What Do Bulimia Teeth Look Like

Key Takeaways
- "Bulimia teeth" refers to the specific and often severe damage that the self-induced vomiting characteristic of bulimia nervosa inflicts on a person's oral health. It's a critical issue, affecting approximately 1.5% of women and 0.5% of men in the US at some point in their lives, with many more
"Bulimia teeth" refers to the specific and often severe damage that the self-induced vomiting characteristic of bulimia nervosa inflicts on a person's oral health. It's a critical issue, affecting approximately 1.5% of women and 0.5% of men in the US at some point in their lives, with many more experiencing subclinical forms. This condition, an eating disorder marked by cycles of binging and purging, exposes teeth to highly corrosive stomach acid, leading to irreversible changes that are not only physically painful but also profoundly impact self-esteem and overall quality of life. Understanding what do bulimia teeth look like is the first step toward recognizing the signs, seeking help for the underlying disorder, and mitigating the significant dental damage that ensues. This article will delve into the precise mechanisms of this damage, detailing the visible signs, potential treatments, preventative measures, and crucial considerations for recovery.
Key Takeaways:
- Distinctive Dental Erosion: The most prominent sign of bulimia is perimylolysis – smooth, rounded erosion on the inner surfaces of teeth, particularly the upper front teeth, caused by stomach acid.
- Increased Sensitivity & Pain: Eroded enamel exposes the sensitive dentin layer, leading to heightened pain from hot, cold, or sweet foods and drinks.
- Restorative Treatments are Costly: Repairing bulimia-related dental damage can range from $200 for a single bonding to $2,500+ per tooth for veneers or crowns, potentially totaling tens of thousands of dollars for a full mouth restoration.
- Irreversible Enamel Loss: Enamel, once eroded by acid, cannot regenerate. Dental treatments focus on protecting remaining tooth structure and restoring appearance and function.
- Underlying Disorder Treatment is Paramount: While dental interventions are crucial, sustained oral health recovery depends entirely on addressing the bulimia nervosa itself through psychological and medical support.
- Long-Term Oral Care is Essential: After treatment, diligent oral hygiene, specialized fluoride therapies, and regular dental check-ups (every 3-4 months initially) are vital for maintaining dental health.
- Insurance Coverage Varies: Many cosmetic and restorative procedures may not be fully covered by standard dental insurance, which typically caps benefits at $1,000-$2,000 per year. Comprehensive care for severe damage often requires out-of-pocket payment or specialized financing.
What It Is / Overview: Understanding Bulimia Nervosa's Dental Impact
Bulimia nervosa is an eating disorder characterized by recurrent episodes of binge eating followed by compensatory behaviors, most commonly self-induced vomiting (purging). While the psychological and systemic health impacts are severe, the oral cavity bears some of the most visible and direct consequences. When stomach acid, with its incredibly low pH (typically between 1.5 and 3.5), repeatedly washes over the teeth during vomiting, it initiates a process known as dental erosion. This is a chemical dissolution of the tooth structure, primarily enamel, without bacterial involvement (unlike cavities).
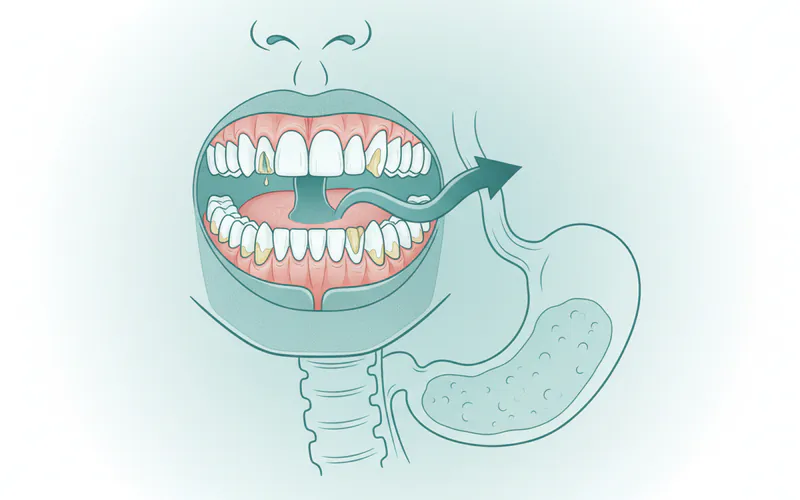
Unlike damage from acidic foods or drinks, which often affects the outer surfaces of teeth, bulimia-induced erosion is distinctive because it primarily affects the lingual (tongue-side) and palatal (roof of the mouth-side) surfaces of the upper front teeth and, less commonly, the chewing surfaces of molars. The repetitive exposure to gastric acid gradually demineralizes the enamel, leading to a host of structural and aesthetic problems that become progressively worse over time if the purging behavior continues. The term "bulimia teeth" encapsulates this constellation of dental issues, serving as a significant diagnostic marker for the disorder.
Types / Variations: Methods of Purging and Their Dental Effects
While self-induced vomiting is the most common purging behavior leading to dental erosion, other methods can also contribute to oral health problems or exacerbate existing damage.
- Self-Induced Vomiting (The Primary Culprit): This is the main focus when discussing "what do bulimia teeth look like." The direct contact of highly acidic stomach contents with tooth surfaces leads to perimylolysis. This erosion pattern is so characteristic that dentists are often the first healthcare professionals to suspect an eating disorder.
- Laxative Abuse: While laxatives do not directly expose teeth to stomach acid, their chronic use can lead to severe dehydration and electrolyte imbalances. Dehydration contributes to xerostomia (dry mouth) and reduces saliva's protective buffering capacity, indirectly increasing the risk of tooth decay and gum disease.
- Diuretic Abuse: Similar to laxative abuse, diuretics can cause dehydration and dry mouth, diminishing saliva's protective role and making teeth more vulnerable to acid attacks from other sources (e.g., acidic foods/drinks, or even undiagnosed acid reflux, which can occur comorbidly).
- Excessive Exercise: While not directly causing dental damage, this compensatory behavior can also lead to dehydration if fluid intake isn't sufficient, contributing to dry mouth.
It's crucial to understand that while other purging methods contribute to general oral health decline, self-induced vomiting is overwhelmingly responsible for the specific and severe erosive patterns seen in bulimia teeth.
Causes / Why It Happens: The Mechanism of Acid Erosion
The underlying cause of dental damage in bulimia is the repeated exposure of teeth to gastric acid. This happens primarily through self-induced vomiting. Here's a breakdown of the mechanism:
- Stomach Acid: The human stomach produces hydrochloric acid (HCl) to aid digestion. This acid is extremely potent, with a pH of 1.5-3.5, designed to break down food.
- Contact with Teeth: During vomiting, this acid-rich chyme is propelled from the stomach, through the esophagus, and into the mouth, washing over the tooth surfaces. The back-and-forth motion can also contribute to erosion.
- Demineralization: Tooth enamel, the hardest substance in the human body, is primarily composed of hydroxyapatite crystals. These crystals are highly susceptible to dissolution by acid. When the pH in the mouth drops below a critical level (approximately 5.5 for enamel, 6.2 for dentin), calcium and phosphate ions begin to leach out of the enamel structure.
- Saliva's Role (and Limitations): Saliva is the body's natural defense against acid. It contains bicarbonate and other buffers that neutralize acids, as well as calcium and phosphate ions that can help remineralize early enamel lesions. However, with repeated and prolonged exposure to strong stomach acid, saliva's buffering capacity is overwhelmed.
- Irreversible Loss: Over time, with consistent exposure, the enamel is progressively worn away, a process known as perimylolysis when the pattern is characteristic of intrinsic acid erosion. This loss is irreversible because adult enamel cannot regenerate. Once the enamel is gone, the underlying dentin, which is softer and more porous, becomes exposed and erodes even more rapidly.
Beyond the direct acid attack, other factors contribute:
- Brushing after Vomiting: A common, yet detrimental, instinct is to brush immediately after vomiting. While well-intentioned, brushing teeth when the enamel has been softened by acid can physically abrade the weakened tooth surface, accelerating enamel loss.
- Dry Mouth (Xerostomia): Bulimia can lead to dehydration and salivary gland dysfunction (sialadenosis), resulting in dry mouth. Reduced saliva means less natural buffering and remineralization, making teeth more vulnerable to acid and increasing the risk of cavities and gum disease.
- Dietary Habits: Individuals with bulimia may also consume large amounts of sugary and acidic foods during binge episodes, further compounding the damage.
Signs and Symptoms: What Do Bulimia Teeth Look Like?
Recognizing the signs of bulimia in the oral cavity is crucial for early intervention. The dental manifestations are often characteristic and can progress from subtle changes to severe, widespread damage.
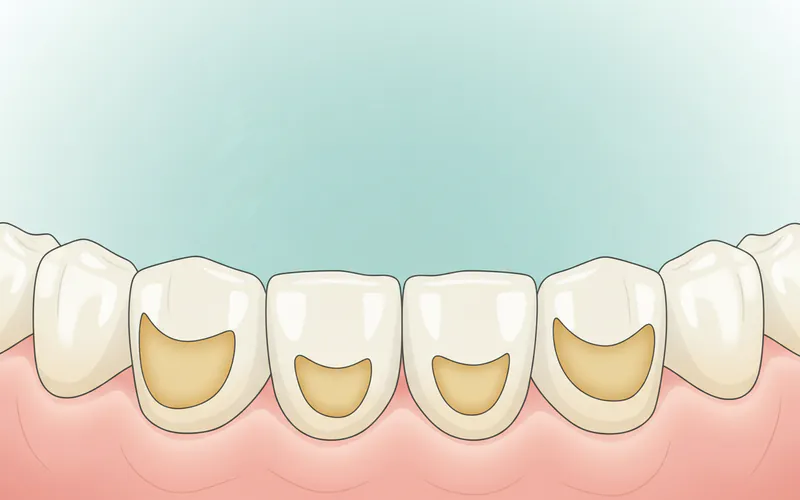
1. Dental Erosion (Perimylolysis)
This is the hallmark sign and answers directly "what do bulimia teeth look like."
- Location: Primarily affects the lingual (tongue-side) and palatal (roof of the mouth-side) surfaces of the upper front teeth. The acid flows over these surfaces as it exits the mouth. The chewing (occlusal) surfaces of molars can also be affected, developing a "scooped out" or "cupped" appearance around existing fillings.
- Appearance: Enamel appears smooth, shiny, and highly polished, often described as a "frosted glass" look in early stages. As erosion progresses, the enamel thins, becoming translucent, especially at the biting edges.
- Loss of Tooth Anatomy: The natural contours and cusps of teeth become flattened or rounded.
- "Cupping" of Fillings: Amalgam (silver) fillings may appear to stand proud or be higher than the surrounding tooth structure. This isn't because the filling grew, but because the enamel and dentin around it have eroded away.
2. Increased Tooth Sensitivity
- As enamel erodes, the underlying dentin, which contains microscopic tubules leading to the tooth's pulp, becomes exposed. This exposure leads to heightened sensitivity, particularly to:
- Hot and cold temperatures.
- Sweet and acidic foods/drinks.
- Air exposure.
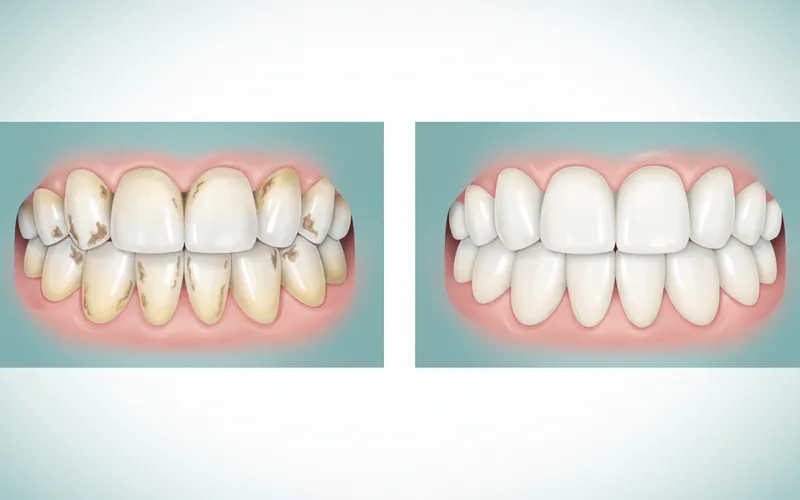
3. Changes in Tooth Color and Translucency
- Yellowing: When the white enamel layer is worn away, the yellowish dentin underneath becomes more visible, making the teeth appear discolored or yellow.
- Translucency: Thinning enamel can make the biting edges of front teeth appear glass-like or translucent.
4. Chipping and Fractures
- Eroded enamel weakens the overall tooth structure. Teeth become more brittle and susceptible to chipping, particularly on the biting edges of front teeth, or even stress fractures.
- Restorations (fillings, crowns) may also fracture or come loose due to the weakening of the surrounding tooth.
5. Altered Occlusion (Bite) and Tooth Length
- Significant enamel loss can actually shorten the clinical crowns of the teeth, altering the bite. This can lead to issues with chewing efficiency and even temporomandibular joint (TMJ) problems.
6. Dental Caries (Cavities)
- While erosion is non-bacterial, the reduction in saliva, compromised enamel, and often a diet high in fermentable carbohydrates during binges, make individuals more prone to traditional cavities. These often appear at the gumline (cervical caries) or on surfaces where acid has already weakened the enamel.
- Pro Tip: Even though bulimia causes erosion, the risk of traditional cavities remains high. Regular fluoride exposure and meticulous oral hygiene are vital.
7. Oral Mucosal Lesions
- The acidic environment can irritate and inflame the soft tissues of the mouth, leading to:
- Sore throat and hoarseness.
- Dry, cracked lips.
- Redness and inflammation of the palate and pharynx.
- Oral candidiasis (yeast infections) due to dry mouth and altered oral flora.
8. Xerostomia (Dry Mouth)
- Chronic dehydration, salivary gland dysfunction, and some medications used to treat eating disorders can lead to a persistent dry mouth. Symptoms include:
- Difficulty speaking, swallowing, and eating.
- A sticky, dry feeling in the mouth.
- Bad breath (halitosis).
- Increased risk of cavities and gum disease due to reduced salivary flow and buffering capacity.
9. Sialadenosis (Salivary Gland Enlargement)
- Repeated vomiting can lead to the painless, non-inflammatory enlargement of the parotid (and sometimes submandibular) salivary glands. This often manifests as noticeable swelling in the cheeks, giving a "chipmunk-like" appearance. This swelling can be a significant indicator to a dental professional.
10. Temporomandibular Joint (TMJ) Issues
- Changes in bite due to tooth wear can put strain on the TMJ, leading to:
- Jaw pain or tenderness.
- Difficulty chewing.
- Clicking or popping sounds in the jaw.
- Headaches or earaches.
11. Periodontal Disease (Gum Disease)
- While not directly caused by acid, the overall compromised oral health, dry mouth, and potential for poor oral hygiene due to psychological distress can increase the risk of gingivitis (gum inflammation) and periodontitis (more severe gum disease with bone loss).
Treatment Options: Restoring and Protecting Bulimia-Affected Teeth
Addressing bulimia-affected teeth requires a multi-faceted approach, prioritizing the cessation of purging behaviors as the foundation for any successful dental intervention. Dental treatments aim to protect existing tooth structure, alleviate symptoms, and restore aesthetics and function.
1. Addressing the Underlying Eating Disorder (Crucial First Step)
- Pros: Absolutely essential for long-term dental health. No dental treatment will be successful or durable if purging continues. It halts further erosion.
- Cons: Requires commitment and specialized psychological/medical support, which can be a lengthy and challenging process.
- What to Expect: This involves psychotherapy (CBT, DBT, family-based therapy), nutritional counseling, and sometimes medication. Referral to an eating disorder specialist is paramount.
2. Fluoride Therapy
- Pros: Strengthens remaining enamel, makes teeth more resistant to acid, and can help remineralize early lesions. Reduces sensitivity. Non-invasive.
- Cons: Does not replace lost enamel. Requires consistent application.
- What to Expect:
- Prescription-strength fluoride toothpaste or mouthrinse: Contains higher concentrations of fluoride than over-the-counter products, typically used daily.
- In-office fluoride varnish or gel applications: Applied by the dentist or hygienist during regular check-ups.
- Custom fluoride trays: For daily home use, similar to whitening trays, filled with prescription fluoride gel.
3. Management of Dry Mouth (Xerostomia)
- Pros: Improves comfort, reduces risk of cavities and gum disease, aids natural buffering.
- Cons: Often manages symptoms rather than curing the cause.
- What to Expect:
- Over-the-counter saliva substitutes: Gels, sprays, or rinses that mimic natural saliva.
- Xylitol products: Chewing gum or lozenges with xylitol can stimulate saliva flow and inhibit bacterial growth.
- Prescription medications: Pilocarpine or cevimeline can stimulate salivary glands if they are still functional.
- Increased water intake: Consistent hydration is vital.
4. Dental Restorations
The choice of restoration depends on the extent of erosion and individual needs.
a. Dental Bonding (Composite Resin)
- Pros: Minimally invasive, relatively inexpensive, can be done in one visit, good aesthetic match.
- Cons: Less durable than veneers or crowns, can stain over time, not suitable for severe erosion or bite issues.
- What to Expect: A tooth-colored resin material is applied to the tooth, sculpted to shape, and hardened with a light. It can repair minor chips, mask sensitivity, and restore some tooth length.
- Cost: $200 - $600 per tooth (US average).
b. Dental Veneers (Porcelain or Composite)
- Pros: Highly aesthetic, durable (porcelain), can significantly improve tooth shape, color, and length. Porcelain veneers are stain-resistant.
- Cons: More expensive than bonding, porcelain veneers require removal of a small amount of enamel, irreversible, can take multiple appointments.
- What to Expect: For porcelain, a thin layer of enamel is removed, impressions are taken, and custom veneers are fabricated in a lab. For composite, material is applied directly and sculpted. Veneers are bonded to the front surface of the tooth.
- Cost:
- Composite Veneers: $250 - $1,500 per tooth.
- Porcelain Veneers: $800 - $2,500 per tooth.
c. Dental Crowns (Caps)
- Pros: Provides full coverage and protection for severely damaged or weakened teeth, restores function and aesthetics, highly durable.
- Cons: Most invasive, requires significant tooth reduction, most expensive, typically 2 appointments.
- What to Expect: The tooth is reshaped, an impression is taken, and a custom crown (porcelain, zirconia, gold, or PFM) is fabricated and permanently cemented over the prepared tooth.
- Cost: $800 - $3,000 per tooth (US average, varies by material).
d. Dental Fillings
- Pros: Repairs cavities and protects tooth from further decay.
- Cons: Does not address widespread erosion.
- What to Expect: Removal of decayed tooth structure and filling with composite resin or amalgam.
- Cost: $100 - $450 per filling (US average, varies by size and material).
5. Management of Salivary Gland Enlargement (Sialadenosis)
- Pros: Reduces facial swelling, improves aesthetics.
- Cons: May take time to resolve after purging cessation.
- What to Expect: Primarily resolves spontaneously once the purging behavior stops. Sometimes warm compresses or gentle massage can offer comfort. Medical evaluation is needed to rule out other causes.
6. Treatment for TMJ Issues
- Pros: Alleviates pain and discomfort, improves jaw function.
- Cons: Can be complex, may require ongoing management.
- What to Expect: Custom oral splints (nightguards), physical therapy, pain medication, stress management, and in severe cases, orthodontics or surgery.
Step-by-Step Process: What to Expect During Dental Treatment
The exact process will depend on the severity of the damage and the chosen treatment, but here’s a general overview for comprehensive restoration:
-
Initial Consultation & Diagnosis:
- What happens: Comprehensive oral exam, X-rays, possibly intraoral photos. The dentist assesses the extent of erosion, sensitivity, and overall oral health. Discussion of medical history, including any eating disorders.
- Goal: To establish a baseline, identify immediate concerns, and formulate a personalized treatment plan.
- Key discussion: Emphasis on treating the underlying eating disorder first. No extensive restorative work should commence until purging behaviors have ceased or are well-managed for several months (typically 6 months minimum) to ensure treatment longevity.
-
Addressing Immediate Concerns & Prevention:
- What happens: Prescription for high-fluoride toothpaste/mouthrinse. Education on proper oral hygiene (e.g., not brushing immediately after vomiting, instead rinsing with water or baking soda solution). Recommendations for dry mouth remedies.
- Goal: To stop further damage, manage sensitivity, and create a healthier oral environment before major restorative work.
-
Restorative Phase Planning:
- What happens: Detailed treatment planning, which may involve digital scans, wax-ups (a model of proposed new teeth), and discussions about material choices (e.g., composite, porcelain, zirconia).
- Goal: To visualize the final outcome, ensure patient satisfaction, and prepare for the restorative procedures.
-
Preparation for Restorations (e.g., Veneers or Crowns):
- What happens: For veneers or crowns, a small amount of enamel is precisely removed from the tooth surface to create space for the restoration. For severe erosion, more extensive preparation might be needed. Impressions (molds) of the prepared teeth are taken. Temporary restorations may be placed.
- Goal: To create an ideal foundation for the permanent restorations.
-
Laboratory Fabrication (for Indirect Restorations like Porcelain Veneers/Crowns):
- What happens: The impressions are sent to a dental lab where skilled technicians craft the custom veneers or crowns based on the dentist's specifications. This typically takes 1-3 weeks.
- Goal: To create high-quality, custom-fit, and aesthetically pleasing restorations.
-
Placement of Permanent Restorations:
- What happens: The temporary restorations are removed. The permanent veneers or crowns are carefully fitted, checked for bite and aesthetics, and then permanently bonded or cemented to the teeth using strong dental adhesives. For bonding or composite fillings, this is done in a single visit after preparation.
- Goal: To restore the teeth's strength, appearance, and function.
-
Follow-up and Maintenance:
- What happens: Regular dental check-ups (initially every 3-4 months, then every 6 months), professional cleanings, continued fluoride therapy, and monitoring for any new issues.
- Goal: To ensure the longevity of the restorations and maintain overall oral health.
Cost and Insurance: US Price Ranges and Coverage
The cost of treating bulimia-related dental damage can be substantial, often ranging from hundreds to tens of thousands of dollars, depending on the severity and extent of the erosion.
Average US Costs for Common Treatments:
| Treatment Type | Typical Cost Range (Per Tooth) | Notes |
|---|---|---|
| Dental Bonding | $200 - $600 | Least expensive, good for minor chips, sensitivity, and surface irregularities. |
| Composite Fillings | $100 - $450 | For cavities, price varies by size and number of surfaces. |
| In-Office Fluoride App | $25 - $75 | Often covered by insurance as part of preventative care. |
| Custom Fluoride Trays | $150 - $350 | May be covered partially if prescribed for a specific condition. |
| Composite Veneers | $250 - $1,500 | Direct application, less durable than porcelain. |
| Porcelain Veneers | $800 - $2,500 | Highly aesthetic, durable, multiple visits required. Full mouth restorations can be $10,000 - $40,000+. |
| Dental Crowns | $800 - $3,000 | For severely damaged or weakened teeth, varies by material (e.g., porcelain-fused-to-metal, all-ceramic, zirconia). Full mouth restorations can be $15,000 - $50,000+. |
| Periodontal Treatment | $100 - $1,000+ | Varies widely based on severity (e.g., deep cleaning $100-$300 per quadrant, scaling and root planing $200-$500 per quadrant, gum surgery $500-$1,000+ per tooth/area). |
| TMJ Splints (Nightguard) | $300 - $800 | Custom-made oral appliance. |
Insurance Coverage Details:
Dental insurance coverage for bulimia-related damage can be complex.
- Preventative Care: Most insurance plans fully cover or heavily subsidize preventative services like routine exams, cleanings, and in-office fluoride applications (typically 1-2 per year).
- Basic Restorative Care: Fillings are usually covered at 50-80% after deductibles.
- Major Restorative Care (Veneers, Crowns): This is where coverage varies significantly.
- "Medically Necessary" vs. "Cosmetic": Insurance companies often distinguish between "medically necessary" procedures (e.g., crowns to restore severely fractured teeth, fillings for cavities) and "cosmetic" ones (e.g., veneers primarily for aesthetics). If the erosion is extensive and impacts function, the procedures may be covered, but documentation from the dentist linking the damage to functional impairment is crucial.
- Coverage Percentage: If covered, major procedures typically receive 50% coverage after the deductible is met.
- Annual Maximums: Most dental insurance plans have an annual maximum benefit, often ranging from $1,000 to $2,000 per year. For extensive full-mouth rehabilitation, this amount is quickly exhausted, leaving the patient to pay a significant portion out-of-pocket.
- Waiting Periods: Some plans have waiting periods (e.g., 6-12 months) for major restorative work.
Payment Plans and Financing Options:
Given the high costs, many patients explore financing:
- In-Office Payment Plans: Some dental practices offer flexible payment schedules directly.
- Third-Party Medical Financing: Companies like CareCredit or LendingClub offer specialized healthcare credit cards with deferred interest options for qualified applicants.
- Health Savings Accounts (HSAs) and Flexible Spending Accounts (FSAs): If you have an HSA or FSA, you can use these tax-advantaged accounts to pay for qualified dental expenses.
- Dental Schools: University dental schools often provide comprehensive care at a reduced cost, as treatments are performed by students under the supervision of experienced faculty. This can be a significantly more affordable option for extensive work but may involve longer appointment times.
- Dental Discount Plans: These are not insurance but membership plans that offer discounts on dental services from participating providers.
Pro Tip: Always discuss treatment costs and insurance coverage in detail with your dental office's financial coordinator. They can help you understand your benefits, estimate out-of-pocket expenses, and explore financing solutions.
Recovery and Aftercare: Maintaining Your Restored Smile
Recovery from bulimia-related dental damage is a long-term commitment that extends far beyond the final dental appointment. It hinges on sustained recovery from the eating disorder and meticulous ongoing oral care.
1. Sustained Eating Disorder Recovery
- Ongoing Therapy: Continuing psychological counseling, support groups, and nutritional guidance is paramount to prevent relapse, which would negate all dental progress.
- Self-Monitoring: Developing coping mechanisms for triggers and recognizing early warning signs of purging urges.
2. Meticulous Oral Hygiene
- Gentle Brushing: Use a soft-bristled toothbrush and non-abrasive fluoride toothpaste. Brush twice a day for two minutes.
- Flossing: Floss daily to remove plaque and food particles from between teeth and under the gumline.
- Rinsing, Not Brushing, After Purging: If a relapse occurs, do not brush immediately. Instead, rinse your mouth thoroughly with water, a fluoride mouthwash, or a baking soda solution (1 teaspoon baking soda in 8 ounces of water) to neutralize the acid. Wait at least 30-60 minutes before brushing.
- Limit Acidic Foods & Drinks: Reduce consumption of highly acidic beverages (soda, sports drinks, fruit juices, sparkling water) and acidic foods (citrus fruits, vinegar-based dressings), which can further erode weakened enamel and stress restorations.
- Use a Straw: When consuming acidic drinks, use a straw to minimize contact with teeth.
3. Continued Fluoride Therapy
- Prescription Fluoride: Continue using prescribed high-fluoride toothpaste or rinses as directed by your dentist to strengthen remaining enamel and reduce sensitivity.
- In-Office Fluoride: Regular professional fluoride applications during dental visits are beneficial.
4. Saliva Management
- Stay Hydrated: Drink plenty of water throughout the day.
- Saliva Stimulants: Use over-the-counter or prescription saliva substitutes, xylitol gums/lozenges as recommended to combat dry mouth.
5. Regular Dental Check-ups
- Increased Frequency: Initially, you may need more frequent dental visits (e.g., every 3-4 months) to monitor the condition of your teeth, assess the stability of restorations, and provide preventative care. Once stable, visits can return to every 6 months.
- Professional Cleanings: Essential for removing plaque and calculus (tartar) that can accumulate even with good home care.
6. Diet and Nutrition
- Balanced Diet: A healthy, balanced diet supports overall health, including oral health.
- Calcium-Rich Foods: Incorporate dairy products, leafy greens, and fortified foods to support bone and tooth health. While calcium supplements for teeth are generally beneficial for overall bone density and can contribute to tooth strength, they cannot reverse existing enamel erosion. Their primary role in oral health is preventative for general tooth mineralization.
Prevention: How to Safeguard Your Oral Health
True prevention of bulimia teeth lies in preventing or treating bulimia nervosa itself. However, for individuals struggling with purging behaviors, there are critical steps to minimize ongoing dental damage:
1. Seek Professional Help for Bulimia Nervosa
- This is the most crucial preventative measure. Early intervention for an eating disorder dramatically reduces the severity and extent of dental damage.
2. Implement Immediate Damage Control Strategies
These strategies are vital for individuals currently experiencing purging episodes:
- Do NOT Brush Immediately After Vomiting: As detailed above, wait at least 30-60 minutes.
- Rinse with Water or Baking Soda Solution: Immediately after purging, rinse your mouth vigorously with plain water or a solution of 1 teaspoon baking soda mixed in 8 ounces of water. Baking soda helps neutralize the stomach acid.
- Use Fluoride Toothpaste and Mouthwash: Regularly use fluoride products to strengthen enamel. Your dentist may prescribe a higher-concentration fluoride product.
- Avoid Excessive Acidic Foods and Drinks: While teeth are already compromised, limit additional acid exposure from sodas, citrus fruits, vinegar, etc.
- Stay Hydrated: Drink plenty of water to help maintain saliva flow and dilute acids.
- Consider Chewing Sugar-Free Gum with Xylitol: This can stimulate saliva flow, which helps neutralize acids and remineralize enamel.
- Inform Your Dentist: Open communication with your dentist is essential. They can provide targeted preventative advice and monitor your oral health closely.
3. Regular Dental Check-ups
- Consistent dental visits allow for early detection of erosion or cavities, enabling prompt intervention before damage becomes extensive. Your dentist can also apply protective sealants or fluoride varnishes.
4. Nutritional Considerations for Enamel Strength
- Ensure adequate intake of calcium and Vitamin D, which are crucial for overall bone and tooth health. While calcium supplements for teeth won't replace lost enamel, they support the healthy mineralization of existing tooth structure and bone, which is important for teeth supported by strong jawbones. This is a general recommendation for dental health, but not a direct solution for existing erosion.
Risks and Complications: What Can Go Wrong
If bulimia-related dental damage goes untreated or if purging behaviors continue, the complications can be severe and far-reaching:
- Progressive, Irreversible Tooth Loss: Enamel will continue to erode, eventually exposing dentin and pulp, leading to significant structural damage.
- Severe Tooth Sensitivity and Pain: Exposed dentin causes chronic pain and sensitivity, making eating, drinking, and even breathing difficult.
- Increased Risk of Cavities: Weakened enamel, dry mouth, and poor oral hygiene create a perfect environment for widespread tooth decay, often leading to deep cavities requiring root canals or extractions.
- Tooth Fractures and Breakage: Severely eroded teeth become brittle and can easily chip, crack, or fracture, leading to emergency dental situations.
- Gum Disease: Dry mouth and compromised oral health can exacerbate gingivitis and periodontitis, potentially leading to gum recession and bone loss around the teeth.
- Difficulty Chewing and Speaking: Extensive tooth loss or damage can impair oral function, affecting nutrition and communication.
- TMJ Disorders: Changes in bite caused by tooth wear can lead to chronic jaw pain, headaches, and dysfunction.
- Oral Infections: Dry mouth increases susceptibility to bacterial and fungal infections (like oral candidiasis).
- Compromised Aesthetics and Self-Esteem: Discolored, shortened, and damaged teeth can severely impact a person's appearance, leading to social anxiety and reduced quality of life.
- Higher Treatment Costs: Delaying treatment leads to more extensive damage, requiring more complex, invasive, and expensive restorative procedures in the long run.
Children / Pediatric Considerations
Eating disorders, including bulimia, can affect adolescents and even pre-adolescents. The dental consequences in children are particularly concerning because their teeth are still developing, and they have many years of dental health ahead of them.
- Developing Dentition: While primary (baby) teeth are also susceptible to erosion, the greater concern is the damage to newly erupted permanent teeth. These teeth have softer, less mature enamel that is more vulnerable to acid attack.
- Rapid Progression of Damage: Because children's enamel is thinner and less mineralized, erosion can progress more rapidly than in adults.
- Early Detection is Crucial: Parents, pediatricians, and pediatric dentists play a vital role in identifying potential signs. Swelling in the cheeks (sialadenosis), changes in tooth appearance, or unusual sensitivity in a child or teenager should prompt further investigation.
- Psychological Impact: The aesthetic damage to teeth can be particularly devastating for a child or adolescent's self-image and social development.
- Treatment Challenges: Restorative treatments in children may be more complex due to ongoing growth and development.
- Parental Guidance: Parents need to be educated on the subtle signs of eating disorders and understand the importance of seeking help for both the disorder and the dental damage. Regular dental check-ups are essential for all children, but especially those at risk or with known eating disorders. Pediatric dentists can offer age-appropriate fluoride therapies and protective measures.
Frequently Asked Questions
What does calcium build up on teeth look like, and is it related to bulimia?
What is calcium build up on teeth refers to dental calculus or tartar, which is hardened plaque. It typically appears as a yellow, brown, or white crust along the gumline or between teeth. While it's a common dental problem, it is generally not directly caused by bulimia. Bulimia primarily causes erosion (loss) of tooth structure due to acid, whereas calculus is an addition of mineralized deposits. However, poor oral hygiene, which can sometimes accompany an eating disorder, can increase calculus formation, exacerbating other dental issues.
Can bulimia teeth be fully restored to their original condition?
While the lost enamel cannot regenerate, dental professionals can restore the appearance, function, and strength of bulimia-affected teeth through various restorative treatments like bonding, veneers, and crowns. These treatments can make teeth look and feel like new, but they are replacements for the lost natural structure. Full restoration depends heavily on the cessation of purging behaviors.
How long does it take for bulimia to damage teeth?
Dental damage can begin fairly quickly, sometimes within a few months of consistent purging. The severity and speed of erosion depend on the frequency and duration of vomiting, the acidity of stomach contents, and individual salivary factors. Visible damage, such as sensitivity and erosion, typically becomes noticeable after 1-2 years of regular purging, but can occur sooner.
Is the treatment for bulimia teeth painful?
Many dental treatments can be performed with local anesthesia, making them generally pain-free during the procedure. Afterwards, some sensitivity or discomfort is common, especially with more invasive procedures like crown preparations, but this is usually manageable with over-the-counter pain relievers. Managing pre-existing sensitivity is also a priority.
Does dental insurance cover the full cost of bulimia teeth restoration?
It is rare for dental insurance to cover the full cost. While preventative care and basic fillings are usually covered, major restorative work like veneers and crowns are often covered at 50%, and often subject to annual maximums (typically $1,000-$2,000). Cosmetic-only treatments may not be covered at all. Extensive rehabilitation often requires significant out-of-pocket expenses.
How can calcium supplements for teeth help, given the erosion?
Calcium supplements for teeth primarily support the remineralization process of existing enamel and contribute to overall bone health, which supports tooth stability. They do not reverse already eroded enamel. For bulimia-affected teeth, their role is more indirect, supporting the general health of remaining tooth structure and the surrounding bone, and they are generally recommended as part of a comprehensive dietary approach rather than a direct treatment for erosion.
What is the most effective way to prevent further damage if someone is still struggling with bulimia?
The most effective way is to cease purging behaviors. However, if still struggling, immediate rinsing with water or a baking soda solution after vomiting (not brushing), using prescription-strength fluoride products, and avoiding additional acidic foods/drinks are critical harm-reduction strategies. Regular dental check-ups for protective fluoride applications and early intervention are also vital.
Can dentists identify bulimia just by looking at someone's teeth?
Yes, dentists are often the first healthcare professionals to identify signs consistent with bulimia nervosa. The distinct pattern of perimylolysis (smooth erosion on the lingual/palatal surfaces of upper front teeth), combined with other oral signs like salivary gland enlargement (sialadenosis), dry mouth, and possibly oral lesions, is highly indicative. A skilled dentist will often initiate a sensitive conversation and recommend further medical evaluation.
Are there any natural remedies for eroded teeth?
No, once enamel is physically eroded, it cannot be naturally regrown or repaired by home remedies. Natural remedies might help with symptoms like dry mouth or sensitivity (e.g., xylitol, aloe vera rinses), but they cannot restore lost tooth structure. Professional dental intervention is necessary to protect and rebuild eroded teeth.
How important is treating the underlying eating disorder for dental health?
Treating the underlying eating disorder is absolutely paramount. No dental treatment, no matter how extensive or expensive, will be successful long-term if the purging behavior continues. The acid will simply continue to destroy new restorations and remaining tooth structure. Dental care is a critical component of overall recovery, but it must be paired with comprehensive psychological and medical treatment for bulimia nervosa.
When to See a Dentist
It is crucial to see a dentist immediately if you suspect you or someone you know might be experiencing bulimia-related dental damage, or if you are struggling with an eating disorder that involves purging. Early intervention can significantly limit the extent of permanent damage.
You should schedule a dental appointment if you notice any of the following warning signs:
- Increased tooth sensitivity to hot, cold, or sweet foods and drinks.
- Changes in the appearance of your teeth, such as them appearing more yellow, translucent, rounded, or shorter.
- Chipping or fracturing of your teeth without apparent trauma.
- Fillings appearing "raised" above the surrounding tooth surface.
- Frequent dry mouth or sore throat that doesn't resolve.
- Swelling in your cheeks or jaw area (sialadenosis).
- Any pain in your teeth or jaw.
- If you are currently, or have previously, engaged in purging behaviors, even if you don't notice obvious dental issues yet.
Emergency vs. Scheduled Appointment Guidance:
- Emergency Dental Visit (ASAP):
- Severe, persistent toothache that is not relieved by over-the-counter pain medication.
- A broken or fractured tooth that causes sharp pain or exposes sensitive pulp.
- Significant swelling in your face or gums, possibly indicating an infection.
- Rapidly progressing sensitivity or sudden, acute pain.
- Scheduled Dental Appointment (Promptly):
- All other signs of bulimia teeth, even if not immediately painful, warrant a prompt, non-emergency visit. The damage is cumulative and progressive, so waiting will only lead to more extensive and costly treatments.
- If you are seeking help for bulimia nervosa, inform your dentist during your consultation so they can provide specialized care and support as part of your overall recovery team.
Remember: Your dentist is a healthcare professional who can offer support and solutions without judgment. Open communication about your health, including mental health challenges like eating disorders, is vital for comprehensive care.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

What Are Calcium Deposits on Teeth
Are you one of the millions of Americans who notices a stubborn, yellowish buildup on your teeth despite regular brushing? You're likely experiencing what many refer to as "calcium deposits on teeth." This common dental concern, medically known as dental calculus or tartar, affects a vast ma
February 23, 2026

Calcium Good for Teeth: Complete Guide
More than 99% of your body's calcium resides in your bones and teeth, making it an undeniable cornerstone of skeletal and oral health. But did you know that an estimated 42% of American adults don't get enough calcium from their diet? This staggering statistic underscores a critical question
February 23, 2026

Erosion in Teeth: Complete Guide
Erosion in Teeth: Complete Guide
February 23, 2026

Do Teeth Have Calcium
When you flash a confident smile, what are you truly showing? Many people might assume their teeth are solid, unchanging structures made primarily of bone, or even pure calcium. But do teeth have calcium? The answer is a resounding yes, though not in the simplistic way some might imagine. Calciu
February 23, 2026