Mouth Cancer Photos: Complete Guide

Key Takeaways
- Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,23
Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,230 deaths are attributed to it each year. Understanding what mouth cancer looks like, recognizing its early signs, and knowing the available treatments are crucial steps in improving survival rates and quality of life. This comprehensive guide, complete with insights into identifying potential issues, including what to look for in mouth cancer photos, aims to be your definitive resource. We will delve into the various types of oral cancers, their causes, diagnostic methods, extensive treatment options including oral cancer surgery, recovery pathways, and critical prevention strategies. Our goal is to empower you with the knowledge to protect your oral health and seek timely professional care.
Key Takeaways:
- Early Detection is Crucial: Oral cancer survival rates increase significantly from 69% for localized disease to 39% for distant metastasis if detected early. Regular dental check-ups are vital for screening.
- Common Signs: Persistent sores (lasting >2 weeks), red or white patches (erythroplakia or leukoplakia), lumps, difficulty swallowing, or unexplained numbness are red flags.
- Primary Risk Factors: Tobacco use (smoking and smokeless), heavy alcohol consumption, and Human Papillomavirus (HPV) infection are leading causes.
- Treatment Modalities: Treatment typically involves oral cancer surgery, radiation therapy, chemotherapy, or a combination. The choice depends on cancer type, stage, and location.
- Cost Implications: Oral cancer treatment can be extremely expensive, ranging from $10,000 for early-stage surgery to over $200,000 for advanced, multi-modal therapies, even with insurance.
- Recovery Focus: Post-treatment care often requires speech therapy, nutritional support, and physical therapy to regain function, lasting from several weeks to many months.
- Prevention is Key: Quitting tobacco and alcohol, HPV vaccination, maintaining a healthy lifestyle, and consistent dental screenings are the most effective preventive measures.
Understanding Mouth Cancer: What It Is
Mouth cancer, also known as oral cancer or oral cavity cancer, refers to any cancer that develops in the tissues of the mouth. This includes the lips, tongue, gums, the floor of the mouth, the inner lining of the cheeks (buccal mucosa), the hard and soft palate, and the area behind the wisdom teeth (retromolar trigone). When discussing oral cancer, medical professionals often include oropharyngeal cancer, which affects the back of the throat, tonsils, and base of the tongue.

Oral cancer is characterized by the uncontrolled growth of abnormal cells that form tumors. These tumors can invade surrounding tissues and, if left untreated, can metastasize (spread) to other parts of the body, such as the lymph nodes in the neck, lungs, or liver. Early detection is paramount because oral cancer, like many cancers, is most treatable in its initial stages before it has a chance to spread extensively. Unfortunately, a significant number of oral cancers are diagnosed in later stages due to a lack of awareness of symptoms or delayed dental visits.
The Importance of Visual Identification
While a professional diagnosis is always required, familiarizing yourself with mouth cancer photos can be a critical first step in recognizing potential issues. Understanding what early lesions might look like can prompt you to seek a dental or medical evaluation sooner, potentially making a life-saving difference. It's important to remember that many benign conditions can mimic early signs of oral cancer, which is why self-diagnosis based solely on images is not recommended. Instead, use visual guides as an educational tool to know when to seek expert opinion.
Types of Mouth Cancer
Oral cancers are not a single disease but rather a group of cancers originating from different cell types within the mouth. The vast majority, however, fall under one primary category:
Squamous Cell Carcinoma (SCC)
This is by far the most common type of oral cancer, accounting for approximately 90% of all cases. Squamous cells are the flat, thin cells that line the surfaces of the mouth and throat. SCC can appear in various forms, including:
- Leukoplakia: White or grayish patches that cannot be scraped off. While often benign, approximately 5-17% of leukoplakia cases are precancerous (dysplastic) or already cancerous.
- Erythroplakia: Red, velvety patches that are often flat or slightly raised. These are significantly more likely to be cancerous or severely dysplastic than leukoplakia, with 75-90% posing a risk.
- Erythroleukoplakia (Speckled Leukoplakia): A mix of red and white patches, which also carries a high risk of malignancy.
- Ulcers: Persistent sores that do not heal within two weeks.
Verrucous Carcinoma
A rare, slow-growing subtype of squamous cell carcinoma, verrucous carcinoma accounts for less than 10% of oral cancers. It typically presents as a large, warty growth, often in individuals who use smokeless tobacco. While it rarely metastasizes, it can be locally destructive.
Minor Salivary Gland Cancers
These cancers develop in the small salivary glands located throughout the mouth lining. Types include adenoid cystic carcinoma, mucoepidermoid carcinoma, and polymorphous adenocarcinoma. These are much less common but can occur on the palate, buccal mucosa, or tongue.
Lymphoma
Lymphoma can sometimes originate in the oral cavity, particularly on the tonsils or base of the tongue, as part of non-Hodgkin lymphoma. This type of cancer affects the lymphocytes (immune cells).
Melanoma
Oral melanoma is extremely rare, accounting for less than 1% of all melanomas. It appears as dark, pigmented lesions, often on the palate or gingiva. Oral melanoma is aggressive and often diagnosed at a late stage.
Causes and Risk Factors for Oral Cancer
Oral cancer development is often multifactorial, meaning several elements can contribute to its onset. Recognizing these risk factors is key to prevention.
1. Tobacco Use
Tobacco is the single biggest risk factor for oral cancer. This includes:
- Smoking: Cigarettes, cigars, and pipes significantly increase risk. The heat and carcinogens directly irritate oral tissues.
- Smokeless Tobacco: Chewing tobacco, snuff, and dip are particularly dangerous, as the tobacco is held directly against the gums and inner cheek, where carcinogens are absorbed directly. Users of smokeless tobacco have a 50-fold increased risk of developing oral cancer compared to non-users.
2. Alcohol Consumption
Heavy and prolonged alcohol consumption is another major risk factor. Alcohol acts as an irritant and can also enhance the penetration of other carcinogens into the oral tissues. The risk is significantly amplified when alcohol use is combined with tobacco use, creating a synergistic effect that can increase the risk by up to 15 times compared to individuals who neither smoke nor drink.
3. Human Papillomavirus (HPV) Infection
Certain strains of HPV, particularly HPV-16, are a growing cause of oropharyngeal cancers (cancers of the back of the throat, tonsils, and base of the tongue). This sexually transmitted infection is now considered a leading cause of oropharyngeal cancer, especially in younger, non-smoking individuals. HPV-related oral cancers tend to respond better to treatment than those caused by tobacco and alcohol.
4. Sun Exposure
Excessive exposure to sunlight is a primary cause of lip cancer, particularly on the lower lip. Farmers, fishermen, and others who spend extended periods outdoors are at higher risk.
5. Poor Nutrition
A diet low in fruits and vegetables and high in processed foods may increase the risk of oral cancer. Antioxidants found in fresh produce are believed to protect cells from damage.
6. Weakened Immune System
Individuals with compromised immune systems, such as organ transplant recipients or those with HIV/AIDS, have an increased risk of developing various cancers, including oral cancer.
7. Genetics and Family History
While not as strong a factor as tobacco or alcohol, a family history of head and neck cancers may slightly increase an individual's risk. Certain genetic predispositions can make some people more susceptible.
8. Age and Gender
Oral cancer predominantly affects older adults, with the average age of diagnosis around 62. However, HPV-related cases are increasingly seen in younger individuals. Historically, men have been twice as likely as women to develop oral cancer, largely due to higher rates of tobacco and alcohol use, though this gap is narrowing.
Recognizing the Signs and Symptoms of Mouth Cancer
Early detection is paramount, and knowing what to look for can be life-saving. The key is persistence – any change that doesn't resolve within two weeks warrants a professional evaluation.
Common Warning Signs:
- Persistent Sore or Ulcer: A sore in the mouth or on the lip that does not heal within two weeks. This is one of the most common early indicators. It may be painless initially, which can lead to delayed diagnosis.
- Red or White Patches:
- Leukoplakia: White or grayish patches on the gums, tongue, cheek lining, or floor of the mouth. These are typically firm and cannot be wiped away. While often benign, they can be precancerous.
- Erythroplakia: Red, velvety patches in the mouth. These are less common than leukoplakia but are significantly more likely to be cancerous or severely dysplastic.
- Erythroleukoplakia (Speckled Leukoplakia): A mix of red and white patches, carrying a very high risk of malignancy.
- Lump or Thickening: Any unexplained lump, thickening, swelling, crust, or eroded area on the lips, gums, tongue, or anywhere else in the mouth or throat.
- Difficulty Chewing or Swallowing (Dysphagia): A persistent sensation that food is catching in your throat, or pain when chewing or swallowing.
- Chronic Sore Throat or Hoarseness: A persistent sore throat, feeling of something caught in the throat, or voice changes that don't improve.
- Numbness or Pain: Unexplained numbness, tingling, or pain in any area of the face, mouth, or neck. This could indicate nerve involvement.
- Bleeding in the Mouth: Unexplained bleeding from the mouth or gums that isn't related to injury or routine brushing.
- Loose Teeth or Dentures: Teeth that become loose without a clear dental reason, or dentures that no longer fit properly.
- Jaw Swelling or Pain: Swelling of the jaw or pain in the jaw.
- Earache: A persistent earache in one ear, especially when there are no signs of infection and it's accompanied by other oral symptoms. This is often referred to as "referred pain" from the tumor.
- Unexplained Weight Loss: Significant, unintentional weight loss can be a symptom of advanced cancer.
Pro Tip: Perform regular self-checks of your mouth. Stand in front of a mirror with good lighting. Open your mouth wide, stick out your tongue, and use your fingers to feel for any lumps or tender spots on your tongue, cheeks, and floor of your mouth. Check your lips and roof of your mouth. Pay close attention to any changes in color or texture. If anything looks or feels unusual and persists for more than two weeks, schedule an appointment with your dentist or doctor.
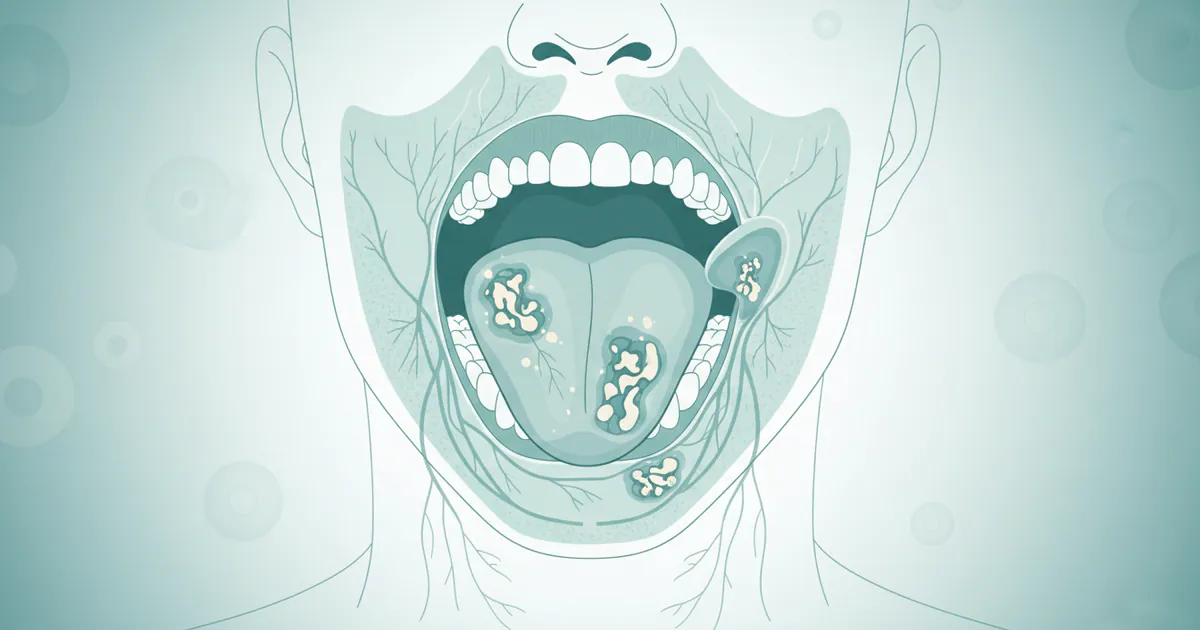
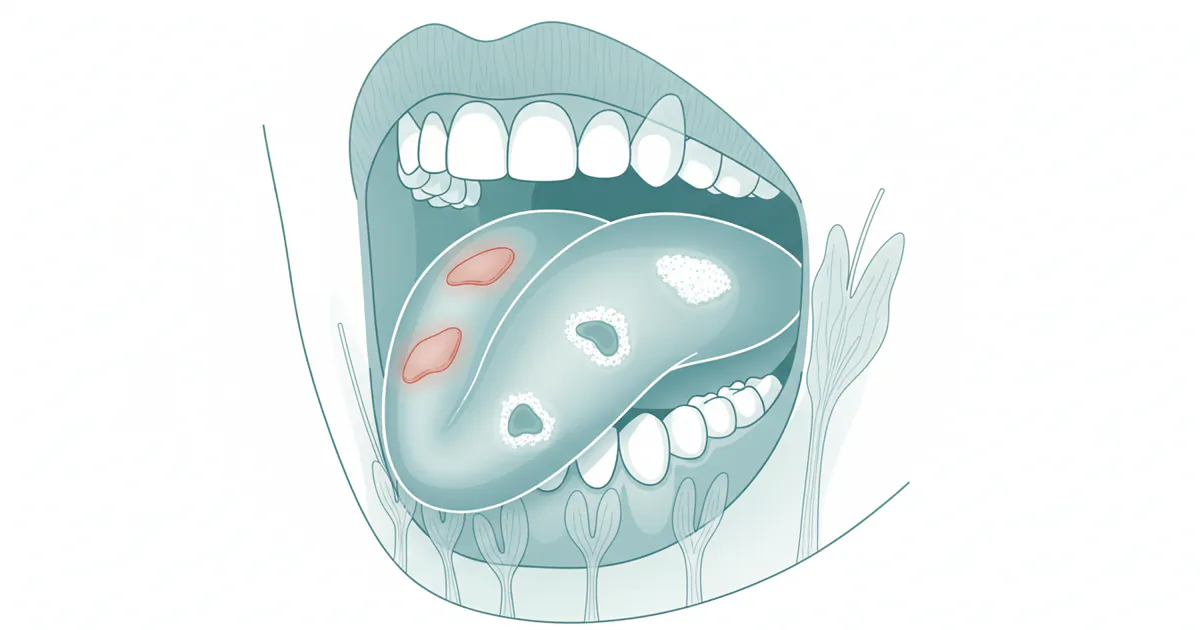
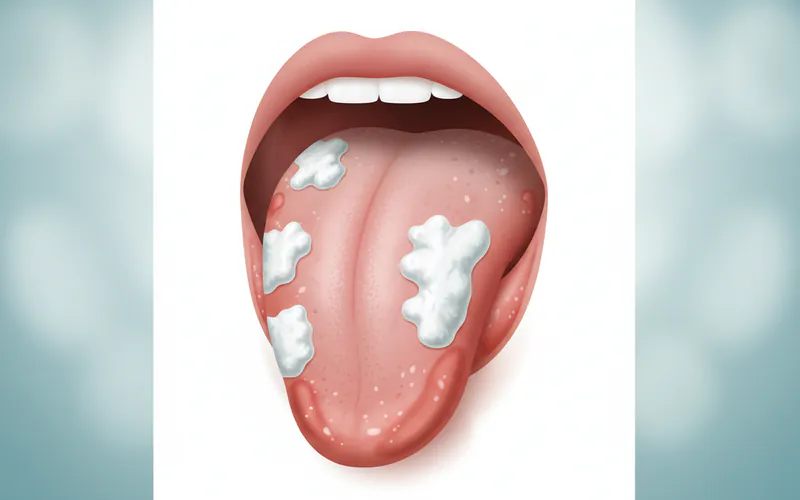 This image should display clear, distinct examples of a white patch (leukoplakia) on the tongue or inner cheek, and a red velvety patch (erythroplakia) on the floor of the mouth or soft palate, highlighting the subtle but crucial visual differences.
This image should display clear, distinct examples of a white patch (leukoplakia) on the tongue or inner cheek, and a red velvety patch (erythroplakia) on the floor of the mouth or soft palate, highlighting the subtle but crucial visual differences.
Diagnosing Mouth Cancer
A thorough diagnostic process is essential to confirm the presence of cancer, determine its type, and establish its stage.
1. Oral Examination and Screening
Your dentist or doctor will perform a visual and manual examination of your mouth, throat, and neck. They will look for any suspicious lesions, swellings, or areas of tenderness. Many dental professionals use adjunctive screening tools like special lights (e.g., VELscope, Identafi) or rinses (e.g., Toluidine blue) to help identify abnormal tissues that might not be visible to the naked eye. While these tools can help flag suspicious areas, they are not diagnostic on their own. The American Dental Association (ADA) recommends regular oral cancer screenings as part of routine dental check-ups, especially for high-risk individuals.
2. Biopsy
If a suspicious area is found, a biopsy is the definitive diagnostic test. A small tissue sample is removed and sent to a pathologist for microscopic examination.
- Incisional Biopsy: A small piece of the lesion is removed.
- Excisional Biopsy: The entire lesion is removed.
- Brush Biopsy (OralCDx): A brush is used to collect cells from the suspicious area. While less invasive, it's generally used for screening or in conjunction with an incisional biopsy for definitive diagnosis.
3. Imaging Tests
Once cancer is diagnosed, imaging tests are used to determine the extent of the cancer (staging) and check for metastasis.
- CT Scan (Computed Tomography): Provides detailed cross-sectional images, useful for assessing bone involvement and spread to lymph nodes.
- MRI (Magnetic Resonance Imaging): Offers excellent soft tissue contrast, helpful for evaluating tumor size, depth of invasion, and nerve involvement.
- PET Scan (Positron Emission Tomography): Often combined with CT (PET-CT), it helps identify metabolically active cancer cells throughout the body, detecting spread to distant sites.
- Panorex X-ray: A panoramic X-ray of the jaws and teeth can show bone involvement.
- Ultrasound: Can be used to assess lymph nodes in the neck.
Treatment Options for Oral Cancer
Treatment for oral cancer is highly individualized, depending on the cancer's stage, location, type, the patient's overall health, and personal preferences. A multidisciplinary team of specialists, including oral surgeons, oncologists, radiation oncologists, reconstructive surgeons, speech therapists, and nutritionists, typically collaborates on the treatment plan.
Surgery
Oral cancer surgery is often the primary treatment for early-stage oral cancers and a critical component for many advanced stages. The goal is to remove the tumor completely along with a margin of healthy tissue (known as a "clear margin") to ensure all cancer cells are eradicated.
Types of Surgical Procedures:
- Wide Excision: Removal of the primary tumor and a surrounding margin of healthy tissue. This can involve parts of the tongue (glossectomy), jawbone (mandibulectomy), or palate (maxillectomy).
- Glossectomy: Partial or total removal of the tongue.
- Mandibulectomy: Removal of a portion of the jawbone.
- Maxillectomy: Removal of part of the upper jaw or palate.
- Neck Dissection: If cancer has spread to the lymph nodes in the neck, or if there's a high risk of spread, these nodes are surgically removed to prevent further metastasis.
- Reconstructive Surgery: After extensive tumor removal, reconstructive surgery (e.g., using tissue flaps from other parts of the body like the forearm or thigh) may be necessary to restore function (swallowing, speech) and appearance. This is a complex procedure often performed immediately after tumor removal.
Pros of Surgery:
- Offers the best chance of cure for early-stage cancers.
- Can provide immediate removal of the cancerous tissue.
- Allows for clear margin assessment to confirm complete removal.
Cons of Surgery:
- Can lead to significant disfigurement and functional impairment (speech, swallowing, chewing).
- Risk of complications like infection, bleeding, nerve damage.
- Requires a significant recovery period.
- May necessitate reconstructive surgeries.
Radiation Therapy
Radiation therapy uses high-energy X-rays or other particles to kill cancer cells or inhibit their growth. It can be used:
- As a primary treatment: For smaller tumors or when surgery is not feasible.
- Adjuvantly (after surgery): To kill any remaining cancer cells and reduce the risk of recurrence, especially if margins were close or positive, or if lymph nodes were involved.
- Neoadjuvantly (before surgery): To shrink large tumors.
- Palliatively: To relieve symptoms of advanced cancer.
Types of Radiation Therapy:
- External Beam Radiation Therapy (EBRT): The most common type, delivered from a machine outside the body. Often administered daily for 5-7 weeks.
- Brachytherapy: Radioactive seeds or pellets are temporarily or permanently placed directly into the tumor or nearby tissues.
Pros of Radiation Therapy:
- Non-invasive (EBRT).
- Can preserve organ function and appearance in some cases.
Cons of Radiation Therapy:
- Significant side effects: mucositis (painful mouth sores), xerostomia (dry mouth), difficulty swallowing, taste changes, skin reactions, fatigue, osteoradionecrosis (bone death, especially in the jaw).
- Long treatment duration.
- Damage to surrounding healthy tissues.
Chemotherapy
Chemotherapy uses drugs to kill cancer cells throughout the body. It is rarely used alone for oral cancer but is often combined with radiation therapy (chemoradiation) for more advanced stages, or when cancer has spread.
Pros of Chemotherapy:
- Systemic treatment, can target cancer cells wherever they are in the body.
- Can enhance the effectiveness of radiation therapy.
Cons of Chemotherapy:
- Significant systemic side effects: nausea, vomiting, hair loss, fatigue, mouth sores, weakened immune system, nerve damage.
- Does not typically cure oral cancer on its own.
Targeted Therapy
These drugs specifically target molecules involved in cancer cell growth and survival, often with fewer side effects than traditional chemotherapy. For oral cancer, agents that target the epidermal growth factor receptor (EGFR) are sometimes used.
Immunotherapy
Immunotherapy harnesses the body's own immune system to fight cancer. Drugs like checkpoint inhibitors help the immune system recognize and attack cancer cells that have been "hiding" from it. This is a newer treatment option, mainly used for recurrent or metastatic oral cancers.
[TABLE: Comparison of Oral Cancer Treatment Modalities]
| Treatment Modality | Primary Use Cases | Pros | Cons | Estimated Cost Range (USD, per cycle/course) | Recovery Time |
|---|---|---|---|---|---|
| Surgery | Early-stage, localized tumors; removing metastases | Best chance of cure for localized disease; immediate tumor removal. | Invasive; potential for disfigurement, functional loss; risk of infection/bleeding. | $10,000 - $100,000+ (depending on complexity) | Weeks to months; long-term rehabilitation often needed. |
| Radiation Therapy | Early-stage (alone), adjuvant to surgery, palliative, chemoradiation. | Non-invasive (EBRT); can preserve organ appearance. | Significant side effects (mucositis, dry mouth, taste changes, bone damage); long daily sessions. | $20,000 - $50,000+ (per course) | Weeks to months for side effects to resolve. |
| Chemotherapy | Advanced stages; adjuvant to radiation/surgery; metastatic disease. | Systemic action; enhances radiation; effective against widespread cancer. | Significant systemic side effects (nausea, fatigue, hair loss, immune suppression). | $10,000 - $200,000+ (per course/multiple cycles) | Days to weeks after each cycle. |
| Targeted Therapy | Recurrent/metastatic cancer; specific genetic markers. | More targeted action; potentially fewer systemic side effects than chemo. | Only effective for specific cancer types/mutations; can be expensive; still has side effects. | $10,000 - $20,000+ (per month) | Varies, usually less severe than chemo/rad. |
| Immunotherapy | Recurrent/metastatic cancer; specific immune markers. | Harnesses body's immune system; long-lasting responses possible. | Not effective for all; unique immune-related side effects; very high cost. | $10,000 - $30,000+ (per infusion/month) | Varies, can be well-tolerated or have severe immune reactions. |
The Treatment Journey: A Step-by-Step Process
Undergoing oral cancer treatment is a complex journey that typically follows a structured path.
1. Diagnosis and Staging
After initial symptoms prompt a dental visit, diagnosis involves a biopsy. If cancer is confirmed, further imaging tests (CT, MRI, PET) are performed to determine the cancer's stage (TNM staging system: Tumor size, Nodal involvement, Metastasis). This critical step guides treatment planning.
2. Treatment Planning
A multidisciplinary team convenes to discuss the best course of action. This team typically includes an oral and maxillofacial surgeon, head and neck surgeon, radiation oncologist, medical oncologist, pathologist, radiologist, reconstructive surgeon, and supportive care professionals (e.g., speech therapist, nutritionist, social worker). They weigh the risks and benefits of each treatment option, considering the cancer's characteristics and the patient's overall health and preferences.
3. Treatment Execution
- Surgery: If surgery is chosen, it is usually performed first. This could involve removing the tumor and possibly affected lymph nodes. Depending on the extent, immediate reconstructive surgery might follow.
- Adjuvant Therapy: After surgery, pathology reports are reviewed. If cancer cells are found at the margins or in lymph nodes, or if the tumor was large, radiation therapy (with or without chemotherapy) may be recommended to destroy any remaining cancer cells. This usually starts a few weeks after surgery to allow for initial healing.
- Primary Radiation/Chemoradiation: For certain stages or in cases where surgery is not ideal, a combination of radiation and chemotherapy might be the primary treatment. This typically involves daily radiation sessions for several weeks, with chemotherapy administered periodically.
4. Recovery and Rehabilitation
This phase begins immediately after active treatment concludes and can be extensive. It focuses on managing side effects, restoring function, and improving quality of life. (Detailed in the "Recovery and Aftercare" section below).
5. Follow-up and Surveillance
Regular follow-up appointments are crucial to monitor for recurrence and manage long-term side effects. Initially, these might be every 1-3 months, gradually decreasing in frequency over several years. Surveillance includes clinical exams, imaging, and sometimes blood tests.
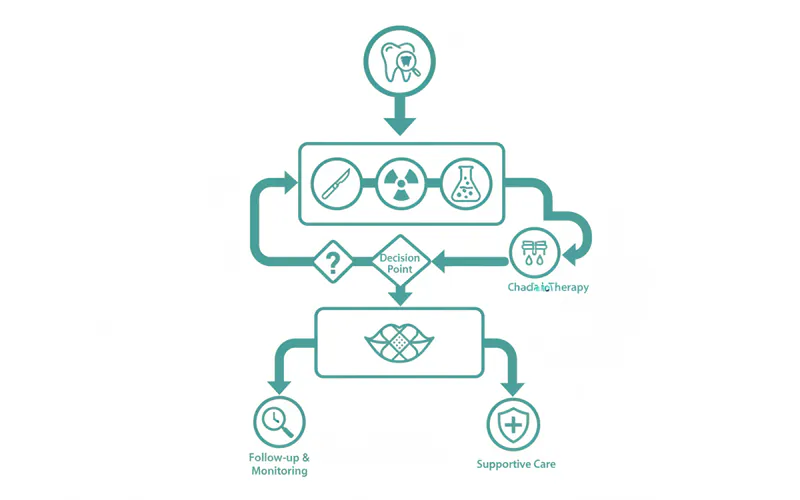 This image should be a clear, easy-to-follow infographic showing the patient's journey: "Symptoms -> Dental/Medical Exam -> Biopsy -> Diagnosis & Staging -> Multidisciplinary Treatment Planning -> Treatment (Surgery / Radiation / Chemotherapy / Combo) -> Recovery & Rehabilitation -> Long-term Follow-up."
This image should be a clear, easy-to-follow infographic showing the patient's journey: "Symptoms -> Dental/Medical Exam -> Biopsy -> Diagnosis & Staging -> Multidisciplinary Treatment Planning -> Treatment (Surgery / Radiation / Chemotherapy / Combo) -> Recovery & Rehabilitation -> Long-term Follow-up."
Cost and Insurance Considerations for Oral Cancer Treatment
The cost of oral cancer treatment in the US is substantial and can be a significant financial burden. These costs vary widely based on the stage of cancer, the specific treatments received, the duration of therapy, the facility (academic vs. community hospital), geographic location, and whether complications arise.
Estimated Cost Ranges (Without Insurance):
- Diagnosis (Biopsy, Imaging): $1,000 - $15,000
- Biopsy: $500 - $2,000
- CT/MRI Scans: $1,000 - $7,000 per scan
- PET Scan: $3,000 - $10,000 per scan
- Surgery: $10,000 - $100,000+
- Basic tumor excision: $10,000 - $30,000
- Complex resections (e.g., glossectomy, mandibulectomy, neck dissection): $30,000 - $100,000+
- Microvascular free flap reconstruction: $50,000 - $150,000+ (often performed simultaneously with tumor removal)
- Radiation Therapy: $20,000 - $50,000+ per course
- Includes treatment planning, daily sessions for 5-7 weeks, and follow-up.
- Chemotherapy: $10,000 - $200,000+ per course/cycles
- Depends on the drugs used, number of cycles, and administration method.
- Targeted/Immunotherapy: $10,000 - $30,000+ per month/infusion
- These newer therapies can be exceptionally expensive.
- Supportive Care (Rehabilitation): $5,000 - $50,000+
- Speech therapy, physical therapy, nutrition counseling, dental prosthetics, psychological support.
Insurance Coverage:
Most major medical insurance plans (HMO, PPO, EPO) and government programs like Medicare and Medicaid will cover a significant portion of oral cancer treatment, as it is considered medically necessary. However, patients will still be responsible for:
- Deductibles: The amount you must pay out-of-pocket before your insurance starts to cover costs (can range from hundreds to several thousands of dollars).
- Co-payments: Fixed amounts you pay for doctor visits, prescriptions, or treatments.
- Co-insurance: A percentage of the cost of treatment that you are responsible for after your deductible is met (e.g., 20%).
- Out-of-Pocket Maximums: The maximum amount you will have to pay for covered services in a plan year. Once this limit is reached, your insurance plan pays 100% of the cost of covered benefits. This can still be several thousand to tens of thousands of dollars.
Pro Tip: Always understand your specific insurance plan's coverage, deductibles, co-pays, and out-of-pocket maximums before treatment begins. Work closely with your hospital's financial counseling department. They can help navigate insurance claims, identify potential financial aid programs, and discuss payment plan options.
Payment Plans and Financing Options:
- Hospital Payment Plans: Many hospitals offer interest-free payment plans to help manage large bills.
- Medical Credit Cards: Options like CareCredit allow you to finance medical expenses, often with deferred-interest periods.
- Patient Assistance Programs: Numerous non-profit organizations (e.g., Oral Cancer Foundation, CancerCare, American Cancer Society) offer financial assistance, grants, or resources to help patients with treatment costs, travel, and lodging.
- Government Programs: Beyond Medicare/Medicaid, state-specific programs may offer additional assistance.

Recovery and Aftercare Post-Oral Cancer Treatment
Recovery from oral cancer treatment can be a long and challenging journey, often requiring extensive rehabilitation to restore function and improve quality of life.
1. Pain Management
Post-surgical pain is common and managed with prescription pain medications, which are gradually tapered off. Neuropathic pain (nerve pain) can also occur, requiring specific medications.
2. Nutritional Support
- Swallowing Difficulties: Surgery and radiation can severely impact swallowing (dysphagia). Patients may require a feeding tube (nasogastric or gastrostomy tube) for weeks or months to ensure adequate nutrition and hydration.
- Dietary Modifications: A soft, pureed, or liquid diet may be necessary. Nutritionists play a crucial role in creating a balanced dietary plan to promote healing and maintain weight.
- Xerostomia (Dry Mouth): Radiation often damages salivary glands, leading to chronic dry mouth, which can affect eating, speaking, and dental health. Management includes artificial saliva, humidifiers, and specific medications.
3. Speech and Swallowing Therapy
Speech-language pathologists are essential members of the recovery team. They help patients:
- Regain speech clarity.
- Improve swallowing function through exercises and techniques.
- Manage issues like aspiration (food or liquid entering the airway).
4. Physical Therapy
For patients with neck dissection or extensive surgery, physical therapy may be needed to improve neck and shoulder mobility and reduce stiffness.
5. Dental Rehabilitation
- Oral Hygiene: Meticulous oral hygiene is critical to prevent infections and manage dry mouth. Special toothpastes, rinses, and frequent dental check-ups are required.
- Prosthetics: If parts of the jaw, palate, or teeth were removed, dental prosthetics (e.g., obturators, dentures, dental implants) may be needed to restore chewing function and aesthetics.
- Osteoradionecrosis: A severe complication of radiation is bone death (osteoradionecrosis) of the jaw, which can be difficult to treat and may require hyperbaric oxygen therapy or further surgery.
6. Psychological and Emotional Support
Coping with cancer diagnosis, treatment side effects, and changes in appearance or function can be emotionally taxing. Support groups, counseling, and psychological services are invaluable resources.
7. Long-Term Follow-up and Surveillance
Regular follow-up with the oncology team is paramount for years after treatment. This includes physical exams and imaging to monitor for cancer recurrence, which is highest in the first 2-3 years. Patients are also at increased risk for developing secondary primary cancers, particularly if they continue to use tobacco or alcohol.
Prevention: Reducing Your Risk of Mouth Cancer
Many cases of oral cancer are preventable by addressing key risk factors.
1. Avoid Tobacco in All Forms
This is the most impactful step you can take. Quitting smoking and smokeless tobacco significantly reduces your risk over time. The longer you abstain, the lower your risk becomes, eventually approaching that of someone who has never used tobacco.
2. Moderate Alcohol Consumption
Limit alcohol intake. If you drink, do so in moderation (up to one drink per day for women, up to two for men). Avoiding the combination of tobacco and alcohol is especially crucial due to their synergistic effect.
3. HPV Vaccination
The HPV vaccine (Gardasil 9) is highly effective in preventing infections with high-risk HPV strains, including HPV-16, which is linked to oropharyngeal cancer. It is recommended for adolescents (ages 11-12) but can be administered up to age 45.
4. Protect Your Lips from Sun Exposure
Use lip balm with SPF 15 or higher, and wear a wide-brimmed hat when spending time outdoors to protect your lips from harmful UV rays.
5. Maintain a Healthy Diet
Consume a diet rich in fruits, vegetables, and whole grains. These foods contain antioxidants that can protect cells from damage and may reduce cancer risk.
6. Regular Dental Check-ups and Oral Cancer Screenings
Visit your dentist regularly, ideally every six months, for comprehensive oral exams. Your dentist is often the first healthcare provider to identify suspicious lesions during routine screenings. The ADA emphasizes the importance of these screenings for early detection.
Pro Tip: Be proactive about your oral health. Beyond regular dental visits, learn to perform a simple self-examination of your mouth monthly. Look for any changes in color, texture, or persistent sores. If you find anything suspicious that doesn't resolve within two weeks, schedule an appointment with your dentist or an oral surgeon promptly.
Risks and Complications of Oral Cancer and Its Treatment
Oral cancer and its treatments carry various risks and potential complications that patients should be aware of.
Risks of the Disease Itself:
- Metastasis: The most significant risk is the spread of cancer to other parts of the body, primarily to regional lymph nodes in the neck, and then potentially to distant sites like the lungs, liver, or bone.
- Recurrence: Even after successful treatment, there is always a risk that the cancer may return, either in the original location (local recurrence) or in a nearby area (regional recurrence).
- Secondary Primary Cancers: Patients who have had one oral cancer are at an increased risk of developing another primary cancer in the head and neck region, esophagus, or lungs, particularly if they continue to engage in high-risk behaviors like smoking and drinking.
- Functional Impairment: Even before treatment, large tumors can interfere with speech, swallowing, and breathing.
- Pain and Discomfort: As the cancer progresses, it can cause significant pain, nerve involvement, and difficulty with daily functions.
Complications of Treatment:
Surgery:
- Bleeding and Infection: Standard surgical risks.
- Nerve Damage: Can lead to numbness, facial weakness, or difficulty with tongue movement.
- Speech and Swallowing Impairment: Depending on the extent of tissue removal, particularly of the tongue, jaw, or throat.
- Disfigurement: Especially for extensive resections requiring reconstructive surgery.
- Fistula Formation: An abnormal connection between internal organs or to the outside of the body.
Radiation Therapy:
- Mucositis: Painful inflammation and ulceration of the mouth lining, often severe.
- Xerostomia (Dry Mouth): Permanent damage to salivary glands, leading to chronic dry mouth, difficulty eating, and increased risk of dental decay.
- Dysphagia: Difficulty and pain with swallowing, often long-lasting.
- Taste Changes: Loss or alteration of taste.
- Skin Reactions: Redness, peeling, and blistering of the skin in the treated area.
- Osteoradionecrosis (ORN): A severe complication where bone tissue in the irradiated area (often the jaw) dies due to impaired blood supply, leading to chronic pain, infection, and potential need for surgery. This risk is exacerbated by dental extractions after radiation.
- Trismus: Stiffness and limited opening of the jaw due to scarring and fibrosis of muscles.
- Dental Issues: Increased risk of cavities and gum disease.
Chemotherapy:
- Nausea and Vomiting: Common side effects.
- Fatigue: Extreme tiredness.
- Hair Loss: Varies by drug.
- Bone Marrow Suppression: Leading to increased risk of infection (low white blood cells), anemia (low red blood cells), and bruising/bleeding (low platelets).
- Peripheral Neuropathy: Numbness, tingling, or pain in hands and feet.
- Mucositis: Can exacerbate radiation-induced mucositis.
Understanding Mouth Cancer in Dogs
While this article primarily focuses on human oral cancer, the target keyword "mouth cancer in dogs" warrants a brief mention. It's crucial to understand that canine oral cancers are distinct from human cancers in terms of specific types, prevalence, and treatment protocols, and should always be diagnosed and managed by a veterinarian.
In dogs, oral tumors are relatively common, accounting for about 6% of all canine cancers. Common types include:
- Malignant Melanoma: The most common oral cancer in dogs, often aggressive and prone to metastasis.
- Squamous Cell Carcinoma (SCC): Similar to humans, but different genetic factors and environmental triggers.
- Fibrosarcoma: Another aggressive tumor of the connective tissues.
- Epulides: Benign gum growths, but some can be locally invasive.
Signs of Oral Cancer in Dogs:
- Bad breath (halitosis).
- Difficulty eating, dropping food.
- Excessive drooling, sometimes bloody.
- Swelling or lumps on the gums, tongue, lips, or jaw.
- Loose teeth.
- Bleeding from the mouth.
- Facial swelling.
If you notice any of these signs in your pet, it's essential to seek veterinary attention immediately. Diagnosis involves a thorough oral exam, biopsy, and imaging. Treatment often includes surgery, radiation, and sometimes chemotherapy, similar in principle but tailored to veterinary medicine.
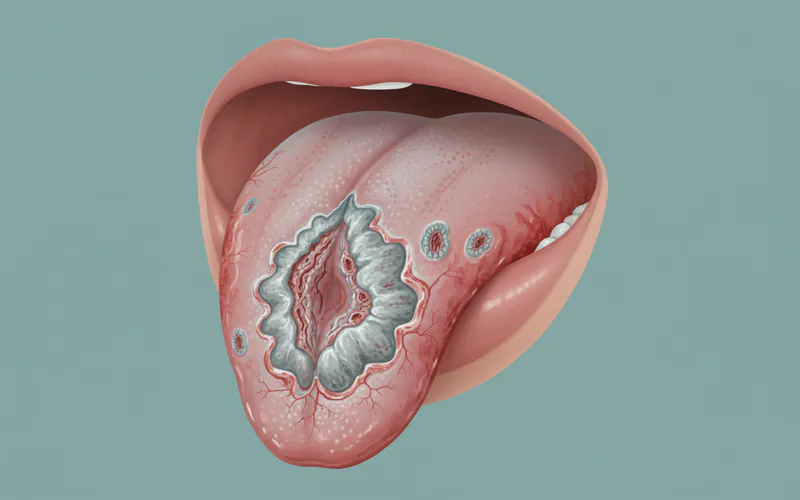 This image should depict a more advanced stage of human oral cancer, showing a clearly ulcerated, irregular, and possibly fungating mass on the tongue or inner cheek, with visible surrounding inflammation or color changes, to illustrate what might be seen if diagnosis is delayed.
This image should depict a more advanced stage of human oral cancer, showing a clearly ulcerated, irregular, and possibly fungating mass on the tongue or inner cheek, with visible surrounding inflammation or color changes, to illustrate what might be seen if diagnosis is delayed.
Pediatric Considerations: Oral Cancer in Children
Oral cancer is exceedingly rare in children. When it does occur, it is often associated with specific genetic syndromes, immunodeficiency, or systemic conditions rather than the typical risk factors seen in adults (tobacco, alcohol, HPV).
Types of oral malignancies in children can include:
- Rhabdomyosarcoma: A type of soft tissue sarcoma.
- Lymphoma: Often non-Hodgkin lymphoma affecting the head and neck.
- Squamous Cell Carcinoma: Extremely rare but can occur.
Symptoms in children can be vague and easily missed or attributed to more common childhood ailments like infections or injuries. Parents should be vigilant for:
- Persistent lumps or swellings in the mouth or neck.
- Non-healing sores.
- Unexplained bleeding.
- Difficulty eating, swallowing, or speaking that is not improving.
If a child presents with persistent, unexplained oral symptoms, especially if accompanied by other systemic signs (e.g., fever, weight loss, night sweats), prompt medical evaluation by a pediatrician or pediatric oncologist is crucial. Early diagnosis is just as important in children, even though the specific risk factors and treatment approaches may differ from adults.
Cost Breakdown for Oral Cancer Care in the US
Navigating the financial aspects of oral cancer care can be daunting. Here's a consolidated overview of average US costs, with and without insurance, and tips for managing expenses.
Average US Costs for Key Components (Estimates, without insurance):
- Initial Diagnosis & Staging (Consults, Biopsy, Scans): $5,000 - $20,000
- This covers specialist consultations, the biopsy procedure itself, pathology analysis, and essential imaging like CT, MRI, and PET scans.
- Primary Surgery: $20,000 - $150,000+
- This range accounts for simple excisions to complex resections involving multiple structures (jaw, tongue, neck dissection) and immediate microvascular reconstruction. Hospital stay, surgeon fees, anesthesiology, and operating room charges are included.
- Radiation Therapy Course: $30,000 - $60,000+
- A full course typically involves daily treatments for 5-7 weeks. Costs cover treatment planning, simulation, daily fractions, and follow-up radiation oncology visits.
- Chemotherapy Course: $20,000 - $250,000+
- Highly variable based on the specific drugs, number of cycles (often 3-6 cycles), and administration (IV vs. oral). Newer targeted and immunotherapies can push these costs significantly higher.
- Rehabilitation & Supportive Care (Post-Treatment): $10,000 - $75,000+
- This can include extensive speech therapy, physical therapy, nutritional counseling, dental prosthetics, psychological support, and ongoing medication for side effects like dry mouth.
- Long-term Follow-up & Surveillance: $1,000 - $5,000 per year (for first 5 years)
- Includes regular clinical exams, imaging scans (e.g., CT/PET annually), and blood tests to monitor for recurrence.
Total Estimated Cost for a Full Treatment Course (without insurance): $50,000 to over $500,000 for advanced cases requiring multi-modal therapy and extensive reconstruction.
With vs. Without Insurance:
- Without Insurance: The patient is responsible for 100% of the above costs, which are often charged at higher "list" prices by healthcare providers.
- With Insurance: While insurance covers a significant portion, patients are still responsible for:
- Deductibles: Often $1,000 - $10,000 annually.
- Co-insurance: Typically 10-30% of covered services after the deductible is met.
- Co-payments: Fixed fees for doctor visits or prescriptions ($20 - $100).
- Out-of-Pocket Maximum: While this caps your annual spending (e.g., $5,000 - $15,000 for individuals, more for families), it is a substantial amount.
Example Scenario (PPO plan with $5,000 deductible, 20% co-insurance, $10,000 out-of-pocket maximum): For a $100,000 treatment bill, you would pay your $5,000 deductible, then 20% of the remaining $95,000 ($19,000), until your $10,000 out-of-pocket maximum is reached. In this case, you would pay the $5,000 deductible + $5,000 of co-insurance, totaling $10,000 for the year, with the insurance covering the rest. However, if the treatment spans two calendar years, you might hit your out-of-pocket maximum twice.
Payment Plans and Financing Options:
- Hospital Financial Assistance: Hospitals often have programs to help uninsured or underinsured patients. Social workers or financial counselors can guide you.
- Medical Credit Cards: Companies like CareCredit offer special financing for healthcare expenses, sometimes with promotional interest-free periods.
- Patient Advocacy Organizations: Groups like the Oral Cancer Foundation, CancerCare, and the American Cancer Society offer direct financial aid, grants for specific expenses (travel, lodging, medication), or navigation services to find resources.
- State & Federal Programs: Medicaid (for low-income individuals), Medicare (for those 65+ or with certain disabilities), and state-specific cancer programs can provide coverage.
Cost-Saving Tips:
- Early Detection: The single most effective cost-saving measure. Treating early-stage cancer is significantly less expensive than advanced-stage cancer with metastasis.
- Understand Your Insurance: Thoroughly review your policy, understand what's covered, and know your out-of-pocket responsibilities.
- Seek In-Network Providers: Using doctors and facilities within your insurance network will always result in lower costs.
- Negotiate Bills: For uninsured patients or for charges not covered by insurance, you may be able to negotiate a lower cash price with providers.
- Generic Medications: Opt for generic versions of prescription drugs whenever possible.
- Leverage Patient Resources: Don't hesitate to reach out to social workers, patient navigators, and non-profit organizations for help.
[TABLE: Estimated Cost Ranges for Oral Cancer Treatment Components (USA)]
| Component | Low Range (USD) | Mid Range (USD) | High Range (USD) | Notes |
|---|---|---|---|---|
| Initial Consults | $200 | $500 | $1,000 | Specialist visits (oral surgeon, ENT, oncologist). |
| Biopsy (procedure) | $500 | $1,500 | $3,000 | Includes local anesthesia, tissue removal, and lab pathology. |
| CT/MRI Scan | $1,000 | $3,000 | $7,000 | Per scan, varies by facility and whether contrast is used. |
| PET Scan | $3,000 | $6,000 | $10,000 | Often combined with CT. |
| Simple Tumor Excision | $10,000 | $25,000 | $40,000 | Early stage, localized, no complex reconstruction. |
| Complex Resection | $40,000 | $80,000 | $150,000+ | Mandibulectomy, glossectomy, neck dissection, immediate microvascular reconstruction. |
| Radiation Therapy | $30,000 | $45,000 | $60,000+ | Full course (5-7 weeks), includes planning and delivery. |
| Chemotherapy (per cycle) | $5,000 | $15,000 | $50,000+ | Highly variable by drug type; multiple cycles common. |
| Targeted/Immunotherapy (per month) | $10,000 | $20,000 | $40,000+ | Newer drugs, very high monthly cost. |
| Speech/Swallow Therapy (per session) | $100 | $250 | $500 | Many sessions over months/years may be needed. |
| Dental Prosthetics | $5,000 | $15,000 | $50,000+ | Obturators, dental implants, complex dentures (reconstruction). |
Frequently Asked Questions
H3: Is mouth cancer painful?
Early-stage mouth cancer is often painless, which is why it can go undetected. As it progresses, it can cause persistent pain, numbness, burning sensations, or referred pain to the ear. Any persistent oral pain, especially if accompanied by other suspicious signs, should be evaluated by a dentist.
H3: How long does oral cancer treatment take?
The duration varies significantly. Surgery can be a single event, followed by weeks or months of recovery. Radiation therapy typically lasts 5-7 weeks, daily. Chemotherapy cycles can span several months. Overall, the active treatment phase can range from a few weeks to 6-8 months, followed by extensive rehabilitation that can last for years.
H3: What are the survival rates for mouth cancer?
The 5-year survival rate for localized oral and oropharyngeal cancer (cancer that has not spread) is 84%. If it has spread to regional lymph nodes, the rate drops to 67%. If it has spread to distant parts of the body, the survival rate is 40%. Early detection is key to improving these statistics.
H3: Can mouth cancer be cured?
Yes, mouth cancer can be cured, especially when detected and treated early. For localized disease, the cure rate is high with appropriate treatment. However, late-stage cancers are much more challenging to treat and have lower cure rates.
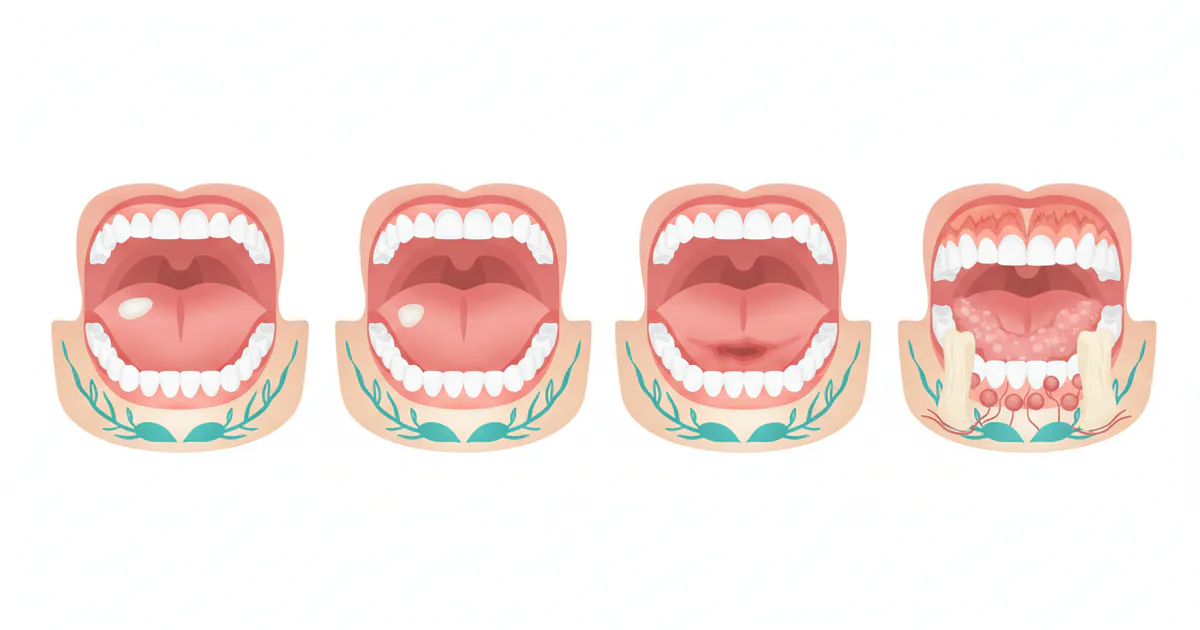
H3: What does early mouth cancer look like?
Early mouth cancer can appear as a persistent white patch (leukoplakia), a red velvety patch (erythroplakia), a non-healing sore or ulcer, or a small, firm lump or thickening. These lesions are often painless in their initial stages. Crucially, any such change lasting more than two weeks should be examined by a dental professional.
H3: Are mouth cancer photos graphic?
Yes, advanced mouth cancer photos can be quite graphic and disturbing, depicting significant tissue destruction, disfigurement, and large lesions. However, images of early signs, like those found in educational resources, are typically presented to highlight subtle changes for identification without being overly graphic. The purpose of these images is to educate on early detection.
H3: How often should I get screened for oral cancer?
The American Dental Association (ADA) recommends that a comprehensive oral cancer screening be part of your routine dental check-up, typically every 6 to 12 months. Individuals with higher risk factors (tobacco/alcohol use, HPV history, previous oral cancer) may benefit from more frequent screenings.
H3: What are the alternatives to traditional oral cancer surgery?
For early-stage cancers, surgery is often the gold standard. However, alternatives or adjuncts include radiation therapy (sometimes as a primary treatment), chemotherapy (usually combined with radiation for more advanced cases), targeted therapy, and immunotherapy. The best approach depends on the specific cancer characteristics and patient factors.
H3: Does HPV cause all mouth cancers?
No, HPV (Human Papillomavirus) does not cause all mouth cancers. While HPV-16 is a leading cause of oropharyngeal cancers (those in the back of the throat, tonsils, and base of the tongue), most oral cavity cancers (lips, front of tongue, gums, floor of mouth) are still primarily linked to tobacco and alcohol use.
H3: Can dentists detect mouth cancer?
Yes, dentists are often the first healthcare providers to detect oral cancer. They are trained to perform thorough oral cancer screenings during routine dental exams, looking for suspicious lesions and abnormalities. If something concerning is found, they will refer you to a specialist for further evaluation and biopsy.
When to See a Dentist
Recognizing when to seek professional dental or medical attention for oral health concerns is crucial for early detection and successful outcomes.
See a dentist immediately (within a few days) if you experience any of the following "red flag" symptoms:
- Any sore, ulcer, or patch (white, red, or mixed) in your mouth or on your lip that does not heal or go away within two weeks. This is the most critical warning sign.
- A persistent lump, thickening, or swelling in your mouth, throat, or neck.
- Unexplained bleeding from your mouth.
- Chronic sore throat, hoarseness, or feeling of something caught in your throat that persists for more than two weeks and isn't linked to a cold or flu.
- Difficulty or pain when chewing, swallowing, or moving your tongue or jaw.
- Numbness or persistent pain in any area of your face, mouth, or neck without an obvious cause.
- Loose teeth or dentures that no longer fit well without a clear dental reason.
- A persistent one-sided earache when there are no signs of ear infection.
Routine Care Guidance: Even without specific symptoms, schedule regular dental check-ups, typically every six months. These appointments include an oral cancer screening as part of a comprehensive examination. Many early cancers are discovered during these routine visits before you even notice any symptoms.
Emergency vs. Scheduled Appointment: While some of the "red flag" symptoms warrant immediate attention, they usually do not constitute a dental emergency requiring an emergency room visit unless accompanied by severe, uncontrolled bleeding, sudden inability to breathe or swallow, or extreme, debilitating pain. For most suspicious oral lesions, contacting your regular dentist or an oral surgeon promptly for a scheduled diagnostic appointment is the appropriate first step. Do not delay, as early detection is vital for the best prognosis.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Floor of Mouth Cancer: Complete Guide
Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral c
February 23, 2026
Oral Cancer Stages Pictures: Complete Guide
Oral cancer, a serious and potentially life-threatening disease, affects thousands of Americans each year. According to the American Cancer Society, approximately 54,000 new cases of oral cavity or oropharyngeal cancer are diagnosed annually in the United States. While these numbers can be daunt
February 23, 2026
Can You Die From Mouth Cancer
Oral cancer is a formidable disease, often striking with insidious subtlety before revealing its devastating potential. It's a question that weighs heavily on the minds of those who receive a diagnosis or even those simply concerned about unusual oral symptoms: can you die from mouth cancer? The
February 23, 2026
Mouth Cancer Pictures Early Stages: Complete Guide
Few diagnoses can be as unsettling as cancer, and when it affects a part of your body as central to daily life as your mouth, the concern is profound. Oral cancer, often referred to simply as mouth cancer, is a serious condition that, if detected early, has a significantly higher chance of s
February 23, 2026