and thus the amount of space available for teeth, are largely inherited. A mismatch between jaw size and tooth size (e.g., large teeth in a small jaw leading to crowding, or small teeth in a large jaw leading to spacing) is common.
- Tooth Size and Number: Genetically, some individuals may have larger or smaller teeth, or even congenitally missing teeth (hypodontia) or extra teeth (supernumerary teeth).
- Facial and Craniofacial Development: Genetic predispositions can influence the overall growth pattern of the face and skull, impacting how the upper and lower jaws relate to each other.
II. Oral Habits:
- Thumb Sucking and Pacifier Use: Prolonged and intense thumb or pacifier sucking past the age of 3-4 years can significantly influence jaw development and tooth position. It can lead to open bites, flared upper front teeth, and constricted upper jaws.
- Tongue Thrusting: An abnormal swallowing pattern where the tongue pushes forward against the front teeth. This can contribute to an open bite.
- Mouth Breathing: Chronic mouth breathing, often due to allergies or enlarged tonsils/adenoids, can alter facial development, leading to a long, narrow face and a constricted upper arch.
III. Early or Late Loss of Primary (Baby) Teeth:
- Premature Loss: If a baby tooth is lost too early due to decay or injury, the surrounding teeth may drift into the vacant space, preventing the permanent tooth from erupting properly. This often necessitates space maintainers.
- Delayed Loss: If baby teeth are retained for too long, they can block the eruption path of the permanent teeth, forcing them to erupt in abnormal positions or become impacted.
IV. Trauma and Injury:
- Dental Trauma: Injuries to the face or mouth can shift teeth, damage developing permanent teeth, or even fracture the jaw, leading to misalignment.
- Jaw Fractures: Improper healing of a jaw fracture can result in a permanent change in the bite.
V. Medical Conditions and Diseases:
- Cleft Lip and Palate: These birth defects significantly impact oral and facial structures, requiring extensive orthodontic and surgical intervention.
- Tumors or Cysts: Growths in the jaws can displace teeth and bone.
- Certain Genetic Syndromes: Conditions like Down syndrome can be associated with specific types of malocclusion.
VI. Poor Dental Hygiene: While not a direct cause of malocclusion, untreated cavities can lead to premature tooth loss, which in turn can cause drifting and misalignment.
Signs and Symptoms to Watch For
Recognizing the signs of malocclusion or other orthodontic issues is crucial for timely intervention. Pay attention to these indicators:
- Visibly Crooked or Crowded Teeth: This is often the most obvious sign and a common reason for seeking orthodontic care.
- Gaps or Spaces Between Teeth (Diastema): Visible spaces that bother you aesthetically or functionally.
- Difficulty Chewing or Biting: If you find it hard to properly chew food, or if your teeth don't meet comfortably.
- Speech Difficulties: Lisping or other speech impediments can sometimes be linked to tooth position or jaw alignment.
- Jaw Pain, Clicking, or Popping: Symptoms of temporomandibular joint (TMJ) disorders, which can be exacerbated by an improper bite.
- Frequent Biting of the Cheek or Tongue: A sign that teeth are misaligned and causing trauma to soft tissues.
- Abnormal Wear of Tooth Enamel: When teeth meet improperly, certain teeth can experience excessive force and wear down prematurely.
- Facial Imbalance or Asymmetry: An underbite or overbite can sometimes be visible in the profile or overall facial appearance.
- Mouth Breathing: If a child consistently breathes through their mouth, especially during sleep, it can impact jaw development.
- Early or Late Loss of Baby Teeth: As mentioned, this can indicate underlying issues for permanent tooth eruption.
- Protruding Teeth: Upper front teeth that stick out, making them vulnerable to injury.
- Grinding or Clenching Teeth (Bruxism): While often stress-related, it can worsen or be worsened by malocclusion.
If you or your child exhibit any of these signs, an orthodontic evaluation is recommended.
Diagnosis Process — What Your Dentist Does
A thorough diagnosis is the cornerstone of effective orthodontic treatment. It involves a detailed examination and a series of diagnostic records.

- Initial Consultation: Your general dentist or an orthodontist will discuss your concerns, medical and dental history, and any symptoms you’re experiencing.
- Clinical Examination: The orthodontist will perform a comprehensive oral exam, evaluating your teeth, gums, jaw joints (TMJ), and overall facial structure. They will check:
- The alignment of your teeth.
- How your upper and lower teeth meet (occlusion).
- The symmetry of your face and jaws.
- Signs of tooth wear, decay, or gum disease.
- Habits like tongue thrusting or mouth breathing.
- Diagnostic Records: To get a complete picture, the orthodontist will typically take:
- Dental X-rays:
- Panoramic X-ray: Provides a broad view of all teeth (erupted and unerupted), jaws, and surrounding structures. It can reveal missing teeth, impacted teeth, or abnormal bone growth.
- Cephalometric X-ray: A lateral (side view) X-ray of the head that shows the relationship between the jaws, teeth, and soft tissues in the profile. This is crucial for planning treatment, especially for jaw discrepancies.
- Periapical and Bitewing X-rays: May be taken to check for specific tooth health issues or bone levels around individual teeth.
- Digital Scans or Impressions:
- Intraoral Scanners: Many modern practices use 3D digital scanners (e.g., iTero, Trios) to create highly accurate digital models of your teeth and bite. These replace messy traditional impressions and allow for precise treatment planning and tracking.
- PVS Impressions: If digital scans are not available, traditional silicone-based impressions are taken to create plaster models of your teeth.
- Photographs: Extraoral (face and profile) and intraoral (inside the mouth) photographs help document the initial condition, track progress, and evaluate facial aesthetics.
- Dental X-rays:
Once all diagnostic information is gathered, the orthodontist will analyze the data to formulate a precise diagnosis and develop a personalized treatment plan, explaining the recommended approach, duration, and expected outcomes.
Treatment Options with Pros, Cons, and Costs
Orthodontic treatment has evolved significantly, offering various options to suit different needs, lifestyles, and budgets.
1. Braces
Braces are the traditional and highly effective method for correcting malocclusion. They consist of brackets bonded to the teeth, connected by an archwire that exerts continuous, gentle pressure to move teeth into desired positions.
- Types of Braces:
- Traditional Metal Braces:
- Pros: Most durable, cost-effective, highly effective for complex cases, can use colored elastics for personalization.
- Cons: Most noticeable, can cause some initial irritation.
- Cost: $3,000 - $7,500
- Ceramic Braces:
- Pros: Less noticeable than metal braces due to translucent or tooth-colored brackets, strong and effective.
- Cons: Can stain (especially clear elastics), slightly more fragile than metal, often more expensive, may cause more friction, potentially extending treatment time slightly.
- Cost: $3,500 - $8,000
- Lingual Braces:
- Pros: Completely invisible as they are custom-made and bonded to the back (tongue side) of the teeth.
- Cons: Most expensive, can be initially uncomfortable for the tongue, may affect speech temporarily, more challenging to clean, fewer orthodontists offer them.
- Cost: $8,000 - $12,000+
- Self-Ligating Braces (e.g., Damon System):
- Pros: Use a specialized clip instead of elastic ties to hold the archwire, potentially reducing friction, fewer adjustment appointments, may be more comfortable. Available in metal or clear options.
- Cons: Can be slightly more expensive than traditional metal braces.
- Cost: $4,000 - $8,500
- Traditional Metal Braces:
2. Clear Aligners (e.g., Invisalign)
Invisalign is the most well-known brand of clear aligner systems, which use a series of custom-made, removable, transparent trays to gradually shift teeth.
- Pros: Nearly invisible, removable for eating and oral hygiene (brushing/flossing), generally more comfortable than braces, fewer emergency appointments.
- Cons: Requires strict adherence to wearing them 20-22 hours per day, can be lost, not suitable for all complex cases (though capabilities are expanding), typically more expensive than traditional metal braces.
- Cost: $3,500 - $8,500
3. Other Orthodontic Appliances
- Palatal Expanders: Widen the upper jaw to correct crossbites or create space for crowded teeth. Often used in children.
- Headgear: Used primarily for children and adolescents to influence jaw growth and tooth movement, usually worn several hours a day and overnight.
- Elastics (Rubber Bands): Used with braces or aligners to correct bite relationships (e.g., Class II or Class III malocclusions).
- Space Maintainers: Custom-made devices to hold space open for a permanent tooth when a baby tooth is lost prematurely.
- Temporary Anchorage Devices (TADs): Small, temporary screws placed in the bone to provide a stable anchor for more efficient tooth movement.
- Retainers: Crucial for maintaining treatment results after braces or aligners are removed. (Detailed in "Recovery timeline and aftercare").
4. Surgical Orthodontics (Orthognathic Surgery)
For severe skeletal discrepancies where the jaws are significantly misaligned and cannot be corrected by orthodontics alone, orthognathic surgery (jaw surgery) may be necessary. This involves repositioning the upper jaw, lower jaw, or both. Orthodontic treatment is always performed in conjunction with surgery, both before and after, to align the teeth properly within the newly positioned jaws.
- Pros: Can correct severe functional problems, dramatically improve facial balance and aesthetics.
- Cons: Major surgery with associated risks, longer recovery period, higher overall cost due to surgical fees.
- Cost: $20,000 - $40,000+ (includes orthodontic treatment and surgical fees).
Step-by-Step: What to Expect During Treatment
Orthodontic treatment is a journey, typically spanning several months to a few years. Here’s a general overview of what to expect:
- Initial Consultation and Diagnosis: (As described above) This phase involves examinations, X-rays, and scans to determine the best course of action.
- Treatment Planning: The orthodontist reviews your diagnostic records and presents a personalized treatment plan, explaining the chosen appliance (e.g., braces or Invisalign), estimated duration, cost, and what results to expect.
- Appliance Placement (Bonding/Fitting):
- For Braces: The teeth are thoroughly cleaned and prepared. Brackets are then precisely bonded to each tooth, and an archwire is threaded through them, secured by tiny elastic bands (ligatures) or self-ligating clips. This usually takes 1-2 hours. You'll receive instructions on oral hygiene and what to expect regarding initial discomfort.
- For Invisalign: Once your custom aligners arrive, you'll receive your first few sets. The orthodontist will explain how to insert and remove them, emphasizing the importance of wearing them 20-22 hours a day and changing them every 1-2 weeks (as directed). Small, tooth-colored "attachments" may be bonded to some teeth to help the aligners grip and move them more effectively.
- ``
- Adjustment Appointments:
- For Braces: You'll typically visit the orthodontist every 4-8 weeks for adjustments. During these appointments, the archwires may be tightened, changed to a different size/material, or ligatures replaced. This keeps the teeth moving progressively.
- For Invisalign: You'll have check-up appointments every 6-10 weeks to ensure treatment is progressing as planned, address any issues, and receive new sets of aligners.
- Managing Discomfort: It’s normal to experience some soreness or mild discomfort for a few days after initial placement and after each adjustment. Over-the-counter pain relievers (like ibuprofen or acetaminophen), soft foods, and orthodontic wax (for braces) can help.
- Oral Hygiene: Meticulous oral hygiene is paramount throughout treatment. Braces can trap food, increasing the risk of cavities and gum inflammation. You'll learn special brushing and flossing techniques (e.g., using interdental brushes, floss threaders for braces, or removing aligners for thorough cleaning).
- Dietary Restrictions:
- With Braces: You'll need to avoid hard, sticky, or chewy foods (e.g., popcorn, nuts, hard candy, gum) that can damage brackets or wires.
- With Invisalign: You can eat anything you like, as aligners are removed for meals. However, you must brush your teeth before putting aligners back in to prevent staining and trapping food particles.
- Debonding/Treatment Completion: Once the teeth have reached their ideal positions, the braces are carefully removed, or you complete your final aligner set. This is often an exciting day! The teeth are then thoroughly cleaned and polished.
- Retention Phase: This is the most critical final step. Immediately after active treatment, your teeth are prone to shifting back to their original positions (relapse). To prevent this, retainers are essential.
Recovery Timeline and Aftercare
The "recovery" phase in orthodontics refers to the retention phase, which is lifelong. Without proper retention, your newly aligned teeth will almost certainly shift back over time.
- Immediate Post-Treatment:
- After braces are removed, your teeth may feel slightly sensitive, and your gums might be a little tender. This usually subsides quickly.
- The orthodontist will take impressions or a digital scan for your retainers.
- Retainer Placement: You will typically receive your custom-made retainers within a few days to a week. There are two main types:
- Removable Retainers:
- Hawley Retainers: Made of acrylic and wire, they are custom-fitted to your mouth.
- Clear Plastic Retainers (Essix Retainers): Similar in appearance to Invisalign aligners, these are clear, vacuum-formed plastic trays.
- Initial Wear: Your orthodontist will instruct you to wear removable retainers full-time (20-22 hours a day) for a specified period, often for 6-12 months.
- Long-Term Wear: After the initial full-time period, wear typically transitions to nighttime only, indefinitely.
- Fixed (Permanent/Bonded) Retainers:
- A thin, custom-fitted wire is bonded to the back of the front teeth (usually canine to canine) on either the upper or lower arch, or both.
- Pros: Always in place, so no compliance issues; invisible from the front.
- Cons: Can be more challenging to clean (requiring floss threaders); if it breaks or debonds, teeth can shift; requires regular check-ups to ensure it's intact.
- Removable Retainers:
- Lifelong Retention: It's a common misconception that once braces are off, treatment is over. The truth is, teeth have a natural tendency to shift throughout life. Therefore, lifelong retainer wear, typically nightly, is crucial to maintain your results. Not wearing your retainers as prescribed is the leading cause of orthodontic relapse.
- Oral Hygiene with Retainers: Clean removable retainers daily with a toothbrush and mild soap or a specialized retainer cleaner. Brush and floss around fixed retainers carefully, using floss threaders.
- Regular Dental Check-ups: Continue with your regular dental check-ups and cleanings, and ensure your orthodontist checks your retainers periodically to ensure they are fitting correctly and intact.
Prevention Strategies
While genetics play a significant role in malocclusion, some issues can be mitigated or prevented through early intervention and management of risk factors.
- Early Orthodontic Evaluation (Age 7): The American Association of Orthodontists (AAO) recommends that children have their first orthodontic evaluation no later than age 7. At this age, the orthodontist can identify subtle problems with jaw growth and erupting teeth that might not be obvious to a general dentist or parent.
- Benefits of Early Evaluation:
- Interceptive Orthodontics (Phase I Treatment): For some children, early treatment can guide jaw growth, create space for permanent teeth, correct harmful oral habits (like thumb-sucking), or address crossbites before they cause permanent damage. This can simplify or even eliminate the need for more complex treatment later.
- Monitoring: For most children, an early evaluation simply establishes a baseline, and the orthodontist can monitor growth and development to determine the optimal time to begin treatment (Phase II, typically during adolescence).
- Benefits of Early Evaluation:
- Addressing Harmful Oral Habits:
- Thumb Sucking/Pacifier Use: Encourage cessation by age 3-4. If habits persist, consult a dentist or orthodontist for strategies or appliances (like habit breakers) to help.
- Tongue Thrusting: Can sometimes be corrected with myofunctional therapy or specific appliances.
- Mouth Breathing: Address underlying causes like allergies or enlarged tonsils/adenoids with a pediatrician or ENT specialist.
- Space Maintenance: If a baby tooth is lost prematurely due to decay or injury, a space maintainer can be placed to hold the space open for the permanent tooth, preventing adjacent teeth from drifting.
- Good Oral Hygiene: Preventing cavities and gum disease helps ensure baby teeth are retained for their full term and adult teeth remain healthy, reducing the risk of premature tooth loss and subsequent alignment issues.
- Protecting Teeth from Trauma: Wearing mouthguards during sports can prevent dental injuries that could lead to tooth loss or displacement.
Cost Ranges in the US (with/without insurance)
The cost of orthodontic treatment varies widely based on the complexity of the case, the type of appliance chosen, the duration of treatment, and the geographic location of the practice.
General Cost Ranges (without insurance):
- Traditional Metal Braces: $3,000 - $7,500
- Ceramic Braces: $3,500 - $8,000
- Self-Ligating Braces: $4,000 - $8,500
- Invisalign (Clear Aligners): $3,500 - $8,500 (Full treatment)
- Lingual Braces: $8,000 - $12,000+
- Limited/Phase I Treatment (Children): $1,500 - $4,000 (Often involving only a few teeth or an expander)
- Retainers (post-treatment): Often included in the total treatment cost, but replacement retainers can cost $100 - $500 each.
Impact of Dental Insurance:
- Orthodontic Coverage: Many dental insurance plans offer some orthodontic coverage, especially for children under 18 years old. Adult orthodontic coverage is less common but increasing.
- Lifetime Maxima: Most plans with orthodontic benefits have a lifetime maximum (e.g., $1,000 - $3,000), rather than an annual maximum. Once this amount is paid out, the benefits are exhausted for that individual.
- Percentage Coverage: Plans typically cover a percentage of the total cost (e.g., 50%) up to their lifetime maximum.
- Payment Plans: Most orthodontic offices offer flexible payment plans, often with a down payment followed by monthly installments, making treatment more affordable.
- Health Savings Accounts (HSAs) and Flexible Spending Accounts (FSAs): These tax-advantaged accounts can be used to pay for orthodontic treatment, saving you money on taxes.
It's highly recommended to consult with your orthodontist's office and your insurance provider to understand your specific benefits and out-of-pocket expenses.
Comparison Table: Braces vs. Clear Aligners
| Feature | Traditional Braces (Metal, Ceramic) | Clear Aligners (Invisalign) |
|---|---|---|
| Visibility | Noticeable (metal most, ceramic less) | Nearly invisible |
| Removability | Non-removable, fixed to teeth | Removable for eating, brushing, flossing |
| Comfort | Can cause initial irritation from brackets/wires, sores on cheeks | Generally smoother, but can cause pressure during aligner changes |
| Oral Hygiene | More challenging, requires special tools (floss threaders, interdental brushes) | Easier, remove aligners to brush and floss normally |
| Dietary Restrictions | Many restrictions (avoid sticky, hard, chewy foods) | None (aligners are removed for eating) |
| Treatment for Complex Cases | Highly effective for all types, including severe malocclusion | Effective for most cases, but complex movements may require braces or attachments |
| Treatment Duration | Varies, typically 12-36 months | Varies, typically 6-24 months (can be shorter for minor cases) |
| Cost (US) | $3,000 - $8,500 (depending on type) | $3,500 - $8,500 |
| Maintenance/Compliance | Requires fewer self-discipline, relies on orthodontist adjustments | Requires high patient compliance (must wear 20-22 hours/day) |
| Emergency Appointments | Can occur for broken wires or brackets | Less common, but lost aligners or attachment issues can happen |
| `` |
For Parents / Pediatric Considerations
Early orthodontic care, often referred to as Phase I or interceptive orthodontics, is a critical component of pediatric dentistry.
- The "Age 7 Rule": As recommended by the American Association of Orthodontists, children should have their first orthodontic evaluation by the age of 7 years. At this age, permanent molars and incisors have usually erupted, allowing the orthodontist to assess the developing bite and identify potential problems with jaw growth, crowding, or harmful habits.
- Why Early Evaluation Matters:
- Guiding Jaw Growth: If there’s a significant discrepancy in jaw size or an incorrect bite pattern (like a crossbite or severe underbite), early treatment can guide the growth of the jaws to create a more balanced facial structure. This might involve palatal expanders or functional appliances.
- Creating Space: Interceptive treatment can create space for crowded, erupting permanent teeth, potentially avoiding extractions later.
- Correcting Harmful Habits: Early intervention can stop habits like prolonged thumb sucking or tongue thrusting before they cause irreversible damage to jaw development and tooth position.
- Reducing Risk of Trauma: Protruding front teeth (often seen in Class II malocclusions) are more prone to injury. Early treatment can reduce this risk.
- Simplifying Future Treatment: Addressing issues early can make Phase II (comprehensive adolescent treatment with braces or aligners) shorter and less complex.
- Phase I Treatment (Interceptive): This usually occurs between ages 7-10 and typically lasts for 6-18 months. It focuses on specific problems, not full tooth alignment. Appliances might include expanders, partial braces, or habit breakers. After Phase I, there’s usually a resting period to allow remaining permanent teeth to erupt.
- Phase II Treatment (Comprehensive): This involves full braces or clear aligners once most or all permanent teeth have erupted (typically ages 11-14). It addresses overall tooth alignment and bite correction.
- Growth and Development: Orthodontists are experts in facial and dental growth. Treating a child during their growth spurts can be highly effective in making significant jaw corrections that would be much more challenging (or require surgery) in adulthood.
Frequently Asked Questions
What is the average cost of orthodontics in the US?
The average cost of full orthodontic treatment in the US ranges from $3,000 to $8,500 without insurance, depending on the type of appliance (braces vs. Invisalign), the complexity of your case, and the duration of treatment. More specialized options like lingual braces can exceed $10,000. Many practices offer payment plans, and dental insurance may cover a portion, typically up to a lifetime maximum.
How much does orthodontic treatment hurt?
Modern orthodontic treatment is much more comfortable than in the past. You can expect some mild discomfort or soreness for a few days after braces are first placed or tightened, or after switching to a new set of Invisalign aligners. This is a sign that your teeth are moving. Over-the-counter pain relievers (like ibuprofen), soft foods, and orthodontic wax (for braces) can help manage this initial discomfort. Most patients adapt quickly.
How long does orthodontic treatment typically last?
The duration of orthodontic treatment varies widely depending on the complexity of the case, the patient's age, and the chosen appliance. On average, full treatment with braces or Invisalign lasts between 12 to 36 months. Minor corrections might take less than a year, while very complex cases, especially those involving jaw surgery, can extend beyond three years. Consistent wear of aligners or proper care of braces can help keep treatment on schedule.
What are the alternatives to traditional braces?
The most popular alternative to traditional metal braces is clear aligner therapy, such as Invisalign. Other options include ceramic braces (which are less noticeable than metal), lingual braces (placed on the inside of the teeth for complete invisibility), and sometimes removable appliances for very minor corrections. For mild cases, some individuals might opt for cosmetic procedures like veneers if the primary concern is aesthetics rather than bite correction.
Does dental insurance cover orthodontics?
Many dental insurance plans offer some coverage for orthodontics, especially for children under 18 years old. Adult orthodontic coverage is less common but becoming more prevalent. Most plans have a lifetime maximum benefit (e.g., $1,000 to $3,000) for orthodontics, rather than an annual limit. It's essential to check with your specific insurance provider and the orthodontic office to understand your benefits and estimated out-of-pocket costs. Health Savings Accounts (HSAs) and Flexible Spending Accounts (FSAs) can also be used.
Do I have to wear a retainer forever after braces?
Yes, absolutely. The retention phase is a lifelong commitment. While you'll likely wear your retainer full-time for the first 6-12 months after active treatment, your teeth have a natural tendency to shift back to their original positions (relapse) throughout life. To maintain your beautiful new smile and bite, most orthodontists recommend wearing your retainer nightly for the rest of your life. Failure to do so is the most common reason for teeth to become misaligned again.
Can adults get braces, or is it just for kids?
Orthodontic treatment is definitely not just for kids! A significant percentage of orthodontic patients are adults, with nearly 2 million adults receiving care from AAO orthodontists in the U.S. and Canada. Thanks to advancements like Invisalign and less noticeable braces options (ceramic, lingual), more adults are seeking treatment to improve their dental health, correct long-standing bite issues, or address shifting teeth. Age is rarely a barrier to orthodontic treatment, provided your teeth and gums are healthy.
When to See a Dentist
Knowing when to seek professional orthodontic advice is key to maintaining optimal oral health.
Routine Care & Evaluation:
- Early Childhood (by age 7): As recommended by the AAO, every child should have an orthodontic evaluation by age 7. This allows the orthodontist to assess growth and development and determine if early intervention (Phase I) is necessary or if monitoring is sufficient.
- Adolescence: If your child has noticeable crooked teeth, gaps, bite problems (like an overbite or underbite), or if their dentist has recommended an orthodontic referral, schedule a consultation during their pre-teen or early teen years when most permanent teeth have erupted.
- Adulthood: If you're an adult experiencing any of the following:
- Noticeable shifting of teeth.
- Discomfort or pain in your jaw (TMJ issues).
- Difficulty chewing or speaking.
- Excessive wear on certain teeth.
- Concerns about your smile's aesthetics due to crooked teeth or gaps.
- Referred by your general dentist for malocclusion or bite issues.
Emergency Signs (See a Dentist/Orthodontist Promptly):
While most orthodontic issues aren't emergencies, some situations warrant immediate attention:
- Severe Pain: If you or your child experience sudden, severe, and persistent pain in the teeth, gums, or jaw that doesn't subside with over-the-counter pain relievers.
- Trauma to the Mouth/Face: Any injury to the teeth, gums, or jaw resulting from an accident, fall, or sports injury. This could include knocked-out, chipped, or displaced teeth.
- Swelling: Unexplained swelling in the gums, face, or jaw area.
- Broken or Damaged Appliances Causing Injury:
- A broken brace bracket that is poking or cutting your cheek or tongue.
- A loose or broken archwire that is causing significant discomfort or injury.
- A lost or severely damaged Invisalign aligner that is preventing proper tooth movement (contact your orthodontist for a replacement).
- ``
In these emergency situations, contact your orthodontist or general dentist as soon as possible. If it's outside of office hours and a true emergency (e.g., severe trauma, uncontrolled bleeding), seek care at an urgent care center or emergency room. For routine concerns or to simply explore your options, a scheduled consultation is the best first step.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.