Floor of Mouth Cancer: Complete Guide

Key Takeaways
- Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral c
Floor of Mouth Cancer: Complete Guide
Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral cavity malignancies. The floor of the mouth, the horseshoe-shaped area beneath the tongue, is a critical region due to its rich blood supply, lymphatic drainage, and proximity to vital structures involved in speech, swallowing, and chewing. Understanding this specific type of cancer – its causes, symptoms, and the crucial role of early stage oral cancer detection – is paramount for effective treatment and improved outcomes. This comprehensive guide will equip you with vital information, from prevention strategies like how to prevent oral cancer, to navigating the complexities of diagnosis, treatment, and recovery, ensuring you are empowered to protect your oral health.

Key Takeaways:
- Floor of mouth cancer is a common and aggressive oral cancer, primarily squamous cell carcinoma, with a strong link to tobacco and alcohol use.
- Early detection is crucial: Look for persistent red or white patches, non-healing sores, lumps, or pain under the tongue. Regular dental check-ups, typically every 6 months, are vital for screening.
- Treatment often involves a multidisciplinary approach: Combining surgery (ranging from $5,000 to over $50,000), radiation therapy (typically $30,000-$50,000), and sometimes chemotherapy ($10,000-$30,000 per cycle).
- Prevention is key: Quitting tobacco and excessive alcohol, maintaining a healthy diet, and considering the HPV vaccine (especially for adolescents and young adults) significantly reduce risk.
- Recovery can be extensive: Involving speech, swallowing, and physical therapy, potentially for months to years, with costs varying widely based on individual needs and insurance.
- Insurance coverage: Most treatments are covered by medical insurance, but out-of-pocket costs can range from hundreds to thousands of dollars depending on deductibles, co-pays, and plan specifics.
What It Is / Overview
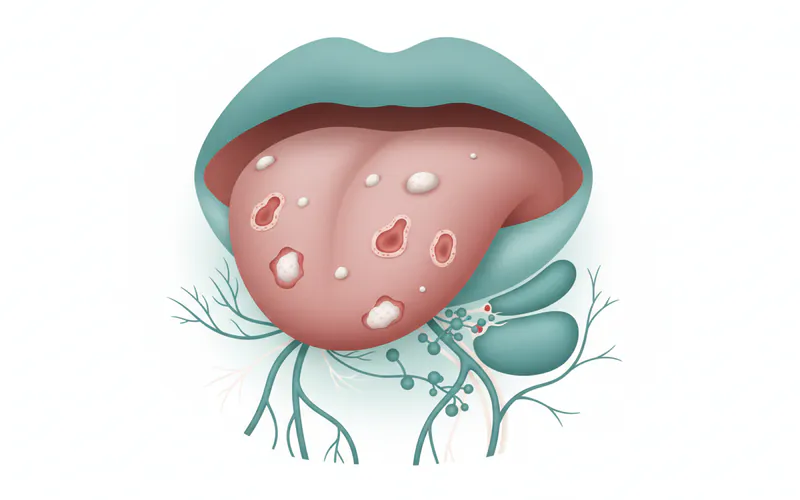
Floor of mouth cancer refers to a malignant growth that originates in the tissues lining the floor of the mouth. This area is located directly beneath the tongue, extending from the inner surface of the lower jawbone (mandible) to the undersurface of the tongue. It's a highly sensitive and vascularized region, housing salivary glands (sublingual and submandibular glands), numerous blood vessels, and nerves essential for sensation, movement, and taste.
The vast majority of floor of mouth cancers, about 90-95%, are a type of cancer known as squamous cell carcinoma (SCC). Squamous cells are the flat, thin cells that line the surface of the mouth, throat, and other organs. When these cells begin to grow abnormally and uncontrollably, they can form a malignant tumor. These cancers often begin as precancerous lesions, which are changes in the tissue that are not yet cancerous but have the potential to become so over time. These lesions might appear as white patches (leukoplakia) or red patches (erythroplakia), which are significant warning signs.
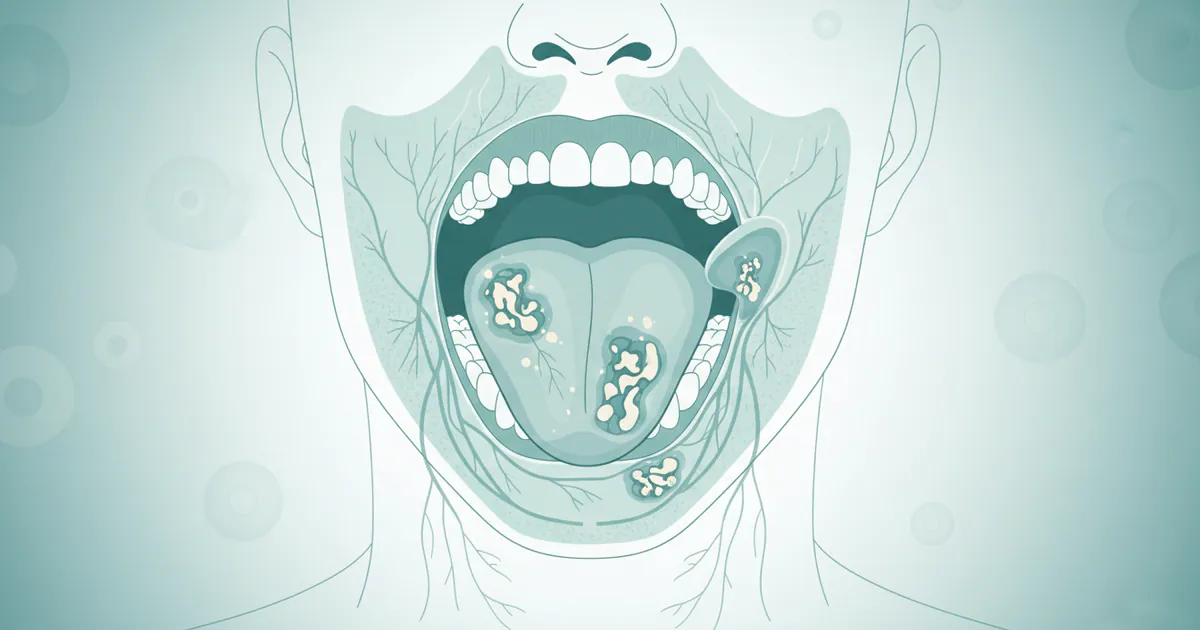
Due to the floor of the mouth's rich lymphatic network, these cancers have a tendency to spread to nearby lymph nodes in the neck relatively early in their development. This characteristic makes early detection and prompt treatment particularly vital. The proximity to the jawbone, major blood vessels, and nerves also means that advanced floor of mouth cancers can invade these structures, making treatment more complex and potentially impacting critical functions like chewing, swallowing, and speaking.
Pro Tip: Regular self-exams, including lifting your tongue to inspect the floor of your mouth, can help you identify suspicious changes early. Always report any persistent anomalies to your dentist.
Types / Variations
While squamous cell carcinoma (SCC) accounts for the overwhelming majority of floor of mouth cancers, there are a few other, much rarer types that can occur:
- Squamous Cell Carcinoma (SCC): This is by far the most prevalent type. SCCs in the floor of the mouth often present as non-healing ulcers, red or white patches (erythroleukoplakia), or firm, irregular masses. They can grow quickly and have a high propensity for regional metastasis (spread to nearby lymph nodes).
- Verrucous Carcinoma: A less aggressive variant of SCC, verrucous carcinoma grows slowly and rarely spreads to distant sites. It typically appears as a warty, cauliflower-like growth. While it's still a form of SCC, its distinct growth pattern and lower metastatic potential often lead to different treatment considerations, often primarily surgical.
- Minor Salivary Gland Cancers: The floor of the mouth contains numerous minor salivary glands. Cancers can originate from these glands, though they are rare. Examples include mucoepidermoid carcinoma and adenoid cystic carcinoma. These types of cancers behave differently than SCC, often growing more slowly but potentially being more prone to nerve invasion.
- Sarcomas: Extremely rare, sarcomas arise from the connective tissues (like muscle or bone) rather than the epithelial lining.
- Lymphomas: While lymphomas can affect the oral cavity, they are exceedingly rare on the floor of the mouth itself and are typically a manifestation of systemic disease rather than a primary oral lesion.
For the purpose of this guide, the focus will primarily remain on squamous cell carcinoma due to its prevalence and the vast majority of information pertaining to floor of mouth cancer referring to this specific type.
Causes / Why It Happens
The development of floor of mouth cancer, like most oral cancers, is multifactorial, meaning several risk factors can contribute to its onset. However, certain factors are overwhelmingly implicated:
- Tobacco Use: This is the single most significant risk factor. All forms of tobacco, including cigarettes, cigars, pipes, and smokeless tobacco (chewing tobacco, snuff), contain carcinogens (cancer-causing chemicals) that directly irritate and damage the cells lining the mouth. The risk increases with the duration and intensity of tobacco use. For instance, a long-term heavy smoker may have a risk 10-20 times higher than a non-smoker.
- Alcohol Consumption: Excessive and prolonged alcohol use is another major risk factor. Alcohol itself can act as an irritant and also enhance the ability of other carcinogens (like those in tobacco) to penetrate oral tissues. The combination of heavy smoking and heavy drinking creates a synergistic effect, exponentially increasing the risk – sometimes by as much as 30 times compared to those who neither smoke nor drink.
- Human Papillomavirus (HPV) Infection: While HPV is a well-known cause of oropharyngeal cancers (cancers of the tonsils and base of the tongue), its direct role in floor of mouth cancer is less pronounced but still a contributing factor in some cases, particularly HPV-16. This virus can alter cells, leading to uncontrolled growth.
- Sun Exposure (for lip cancer, less so for floor of mouth): While UV radiation is a primary cause of lip cancer, it is not a direct cause for cancers on the floor of the mouth, which is an internal site.
- Poor Nutrition: A diet consistently low in fruits and vegetables, which are rich in antioxidants, may weaken the body's natural defenses against cell damage and cancer development. Specific vitamin deficiencies, such as Vitamin A and B, have been linked to increased risk.
- Chronic Irritation: While less definitively proven than tobacco and alcohol, persistent irritation from poorly fitting dentures, sharp broken teeth, or chronic viral infections might contribute to cellular changes over time. However, this is typically seen as a co-factor rather than a primary cause.
- Weakened Immune System: Individuals with compromised immune systems (e.g., organ transplant recipients on immunosuppressive drugs, people with HIV/AIDS) have a higher risk of developing various cancers, including oral cancers.
- Genetics: While not a direct cause, a family history of oral or other head and neck cancers might indicate a genetic predisposition, though environmental factors often play a larger role.
- Age: The risk of developing floor of mouth cancer increases with age, with most diagnoses occurring in people over 50.
- Gender: Men are more likely to develop floor of mouth cancer than women, largely due to historical trends in tobacco and alcohol use.
Understanding these risk factors is the first step in how to prevent oral cancer, enabling individuals to make informed lifestyle choices.
Signs and Symptoms
Recognizing the signs and symptoms of floor of mouth cancer is critical for early stage oral cancer detection, which significantly improves prognosis. Many of these symptoms can be subtle or mimic less serious conditions, making regular dental check-ups essential.
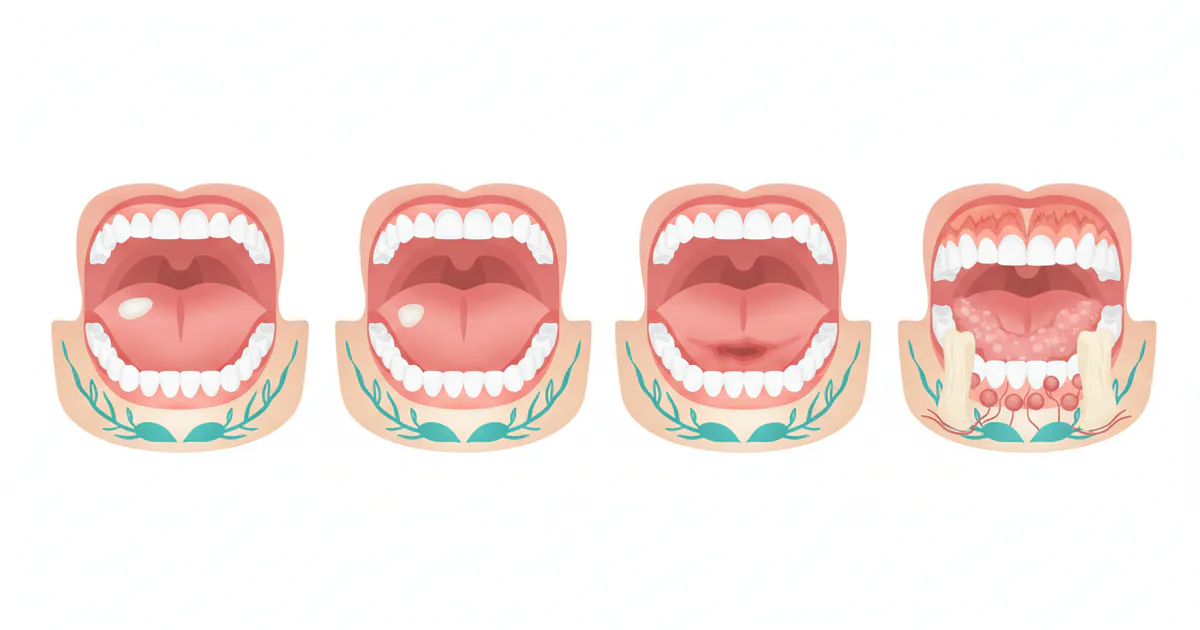
Early Stage Signs (often painless):
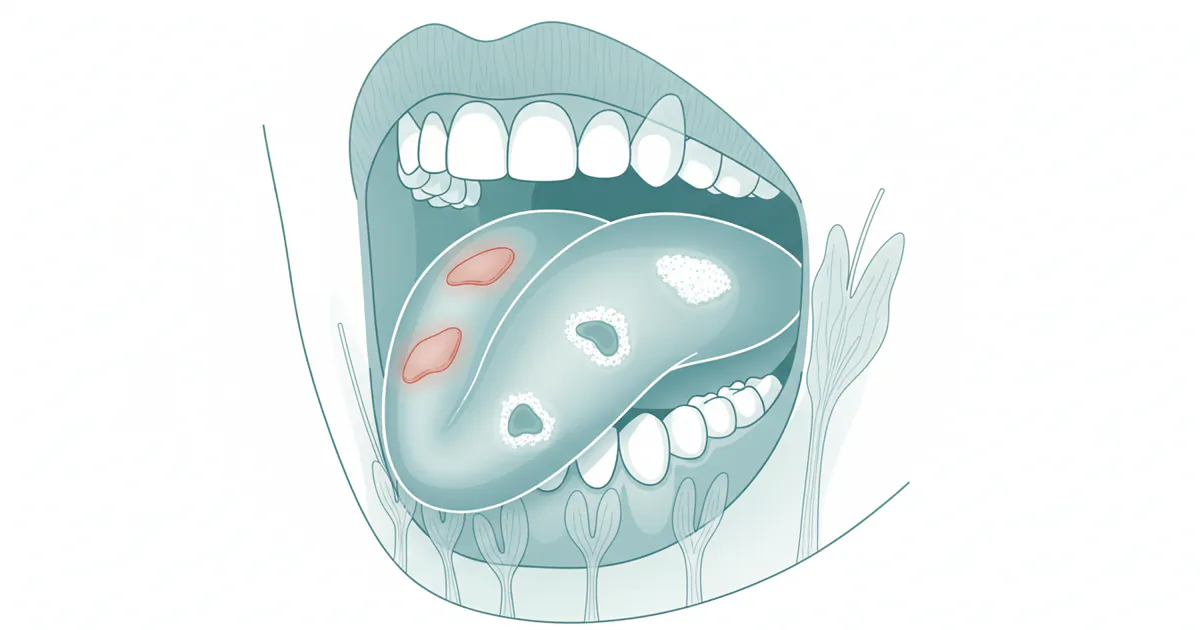
- Persistent Red or White Patches (Erythroplakia or Leukoplakia): These are often the earliest visual signs.
- Erythroplakia (red patch): A velvety red area that cannot be scraped off. These are often considered more concerning than leukoplakia and have a higher likelihood of being or becoming cancerous.
- Leukoplakia (white patch): A thick, white patch or lesion that cannot be wiped away. While many leukoplakias are benign, a significant percentage can become malignant.
- A Sore that Doesn't Heal: Any ulcer or sore on the floor of the mouth that persists for more than two weeks, even if painless, should be evaluated by a dentist or oral surgeon. This is a crucial warning sign.
- Lump or Thickening: A new, firm lump or thickened area under the tongue or on the floor of the mouth, even if small and painless.
- Unexplained Bleeding: Spontaneous bleeding from the mouth without an obvious cause, such as trauma.
Advanced Stage Signs (may indicate spread or progression):
- Persistent Mouth Pain: Pain, soreness, or tenderness that doesn't go away. This may be localized or radiate to the ear.
- Difficulty or Painful Swallowing (Dysphagia): As the tumor grows, it can interfere with the movement of the tongue and the swallowing reflex.
- Difficulty Moving the Tongue: The tumor can restrict the tongue's mobility, making it hard to speak, chew, or swallow.
- Changes in Voice (Dysphonia): While less common for the floor of the mouth, if the tumor impacts structures that affect vocal cord movement or resonance, changes can occur.
- Numbness or Tingling: A persistent numb sensation in the tongue, mouth, or lower lip (due to nerve involvement).
- Weight Loss: Unexplained weight loss can occur due to difficulty eating, pain, or the metabolic demands of cancer.
- Lump in the Neck: Swollen, firm, persistent lymph nodes in the neck can indicate that the cancer has spread from the floor of the mouth.
- Loose Teeth or Dentures that No Longer Fit: If the cancer invades the jawbone, it can cause teeth to loosen or alter the fit of dentures.
- Bad Breath (Halitosis): Persistent, unusual bad breath unrelated to oral hygiene can sometimes be a sign of infection associated with a cancerous lesion.
Pro Tip: Do not wait for pain to seek help. Many early oral cancers are painless. If you notice any of these signs persisting for more than two weeks, schedule an immediate appointment with your dentist or an oral surgeon.
Treatment Options
The treatment for floor of mouth cancer is complex and highly individualized, depending on the stage of the cancer (size, depth of invasion, presence of lymph node involvement, distant metastasis), the patient's overall health, and their preferences. A multidisciplinary team, typically including an oral surgeon, head and neck surgeon, radiation oncologist, medical oncologist, and speech-language pathologist, will collaborate to develop the best treatment plan.

Surgical Removal (Resection)
Surgery is often the primary treatment for floor of mouth cancer, particularly in early stages. The goal is to remove the tumor completely along with a margin of healthy tissue (known as clear margins) to ensure all cancer cells are eradicated.
- Partial Glossectomy/Floor of Mouth Resection: For smaller tumors, part of the tongue or the affected floor of the mouth tissue is removed.
- Mandibulectomy: If the cancer has invaded or is very close to the lower jawbone (mandible), part of the bone may need to be removed. This can be a segmental mandibulectomy (removing a section of bone) or a marginal mandibulectomy (shaving off the inner surface of the bone).
- Neck Dissection: If there is evidence or high suspicion of cancer spread to the lymph nodes in the neck, a neck dissection is performed to remove these lymph nodes. This is often done even if imaging doesn't show obvious spread, due to the high risk of microscopic metastasis.
- Reconstructive Surgery: After significant tissue removal, reconstructive surgery is often necessary to restore function (speech, swallowing) and appearance. This may involve using tissue grafts from other parts of the body (e.g., forearm, thigh) to create a new floor of the mouth or tongue.
Pros of Surgery:
- Offers the best chance for complete eradication of early-stage localized cancer.
- Can provide immediate removal of the tumor.
Cons of Surgery:
- Can lead to significant functional impairments (speech, swallowing, chewing) and cosmetic changes, especially for larger resections.
- Risk of infection, bleeding, nerve damage, and wound healing complications.
- Requires a significant recovery period.
Radiation Therapy
Radiation therapy uses high-energy X-rays or other particles to kill cancer cells or inhibit their growth. It can be used as a primary treatment for smaller tumors, after surgery to kill any remaining cancer cells (adjuvant therapy), or to relieve symptoms in advanced cancers (palliative therapy).
- External Beam Radiation Therapy (EBRT): The most common type, where radiation is delivered from a machine outside the body. Modern techniques like Intensity-Modulated Radiation Therapy (IMRT) or Stereotactic Body Radiation Therapy (SBRT) allow for more precise targeting, reducing damage to healthy tissues.
- Brachytherapy: Less common for the floor of mouth, this involves placing radioactive seeds or pellets directly into or near the tumor.
Pros of Radiation Therapy:
- Can be effective in preserving function and appearance, especially for small tumors.
- Non-invasive (EBRT).
Cons of Radiation Therapy:
- Side effects can include dry mouth (xerostomia), difficulty swallowing, mucositis (painful mouth sores), taste changes, skin irritation, and potential long-term damage to the jawbone (osteoradionecrosis).
- Treatment schedule often involves daily sessions over 5-7 weeks.
Chemotherapy
Chemotherapy uses powerful drugs to kill cancer cells throughout the body. It is rarely used as a standalone treatment for floor of mouth cancer. Instead, it is typically used in combination with radiation therapy (chemoradiation) for more advanced cancers or as part of palliative care to control widespread disease.
Pros of Chemotherapy:
- Can treat cancer cells that have spread beyond the primary tumor site.
- Enhances the effectiveness of radiation therapy (radio-sensitizer).
Cons of Chemotherapy:
- Systemic side effects like nausea, vomiting, fatigue, hair loss, mouth sores, and increased risk of infection due to lowered white blood cell count.
- Potential for severe side effects depending on the drugs used.
Targeted Therapy and Immunotherapy
These are newer treatment modalities that may be used for specific cases, often in advanced or recurrent cancers:
- Targeted Therapy: Drugs that specifically target molecules involved in cancer cell growth and survival, with fewer side effects than traditional chemotherapy. An example is Cetuximab, which targets the epidermal growth factor receptor (EGFR), often overexpressed in head and neck cancers.
- Immunotherapy: Drugs that boost the body's own immune system to recognize and destroy cancer cells. Checkpoint inhibitors (e.g., Nivolumab, Pembrolizumab) are examples used for recurrent or metastatic head and neck cancers that have not responded to other treatments.
Pros of Newer Therapies:
- Can offer options for advanced cancers or those resistant to conventional treatments.
- Potentially fewer systemic side effects than traditional chemotherapy.
Cons of Newer Therapies:
- Can be very expensive.
- May not be effective for all patients or all types of cancer.
- Can have their own unique side effect profiles.
Pro Tip: Discuss all potential treatment options, including clinical trials, with your oncology team. Each option comes with specific risks and benefits that should be thoroughly understood in the context of your individual diagnosis.
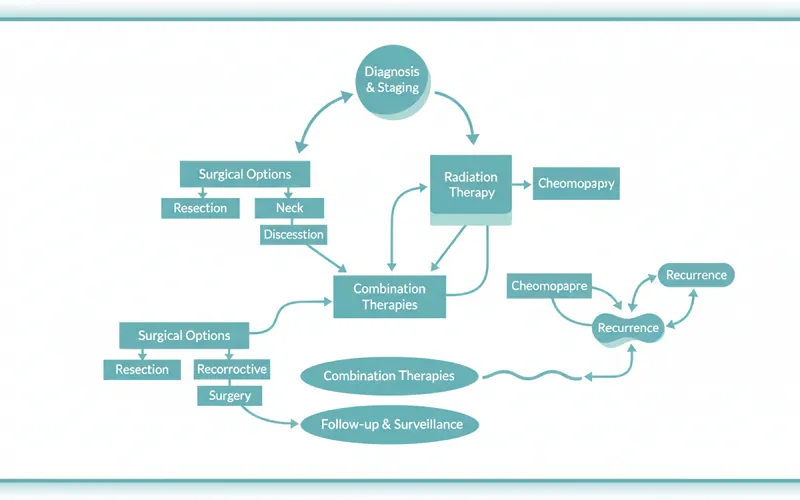
Step-by-Step Process: What to Expect During Treatment
Navigating a cancer diagnosis and treatment can be daunting. Here's a general step-by-step overview of what you can expect:
-
Diagnosis and Staging:
- Initial Visit: You'll likely first see your dentist or an oral surgeon for any suspicious lesions.
- Biopsy: A small tissue sample from the suspicious area is taken (incisional biopsy or punch biopsy) and sent to a pathologist for microscopic examination. This is the only definitive way to diagnose cancer.
- Imaging: If cancer is confirmed, imaging tests like CT scans, MRI, and PET scans are performed to determine the tumor's size, depth of invasion, involvement of nearby structures, and whether it has spread to lymph nodes or distant organs (staging).
- Multidisciplinary Team Consultation: Your case will be reviewed by a team of specialists (head and neck surgeon, radiation oncologist, medical oncologist, speech-language pathologist, dietitian) who will collaborate on a comprehensive treatment plan.
-
Treatment Planning:
- Based on staging results, your team will recommend a primary treatment (usually surgery, radiation, or a combination).
- You will have detailed consultations to discuss the pros, cons, potential side effects, and expected outcomes of each recommended option.
- Dental evaluations are crucial before radiation therapy to address any potential issues that could worsen post-radiation (e.g., extractions of compromised teeth).
-
Treatment Implementation:
- Surgery (if indicated): Typically performed first. This involves the surgical removal of the tumor and potentially lymph nodes. This is often followed by reconstructive surgery if a significant amount of tissue was removed. Hospital stay can range from a few days to several weeks.
- Radiation Therapy (if indicated): Usually starts 3-6 weeks after surgery, allowing for initial healing. It involves daily sessions (Monday-Friday) for 5-7 weeks. Each session is relatively short (15-30 minutes). If radiation is the primary treatment, it might be combined with chemotherapy.
- Chemotherapy (if indicated): Can be given concurrently with radiation (chemoradiation) or as a standalone systemic treatment. Cycles vary in duration and frequency, often over several months.
- Targeted/Immunotherapy: Administered intravenously, often in cycles, for advanced or recurrent cases.
-
Recovery and Rehabilitation:
- Post-Surgery: Pain management, wound care, and early mobilization.
- Speech and Swallowing Therapy: Essential to regain function, often starting during treatment and continuing for months.
- Nutritional Support: Many patients require a feeding tube (nasogastric or gastrostomy) during or after treatment due to difficulty eating.
- Psychological Support: Cancer treatment can be emotionally and psychologically challenging. Support groups, counseling, and mental health professionals can be invaluable.
-
Follow-up and Surveillance:
- After completing treatment, regular follow-up appointments with your oncology team are crucial. Initially, these may be every 1-3 months, gradually extending to every 6 months or annually.
- These appointments include thorough oral examinations, imaging, and monitoring for recurrence or new primary cancers.
Cost and Insurance
The cost of floor of mouth cancer treatment in the US can be substantial, ranging from tens of thousands to hundreds of thousands of dollars, depending on the stage of cancer, chosen treatments, complications, and geographic location.
| Treatment Phase/Procedure | Average US Cost (Without Insurance) | Average US Cost (With Insurance, Patient Share) |
|---|---|---|
| Initial Diagnosis | ||
| Oral Biopsy | $300 - $1,500 | $50 - $300 (after deductible) |
| CT Scan / MRI | $1,000 - $5,000 | $100 - $1,000 (after deductible) |
| PET Scan | $3,000 - $10,000 | $300 - $2,000 (after deductible) |
| Primary Treatment | ||
| Minor Surgery (Resection) | $5,000 - $20,000 | $1,000 - $5,000 |
| Major Surgery (Mandibulectomy, Extensive Resection, Reconstruction, Neck Dissection) | $30,000 - $150,000+ | $5,000 - $15,000+ |
| Radiation Therapy (5-7 weeks) | $30,000 - $50,000 | $2,000 - $8,000 |
| Chemotherapy (per cycle) | $10,000 - $30,000 | $500 - $3,000 |
| Targeted/Immunotherapy | $10,000 - $20,000 (per month) | $1,000 - $5,000 (per month) |
| Supportive Care & Follow-up | ||
| Speech/Swallowing Therapy | $100 - $300 (per session) | $20 - $75 (per session) |
| Nutritional Support (Feeding tube, formula) | $500 - $2,000 (per month) | $50 - $200 (per month) |
| Follow-up Oncologist Visits | $200 - $500 (per visit) | $30 - $100 (per visit) |
Insurance Coverage: Most medical insurance plans (including Medicare and Medicaid) cover the majority of floor of mouth cancer diagnosis and treatment costs, as it is a medically necessary procedure. However, "coverage" does not mean "free." You will still be responsible for:
- Deductibles: The amount you must pay out-of-pocket before your insurance begins to cover costs. These can range from a few hundred to several thousand dollars annually.
- Co-pays: A fixed amount you pay for a doctor's visit or prescription.
- Co-insurance: A percentage of the cost of a medical service that you are responsible for after your deductible has been met. For example, if your plan covers 80%, you pay the remaining 20%.
- Out-of-Pocket Maximums: Most plans have an annual limit on what you pay for covered services. Once you reach this maximum, your insurance pays 100% of covered costs for the rest of the year.
Regional Price Variations: Costs can vary significantly by region. Major metropolitan areas (e.g., New York City, Los Angeles, Boston) often have higher healthcare costs compared to rural areas or cities with a lower cost of living (e.g., parts of the Midwest or South). This can influence both the overall cost and the patient's out-of-pocket responsibility.
Payment Plans and Financing Options:
- Hospital Financial Assistance: Many hospitals have financial counselors who can help you understand your bill, apply for financial assistance programs, or set up payment plans.
- Patient Advocacy Groups: Organizations like the American Cancer Society or local cancer support groups can provide resources for financial assistance.
- Medical Credit Cards: Options like CareCredit offer financing for healthcare expenses, often with deferred interest periods.
- Personal Loans: Banks or credit unions may offer personal loans, but interest rates can vary.
Cost-Saving Tips:
- Understand Your Policy: Know your deductible, co-pays, co-insurance, and out-of-pocket maximum before treatment begins.
- Prior Authorization: Ensure all major procedures and medications receive prior authorization from your insurance company to avoid denied claims.
- Generic Medications: Opt for generic versions of prescription drugs when available.
- Utilize In-Network Providers: Staying within your insurance network can significantly reduce costs.
- Negotiate Bills: Sometimes, you can negotiate directly with providers for a reduced cash price, especially for larger bills.
Recovery and Aftercare
Recovery from floor of mouth cancer treatment is a multifaceted process that extends beyond the immediate post-operative or post-radiation period. It focuses on regaining function, managing side effects, and preventing recurrence.
Immediate Post-Treatment:
- Pain Management: You will be prescribed pain medication, which should be taken as directed to ensure comfort and facilitate healing.
- Wound Care: If surgery was performed, meticulous wound care is essential to prevent infection and promote healing. This may involve specific mouth rinses (e.g., saline rinses recommended by the ADA).
- Nutritional Support: Many patients will have difficulty eating or swallowing initially due to swelling, pain, or surgical changes. A temporary feeding tube (nasogastric or gastrostomy tube) may be placed to ensure adequate nutrition and hydration. A dietitian will provide guidance on appropriate diet modifications and nutritional supplements.
- Tracheostomy Care (if applicable): In some extensive surgeries, a temporary tracheostomy (breathing tube in the neck) may be necessary, requiring specific care.
Rehabilitation and Long-Term Care:
- Speech and Swallowing Therapy: This is a cornerstone of rehabilitation. A speech-language pathologist (SLP) will work with you to improve your ability to speak, chew, and swallow. Exercises will target tongue mobility, oral motor control, and safe swallowing techniques. This therapy can last for months or even years.
- Physical Therapy: If neck dissection was performed, you might experience shoulder stiffness or limited range of motion. Physical therapy can help restore function.
- Dental Care: Regular and meticulous dental hygiene is crucial, especially after radiation, which can increase the risk of dry mouth, tooth decay, and osteoradionecrosis (jawbone death). Your dentist may recommend special fluoride treatments, salivary substitutes, and more frequent check-ups (e.g., every 3 months). The ADA emphasizes diligent oral hygiene for all oral cancer patients, especially those who have undergone radiation.
- Psychological and Emotional Support: Coping with cancer and its aftermath can be challenging. Support groups, counseling, and psychological services are often recommended to help patients and their families adjust.
- Prosthetic Rehabilitation: For significant bone or tissue loss, dental prostheses (e.g., obturators, dental implants) may be needed to restore function and aesthetics.
- Smoking Cessation and Alcohol Moderation: Absolutely critical for preventing recurrence and secondary cancers.
Follow-up Schedule:
- Years 1-2: Every 1-3 months with your oncology team.
- Years 3-5: Every 3-6 months.
- After Year 5: Annually.
These follow-up visits include comprehensive oral examinations, neck palpation for lymph nodes, and sometimes imaging (CT, MRI, PET scans) to monitor for any signs of recurrence.
Prevention
Preventing floor of mouth cancer largely revolves around mitigating the primary risk factors. Proactive steps can significantly reduce your chances of developing this aggressive disease. This section directly addresses how to prevent oral cancer.
-
Eliminate Tobacco Use: This is the most impactful step you can take.
- Quit Smoking: Smoking cigarettes, cigars, and pipes introduces numerous carcinogens directly into your mouth.
- Avoid Smokeless Tobacco: Chewing tobacco, snuff, and dip are particularly dangerous for the floor of the mouth, where the product is often held.
- Seek Support: Quitting can be challenging, but resources like nicotine replacement therapy, medications, counseling, and support groups can dramatically increase your success rate.
-
Moderate Alcohol Consumption:
- Limit Intake: For men, this means no more than two standard drinks per day; for women, no more than one.
- Avoid Heavy Drinking: Binge drinking and chronic heavy alcohol use are strongly linked to oral cancer.
-
Get Vaccinated Against HPV:
- While HPV is more strongly linked to oropharyngeal cancers, vaccination can help prevent certain types of HPV infections that may contribute to some oral cancers. The Centers for Disease Control and Prevention (CDC) recommends HPV vaccination for children at age 11 or 12, but it can be given up to age 26, and in some cases, up to age 45.
-
Maintain a Healthy Diet:
- Eat Plenty of Fruits and Vegetables: A diet rich in a variety of fruits and vegetables provides essential vitamins, minerals, and antioxidants that help protect cells from damage. Aim for at least 5 servings daily.
- Limit Processed Foods: Reduce consumption of processed meats, sugary drinks, and highly processed foods.
-
Practice Good Oral Hygiene and Regular Dental Check-ups:
- Brush and Floss Regularly: Maintain excellent oral hygiene to reduce inflammation and potential chronic irritation.
- Routine Dental Exams: Schedule dental check-ups at least annually, and ideally every six months, even if you have no symptoms. Your dentist is often the first healthcare professional to spot suspicious lesions during a routine oral cancer screening. They can identify subtle changes (like leukoplakia or erythroplakia) before they become cancerous.
- Address Dental Issues: Promptly address sharp teeth, ill-fitting dentures, or any other source of chronic irritation in your mouth.
-
Limit Sun Exposure (for lip cancer, though good practice overall): While not directly related to floor of mouth cancer, protecting your lips from excessive sun exposure by using lip balm with SPF can prevent lip cancer.
-
Know Your Body: Be aware of the signs and symptoms of oral cancer and promptly report any persistent changes to your dentist or doctor.
Risks and Complications
Treatment for floor of mouth cancer can be life-saving, but it is often accompanied by a range of potential risks and complications, both short-term and long-term.

Immediate Surgical Risks:
- Bleeding and Infection: Common risks with any surgery.
- Nerve Damage: Depending on the extent of the resection, nerves controlling sensation (e.g., numbness of the tongue or lower lip), taste, or movement (e.g., difficulty moving the tongue, shoulder drop from neck dissection) can be affected.
- Wound Healing Issues: Especially in areas with poor blood supply or in patients who smoke.
- Fistula Formation: An abnormal connection between surgical sites and the skin, leading to leakage of saliva.
- Swelling and Airway Obstruction: Significant swelling can temporarily compromise the airway, sometimes requiring a temporary tracheostomy.
Side Effects of Radiation Therapy:
- Oral Mucositis: Painful inflammation and sores in the mouth and throat, making eating and swallowing difficult.
- Xerostomia (Dry Mouth): Radiation can damage salivary glands, leading to permanent dry mouth, increasing the risk of tooth decay and gum disease.
- Dysphagia (Difficulty Swallowing): Due to pain, swelling, or changes in muscle function.
- Taste Changes: Loss or alteration of taste.
- Skin Reactions: Redness, irritation, blistering, or peeling in the irradiated area.
- Osteoradionecrosis: Rare but serious complication where radiation damages the jawbone, leading to bone death, especially after dental extractions in the radiated area. This risk highlights the importance of pre-radiation dental evaluations.
- Trismus: Stiffness or limited opening of the jaw due to fibrosis (scarring) of chewing muscles.
Side Effects of Chemotherapy/Targeted/Immunotherapy:
- Nausea, Vomiting, Fatigue: Common systemic side effects.
- Hair Loss: Varies depending on the specific drugs used.
- Myelosuppression: Suppression of bone marrow, leading to low blood counts (anemia, neutropenia, thrombocytopenia), increasing risk of infection and bleeding.
- Neuropathy: Nerve damage causing numbness or tingling in hands and feet.
- Kidney or Liver Damage: Certain drugs can affect organ function.
- Immunotherapy-related Side Effects: Can cause immune reactions in various organs (e.g., skin rash, colitis, thyroid issues).
Long-Term Complications:
- Functional Impairments: Persistent difficulties with speech, swallowing, and chewing, potentially requiring long-term therapy or dietary modifications.
- Cosmetic Changes: Alterations to facial appearance, which can be emotionally challenging.
- Recurrence: The cancer may return in the same area (local recurrence) or in nearby lymph nodes (regional recurrence).
- Second Primary Cancer: Patients treated for one head and neck cancer are at an increased risk of developing another primary cancer in the upper aerodigestive tract (e.g., mouth, throat, esophagus, lung), especially if they continue to use tobacco or alcohol. This risk underscores the importance of continued surveillance and risk factor modification.
- Psychosocial Impact: Depression, anxiety, and social isolation are common after cancer treatment.
| Risk Factor | Impact on Floor of Mouth Cancer Risk | Prevention Strategy |
|---|---|---|
| Tobacco Use | High Risk (10-20x increased) | Quit all forms of tobacco. |
| Excessive Alcohol Use | High Risk (3-5x increased) | Moderate or eliminate alcohol consumption. |
| Tobacco + Alcohol Combo | Very High Risk (up to 30x increased) | Eliminate both tobacco and excessive alcohol. |
| HPV Infection (certain strains) | Moderate Risk (more so for oropharynx) | HPV Vaccination (Gardasil 9). |
| Poor Nutrition | Low-Moderate Risk | Eat a diet rich in fruits and vegetables. |
| Chronic Irritation | Low-Moderate Risk (co-factor) | Address ill-fitting dentures, sharp teeth promptly. |
| Age (>50) | Inherent Risk Factor | N/A (focus on modifiable risks). |
| Genetics/Family History | Inherent Risk Factor | N/A (focus on modifiable risks and regular screening). |
Children / Pediatric Considerations
Floor of mouth cancer is exceedingly rare in children. Oral cancers primarily affect adults, particularly those over 50 with a history of tobacco and alcohol use. When oral lesions or growths occur in children, they are almost invariably benign (non-cancerous) conditions such as cysts, infections, or reactive lesions.
However, any persistent lump, sore, or abnormal change in a child's mouth should still be promptly evaluated by a pediatrician or pediatric dentist. While extremely uncommon, other types of head and neck cancers, such as lymphomas, sarcomas, or rhabdomyosarcomas, can occur in children, and early diagnosis is crucial for these as well. Parents should ensure children receive regular dental check-ups, which include visual examinations of the oral cavity.
Cost Breakdown
While covered generally earlier, let's look at a more precise breakdown for common components of floor of mouth cancer treatment, highlighting the low, mid, and high range within the US, with and without insurance considerations.
Average US Costs (Ranges, without insurance):
- Initial Consultation with Specialist: $150 - $600
- Biopsy (incisional/punch): $300 - $1,500 (plus pathologist fees of $200 - $800)
- Staging Imaging (CT/MRI/PET):
- CT Scan: $1,000 - $5,000
- MRI Scan: $1,500 - $7,000
- PET Scan: $3,000 - $10,000
- Surgery (varying complexity):
- Small lesion excision with no reconstruction: $5,000 - $20,000
- Extensive resection with neck dissection and microvascular reconstruction (free flap): $50,000 - $150,000+ (This can be considerably higher depending on hospital charges, length of stay, and specialized surgical teams).
- Radiation Therapy (full course, 5-7 weeks): $30,000 - $50,000
- Chemotherapy (per cycle): $10,000 - $30,000 (often multiple cycles are needed)
- Targeted Therapy / Immunotherapy (monthly infusion): $10,000 - $20,000 per month (can extend for many months or years)
- Speech and Swallowing Therapy (per session): $100 - $300
- Dietitian Consultations (per session): $75 - $250
- Dental Rehabilitation (post-treatment, e.g., implants, prosthetics): $5,000 - $30,000 (highly variable)
With Insurance (Patient Share): Even with insurance, you should anticipate out-of-pocket costs due to deductibles, co-pays, and co-insurance.
- Deductibles: Typically range from $500 to $7,000 per year for individual plans.
- Co-pays: $20-$75 for specialist visits; $100-$500 for emergency room visits; $10-$100 for prescriptions.
- Co-insurance: Often 10%-30% for major medical procedures and hospital stays after the deductible is met.
- Out-of-Pocket Maximums: Range from $1,500 to $9,000+ per year for individual plans. Once this is met, insurance generally covers 100% of covered services.
Example Scenario (Major Surgery + Chemoradiation with good insurance): A patient undergoes extensive surgery ($100,000 charge), followed by chemoradiation ($60,000 charge).
- Deductible: Let's say $3,000.
- Co-insurance: 20%
- Out-of-pocket Max: $7,000.
In this scenario, the patient would pay their $3,000 deductible. For the remaining $157,000 ($160,000 - $3,000), they would pay 20% until their out-of-pocket maximum ($7,000) is reached. So, they would pay an additional $4,000 to reach their max ($3,000 deductible + $4,000 co-insurance). The insurance would then cover the rest.
However, this doesn't include potentially uncovered services, travel costs, lost wages, or expensive post-treatment dental rehabilitation that may fall under dental insurance (which often has separate, lower limits).
Payment Plans and Financing Options:
- Hospital Financial Assistance Programs: Many hospitals have charitable programs or discounted rates for uninsured or underinsured patients. Inquire with the hospital's financial counseling department.
- Government Programs: Medicaid and CHIP (Children's Health Insurance Program) provide low-cost or free health coverage for eligible low-income individuals and families.
- Non-profit Organizations: Organizations like the American Cancer Society, Oral Cancer Foundation, and regional cancer support groups often have resources or grants for patients facing financial hardship.
- Medical Credit Cards: Companies like CareCredit or Alphaeon Credit offer specialized credit lines for healthcare expenses, often with promotional interest-free periods if paid in full. Be cautious of high-interest rates after the promotional period.
- Crowdfunding: Platforms like GoFundMe allow individuals to raise funds for medical expenses from their social networks.
Cost-Saving Tips:
- Choose In-Network Providers: Always verify that all doctors, hospitals, and facilities are in your insurance network to maximize benefits.
- Pre-authorization: Ensure your medical team obtains pre-authorization from your insurance for all significant tests, procedures, and medications.
- Generic Drugs: Ask your doctor if generic alternatives are available for any prescribed medications.
- Review Bills Carefully: Medical bills can contain errors. Review them thoroughly and question any charges you don't understand.
- Patient Advocate: Consider hiring a professional patient advocate, or having a trusted family member serve in this role, to help navigate billing and insurance complexities.
Frequently Asked Questions
Q1: Is floor of mouth cancer curable?
Yes, floor of mouth cancer is curable, especially when detected at an early stage oral cancer. The overall 5-year survival rate for localized oral cavity cancer is around 84%. However, the cure rate significantly decreases if the cancer has spread to lymph nodes or distant sites. Early detection through regular dental check-ups and prompt treatment are the most critical factors for a positive outcome.
Q2: How painful is floor of mouth cancer and its treatment?
Early-stage floor of mouth cancer is often painless, which is why it can go undetected. As it progresses, it can cause persistent pain, soreness, or burning sensations. Treatment, particularly surgery and radiation, can be quite painful initially. However, effective pain management strategies and medications are always part of the treatment plan to ensure patient comfort during recovery.
Q3: How long does treatment for floor of mouth cancer typically last?
The duration of treatment varies. Surgery typically involves a hospital stay of a few days to several weeks. Radiation therapy usually lasts 5-7 weeks, with daily sessions. Chemotherapy cycles can extend over several months. The entire active treatment phase, including surgery, recovery, and adjuvant therapies, can span 3-6 months, followed by years of rehabilitation and surveillance.
Q4: What are the long-term side effects I should be prepared for?
Long-term side effects can include persistent difficulties with speech, chewing, and swallowing (dysphagia), permanent dry mouth (xerostomia), altered taste, jaw stiffness (trismus), and changes in facial appearance. Regular rehabilitation (speech/swallowing therapy, physical therapy) and ongoing dental care are vital to manage these issues.
Q5: Are there any alternative or natural remedies for floor of mouth cancer?
While a healthy lifestyle, rich in antioxidants and good nutrition, can help in prevention and support overall health during treatment, there is no scientific evidence that alternative or natural remedies alone can cure floor of mouth cancer. These should never replace conventional medical treatment. Always discuss any complementary therapies with your oncology team to ensure they don't interfere with your prescribed treatment.
Q6: How often should I get screened for oral cancer?
The American Dental Association (ADA) recommends routine oral cancer screenings as part of your annual or bi-annual comprehensive dental check-up. Individuals with high-risk factors (tobacco, alcohol use) may benefit from more frequent screenings. If you have any suspicious symptoms, see a dentist immediately, regardless of your last screening.
Q7: Can floor of mouth cancer recur?
Yes, there is a risk of recurrence, which means the cancer can come back in the same area (local recurrence), in nearby lymph nodes (regional recurrence), or as a new primary cancer elsewhere in the head and neck region. This risk is higher for those who continue risky behaviors like smoking and drinking. Regular follow-up appointments are crucial for early detection of any recurrence.
Q8: What is the typical recovery time after surgery?
Initial recovery from surgery can take several weeks, with significant swelling and discomfort. Full recovery of function (speech, swallowing, chewing) may take several months to a year or more, often requiring intensive rehabilitation with speech-language pathologists and other therapists.
When to See a Dentist
Given that early stage oral cancer often presents without pain, knowing when to seek professional evaluation is crucial. Your dentist plays a vital role in routine oral cancer screening, but certain signs warrant immediate attention.
Immediate Attention (within a few days):
- Any sore, lump, or ulcer on the floor of your mouth that doesn't heal within two weeks. This is the single most important warning sign.
- Persistent red (erythroplakia) or white (leukoplakia) patches that cannot be scraped off and are not resolving. Erythroplakia is particularly concerning.
- Any new, unexplained lump or thickening under your tongue or on the floor of your mouth, even if it's painless.
- Difficulty or pain when moving your tongue, chewing, or swallowing that is new and persistent.
- Unexplained numbness or tingling in your tongue, mouth, or lower lip.
- Unexplained bleeding from your mouth.
- A feeling that something is caught in your throat that persists.
Routine Care Guidance:
- Regular Dental Check-ups: Schedule comprehensive dental examinations at least once a year, and ideally every six months, for oral cancer screenings, as recommended by the ADA. Your dentist is trained to identify subtle changes that might indicate precancerous or cancerous conditions.
- Self-Exams: Perform monthly self-exams of your mouth, including lifting your tongue to thoroughly inspect the floor of your mouth, looking for any changes.
- Discussion of Risk Factors: If you have significant risk factors (e.g., tobacco use, heavy alcohol consumption), discuss these with your dentist. They may recommend more frequent screenings or counseling on how to prevent oral cancer.
Do not delay seeking a professional opinion for any persistent changes in your mouth. Early detection is paramount for the successful treatment of floor of mouth cancer.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Oral Cancer Stages Pictures: Complete Guide
Oral cancer, a serious and potentially life-threatening disease, affects thousands of Americans each year. According to the American Cancer Society, approximately 54,000 new cases of oral cavity or oropharyngeal cancer are diagnosed annually in the United States. While these numbers can be daunt
February 23, 2026
Can You Die From Mouth Cancer
Oral cancer is a formidable disease, often striking with insidious subtlety before revealing its devastating potential. It's a question that weighs heavily on the minds of those who receive a diagnosis or even those simply concerned about unusual oral symptoms: can you die from mouth cancer? The
February 23, 2026

Mouth Cancer Photos: Complete Guide
Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,23
February 23, 2026
Mouth Cancer Pictures Early Stages: Complete Guide
Few diagnoses can be as unsettling as cancer, and when it affects a part of your body as central to daily life as your mouth, the concern is profound. Oral cancer, often referred to simply as mouth cancer, is a serious condition that, if detected early, has a significantly higher chance of s
February 23, 2026