Calcium on Teeth: Complete Guide

Key Takeaways
- A staggering 90% of adults in the United States will experience some form of gum disease in their lifetime, often starting with issues directly linked to mineral buildup on teeth. While calcium is vital for strong bones and teeth, its presence on teeth in the wrong form can lead to significant
A staggering 90% of adults in the United States will experience some form of gum disease in their lifetime, often starting with issues directly linked to mineral buildup on teeth. While calcium is vital for strong bones and teeth, its presence on teeth in the wrong form can lead to significant dental problems, including inflammation, decay, and even gum erosion. Understanding the multifaceted role of calcium on teeth—both beneficial and detrimental—is crucial for maintaining optimal oral health.
This comprehensive guide from SmilePedia.net will demystify the complex relationship between calcium and your pearly whites. We'll explore how calcium contributes to tooth strength, when its presence becomes a problem, the causes and symptoms of issues like calculus buildup and calcium deficiency teeth, and most importantly, effective strategies for treatment and prevention. From professional cleanings to dietary considerations, we'll equip you with the knowledge to safeguard your smile.
Key Takeaways:
- Calcium's Dual Role: While essential in teeth for strength (enamel/dentin), excessive mineralized deposits on teeth (calculus/tartar) can lead to gum disease and decay.
- Calculus Formation: Plaque hardens into calculus within 24-72 hours if not removed, primarily due to calcium and phosphate in saliva.
- Gum Erosion Link: Calculus buildup is a major contributor to gum inflammation (gingivitis) and subsequent gum erosion (recession) by trapping bacteria and irritating tissues.
- Calcium Deficiency Risks: Insufficient calcium intake can weaken tooth enamel, increasing susceptibility to cavities and potentially impacting jawbone density, especially during tooth development.
- Professional Cleaning is Key: Regular dental scaling and root planing (typically $75-$200 for a routine cleaning, $200-$600 per quadrant for deep cleaning without insurance) are the only effective ways to remove hardened calculus.
- Prevention is Paramount: Daily brushing with fluoride toothpaste, flossing, a balanced diet rich in calcium and vitamin D, and routine dental check-ups (every 6 months) are critical for preventing calculus and supporting strong teeth.
- Treatment Timelines: A routine cleaning takes about 30-60 minutes. Deep cleaning (scaling and root planing) may require 1-4 appointments, each lasting 45-90 minutes. Gum grafting, if needed for severe erosion, can take 1-2 hours per site, with recovery spanning 1-2 weeks.
What It Is / Overview
When we talk about "calcium on teeth," it's important to differentiate between several concepts that, while related to calcium, have very different implications for your oral health.

Firstly, calcium in teeth refers to the mineral that makes up the bulk of your tooth structure. Along with phosphate, calcium forms hydroxyapatite crystals, the primary component of enamel (the hard outer layer), dentin (the layer beneath enamel), and cementum (the layer covering the tooth root). This calcium is vital for tooth strength, hardness, and resistance to acid attacks. A continuous supply of calcium through diet and saliva is essential for maintaining this structure and repairing microscopic damage through a process called remineralization.
Secondly, calcium on teeth can refer to the beneficial process of remineralization. Your saliva is naturally rich in calcium and phosphate ions. When your teeth are exposed to acids (from food, drinks, or bacteria), these acids can demineralize, or weaken, the enamel surface. Saliva acts as a natural buffer, neutralizing acids and depositing calcium and phosphate back onto the enamel, repairing these tiny lesions and strengthening the tooth. Fluoride plays a crucial role in enhancing this remineralization process, making the enamel more resistant to future acid attacks. This is a natural, protective mechanism.
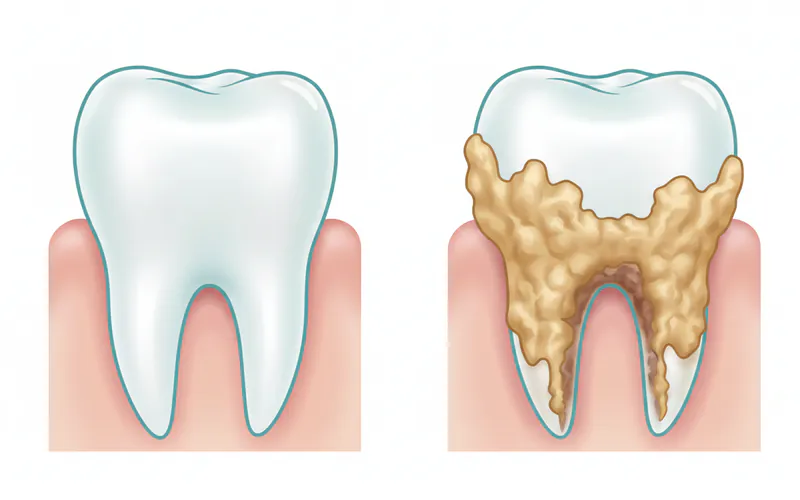
However, the term "calcium on teeth" most commonly and detrimentally refers to calculus, also known as tartar. Calculus is essentially plaque that has hardened or mineralized over time. Plaque is a sticky, colorless film of bacteria that constantly forms on your teeth. If plaque is not thoroughly removed through daily brushing and flossing, the minerals present in your saliva—primarily calcium and phosphate—begin to deposit into the plaque matrix. This process transforms soft plaque into a rough, porous, hard substance that adheres firmly to the tooth surface. This hardened mineral deposit is calculus, and unlike plaque, it cannot be removed by brushing or flossing alone.
Calculus can form both above the gum line (supragingival calculus) and below it (subgingival calculus). Its rough surface provides an ideal environment for more plaque bacteria to accumulate, making it much harder to clean your teeth effectively. This accumulation of bacteria and the physical irritation from the calculus itself are primary drivers of gum inflammation (gingivitis) and, if left untreated, can progress to more severe forms of periodontal disease, including gum erosion and bone loss.
Furthermore, it's crucial to understand the impact of calcium deficiency teeth. While the immediate issue of calculus involves too much mineral buildup on the teeth, a lack of dietary calcium and vitamin D (which aids calcium absorption) can significantly weaken the structural integrity of the teeth. This deficiency can lead to weaker enamel, making teeth more susceptible to cavities and fractures, and can also impact the health of the jawbone, which supports the teeth.
In essence, while calcium is absolutely critical for healthy teeth, its improper accumulation on the teeth as calculus, or its absence from the diet, can lead to serious oral health complications.
Types / Variations
Understanding the different manifestations of calcium-related issues in oral health helps in identifying and addressing them effectively.
Calculus (Tartar) Formation
This is the most common interpretation of problematic "calcium on teeth." Calculus is classified primarily by its location:
- Supragingival Calculus: This type forms above the gum line and is typically visible, appearing as a yellowish, brownish, or even blackish deposit. It commonly forms on the inner surfaces of the lower front teeth and the outer surfaces of the upper molars, areas close to salivary gland ducts where mineral-rich saliva is abundant. Its rough surface traps more plaque and stains easily, contributing to bad breath and an unesthetic appearance.
- Subgingival Calculus: This type forms below the gum line, within the gingival sulcus (the shallow space between the tooth and the gum). It is often darker, denser, and harder than supragingival calculus, due to its exposure to blood products and gingival crevicular fluid. Subgingival calculus is not visible to the naked eye and requires a dental professional to detect and remove. Its presence directly contributes to periodontal inflammation, detaching the gums from the tooth surface, creating periodontal pockets, and leading to gum erosion (recession) and bone loss.
Remineralization
This is the beneficial "calcium on teeth" process:
- Natural Salivary Remineralization: As mentioned, saliva acts as a natural repair system. After acid attacks, calcium and phosphate ions in saliva naturally re-deposit onto the enamel surface, repairing early lesions. This is a continuous, microscopic process.
- Fluoride-Enhanced Remineralization: Fluoride significantly boosts this natural process. When fluoride is present during remineralization, it helps form fluorapatite, a crystal structure that is even stronger and more acid-resistant than the original hydroxyapatite of the enamel. This is why fluoride in toothpaste, water, and dental treatments is so crucial for preventing cavities.
Calcium Deficiency Manifestations
A lack of sufficient calcium can impact teeth, especially during development, and contribute to overall oral health issues:
- Weakened Enamel: In children, inadequate calcium during tooth formation can result in hypocalcification, where enamel is less dense, softer, and more porous. This makes the teeth highly vulnerable to decay. In adults, chronic deficiency can contribute to overall enamel weakness and increased susceptibility to erosion and cavities.
- Increased Caries Risk: Weaker enamel due to calcium deficiency provides less resistance to acid produced by bacteria, accelerating the formation and progression of cavities.
- Jawbone Density Reduction: Calcium is vital for bone health, including the jawbone that supports your teeth. While primarily associated with systemic osteoporosis, severe, long-term calcium deficiency can contribute to reduced jawbone density, potentially affecting tooth stability and increasing the risk of tooth loss, particularly in older adults.
- Osteoporosis-Related Tooth Loss: While not directly "calcium on teeth," systemic calcium deficiency leading to osteoporosis can weaken the alveolar bone (the bone that holds teeth in place), making teeth more prone to mobility and loss.
Causes / Why It Happens
Understanding the root causes of calculus formation, calcium deficiency-related dental issues, and gum erosion is key to effective prevention and treatment.
Causes of Calculus (Tartar) Buildup
Calculus formation is primarily a consequence of inadequate oral hygiene, but several other factors can contribute:
- Poor Oral Hygiene: This is the number one cause. If plaque is not thoroughly removed within 24-72 hours by brushing and flossing, it begins to mineralize due to the calcium and phosphate ions in saliva. The longer plaque remains, the harder it becomes.
- Salivary Composition: Individuals with saliva that is naturally richer in calcium and phosphate, or has a higher pH (less acidic), may be more prone to calculus formation. This doesn't mean "bad" saliva, just a different biochemical profile.
- Diet: While diet doesn't directly cause calculus in the same way it causes cavities, certain dietary habits can influence plaque formation. Frequent consumption of sugary and starchy foods feeds plaque bacteria, leading to a thicker, stickier plaque film that is more difficult to remove.
- Smoking and Tobacco Use: Tobacco users are significantly more likely to develop calculus. Smoking reduces salivary flow, alters the oral microbiome, and impairs the immune response, all of which create a more favorable environment for plaque and calculus formation.
- Dry Mouth (Xerostomia): Reduced salivary flow, caused by certain medications, medical conditions, or aging, can decrease the natural cleansing action of saliva. While it might seem counterintuitive, less saliva means less buffering capacity and potentially a more concentrated environment for minerals to deposit, leading to calculus.
- Genetics: Some individuals are genetically predisposed to forming more calculus than others, even with good oral hygiene.
- Dental Appliances: Braces, retainers, and poorly fitting restorations can create additional surfaces and traps for plaque to accumulate, making thorough cleaning more challenging and increasing calculus risk.
Causes of Calcium Deficiency Teeth
Issues related to insufficient calcium affecting teeth are largely systemic:
- Inadequate Dietary Intake: The most straightforward cause. If your diet consistently lacks calcium-rich foods (dairy, fortified plant milks, leafy greens, certain fish), your body will not have enough calcium to support healthy teeth and bones.
- Vitamin D Deficiency: Vitamin D is crucial for the absorption of calcium from the digestive tract into the bloodstream. Without sufficient vitamin D, even adequate calcium intake may not translate to enough usable calcium for the body, including teeth.
- Malabsorption Issues: Certain medical conditions (e.g., Crohn's disease, celiac disease, some kidney disorders) or medications can impair the body's ability to absorb calcium and vitamin D, regardless of dietary intake.
- Hormonal Imbalances: Conditions affecting parathyroid hormone or estrogen levels (e.g., menopause) can impact calcium metabolism and bone density, indirectly affecting dental health over time.
- Early Childhood Nutrition: Poor nutrition, especially during critical periods of tooth development in infancy and childhood, can lead to structurally weaker enamel (hypocalcification), making teeth more susceptible to decay from the outset.
Causes of Gum Erosion (Recession)
Gum erosion, or gingival recession, is a common problem linked to both calculus and other factors:
- Periodontal Disease (Calculus-Induced): This is a primary driver. Calculus buildup, particularly subgingival calculus, harbors bacteria that release toxins. These toxins trigger an inflammatory response that progressively destroys gum tissue and the underlying bone. As the supporting structures degrade, the gums pull away, or "erode," from the tooth surface, exposing the roots.
- Aggressive Tooth Brushing: Brushing too hard, using a hard-bristled toothbrush, or improper brushing techniques can physically abrade gum tissue over time, leading to recession.
- Traumatic Occlusion (Bite Issues): Misaligned teeth or an uneven bite can put excessive force on certain teeth, contributing to bone loss around those teeth and subsequent gum recession.
- Tobacco Use: Smoking and chewing tobacco are significant risk factors for gum disease and recession. They impair blood flow to the gums, hinder healing, and promote bacterial growth.
- Genetics: Some individuals are genetically predisposed to thinner gum tissue or a higher susceptibility to gum disease, making them more prone to recession.
- Clenching and Grinding (Bruxism): Chronic clenching or grinding of teeth can exert excessive forces on the teeth and supporting structures, potentially contributing to bone loss and gum recession.
- Oral Piercings: Jewelry in the lip or tongue can rub against gum tissue, causing chronic irritation and eventually recession.
- Orthodontic Treatment: While usually corrective, improper orthodontic forces or prolonged treatment can sometimes contribute to recession in susceptible individuals.
Signs and Symptoms
Recognizing the signs and symptoms early can prevent further complications related to calculus, calcium deficiency, and gum erosion.
Signs and Symptoms of Calculus (Tartar) Buildup
Calculus often presents with noticeable visual and sensory cues:
- Rough Spots on Teeth: Even if not highly visible, you might feel a rough, bumpy texture on your tooth surfaces, especially near the gum line, when you run your tongue over them.
- Visible Deposits: Yellowish, brownish, or even blackish hard deposits, most commonly seen on the inner surfaces of lower front teeth and outer surfaces of upper molars.
- Bad Breath (Halitosis): Calculus provides a porous surface for bacteria to thrive, which produce foul-smelling gases.
- Swollen, Red, or Tender Gums: Calculus near the gum line irritates the gum tissue, leading to inflammation, which manifests as redness, swelling, and tenderness.
- Bleeding Gums: Gums that bleed easily during brushing, flossing, or even when eating, are a classic sign of gingivitis, often exacerbated by calculus.
- Receding Gums: As calculus pushes the gums away and causes inflammation, the gum tissue can start to pull back, exposing more of the tooth root.
- Tooth Sensitivity: Exposed tooth roots due to gum recession (caused by calculus) can lead to sensitivity to hot, cold, sweet, or acidic foods and drinks.
Signs and Symptoms of Calcium Deficiency Teeth
The impact of calcium deficiency on teeth might be more subtle or develop over a longer period:
- Increased Cavities: Weakened or hypocalcified enamel is less resistant to acid attacks, leading to more frequent or rapidly progressing cavities.
- Brittle or Chipping Teeth: In severe cases, particularly if the deficiency occurred during tooth development, teeth may be unusually brittle or prone to chipping and fracture.
- Enamel Defects: Pits, grooves, or rough spots on the enamel surface (hypoplasia or hypocalcification) can indicate a historical deficiency during tooth development.
- Delayed Eruption or Abnormal Tooth Development: In children, severe calcium deficiency can interfere with proper tooth formation and eruption patterns.
- Overall Bone Weakness (Systemic): While not a direct tooth symptom, systemic signs like frequent bone fractures or osteoporosis can signal a calcium deficiency that may also be impacting jawbone density and indirectly tooth stability.
- Tooth Mobility (Advanced Cases): If severe calcium deficiency contributes to significant jawbone loss, teeth may become loose.
Signs and Symptoms of Gum Erosion (Recession)
Gum erosion has specific visual and symptomatic indicators:
- Longer-Looking Teeth: The most obvious sign is when teeth appear longer than usual because the gum line has pulled back, exposing more of the tooth root.
- Tooth Sensitivity: Exposed root surfaces lack enamel protection and contain tiny tubules that lead to the tooth's nerve. This exposure causes increased sensitivity to temperature changes, sweet foods, and touch.
- Visible Roots: The yellow-tinged root surface (dentin/cementum) may be visible, contrasting with the white enamel.
- Notches Near the Gum Line: Sometimes, a distinct notch or indentation can be felt or seen at the point where the gum has receded from the tooth. This is often caused by aggressive brushing combined with recession.
- Change in Tooth Color: The exposed root surface may be darker or different in color than the enamel, contributing to a "two-tone" appearance.
- Loose Teeth: In advanced stages of gum disease where significant bone loss accompanies recession, teeth may become loose.
- Food Trapping: Spaces created by recession can make it easier for food to get trapped between teeth and gums, further irritating the area.
Treatment Options
Addressing issues related to calcium on teeth, calcium deficiency, and gum erosion requires a range of dental and sometimes medical interventions.
Treatment for Calculus (Tartar) Buildup and Related Gum Disease
Calculus cannot be removed at home; professional intervention is mandatory.
- Professional Dental Cleaning (Prophylaxis):
- What it is: A routine cleaning involves using specialized hand instruments (scalers) and ultrasonic devices to meticulously remove plaque and supragingival calculus from the tooth surfaces, both above and slightly below the gum line. The teeth are then polished to remove surface stains.
- Pros: Prevents gum disease, removes stains, freshens breath, relatively quick, non-invasive.
- Cons: Only effective for mild calculus and gingivitis; not sufficient for established periodontal disease.
- ADA Guidelines: The ADA recommends professional cleanings typically every six months for most individuals.
- Scaling and Root Planing (Deep Cleaning):
- What it is: This is a non-surgical procedure for treating moderate to severe periodontal disease where subgingival calculus and inflammation are present. Scaling involves thoroughly removing plaque and calculus from above and below the gum line, down to the bottom of the periodontal pockets. Root planing then smooths the root surfaces, making it harder for bacteria and plaque to reattach and promoting gum reattachment. It's often done under local anesthesia and may require multiple appointments.
- Pros: Highly effective at removing deep calculus, reducing gum inflammation, shrinking periodontal pockets, and preventing further bone loss. Can often halt the progression of gum disease.
- Cons: More invasive than a routine cleaning, may cause temporary sensitivity and discomfort, can be costly. Not a cure for advanced disease but a crucial management tool.
- Antibiotics (Adjunctive Therapy):
- What it is: In some cases, systemic (oral pills) or localized (gels/chips placed in pockets) antibiotics may be used in conjunction with scaling and root planing to target specific bacteria causing gum disease.
- Pros: Can enhance the effectiveness of deep cleaning by reducing bacterial load.
- Cons: Potential for side effects (e.g., digestive upset with oral antibiotics), risk of antibiotic resistance.
- Periodontal Surgery (for advanced cases):
- What it is: If scaling and root planing are insufficient, surgical procedures like flap surgery (to access deep calculus and reshape bone) or bone grafts may be necessary to reduce pocket depths and regenerate lost bone/tissue.
- Pros: Can save teeth that would otherwise be lost, reduces severe infection.
- Cons: More invasive, significant recovery time, higher cost, potential for post-operative discomfort and sensitivity.
Treatment for Calcium Deficiency Teeth
Addressing calcium deficiency involves systemic approaches:
- Dietary Modifications:
- What it is: Increasing intake of calcium-rich foods such as dairy products (milk, yogurt, cheese), fortified plant-based milks, leafy green vegetables (kale, spinach), fortified cereals, and certain fish (sardines, salmon).
- Pros: Natural, generally safe, provides other essential nutrients.
- Cons: May require significant dietary changes, consistency is key.
- Calcium and Vitamin D Supplements:
- What it is: Oral supplements can be recommended if dietary intake is insufficient or if there are malabsorption issues. Vitamin D supplements are often paired with calcium as they are synergistic.
- Pros: Ensures adequate intake, especially for those with dietary restrictions or absorption problems.
- Cons: Can have side effects (e.g., constipation), potential for overdose if not monitored, should be taken under medical guidance.
- Fluoride Treatments:
- What it is: Professional fluoride varnishes or gels applied in the dental office, or prescription fluoride toothpastes/rinses for home use, help strengthen enamel and enhance remineralization, making teeth more resistant to decay that might arise from weakened enamel due to deficiency.
- Pros: Direct strengthening of enamel, highly effective in cavity prevention.
- Cons: Not a substitute for adequate calcium intake; primarily addresses the symptom (weak enamel) rather than the underlying cause (systemic deficiency).
- Addressing Underlying Medical Conditions:
- What it is: If malabsorption or hormonal issues are contributing to calcium deficiency, managing these conditions with a physician is paramount.
- Pros: Addresses the root cause, leading to overall health improvement.
- Cons: May involve complex medical treatments.
Treatment for Gum Erosion (Recession)
Treatment for gum erosion depends on its severity and cause:
- Addressing Underlying Causes:
- What it is: This is the first step. If calculus is present, scaling and root planing are performed. If aggressive brushing is the cause, instruction on proper brushing technique and switching to a soft-bristled brush is essential. Treating bruxism with a nightguard may also be part of the plan.
- Pros: Prevents further recession, non-invasive initial approach.
- Cons: May not reverse existing recession.
- Desensitizing Agents/Bonding:
- What it is: For mild sensitivity caused by exposed roots, topical desensitizing varnishes or dental bonding (a tooth-colored resin material) can be applied to cover the exposed root surface and reduce sensitivity.
- Pros: Reduces discomfort, relatively inexpensive and quick.
- Cons: Does not address the underlying recession, may need reapplication.
- Gum Grafting:
- What it is: A surgical procedure where gum tissue is taken from another area of your mouth (e.g., the palate) or from a donor source and attached to the site of recession to cover the exposed root. Various techniques exist (e.g., connective tissue graft, free gingival graft, pedicle graft).
- Pros: Effectively covers exposed roots, reduces sensitivity, improves aesthetics, protects roots from decay, can stop further recession.
- Cons: Surgical procedure, involves a donor site (if autogenous graft), discomfort during healing, higher cost, potential for graft failure.
- Orthodontic Treatment:
- What it is: In cases where misaligned teeth or bite issues contribute to recession, orthodontic treatment may be recommended to correctly position the teeth, which can sometimes allow gums to heal or make grafting more successful.
- Pros: Corrects underlying bite problems, improves long-term stability.
- Cons: Long treatment duration, significant cost, potential for temporary discomfort.

Comparison Table: Key Dental Treatments for Calculus and Gum Disease
| Feature | Professional Dental Cleaning (Prophylaxis) | Scaling and Root Planing (Deep Cleaning) | Gum Grafting (for Recession) |
|---|---|---|---|
| Primary Goal | Preventative, remove supragingival plaque/calculus | Treat active gum disease, remove subgingival calculus, smooth roots | Cover exposed roots, prevent further recession, reduce sensitivity |
| Procedure Type | Non-invasive, routine | Non-surgical, therapeutic | Surgical |
| Anesthesia | Usually none, sometimes topical anesthetic | Local anesthesia for treated quadrants | Local anesthesia, sometimes sedation |
| Duration (per visit) | 30-60 minutes | 45-90 minutes (per quadrant), 1-4 visits | 1-2 hours (per site) |
| Recovery Time | Immediate, minor sensitivity | 1-3 days mild soreness/sensitivity | 1-2 weeks, discomfort, swelling |
| Average US Cost (out-of-pocket) | $75 - $200 (per visit) | $200 - $600 (per quadrant) | $600 - $2,500+ (per tooth/site) |
| Insurance Coverage | Often 100% covered (2x annually) | Typically 50-80% covered after deductible | Varies, 0-50% covered, depends on plan |
| Effectiveness | High for prevention and mild gingivitis | High for halting moderate-severe gum disease | High for treating recession and sensitivity |
| Risks/Side Effects | Minor bleeding, temporary sensitivity | Sensitivity, swelling, minor bleeding | Pain, swelling, bleeding, infection, graft failure, altered sensation |
Step-by-Step Process
Here's what to expect during a common treatment for calculus and related issues: Scaling and Root Planing.
Step-by-Step: Scaling and Root Planing (Deep Cleaning)
-
Initial Examination and Diagnosis:
- Your dentist or periodontist will thoroughly examine your gums and teeth, measuring the depth of periodontal pockets around each tooth with a small probe. X-rays may be taken to assess bone loss. They will discuss their findings and recommend scaling and root planing if signs of gum disease (gingivitis or periodontitis) are present, including significant calculus buildup below the gum line.
-
Anesthesia:
- Before the procedure begins, the hygienist or dentist will typically administer a local anesthetic to numb the specific area(s) of your mouth that will be treated. This ensures you remain comfortable throughout the process. This is usually done in quadrants (e.g., upper left, lower left) to allow for complete numbness and thorough cleaning over multiple appointments.
-
Scaling (Calculus Removal):
- The dental professional will use a combination of specialized instruments to remove plaque and calculus.
- Ultrasonic Scalers: These devices use high-frequency vibrations and a continuous stream of water to break down and wash away large deposits of calculus and plaque, both above and below the gum line. The water also helps flush out debris from the pockets.
- Hand Scalers and Curettes: After initial ultrasonic scaling, fine hand instruments are used to meticulously scrape away any remaining stubborn calculus deposits and smooth the tooth surfaces. These instruments allow for precise removal of even the smallest fragments of calculus from deep within the periodontal pockets.
- The dental professional will use a combination of specialized instruments to remove plaque and calculus.
-
Root Planing (Smoothing Root Surfaces):
- Once all calculus is removed, the focus shifts to root planing. The dental professional will carefully smooth the root surfaces of your teeth. This removes any remaining bacterial toxins, prevents new plaque and calculus from easily adhering, and encourages the gum tissue to reattach to the cleaner, smoother root surfaces. This step is crucial for reducing pocket depths and promoting gum healing.
-
Irrigation (Optional):
- After scaling and root planing, some practitioners may irrigate the treated pockets with an antimicrobial solution (like chlorhexidine) to further reduce bacteria.
-
Post-Procedure Instructions:
- You'll receive detailed instructions on how to care for your mouth following the procedure, including advice on managing sensitivity, discomfort, and maintaining excellent oral hygiene.
- A follow-up appointment is typically scheduled within 4-6 weeks to evaluate healing and re-measure pocket depths. Depending on your condition, ongoing "periodontal maintenance" cleanings (more frequent than routine cleanings) may be recommended.
Cost and Insurance
Understanding the financial aspect of dental treatments related to calculus, calcium deficiency, and gum erosion is essential for planning.

Average US Costs (Out-of-Pocket)
Dental procedure costs can vary significantly based on your geographic location (major cities typically cost more), the dentist's fees, the complexity of your case, and whether a specialist (e.g., periodontist) is involved.
- Routine Dental Cleaning (Prophylaxis - D1110):
- Low: $75
- Mid: $120 - $180
- High: $200
- Scaling and Root Planing (Deep Cleaning - D4341 per quadrant):
- Low: $200 per quadrant
- Mid: $300 - $500 per quadrant
- High: $600+ per quadrant
- Note: A full mouth deep cleaning (4 quadrants) could range from $800 to $2,400+.
- Periodontal Maintenance (D4910):
- Low: $100
- Mid: $150 - $250
- High: $300
- Note: These are follow-up cleanings after deep cleaning, usually every 3-4 months.
- Fluoride Treatment (D1206/D1208):
- Low: $20
- Mid: $35 - $50
- High: $70
- Dental Bonding (for recession/sensitivity - D2910/D2920):
- Low: $100 per tooth
- Mid: $150 - $300 per tooth
- High: $400+ per tooth
- Gum Grafting (D4270/D4271/D4273 per tooth/site):
- Low: $600 per tooth/site
- Mid: $1,000 - $1,800 per tooth/site
- High: $2,500+ per tooth/site
- Note: More complex procedures involving multiple teeth or advanced techniques will be at the higher end.
Insurance Coverage Details
Dental insurance can significantly reduce your out-of-pocket expenses, but coverage varies widely:
- Routine Cleanings: Most dental insurance plans offer 100% coverage for two routine cleanings per year, with no deductible or co-pay. This is a foundational benefit.
- Scaling and Root Planing (Deep Cleaning): This is usually classified as a "major" or "basic" procedure. Coverage typically ranges from 50% to 80% after you've met your annual deductible. Many plans have a waiting period (e.g., 6-12 months) before covering major procedures.
- Periodontal Maintenance: Coverage often falls between routine cleanings and deep cleanings, typically 80-100% after the deductible, but some plans may limit the number of times per year.
- Fluoride Treatments: Often covered at 100% for children up to a certain age (e.g., 14 or 16), and sometimes for adults at a lower percentage or if medically necessary.
- Gum Grafting: This is typically considered a "major" procedure and may have limited coverage, often 0-50%, depending on the plan's specifics and whether it's deemed medically necessary versus purely cosmetic. Many plans have an annual maximum benefit, which can quickly be reached with surgical procedures.
- Calcium/Vitamin D Supplements: These are generally considered medical expenses and are not covered by dental insurance. They may be covered by some medical insurance plans if prescribed by a physician for a diagnosed deficiency.
Pro Tip: Always check with your specific dental insurance provider about your plan's benefits, deductibles, co-pays, annual maximums, and any waiting periods before starting treatment. Many dental offices will help you verify your benefits.
Comparison Table: US Dental Treatment Costs & Insurance Coverage
| Procedure | Average Out-of-Pocket Cost (Range) | Typical Insurance Coverage | Annual Limit/Deductible Impact |
|---|---|---|---|
| Routine Cleaning | $75 - $200 | 100% (2x annually) | Usually exempt from deductible, no annual limit impact |
| Scaling & Root Planing (per quad) | $200 - $600 | 50-80% after deductible | Counts towards annual maximum, deductible applies |
| Periodontal Maintenance | $100 - $300 | 80-100% after deductible | Counts towards annual maximum, deductible may apply |
| Gum Grafting (per site) | $600 - $2,500+ | 0-50% (major procedure) | Significantly impacts annual maximum, deductible applies |
| Fluoride Treatment | $20 - $70 | 100% for children, 0-80% for adults | Minor impact, often covered without deductible |
Recovery and Aftercare
Proper recovery and diligent aftercare are crucial for the success of dental treatments and for preventing recurrence of issues.
After Professional Dental Cleaning (Prophylaxis)
- Immediate: You might experience a minor tingling sensation or temporary sensitivity, especially if you had significant calculus removed or if your gums were inflamed.
- Home Care: Resume your normal oral hygiene routine immediately: brush twice daily with fluoride toothpaste and floss once daily.
- Diet: No specific dietary restrictions, but avoid extremely hot or cold foods if you experience sensitivity.
- Follow-up: Adhere to your dentist's recommendation for your next routine cleaning, typically in six months.
After Scaling and Root Planing (Deep Cleaning)
The recovery for deep cleaning is more involved:
- Pain and Discomfort: Expect some soreness, tenderness, and mild pain in your gums for a few days to a week. Over-the-counter pain relievers (e.g., ibuprofen, acetaminophen) can help manage discomfort. Your dentist might prescribe a stronger pain medication in some cases.
- Sensitivity: Increased tooth sensitivity to hot, cold, or sweets is common as root surfaces are exposed and gums heal. This usually subsides within a few weeks. Your dentist may recommend a desensitizing toothpaste or fluoride rinse.
- Swelling and Bleeding: Gums may be slightly swollen and might bleed a little during brushing or flossing for the first few days. This is normal and a sign of healing.
- Diet: For the first 24-48 hours, stick to soft, lukewarm foods. Avoid hard, crunchy, sticky, or spicy foods. Chew on the opposite side of your mouth if only one side was treated. Avoid alcohol and smoking.
- Oral Hygiene:
- Continue gentle brushing with a soft-bristled toothbrush. Avoid directly scrubbing the treated areas too vigorously initially.
- Rinse your mouth with warm salt water (1/2 teaspoon salt in 8 ounces warm water) several times a day to aid healing and reduce swelling.
- Your dentist might prescribe an antimicrobial mouth rinse (like chlorhexidine) for a short period (e.g., 1-2 weeks). Use as directed.
- Resume flossing gently as soon as comfortable, focusing on not irritating the healing gums.
- Follow-up: Attend all scheduled follow-up appointments. These are critical for assessing healing, measuring pocket depths, and planning ongoing periodontal maintenance cleanings, typically every 3-4 months.
After Gum Grafting
Gum grafting involves surgical recovery:
- Pain and Swelling: You will likely experience moderate pain, swelling, and possibly bruising at both the graft site and the donor site (if tissue was taken from your palate). Your dentist will prescribe pain medication. Ice packs applied to the outside of your face can help reduce swelling.
- Bleeding: Minor oozing or bleeding from the surgical sites is common for the first 24-48 hours.
- Diet: A soft diet is essential for at least 1-2 weeks. Avoid crunchy, chewy, or hot foods. Do not use a straw as the suction can dislodge the graft.
- Oral Hygiene:
- Avoid brushing or flossing the surgical site directly for the recommended period (usually 1-2 weeks).
- You will be given a special antimicrobial mouth rinse (e.g., chlorhexidine) to use instead of brushing in the surgical area. Use it gently.
- Maintain normal brushing and flossing in non-surgical areas.
- Activity: Avoid strenuous activity for the first few days.
- Smoking/Alcohol: Absolutely avoid smoking and alcohol, as they significantly impair healing and can lead to graft failure.
- Follow-up: Multiple follow-up appointments will be necessary to monitor healing, remove sutures (if non-dissolvable), and ensure the graft is successful. The full healing process can take several weeks to months.
Pro Tip: Always follow your dental professional's specific post-operative instructions meticulously. They are tailored to your individual procedure and will optimize your healing and the long-term success of the treatment.
Prevention
Preventing calculus buildup, protecting against calcium deficiency issues, and preventing gum erosion are paramount for lifelong oral health.
Preventing Calculus Buildup
- Effective Brushing:
- Brush at least twice a day for two minutes each time, using a soft-bristled toothbrush and fluoride toothpaste.
- Use the Bass method: Hold your toothbrush at a 45-degree angle to the gum line, gently move it back and forth in short, tooth-wide strokes. Brush all surfaces of every tooth.
- Replace your toothbrush every 3-4 months, or sooner if the bristles are frayed.
- Consider an electric toothbrush, which can be more effective at removing plaque than manual brushing.
- Daily Flossing:
- Floss at least once a day to remove plaque and food particles from between your teeth and under the gum line, where your toothbrush can't reach. This is critical for preventing subgingival calculus.
- Use about 18 inches of floss, wrapping most of it around your middle fingers. Guide the floss between your teeth, forming a "C" shape against each tooth, and gently slide it under the gum line.
- Regular Dental Check-ups and Cleanings:
- Visit your dentist for professional cleanings and check-ups typically every six months. Your dental hygienist will remove any plaque and calculus that you've missed, preventing it from causing further damage. For those prone to calculus or gum disease, more frequent cleanings (e.g., every 3-4 months) may be recommended.
- Antimicrobial Mouthwash (Optional):
- A therapeutic mouthwash (containing ingredients like cetylpyridinium chloride or essential oils) can help reduce plaque bacteria, but it's an adjunct, not a replacement, for brushing and flossing.
- Healthy Diet:
- Limit sugary snacks and drinks, as sugar feeds the bacteria in plaque.
- Avoid excessive consumption of highly acidic foods and beverages that can weaken enamel.
- Quit Smoking/Tobacco:
- Smoking is a major risk factor for calculus and gum disease. Quitting is one of the best things you can do for your oral and overall health.
Preventing Calcium Deficiency Teeth
- Calcium-Rich Diet:
- Ensure your diet includes adequate sources of calcium. The Recommended Dietary Allowance (RDA) for most adults is 1,000 mg per day, increasing to 1,200 mg for women over 50 and men over 70.
- Excellent sources include dairy products (milk, yogurt, cheese), fortified plant milks (almond, soy, oat milk), leafy green vegetables (kale, collard greens), fortified cereals, and canned sardines with bones.
- Adequate Vitamin D Intake:
- Vitamin D is essential for calcium absorption. Spend time in the sun (10-15 minutes most days) or consume vitamin D-rich foods like fatty fish (salmon, tuna), fortified milk and cereals, and eggs.
- The RDA for Vitamin D is generally 600-800 IU per day for adults.
- Calcium and Vitamin D Supplements (If Needed):
- If you can't get enough from diet and sun exposure, consult your doctor or dentist about appropriate calcium and vitamin D supplements. Do not self-prescribe high doses.
- Fluoride Use:
- Use fluoride toothpaste and consider fluoride mouthwash if recommended by your dentist. Fluoride strengthens enamel and enhances remineralization, making teeth more resilient even if calcium intake is marginally low.
- Regular Dental Check-ups:
- Your dentist can monitor the strength of your enamel and identify early signs of demineralization or increased cavity risk that might be related to calcium or other nutritional deficiencies.
Preventing Gum Erosion (Recession)
- Correct Brushing Technique:
- Use a soft-bristled toothbrush and a gentle, circular, or Bass method brushing technique. Avoid scrubbing horizontally or aggressively.
- Daily Flossing:
- Proper flossing removes plaque from below the gum line, preventing the inflammation and calculus that can lead to recession.
- Treat Periodontal Disease:
- Regular dental cleanings and addressing gum disease with scaling and root planing are vital to prevent calculus from driving recession.
- Address Bruxism (Clenching/Grinding):
- If you clench or grind your teeth, your dentist might recommend a nightguard to protect your teeth and gums from excessive forces.
- Avoid Tobacco Products:
- Tobacco use is a major risk factor for gum disease and recession.
- Monitor Oral Piercings:
- If you have oral piercings, be vigilant about their contact with gum tissue. Consider removing them if they are causing irritation or recession.
- Correct Orthodontic Issues:
- If misaligned teeth are contributing to gum issues, discuss orthodontic treatment with your dentist or orthodontist.
- Regular Dental Check-ups:
- Your dentist can identify early signs of recession and help determine the cause, allowing for timely intervention.
Risks and Complications
Failing to address calcium-related dental issues, whether it's excessive buildup or deficiency, carries significant risks and potential complications for your oral and overall health.
Risks and Complications of Untreated Calculus (Tartar) Buildup
Untreated calculus is a primary driver of periodontal disease, which has far-reaching consequences:
- Gingivitis: This is the earliest stage of gum disease, characterized by red, swollen, tender, and bleeding gums. Calculus provides a rough surface for bacteria to thrive, causing this inflammation. If only gingivitis is present, it is reversible with professional cleaning and good home care.
- Periodontitis: If gingivitis is left untreated, the inflammation progresses. Bacteria and their toxins, trapped by subgingival calculus, start to destroy the connective tissues and bone that support your teeth. This leads to the formation of deeper periodontal pockets, further gum recession, and irreversible bone loss.
- Gum Erosion (Recession): As the supporting bone and gum tissue are destroyed by periodontitis, the gums pull away from the teeth, exposing the tooth roots. This leads to increased sensitivity, aesthetic concerns, and makes the roots vulnerable to decay.
- Tooth Sensitivity: Exposed tooth roots due to recession lack the protective enamel layer and are highly sensitive to temperature changes and touch.
- Tooth Mobility and Loss: As bone loss progresses, teeth lose their anchor and can become loose. Eventually, they may need to be extracted or fall out on their own.
- Dental Caries (Cavities): Calculus's rough surface traps food debris and plaque bacteria, increasing the risk of cavities on both the enamel and the exposed root surfaces.
- Halitosis (Chronic Bad Breath): The bacteria thriving in calculus and periodontal pockets produce foul-smelling gases, leading to persistent bad breath.
- Systemic Health Impacts: Periodontal disease has been linked to several systemic health conditions, including increased risk of heart disease, stroke, diabetes complications, respiratory diseases, and adverse pregnancy outcomes. The chronic inflammation and bacterial load in the mouth can affect other parts of the body.
Risks and Complications of Calcium Deficiency Teeth
While calculus is about excess mineral on teeth, a lack of calcium in the body can lead to its own set of problems:
- Weakened Enamel: Especially during tooth development, insufficient calcium can lead to hypocalcified or hypoplastic enamel, which is weaker, softer, and more prone to acid erosion and decay.
- Increased Susceptibility to Cavities: Weak enamel provides less resistance to the acids produced by plaque bacteria, leading to a higher incidence and faster progression of cavities.
- Brittle Teeth: In severe cases, teeth may be more fragile and prone to chipping or fracturing.
- Jawbone Loss (Alveolar Bone): Long-term, severe calcium deficiency can contribute to reduced bone density in the jaw, potentially weakening the support for teeth and increasing the risk of tooth mobility and loss, particularly in the context of osteoporosis.
- Impaired Tooth Development: In children, severe calcium deficiency can lead to delays in tooth eruption and abnormal tooth morphology.
- Overall Skeletal Health Issues: Calcium deficiency directly impacts bone density throughout the body, leading to osteopenia and osteoporosis, increasing the risk of fractures. Oral manifestations are often a reflection of systemic issues.
Risks and Complications of Treatment
While treatments are generally safe and effective, like any medical procedure, they carry some potential risks:
- Professional Dental Cleaning: Very low risk. Temporary sensitivity, minor gum bleeding.
- Scaling and Root Planing:
- Increased Sensitivity: Common after treatment as roots are exposed. Usually temporary, but can be persistent.
- Gum Recession: While deep cleaning aims to reduce inflammation, some gum recession may occur as swollen gums shrink back, which can further expose roots.
- Infection: Rare, but possible if bacteria enter the bloodstream (prophylactic antibiotics may be given to at-risk patients).
- Discomfort/Pain: Mild to moderate, managed with pain relievers.
- Gum Grafting:
- Pain and Swelling: Significant discomfort, swelling, and bruising are common after surgery, especially at the donor site.
- Infection: A risk with any surgery.
- Graft Failure: The graft may not take successfully, requiring a repeat procedure.
- Altered Sensation: Temporary or, rarely, permanent numbness or altered sensation in the surgical area or donor site.
- Unsatisfactory Aesthetics: While often performed for aesthetics, the outcome may not always perfectly match expectations.
Children / Pediatric Considerations
Calcium's role in children's dental health is particularly critical, as their teeth are still developing and highly susceptible to both deficiency and early calculus formation.
Calcium's Role in Developing Teeth
- Enamel and Dentin Formation: During infancy and early childhood, a continuous and adequate supply of calcium, phosphate, and vitamin D is absolutely essential for the proper mineralization of both primary (baby) and permanent teeth. This process, called odontogenesis, determines the strength, hardness, and acid resistance of the enamel and dentin.
- Hypocalcification/Hypoplasia: If a child experiences severe calcium or vitamin D deficiency, or other nutritional deficiencies, illness, or trauma during specific periods of tooth development, the enamel can form improperly. This can lead to conditions like enamel hypocalcification (enamel is soft and poorly mineralized) or hypoplasia (enamel is thin or pitted). Such teeth are extremely vulnerable to cavities, even with good oral hygiene, and may appear chalky, mottled, or discolored.
- Jawbone Development: Calcium is also crucial for the healthy development and density of the jawbones, which support the teeth.
Preventing Calcium Deficiency in Children
- Balanced Diet: Ensure children consume a diet rich in calcium and vitamin D.
- Dairy: Milk, yogurt, and cheese are excellent sources.
- Fortified Foods: Many cereals, orange juices, and plant-based milks are fortified with calcium and vitamin D.
- Leafy Greens: Spinach and kale (though absorption can be less than from dairy).
- Vitamin D: Encourage safe sun exposure and include vitamin D-rich foods. Many pediatricians recommend vitamin D supplements for infants and young children, especially those who are breastfed.
- Regular Pediatric Dental Visits: Pediatric dentists can monitor tooth development, identify early signs of enamel defects, and provide guidance on diet and fluoride use.
- Fluoride: While not calcium, fluoride works synergistically with calcium to strengthen developing and erupted enamel. Children should use fluoride toothpaste (rice-grain amount for under 3, pea-sized for 3-6) and may benefit from professional fluoride varnishes.
Calculus in Children
While less common than in adults, children can develop calculus:
- Causes: Similar to adults, poor oral hygiene (especially if not brushing effectively around erupting teeth or orthodontic appliances), diet, and salivary composition can contribute. Some children with certain medical conditions or medications that cause dry mouth may be at higher risk.
- Signs: Parents might notice yellow or brown deposits near the gum line, particularly on the lower front teeth or upper molars. Red, swollen, or bleeding gums can also indicate gingivitis due to plaque and calculus.
- Prevention: The same principles apply: diligent brushing and flossing from an early age, regular dental check-ups, and professional cleanings. Parents should actively help younger children brush and supervise older children until they develop the dexterity for effective cleaning (around age 7-8).
- Treatment: Professional dental cleanings are necessary to remove calculus in children.
Pro Tip: Early education on oral hygiene and a balanced diet lays the foundation for a lifetime of healthy smiles. Pediatric dentists are invaluable resources for parents navigating these crucial developmental years.
Cost Breakdown
A detailed look at the financial implications of managing calcium on teeth issues, with practical tips for affordability.

Average US Costs (Low, Mid, High) for Key Treatments
| Procedure | Low Range (USD) | Mid Range (USD) | High Range (USD) |
|---|---|---|---|
| Routine Cleaning (Prophylaxis) | $75 | $120 - $180 | $200 |
| Scaling & Root Planing (per quadrant) | $200 | $300 - $500 | $600 |
| Full Mouth Scaling & Root Planing (4 quadrants) | $800 | $1,200 - $2,000 | $2,400 |
| Periodontal Maintenance (per visit) | $100 | $150 - $250 | $300 |
| Fluoride Treatment | $20 | $35 - $50 | $70 |
| Dental Bonding (per tooth for recession) | $100 | $150 - $300 | $400 |
| Gum Grafting (per site) | $600 | $1,000 - $1,800 | $2,500+ |
These are cash prices without insurance. Costs can be higher in metropolitan areas or with specialists.
With vs. Without Insurance
- Without Insurance (Cash Price): You pay the full amount as listed above. Many dentists offer a discount (e.g., 5-10%) for patients who pay in full at the time of service.
- With Insurance:
- Routine Cleanings: Usually covered at 100% (typically 2 per year) with no deductible.
- Scaling & Root Planing / Periodontal Maintenance: Often covered at 50-80% after your deductible is met. If your deductible is $500 and your deep cleaning is $1,600, you'd pay $500 + 20-50% of the remaining $1,100, totaling $720-$1,050. This counts toward your annual maximum.
- Gum Grafting: Coverage varies significantly, from 0% to 50%. It often falls under "major procedures" and will be subject to your deductible and annual maximum. It's common for a single gum graft to exceed an annual maximum (e.g., $1,500-$2,000).
Payment Plans and Financing Options
If you don't have insurance or face high out-of-pocket costs, several options can help:
- In-Office Payment Plans: Many dental offices offer flexible payment arrangements, allowing you to pay in installments.
- Third-Party Financing (e.g., CareCredit, LendingClub): These are healthcare credit cards or loans with various interest rates, including promotional periods of 0% APR if paid in full within a certain timeframe (e.g., 6, 12, or 18 months).
- Dental Savings Plans: These are not insurance but membership plans where you pay an annual fee and receive discounts (typically 10-60%) on dental services from participating providers.
- Health Savings Accounts (HSAs) / Flexible Spending Accounts (FSAs): If you have an HSA or FSA through your employer, you can use these tax-advantaged accounts to pay for qualified dental expenses.
- Dental Schools: University dental schools often provide services at a reduced cost, as students perform the work under the close supervision of experienced faculty.
Cost-Saving Tips
- Prioritize Prevention: The best way to save money is to avoid expensive treatments. Regular brushing, flossing, and routine check-ups are the most cost-effective strategies.
- Utilize Insurance Benefits: Maximize your annual cleaning benefits. If you have deep cleaning or other major work, understand your annual maximum and deductible.
- Compare Costs: Don't hesitate to call multiple dental offices and ask for estimates.
- Negotiate: For extensive work without insurance, ask if the office offers a cash discount.
- Address Issues Early: Small problems are always cheaper and easier to fix than big ones. Don't delay treatment for calculus or gum issues.
- Consider Dental Savings Plans: If you don't have insurance, these plans can offer significant discounts.
Frequently Asked Questions
Is "calcium on teeth" good or bad?
"Calcium on teeth" can be both good and bad, depending on the context. Calcium in your teeth is essential for strength and hardness. Calcium from saliva helps remineralize (repair) early enamel damage, which is beneficial. However, when plaque hardens into calculus (tartar) due to mineral deposits, that's "calcium on teeth" in a detrimental way, leading to gum disease and other problems.
Can I remove calculus (tartar) at home?
No, once plaque has hardened into calculus, it adheres firmly to the tooth surface and cannot be removed by brushing, flossing, or over-the-counter products. Only a dental professional using specialized instruments (scalers) can safely and effectively remove calculus. Attempting to scrape it off yourself can damage your enamel and gums.
What are the main signs of calcium deficiency affecting teeth?
The main signs of calcium deficiency affecting teeth include weakened enamel (making teeth more prone to cavities), increased susceptibility to chipping or fractures, and in severe cases during childhood development, enamel defects like pits or grooves (hypoplasia). It can also indirectly contribute to jawbone density issues over time.
How does gum erosion relate to "calcium on teeth"?
Gum erosion (recession) is strongly related to "calcium on teeth" in the form of calculus. Calculus buildup, particularly below the gum line, traps bacteria that cause inflammation and infection (periodontal disease). This inflammation progressively destroys the gum tissue and supporting bone, causing the gums to pull back or erode from the tooth surface.
How often should I get a professional cleaning to prevent calculus?
The American Dental Association generally recommends professional dental cleanings and check-ups every six months for most individuals. However, if you are prone to heavy calculus buildup, have active gum disease, or other risk factors, your dentist may recommend more frequent cleanings, such as every three or four months.
Is deep cleaning (scaling and root planing) painful?
Deep cleaning is typically performed under local anesthesia, so you should not feel pain during the procedure itself. Some discomfort, soreness, and sensitivity are common after the anesthesia wears off, usually lasting for a few days to a week. Over-the-counter pain relievers and desensitizing toothpastes can help manage these symptoms.
What is the typical cost of a gum graft to treat severe gum erosion?
The cost of gum grafting in the US typically ranges from $600 to $2,500 or more per tooth/site without insurance. This variation depends on the type of graft, the complexity of the case, and the dental professional's fees. Insurance coverage for gum grafts can also vary significantly.
Can diet alone reverse gum erosion?
No, diet alone cannot reverse existing gum erosion. While a healthy, balanced diet rich in essential nutrients supports gum health and overall healing, it cannot regenerate lost gum tissue or bone. Professional dental treatments, such as scaling and root planing to address gum disease, or gum grafting for severe recession, are required.
How long does it take for calculus to form?
Plaque starts to mineralize into calculus fairly quickly. If not removed, soft plaque can begin to harden within 24 to 72 hours. The longer plaque remains on your teeth, the more firmly it adheres and the harder it becomes, eventually turning into calculus.
Are there any home remedies for removing calcium buildup on teeth?
There are no safe or effective home remedies for removing hardened calculus. Products marketed as "tartar removers" for home use are ineffective at removing established calculus and can potentially damage your enamel or gums. Professional dental cleaning is the only medically recommended method.
When to See a Dentist
It's crucial to know when to seek professional dental attention to address issues related to calcium on teeth, gum erosion, and potential deficiencies. Delaying care can lead to more severe problems and more complex, costly treatments.
Routine Care Guidance:
- Regular Check-ups: Schedule a dental check-up and professional cleaning every six months, or as recommended by your dentist. These routine visits are essential for preventing calculus buildup, detecting early signs of gum disease, and monitoring overall oral health.
Clear Warning Signs That Need Attention:
You should make an appointment with your dentist as soon as possible if you notice any of the following signs, which could indicate calculus buildup, gum erosion, or progressing gum disease:
- Visible Hard Deposits: If you can see yellowish, brownish, or dark deposits on your teeth, especially near the gum line.
- Persistent Bad Breath: If you have chronic bad breath that doesn't improve with regular brushing and flossing.
- Red, Swollen, or Tender Gums: Gums that are inflamed, puffy, or painful to the touch.
- Bleeding Gums: If your gums bleed easily when you brush, floss, or even eat. This is a primary sign of gingivitis, often exacerbated by calculus.
- Receding Gums or "Longer-Looking" Teeth: If you notice your gum line pulling away from your teeth, exposing more of the root surface.
- Increased Tooth Sensitivity: Especially if this is a new symptom or has worsened, indicating potential root exposure from gum erosion.
- Loose Teeth: If any of your permanent teeth feel wobbly or appear to be shifting. This is a sign of advanced gum disease and significant bone loss.
- Changes in Your Bite: If your teeth no longer fit together comfortably when you bite down, or if you notice changes in the way your dentures fit.
- Pain or Discomfort: Any persistent toothache, gum pain, or discomfort when chewing.
- Rough Spots on Teeth: If you can feel rough, gritty areas on your tooth surfaces with your tongue, which could indicate plaque or early calculus.
Emergency vs. Scheduled Appointment Guidance:
- Scheduled Appointment: Most of the warning signs listed above warrant a prompt, scheduled dental appointment. It's usually not an emergency, but timely intervention is important to prevent the condition from worsening. Call your dentist's office as soon as you notice these issues.
- Emergency Appointment: Seek immediate dental care if you experience:
- Severe, unmanageable pain that over-the-counter medications don't touch.
- Sudden, uncontrolled bleeding from your gums.
- Rapidly spreading infection, characterized by significant swelling in your face or jaw, fever, or difficulty swallowing/breathing. These could indicate an abscess and require urgent attention.
- Acute trauma to your teeth or gums (e.g., a knocked-out tooth, severe fracture).
Pro Tip: Don't wait for pain to be your indicator. Many serious dental problems, like gum disease, can progress without significant pain in their early stages. Regular check-ups and being proactive about minor symptoms are your best defense.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

What Are Calcium Deposits on Teeth
Are you one of the millions of Americans who notices a stubborn, yellowish buildup on your teeth despite regular brushing? You're likely experiencing what many refer to as "calcium deposits on teeth." This common dental concern, medically known as dental calculus or tartar, affects a vast ma
February 23, 2026

Calcium Good for Teeth: Complete Guide
More than 99% of your body's calcium resides in your bones and teeth, making it an undeniable cornerstone of skeletal and oral health. But did you know that an estimated 42% of American adults don't get enough calcium from their diet? This staggering statistic underscores a critical question
February 23, 2026

What Do Bulimia Teeth Look Like
"Bulimia teeth" refers to the specific and often severe damage that the self-induced vomiting characteristic of bulimia nervosa inflicts on a person's oral health. It's a critical issue, affecting approximately 1.5% of women and 0.5% of men in the US at some point in their lives, with many more
February 23, 2026

Erosion in Teeth: Complete Guide
Erosion in Teeth: Complete Guide
February 23, 2026