Leukoplakia Treatment: Complete Guide

Key Takeaways
- Have you ever noticed a persistent, stubborn white patch inside your mouth that just won't go away, even with brushing? While often harmless, such a lesion, known as leukoplakia, demands your attention. **Statistics indicate that up to 10% of leukoplakia cases can eventually develop into oral cancer
Leukoplakia Treatment: Complete Guide
Have you ever noticed a persistent, stubborn white patch inside your mouth that just won't go away, even with brushing? While often harmless, such a lesion, known as leukoplakia, demands your attention. Statistics indicate that up to 10% of leukoplakia cases can eventually develop into oral cancer, making early detection and appropriate leukoplakia treatment absolutely critical for your long-term health. This isn't just a minor irritation; it's a potential warning sign that your body is sending. Ignoring these white patches can have serious, life-altering consequences. Understanding what leukoplakia is, recognizing its symptoms, and knowing your treatment options are vital steps in protecting your oral and overall health.
This comprehensive guide from SmilePedia.net will demystify leukoplakia, offering an in-depth look at its causes, various forms, diagnostic procedures, and the full spectrum of available treatments. We'll delve into the step-by-step process of managing these lesions, from initial consultation to recovery and prevention. You'll also find crucial information on costs, insurance coverage, and important considerations for aftercare. Our goal is to empower you with the knowledge to make informed decisions and work effectively with your dental professional to ensure the best possible outcome.
Key Takeaways:
- Leukoplakia is a persistent white patch in the mouth that cannot be scraped off and is often considered a precancerous lesion.
- Diagnosis typically involves a clinical examination followed by a biopsy, which is essential to determine if cancerous or precancerous cells are present.
- Treatment options range from watchful waiting for low-risk lesions to surgical excision, laser ablation, or cryotherapy for higher-risk or dysplastic patches.
- Surgical removal costs in the US can range from $500 to $3,000+ depending on size, location, and method, with most insurance plans offering partial coverage.
- Smoking and heavy alcohol use are the primary causes, and cessation is the most effective preventive measure.
- Regular follow-up appointments (every 3-6 months) are crucial after diagnosis and treatment due to the risk of recurrence and malignant transformation.
- While rare, a small percentage of leukoplakia lesions, particularly the "non-homogenous" types or those with dysplasia, can transform into squamous cell carcinoma, the most common type of oral cancer.
What It Is: Understanding Leukoplakia
Leukoplakia, derived from Greek words meaning "white" and "plate," refers to a white patch or plaque on the mucous membranes of the mouth that cannot be characterized as any other diagnosable disease and cannot be scraped off. It is a clinical diagnosis, meaning it's identified by its appearance rather than a specific underlying cause at the outset. While many leukoplakic lesions are benign (non-cancerous), a significant portion exhibit dysplasia, which means there are abnormal cell changes that can be precancerous.
The World Health Organization (WHO) defines leukoplakia as "a white plaque of questionable risk having excluded (other) known diseases or disorders that carry no increased risk for cancer." This definition highlights its crucial role as a potentially malignant disorder of the oral cavity. It's an umbrella term for persistent white lesions that don't fit other categories like candidiasis (thrush), lichen planus, or frictional keratosis. The distinction is critical because leukoplakia, unlike these other conditions, carries an inherent risk of transforming into oral squamous cell carcinoma (OSCC), the most common type of oral cancer.
Types and Variations of Leukoplakia
Leukoplakia is not a monolithic condition; it presents in several forms, each with varying degrees of risk for malignant transformation. Understanding these types is vital for accurate diagnosis and determining the most appropriate leukoplakia treatment.
-
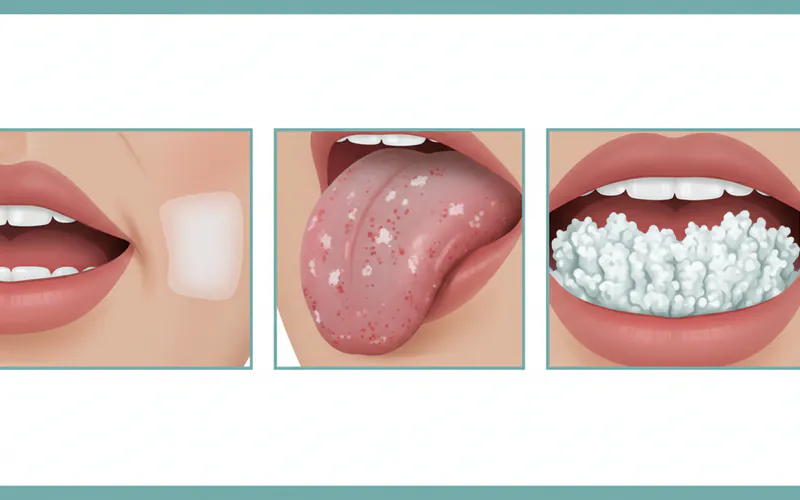
Homogenous Leukoplakia:
- Appearance: This is the most common and generally least concerning type. It appears as a thin, uniformly white, flat lesion with a smooth or finely wrinkled surface. It has a well-defined border and doesn't typically cause symptoms beyond its visible presence.
- Risk: Homogenous leukoplakia has a relatively low risk of malignant transformation, often less than 5%.
- Management: Often managed with watchful waiting and strict removal of causative factors (like tobacco).
-
Non-Homogenous Leukoplakia (Heterogenous Leukoplakia):
- Appearance: This type is more concerning due to its varied and often more aggressive appearance. It can be nodular, verrucous (wart-like), speckled (erythroleukoplakia), or ulcerated. Erythroleukoplakia, in particular, presents as a mixed red and white lesion, with the red (erythroplakic) component being a strong indicator of high-grade dysplasia or carcinoma in situ.
- Risk: Non-homogenous leukoplakia carries a significantly higher risk of malignant transformation, potentially ranging from 10% to over 40%, especially for erythroleukoplakia.
- Management: Due to the higher risk, these lesions almost always warrant immediate biopsy and more aggressive leukoplakia treatment if dysplasia is found.
-
Proliferative Verrucous Leukoplakia (PVL):
- Appearance: PVL is a rare but particularly aggressive form of non-homogenous leukoplakia. It's characterized by multiple, recurrent, widespread white patches that are often wart-like (verrucous) in appearance and tend to expand over time. It can affect various sites in the mouth, often starting in one area and spreading.
- Risk: PVL has an exceptionally high rate of malignant transformation, often exceeding 70-100% over many years. It's highly resistant to treatment and tends to recur, frequently developing into squamous cell carcinoma.
- Management: This type requires highly aggressive and comprehensive management, often involving repeated surgical excisions and very close long-term follow-up.
Understanding these distinctions is crucial, as the type of leukoplakia directly influences the urgency and nature of the leukoplakia treatment plan.
Causes: Why Leukoplakia Happens
While the exact mechanisms aren't always fully understood for every individual case, several key risk factors and contributing causes have been consistently identified for leukoplakia. Addressing these factors is often the first step in both prevention and successful leukoplakia treatment.
-
Tobacco Use:
- Smoking: By far the most significant risk factor. The heat, chemicals, and irritants in cigarette, cigar, and pipe smoke directly damage the oral mucosa, leading to abnormal cellular changes.
- Smokeless Tobacco (Chewing Tobacco, Snuff): The direct contact of tobacco with the oral tissues, especially in the vestibule (the space between the lips/cheeks and teeth), is a potent irritant and carcinogen. "Smoker's keratosis" or "snuff dipper's lesion" are common forms of leukoplakia directly linked to smokeless tobacco.
- Hookah: While sometimes perceived as less harmful, hookah smoke also contains carcinogens and irritants.
-
Alcohol Consumption:
- Heavy and chronic alcohol use, particularly when combined with tobacco use, dramatically increases the risk of leukoplakia and its malignant transformation. Alcohol acts as a solvent, making the oral tissues more permeable to carcinogens from tobacco.
-
Chronic Irritation:
- Ill-fitting dentures: A denture that constantly rubs against the gum or cheek can cause chronic inflammation and tissue changes.
- Rough teeth or fillings: Sharp edges or restorations that constantly irritate the tongue or cheek lining can sometimes lead to localized leukoplakia.
- Trauma: While less common than chemical irritation, repetitive physical trauma can contribute.
-
Human Papillomavirus (HPV):
- Certain high-risk strains of HPV, particularly HPV-16 and HPV-18, are increasingly recognized as contributing factors to oral leukoplakia and subsequent oral cancers, especially those affecting the oropharynx (back of the throat). While traditionally associated with genital warts and cervical cancer, HPV can be transmitted orally.
-
Sun Exposure:
- Actinic Cheilitis: Leukoplakia on the lips, often the lower lip, can be caused by prolonged exposure to sunlight. This condition, known as actinic cheilitis, is a precancerous lesion of the lip.
-
Other Potential Factors:
- Vitamin Deficiencies: Some studies suggest a link between deficiencies in vitamins A, B, and C and an increased risk of leukoplakia, though this is less definitively proven than tobacco and alcohol.
- Candida Infection: While candidiasis (thrush) is a separate condition, some forms of leukoplakia can be secondarily infected with Candida, or a specific type called "candidal leukoplakia" exists, which shares features of both conditions.
- Genetics: While not a primary cause, genetic predisposition may play a role in some individuals' susceptibility.
It's important to note that sometimes, leukoplakia can develop without any clear identifiable cause. These are referred to as idiopathic leukoplakia and still require careful monitoring and management due to their inherent risk.
Signs and Symptoms: What to Look For
Leukoplakia is primarily identified by its visual appearance, and it often causes no pain or discomfort, which is why many individuals delay seeking professional evaluation. This lack of symptoms makes regular self-examinations and professional dental check-ups incredibly important.
Here's what you should look for:
- White Patch or Plaque: The most obvious sign is a white or grayish patch on the soft tissues of your mouth. Unlike food debris or candidiasis (thrush), it cannot be wiped or scraped away.
- Location: While it can appear anywhere in the mouth, common sites include:
- Tongue: Especially the sides or undersurface.
- Floor of the Mouth: The area under the tongue. This site is particularly concerning as lesions here have a higher risk of malignant transformation.
- Inner Cheek (Buccal Mucosa): Often associated with cheek biting or tobacco use.
- Gums (Gingiva): Along the gum line.
- Palate: The roof of the mouth.
- Lips: Especially the lower lip, as mentioned with actinic cheilitis.
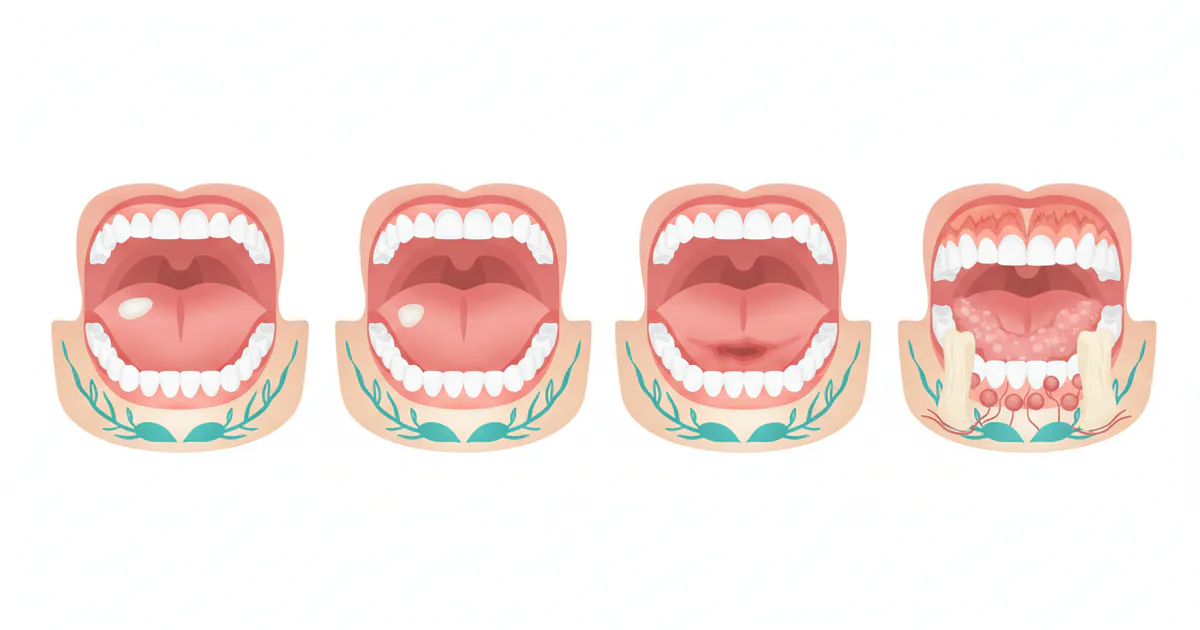
- Texture and Appearance Variations:
- Smooth and Flat: Homogenous leukoplakia typically presents this way.
- Thickened or Hardened: The patch may feel slightly raised or firm to the touch.
- Rough, Wrinkled, or Fissured: The surface might have an irregular texture.
- Verrucous (Wart-like): Bumpy or nodular appearance, common in non-homogenous and PVL.
- Red and White (Erythroleukoplakia): A mixed lesion with both white and red areas. The red areas are particularly suspicious and suggest higher-grade dysplasia or early cancer.
- Size: Leukoplakia can range from a tiny speck to a large, widespread patch covering several centimeters.
- Associated Symptoms (less common, but concerning):
- Discomfort or Pain: While usually painless, some advanced lesions or those that have transformed might cause localized pain, burning, or sensitivity.
- Difficulty Chewing, Swallowing, or Speaking: If the lesion is large or has caused significant tissue changes.
- Changes in Taste: Although rare, some individuals report altered taste sensation.
- Sore Throat or Hoarseness: If the lesion is in the back of the throat or has spread.
Pro Tip: Perform a self-oral cancer screening monthly. Stand in front of a mirror with good lighting. Look at your lips, inner cheeks, gums, tongue (top, sides, and bottom), and the roof of your mouth. Feel for any lumps or changes in texture. If you notice any persistent white or red patches, sores that don't heal, or any unusual changes, schedule an appointment with your dentist immediately. Early detection significantly improves outcomes.
Leukoplakia Treatment Options: A Comprehensive Approach
The primary goal of leukoplakia treatment is to prevent malignant transformation into oral cancer. The choice of treatment depends heavily on the type of leukoplakia, its location, size, and most importantly, the histopathological findings from a biopsy – specifically, the presence and grade of dysplasia (abnormal cell changes).
1. Watchful Waiting and Risk Factor Elimination (Conservative Management)
- When Used: Primarily for homogenous leukoplakia with no or mild dysplasia confirmed by biopsy, especially if the causative factors are clear and reversible (e.g., smoking).
- Process: This involves strict cessation of tobacco and alcohol use. The patient is placed on a rigorous schedule of follow-up appointments (typically every 3-6 months) for clinical examination and repeat biopsies if changes are observed.
- Pros: Non-invasive, avoids surgical risks. Can lead to resolution of the lesion if risk factors are eliminated.
- Cons: Requires significant patient compliance. Carries the inherent risk that the lesion could progress if not closely monitored, delaying definitive leukoplakia treatment.
- Cost: Minimal (follow-up visits, biopsies if needed: $100-$500 per visit/biopsy).
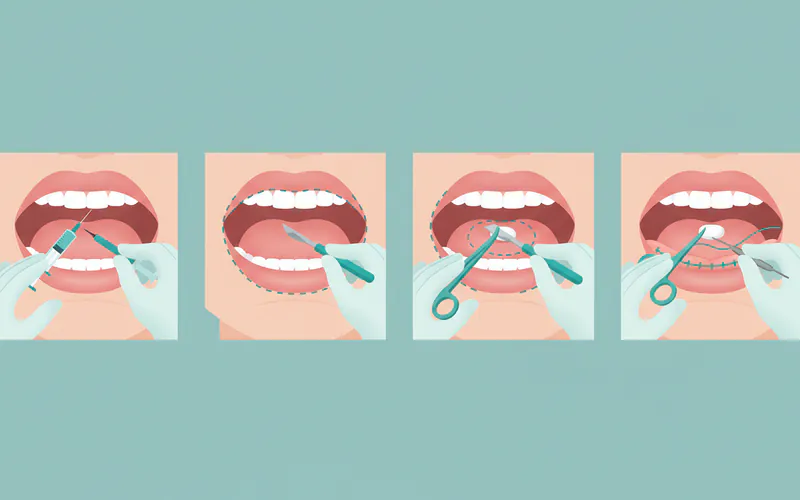
2. Surgical Excision
- When Used: Considered the gold standard for leukoplakia with moderate to severe dysplasia, or when the lesion is small and easily accessible. It allows for complete removal and thorough histopathological evaluation of the entire lesion.
- Process: Under local anesthesia (sometimes general for larger lesions), the lesion is surgically cut out with a margin of healthy tissue around it. The incision is then closed with sutures.
- Pros: High success rate for complete removal, provides definitive diagnosis, and often curative for non-malignant lesions.
- Cons: Can result in scarring, potential for pain and swelling, risk of infection, and nerve damage depending on location. Larger excisions can impact oral function or aesthetics.
- Cost: $500 - $3,000+ in the US, depending on size, location, complexity, and whether it's performed in a dental office or hospital setting. This includes local anesthesia but may not include general anesthesia.
3. Laser Ablation (CO2 Laser)
- When Used: An alternative to conventional surgery, especially for lesions in delicate areas, or those that are widespread but relatively superficial. It's effective for lesions with moderate dysplasia.
- Process: A concentrated beam of light (CO2 laser) is used to vaporize or precisely cut away the abnormal tissue. The laser seals blood vessels and nerve endings, often leading to less bleeding and postoperative pain compared to traditional surgery.
- Pros: Minimally invasive, reduced bleeding, often less postoperative pain and swelling, faster healing, good precision.
- Cons: Does not provide a tissue sample for histopathological analysis of the margins (if vaporized), making it crucial to have a prior definitive biopsy. Can still cause scarring and requires specialized equipment.
- Cost: $1,000 - $4,000+, often slightly more expensive than conventional surgery due to specialized equipment.
4. Cryotherapy
- When Used: Suitable for smaller, superficial lesions, particularly those that are not highly dysplastic.
- Process: Liquid nitrogen or nitrous oxide is used to rapidly freeze and destroy the abnormal tissue. The treated area forms a blister, which then scabs and heals over time.
- Pros: Minimally invasive, relatively quick procedure, generally good healing.
- Cons: Similar to laser ablation, it doesn't always provide a good tissue sample for margin assessment. Can cause temporary pain, swelling, and blistering. Not ideal for large or thick lesions.
- Cost: $300 - $1,500 per session, often requiring multiple sessions.
5. Photodynamic Therapy (PDT)
- When Used: An emerging option for superficial and widespread leukoplakia, especially for patients who are not candidates for surgery or laser. It's gaining traction for its selectivity in targeting abnormal cells.
- Process: A photosensitizing drug is applied topically or injected, which accumulates in the abnormal cells. The area is then exposed to a specific wavelength of light, activating the drug to destroy the precancerous cells.
- Pros: Minimally invasive, highly selective for abnormal cells, can treat large areas.
- Cons: Skin sensitivity to light (photosensitivity) for several weeks post-treatment, can be painful during light exposure, multiple sessions may be required, not yet widely available in all dental practices.
- Cost: $1,500 - $5,000+ per course of treatment, highly variable based on the drug and number of sessions.
6. Medical Management (Topical or Systemic)
- When Used: Primarily as an adjunct to other therapies or for widespread, multifocal leukoplakia with mild dysplasia, especially when surgery is not feasible. Not a standalone primary treatment for high-risk lesions.
- Medications:
- Retinoids (Vitamin A derivatives): Both topical (e.g., tretinoin cream) and systemic (e.g., isotretinoin, etretinate) have been studied. They work by influencing cell growth and differentiation.
- Antioxidants: Beta-carotene, vitamin E, and lycopene have been investigated, often as supplements.
- Anti-inflammatory agents: Some research into NSAIDs or COX-2 inhibitors for their anti-cancer properties.
- Pros: Non-invasive, can be used for widespread lesions.
- Cons: Variable efficacy, often transient results (lesions may recur after stopping medication), potential for significant side effects with systemic retinoids (e.g., liver toxicity, dry skin, teratogenicity). Requires long-term commitment.
- Cost: Varies widely depending on the medication; topical retinoids typically $50-$200/month, systemic retinoids can be $200-$500+/month. Supplements generally $20-$100/month.
ADA Guidelines: The American Dental Association (ADA) emphasizes that a biopsy is mandatory for any persistent white lesion that cannot be diagnosed as another condition and doesn't resolve after removing irritants. For dysplastic lesions, surgical excision remains the preferred treatment due to its definitive nature and ability to confirm clear margins. For high-risk lesions, such as those on the floor of the mouth or lateral tongue, or those with significant dysplasia, immediate and definitive intervention is crucial.
Step-by-Step Process: What to Expect During Leukoplakia Treatment
Understanding the journey from suspicion to resolution can help ease anxiety. Here’s a typical step-by-step process for managing leukoplakia:
1. Initial Consultation and Examination
- Your Role: You notice a suspicious white patch or your dentist identifies one during a routine check-up.
- Dentist's Role: A thorough intraoral examination will be performed. Your dentist will ask about your medical history, lifestyle habits (tobacco, alcohol), and the duration of the lesion. They will visually inspect and palpate (feel) the patch.
- Differentiation: The dentist will attempt to rule out other common white lesions like candidiasis (which can be scraped off), lichen planus, or frictional keratosis.
2. Risk Factor Modification (Initial Phase)
- If a clear irritant is identified (e.g., sharp tooth, ill-fitting denture, tobacco use): Your dentist may advise removing the irritant or stopping the habit (e.g., cessation of smoking/alcohol).
- Re-evaluation: You'll be asked to return in 2-4 weeks to see if the lesion has resolved or significantly diminished. If it has, it was likely a reactive lesion rather than true leukoplakia.
3. Biopsy – The Definitive Diagnostic Step
- If the lesion persists or is suspicious from the outset: A biopsy is the next, crucial step. This is the only way to definitively diagnose leukoplakia and assess for dysplasia or malignant transformation.
- Procedure:
- Local Anesthesia: The area around the lesion is numbed.
- Tissue Removal: A small piece of tissue is surgically removed. This can be an incisional biopsy (removing a part of a larger lesion) or an excisional biopsy (removing the entire small lesion). In some cases, brush biopsy (scraping cells) might be used, but a traditional scalpel biopsy is generally preferred for its diagnostic accuracy.
- Sutures: The site may be closed with a few stitches, which may dissolve or need removal in 7-10 days.
- Pathology Report: The tissue sample is sent to an oral pathologist who examines it under a microscope to determine the precise diagnosis and grade of dysplasia (none, mild, moderate, severe, or carcinoma in situ). This report guides the leukoplakia treatment plan.
- Timeline: Biopsy results typically take 1-2 weeks.
4. Treatment Planning Based on Biopsy Results
- No Dysplasia / Mild Dysplasia: Often managed with strict watchful waiting, cessation of risk factors, and regular follow-up appointments.
- Moderate to Severe Dysplasia / Carcinoma In Situ: These require more aggressive intervention.
- Surgical Excision: Often preferred for complete removal.
- Laser Ablation: A precise option, especially for difficult-to-reach or large superficial lesions.
- Cryotherapy: For smaller, superficial lesions.
- Photodynamic Therapy: Considered in specific cases for widespread lesions.
- Discussion: Your dentist or oral surgeon will discuss all suitable options, their pros and cons, and help you choose the best course of action.
5. Treatment Procedure
- Preparation: You'll receive specific pre-operative instructions (e.g., fasting for general anesthesia, medication adjustments).
- During Treatment: The chosen procedure (surgery, laser, cryotherapy, etc.) is performed. This can take anywhere from 30 minutes to a few hours depending on the complexity.
- Anesthesia: Local anesthesia is common, but general anesthesia may be used for extensive or complex cases.
6. Recovery and Aftercare
- Immediate Post-Op: You'll receive instructions on pain management, diet, oral hygiene, and managing any swelling or bleeding.
- Healing: The healing period can range from 1-2 weeks for minor procedures to several weeks for more extensive surgeries.
- Follow-up: A follow-up appointment is typically scheduled within 1-2 weeks to check healing, remove sutures if necessary, and discuss the final pathology report (if the entire lesion was removed).
7. Long-Term Surveillance
- Crucial Step: Regardless of the initial diagnosis and treatment, long-term surveillance is paramount. Leukoplakia has a significant recurrence rate, and even after successful treatment, new lesions can form, or the original lesion can transform.
- Schedule: You will be advised to have regular follow-up appointments, often every 3-6 months, which may include repeat biopsies if any new or suspicious changes appear. This lifelong vigilance is critical for preventing future issues.
Cost and Insurance for Leukoplakia Treatment in the US
The cost of leukoplakia treatment in the United States can vary significantly based on the diagnostic steps, the chosen treatment method, the size and location of the lesion, the practitioner's fees, geographic location, and whether the procedure is performed in a dental office, outpatient surgical center, or hospital.
Diagnostic Costs:
- Initial Consultation: $50 - $250 (may be covered by insurance).
- Biopsy (Incisional/Excisional):
- Procedure Fee: $250 - $700 (for the dentist/oral surgeon).
- Pathology Fee: $150 - $400 (for the lab analysis).
- Total for Biopsy: $400 - $1,100.
Treatment Costs (Average US Ranges):
| Treatment Method | Average Cost Range (USD) | Key Factors Influencing Cost |
|---|---|---|
| Watchful Waiting | $100 - $500 (per follow-up visit/biopsy if needed) | Number of follow-ups, need for repeat biopsies |
| Surgical Excision | $500 - $3,000+ | Size, location, complexity, type of anesthesia (local vs. general) |
| Laser Ablation | $1,000 - $4,000+ | Size, number of lesions, type of laser, facility fees |
| Cryotherapy | $300 - $1,500 (per session, multiple may be needed) | Size, number of sessions required, clinic fees |
| Photodynamic Therapy | $1,500 - $5,000+ (per course) | Number of sessions, specific photosensitizer drug, facility fees |
| Medical Management | $50 - $500+ (per month for medication) | Type of medication (topical vs. systemic), duration of treatment |
Geographic Variation: Costs tend to be higher in major metropolitan areas (e.g., New York, Los Angeles) compared to rural areas. For example, a surgical excision might be $800 in a small town but $2,000 in a large city.
Insurance Coverage:
- Dental Insurance: Typically covers a portion of diagnostic procedures (exams, X-rays) and some oral surgery. Biopsies and excisions of lesions are often covered under major restorative or oral surgery benefits.
- Coverage can range from 50% to 80% after your deductible is met.
- It's crucial to check if your plan covers "pathology" or "oral surgery for precancerous lesions."
- Medical Insurance: If the lesion is deemed medically necessary for removal (e.g., severe dysplasia, suspicion of malignancy), your medical insurance may cover a significant portion, especially if performed in a hospital or by an oral surgeon.
- Many oral surgeons are also medical doctors (MDs) and can bill medical insurance for these procedures.
- You will likely still be responsible for deductibles, co-pays, and co-insurance.
- Pre-authorization: Always request pre-authorization from your insurance company before any significant procedure to understand your exact coverage and out-of-pocket expenses.
- CPT Codes: Common CPT (Current Procedural Terminology) codes related to leukoplakia treatment include:
- 41110: Excision of lesion of tongue.
- 41116: Excision of lesion of floor of mouth.
- 40810-40814: Excision of lesion of mucosa and submucosa, vestibule of mouth.
- D7465: Excision of benign lesion, intraoral (dental code for biopsy/excision).
Pro Tip: Don't hesitate to ask your dental office or oral surgeon for a detailed cost estimate and to assist you with insurance verification. They often have staff dedicated to navigating insurance claims and can provide clarity on what to expect financially.
Recovery and Aftercare
Proper recovery and aftercare are essential for optimal healing, minimizing complications, and ensuring the success of leukoplakia treatment.
Immediate Post-Treatment:
- Pain Management:
- Over-the-counter (OTC) pain relievers: Ibuprofen (Advil, Motrin) or acetaminophen (Tylenol) are usually sufficient for mild to moderate discomfort.
- Prescription pain medication: May be prescribed for more extensive procedures. Take as directed.
- Swelling: Apply an ice pack to the outside of your face near the treated area for 15-20 minutes on, 15-20 minutes off, for the first 24-48 hours.
- Bleeding: Minor oozing is normal. Avoid rinsing vigorously or spitting, as this can dislodge the blood clot. Apply gentle pressure with a clean gauze pad if bleeding persists.
- Diet:
- Soft foods: For the first few days, stick to soft, cool foods like yogurt, smoothies, mashed potatoes, and scrambled eggs.
- Avoid: Hot, spicy, acidic, crunchy, or hard foods that could irritate the wound.
- Hydration: Drink plenty of fluids.
Oral Hygiene:
- Gentle Rinsing: After 24 hours, gently rinse your mouth with a warm salt water solution (1/2 teaspoon salt in 8 ounces of warm water) 3-4 times a day, especially after meals. This helps keep the area clean and promotes healing.
- Brushing: Continue to brush your teeth, being very gentle around the surgical site. Avoid direct brushing of the wound.
- Antiseptic Mouthwash: Your dentist may prescribe an antiseptic mouthwash (e.g., chlorhexidine) for a short period. Use as directed.
Other Important Instructions:
- Avoid Smoking and Alcohol: This is paramount. These substances significantly impair healing and increase the risk of recurrence and new lesions.
- Avoid Straws: The sucking motion can dislodge blood clots or put pressure on the surgical site.
- Rest: Get plenty of rest to aid your body's healing process.
- Activity: Avoid strenuous exercise for a few days to a week, as advised by your dentist.
- Sutures: If you have non-dissolvable sutures, you'll need to return for their removal, typically in 7-10 days. Dissolvable sutures will disappear on their own.
Follow-Up Appointments:
- Initial Check-up: Your dentist will schedule a follow-up appointment (usually within 1-2 weeks) to monitor healing and discuss the final pathology report.
- Long-Term Surveillance: This is perhaps the most critical aspect of aftercare for leukoplakia. Even after successful treatment, there is a risk of recurrence or the development of new lesions, as well as the potential for malignant transformation over time.
- Frequency: Expect to have regular follow-up examinations with your dentist or oral surgeon every 3-6 months for several years, or even lifelong, depending on the initial diagnosis and risk factors.
- Purpose: These appointments allow for early detection of any changes, which is crucial for successful outcomes.
Prevention: How to Reduce Your Risk
Preventing leukoplakia, and by extension, oral cancer, largely involves modifying lifestyle choices and maintaining excellent oral health practices.
- Eliminate Tobacco Use: This is the single most effective preventive measure.
- Quit Smoking: Cessation programs, nicotine replacement therapy, and support groups can help.
- Stop Smokeless Tobacco: Discontinue use of chewing tobacco, snuff, and dip.
- Moderate Alcohol Consumption:
- Limit alcohol intake to recommended guidelines (up to one drink per day for women, two for men). Ideally, avoid it entirely, especially if you also use tobacco.
- Maintain Excellent Oral Hygiene:
- Brush twice daily, floss daily: Removes plaque and reduces chronic inflammation.
- Regular Dental Check-ups (every 6 months): Crucial for early detection. Your dentist can spot suspicious lesions before you even notice them.
- Oral Cancer Screenings: Many dentists perform visual and tactile oral cancer screenings as part of routine check-ups. Adjunctive screening tools (e.g., light-based systems) may also be used.
- Protect Your Lips from Sun Exposure:
- Use lip balm with SPF 30 or higher when outdoors, especially for prolonged periods.
- Wear a wide-brimmed hat to shade your face.
- Address Chronic Irritation:
- Promptly repair ill-fitting dentures, broken fillings, or sharp teeth. Remove any sources of constant irritation.
- Consider HPV Vaccination:
- The HPV vaccine (Gardasil 9) protects against the strains of HPV most commonly associated with oral cancer (HPV-16 and HPV-18). It's recommended for adolescents and young adults, but adults up to age 45 who have not been adequately vaccinated may also benefit from vaccination after discussion with their healthcare provider.
- Healthy Diet:
- Consume a diet rich in fruits and vegetables, which are high in antioxidants and may help protect against cellular damage.
Risks and Complications
While many leukoplakia lesions remain benign, certain risks and complications are associated with the condition itself and its treatment.
Risks Associated with Leukoplakia Itself:
- Malignant Transformation: This is the most significant risk. A certain percentage of leukoplakia, especially non-homogenous types, those with moderate to severe dysplasia, and PVL, can transform into squamous cell carcinoma. The rate varies but is a compelling reason for vigilance.
- Recurrence: Even after successful removal, leukoplakia can recur in the same location or appear in new locations elsewhere in the mouth. This is particularly common in individuals who continue their risk habits (tobacco, alcohol).
- Progression: Lesions with mild dysplasia can progress to moderate or severe dysplasia over time.
Risks and Complications of Leukoplakia Treatment:
- Pain and Swelling: Common after any surgical or ablative procedure. Usually manageable with medication.
- Infection: Any surgical wound carries a risk of infection. Your dentist may prescribe antibiotics, or you might need them if signs of infection appear (increased pain, swelling, pus, fever).
- Bleeding: Post-operative bleeding can occur, especially in the first 24 hours.
- Scarring: Surgical removal or laser treatment can leave scar tissue, which may impact aesthetics or, in rare cases, oral function (e.g., if on the tongue or near a joint).
- Nerve Damage: Depending on the lesion's location, there's a small risk of temporary or permanent nerve damage, leading to numbness, altered sensation, or (rarely) motor deficits.
- Delayed Healing: Factors like continued smoking, poor nutrition, or underlying medical conditions can prolong the healing process.
- Anesthesia Risks: As with any procedure involving anesthesia, there are minor risks, which your provider will discuss.
- Incomplete Removal: If the entire lesion or all abnormal cells are not removed (e.g., if margins are not clear), the risk of recurrence or malignant transformation remains high. This necessitates further treatment.
Children / Pediatric Considerations
Leukoplakia is extremely rare in children and adolescents. When it does occur, it's typically associated with specific underlying conditions or habits.
- Causes in Children:
- Chronic irritation: Such as persistent cheek biting, prolonged use of pacifiers, or dental trauma.
- Immunosuppression: Children with weakened immune systems due to medical conditions or medications.
- Genetic syndromes: Very rarely, certain genetic conditions can manifest with oral lesions.
- Tobacco exposure: Though uncommon, direct or secondhand tobacco exposure can be a factor.
- HPV: While HPV can be found in children, HPV-related oral leukoplakia is exceedingly rare.
- Diagnosis and Treatment:
- Any persistent white patch in a child's mouth should be promptly evaluated by a pediatric dentist or oral pathologist.
- A biopsy is still the definitive diagnostic tool.
- Treatment would be conservative where possible (e.g., removing the source of irritation), but surgical removal may be necessary if dysplasia is present, similar to adults, albeit with careful consideration of the child's growth and development.
- Parental Guidance: Parents should be vigilant about any unusual or persistent oral lesions in their children and seek professional dental advice without delay. While the risk of malignancy is vastly lower than in adults, any unusual finding warrants investigation.
Cost Breakdown
Understanding the granular cost breakdown can help you prepare financially for leukoplakia treatment.
Typical Scenario (Biopsy & Excision of a Moderately Dysplastic Lesion):
-
Initial Dental Exam/Consultation:
- Cost: $50 - $250
- Insurance Coverage: Often partially or fully covered by dental insurance.
- Out-of-pocket: $0 - $150 (co-pay, deductible)
-
Incisional Biopsy (to diagnose and grade dysplasia):
- Dentist/Surgeon Fee: $250 - $700
- Pathology Lab Fee: $150 - $400
- Total Biopsy: $400 - $1,100
- Insurance Coverage: Typically 50-80% of allowed amount by dental/medical insurance after deductible.
- Out-of-pocket: $200 - $600+
-
Surgical Excision (definitive treatment for moderate dysplasia):
- Surgeon's Fee: $500 - $2,000 (for a single, medium-sized lesion with local anesthesia)
- Anesthesia Fee (if general anesthesia is used): $300 - $1,000+ per hour (for an anesthesiologist/CRNA)
- Facility Fee (if outpatient surgical center): $200 - $800
- Total Excision: $500 - $3,800+ (highly variable)
- Insurance Coverage: Often 50-80% of allowed amount by medical/dental insurance.
- Out-of-pocket: $250 - $1,500+ (depending on total cost and coverage)
-
Post-Treatment Follow-up Appointments:
- Cost: $100 - $300 per visit (typically 3-6 months apart for several years)
- Insurance Coverage: May be covered as routine exams or specific post-operative care.
- Out-of-pocket: $0 - $150 per visit
Total Estimated Out-of-Pocket for a full course of diagnosis and treatment for a single lesion (excluding long-term surveillance):
- Low End: ~$450 - $1,000 (with good insurance, for a simple case)
- Mid-Range: ~$1,000 - $2,500 (average case with standard insurance)
- High End: ~$2,500 - $5,000+ (complex case, extensive lesion, out-of-network, or without insurance)
Payment Plans and Financing Options:
- Dental Office Payment Plans: Many dental offices offer in-house payment plans, allowing you to pay for treatment in installments.
- Third-Party Medical Financing: Services like CareCredit are specifically designed for healthcare expenses, offering interest-free promotional periods or low-interest payment plans.
- Health Savings Accounts (HSAs) & Flexible Spending Accounts (FSAs): If you have an HSA or FSA, you can use pre-tax dollars to cover eligible medical and dental expenses, including leukoplakia treatment.
- Negotiation: For uninsured patients, it's sometimes possible to negotiate a discount for upfront cash payment.
Cost-Saving Tips:
- Use In-Network Providers: Always choose dentists and oral surgeons who are in-network with your insurance plan to maximize benefits and minimize out-of-pocket costs.
- Understand Your Benefits: Before any procedure, thoroughly review your insurance policy or call your provider to understand your deductible, co-pays, co-insurance, and annual maximums.
- Get Itemized Estimates: Ask for a detailed, itemized estimate of all expected costs from your provider before starting treatment.
- Preventive Care: Regular dental check-ups are the best "cost-saving tip." Early detection of leukoplakia can lead to simpler, less expensive treatments.
Frequently Asked Questions
How long does it take for leukoplakia to turn into cancer?
The timeline for malignant transformation is highly variable and unpredictable. It can range from months to many years, or it may never transform at all. Factors like the type of leukoplakia (non-homogenous has a higher risk), degree of dysplasia, and continued risk habits (smoking, alcohol) influence this timeline. This unpredictability is precisely why diligent monitoring and timely leukoplakia treatment are crucial.
Is leukoplakia painful?
Typically, leukoplakia itself is painless and asymptomatic. This lack of discomfort is often why individuals delay seeking professional evaluation. However, if the lesion becomes significantly irritated, infected, or has already transformed into cancer, it can cause localized pain, burning, or sensitivity.
What is the success rate of leukoplakia treatment?
The success rate for complete removal and non-recurrence varies by treatment method and the nature of the lesion. Surgical excision generally has a high success rate (e.g., 80-90% for a single, non-dysplastic lesion). However, the overall "success" is measured by preventing malignant transformation and managing recurrence, which requires lifelong surveillance. Proliferative Verrucous Leukoplakia (PVL) has a very high recurrence rate and a low treatment success rate long-term.
Can leukoplakia go away on its own?
In some cases, especially with homogenous leukoplakia linked to reversible irritants (like tobacco), the lesion can resolve or significantly regress if the irritant is completely removed. However, true leukoplakia that persists after removing irritants generally does not disappear on its own and requires professional management, including a biopsy, to assess its malignant potential.
Is "cat mouth cancer" related to human leukoplakia?
No, "cat mouth cancer" refers to oral cancers that affect felines, which are distinct from human leukoplakia. While cats can develop oral squamous cell carcinoma, this article focuses exclusively on human oral health. If you are concerned about your pet, please consult a veterinarian.
Are there any natural remedies for leukoplakia?
While a healthy diet rich in fruits and vegetables (high in antioxidants) is beneficial for overall oral health and may support cellular health, there are no scientifically proven natural remedies that can effectively treat or cure leukoplakia. Relying solely on natural remedies without professional diagnosis and treatment can be dangerous due to the risk of malignant transformation. Always follow your dental professional's advice.
What is the typical recovery time after leukoplakia surgery?
Recovery time depends on the size and location of the lesion and the method of removal. For a small surgical excision, you might experience mild discomfort for a few days and complete healing within 1-2 weeks. Larger excisions or those in sensitive areas might require longer, up to several weeks, with a softer diet and diligent oral care.
Can stress cause leukoplakia?
While chronic stress can impact overall immune function and lead to various health issues, there is no direct scientific evidence linking stress as a primary cause of leukoplakia. The main risk factors remain tobacco, alcohol, and chronic irritation.
How often do I need follow-up appointments after treatment?
Regardless of the treatment, long-term surveillance is critical. For most cases, follow-up appointments are recommended every 3-6 months for at least a few years, or potentially lifelong, especially if you have persistent risk factors or a history of dysplasia. Your dentist or oral surgeon will determine the precise schedule.
When to See a Dentist
Given the potential for malignant transformation, knowing when to seek professional dental attention for any oral changes is paramount.
You should see a dentist immediately if you notice any of the following:
- A persistent white or reddish patch in your mouth that does not go away after 2-3 weeks, especially if it cannot be scraped off.
- Any non-healing sore or ulcer in your mouth that lasts longer than 2 weeks.
- A lump, thickening, or rough spot in your mouth or on your lip.
- Difficulty chewing, swallowing, speaking, or moving your tongue or jaw.
- Numbness or persistent pain/soreness in any area of your mouth, face, or neck.
- A persistent sore throat or hoarseness that doesn't resolve.
- Unexplained bleeding in your mouth.
- A chronic bad breath that doesn't improve with hygiene.
These are potential red flags that warrant immediate investigation. Do not delay. Early detection of leukoplakia or any form of oral cancer drastically improves the prognosis and the effectiveness of leukoplakia treatment. Regular dental check-ups, ideally every six months, are your best defense, as your dentist is trained to spot subtle changes you might miss during self-examination.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Floor of Mouth Cancer: Complete Guide
Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral c
February 23, 2026
Oral Cancer Stages Pictures: Complete Guide
Oral cancer, a serious and potentially life-threatening disease, affects thousands of Americans each year. According to the American Cancer Society, approximately 54,000 new cases of oral cavity or oropharyngeal cancer are diagnosed annually in the United States. While these numbers can be daunt
February 23, 2026
Can You Die From Mouth Cancer
Oral cancer is a formidable disease, often striking with insidious subtlety before revealing its devastating potential. It's a question that weighs heavily on the minds of those who receive a diagnosis or even those simply concerned about unusual oral symptoms: can you die from mouth cancer? The
February 23, 2026

Mouth Cancer Photos: Complete Guide
Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,23
February 23, 2026