Dentin
4,513 words · 15 min read
Quick Definition
The hard, yellowish tissue that makes up the bulk of a tooth beneath the enamel and cementum. Dentin is softer than enamel and contains microscopic tubules that can transmit sensation.
What is Dentin? Your Definitive Guide to the Tooth's Core
Welcome to SmilePedia.net, your trusted resource for comprehensive dental health information. Today, we delve into dentin, a vital yet often overlooked component of your teeth. If you've ever searched "what is dentin" or "dentin dental," you're in the right place for an in-depth exploration.
Dentin is the hard, yellowish tissue that makes up the bulk of a tooth beneath the enamel (on the crown) and cementum (on the root). It is softer than enamel but harder than bone, providing the tooth's primary structure and resilience. Unlike enamel, dentin is a living tissue, containing microscopic tubules that can transmit sensation to the tooth's innermost layer, the dental pulp.
Understanding dentin is paramount for maintaining optimal dental health because its integrity directly impacts the tooth's strength, sensitivity, and the health of the pulp. When dentin is exposed or damaged, it can lead to a cascade of problems, from persistent tooth sensitivity to the progression of dental caries (cavities), ultimately threatening the tooth's viability. Damage to dentin is remarkably common, often stemming from dental caries, which affects 26% of US adults aged 20-64 with untreated decay, or from acid erosion and aggressive brushing. Recognizing the signs of compromised dentin and seeking timely dental care is crucial for preventing more severe issues.
Key Takeaways:
- Dentin is the main body of the tooth, lying beneath enamel and cementum.
- It is a living tissue, softer than enamel but harder than bone.
- Microscopic channels called dentinal tubules make it sensitive to external stimuli.
- Dentin protects the dental pulp, the tooth's nerve and blood supply.
- Damage to dentin (e.g., from caries or erosion) is a primary cause of tooth sensitivity and can lead to serious dental issues.
- Dentin can form new tissue (tertiary dentin) in response to injury.
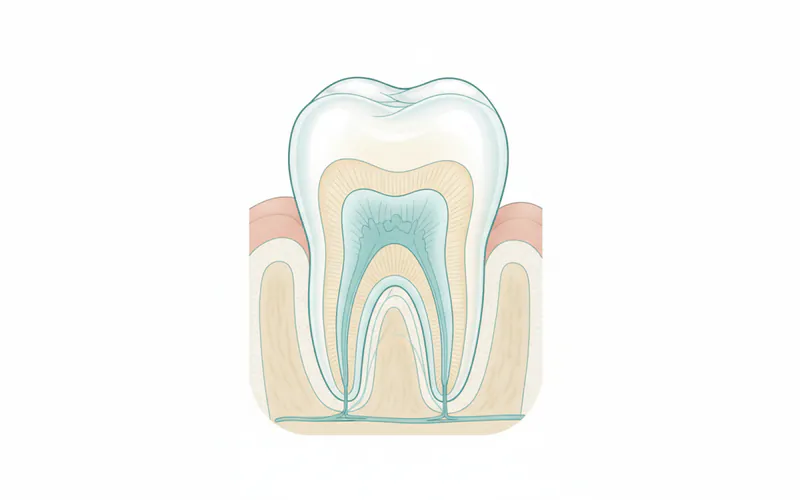
Anatomy and Composition of Dentin
To truly grasp the importance of dentin, it helps to understand its place within the tooth's complex structure. Dentin forms the core of both the crown (the visible part of the tooth) and the root (anchored in the jawbone). In the crown, it is protected by the super-hard enamel, the body's hardest substance. In the root, it is covered by cementum, a bone-like tissue that helps anchor the tooth to the surrounding bone via ligaments.
Structurally, dentin is characterized by millions of microscopic channels known as dentinal tubules. These tubules extend from the outer surface of the dentin all the way to the pulp chamber. Each tubule contains fluid and a nerve fiber extension from the odontoblasts (specialized cells that produce dentin) located on the pulp's outer wall. This intricate network is responsible for dentin's ability to transmit sensations like pain, pressure, and temperature changes.
Dentin is composed of approximately 70% inorganic material (primarily hydroxyapatite crystals, similar to enamel and bone but less dense), 20% organic material (mostly collagen fibers, which provide flexibility), and 10% water. This composition makes dentin more resilient to fracture than enamel, providing a crucial buffer for the tooth. It's also slightly yellowish, which is why teeth may appear more yellow if their outer enamel layer is thin or worn.
Types and Classifications of Dentin
Not all dentin is the same. Dental scientists classify dentin into several types based on when and how it forms, each serving a specific purpose in the tooth's life cycle and response to challenges.
-
Primary Dentin: This is the dentin formed before tooth eruption and completion of root formation. It constitutes the bulk of the tooth structure.
- Mantle Dentin: The outermost layer of primary dentin, located just beneath the enamel or cementum. It's the first dentin formed and has a slightly different structure.
- Circumpulpal Dentin: The main body of primary dentin, forming the layer between the mantle dentin and the pulp chamber. It makes up the majority of the tooth's dentin.
-
Secondary Dentin: Formed throughout a tooth's life after root completion, secondary dentin is deposited slowly and continuously by odontoblasts along the walls of the pulp chamber. This process gradually reduces the size of the pulp chamber and canals, which is a normal physiological response to aging and ongoing tooth function. It is structurally similar to primary dentin but forms at a slower rate.
-
Tertiary Dentin (Reparative or Reactive Dentin): This specialized dentin forms in response to external stimuli or injury, such as caries, trauma, or significant wear. It is a localized, defensive mechanism produced by odontoblasts to protect the underlying pulp from irritation or bacterial invasion.
- Reactionary Dentin: Formed by existing odontoblasts in response to mild to moderate stimuli (e.g., slow-progressing caries, minor abrasion).
- Reparative Dentin: Formed by newly differentiated odontoblast-like cells when original odontoblasts have been destroyed by more severe trauma or infection.
- Sclerotic Dentin: A form of tertiary dentin where the dentinal tubules become completely occluded (blocked) with mineral deposits. This occurs as a protective response to chronic, slow-progressing stimuli, making the dentin less permeable and reducing sensitivity.
Functions of Dentin
The roles of dentin extend far beyond merely providing structural support. Its unique properties make it integral to the tooth's overall health and function.
- Structural Support and Form: As the primary component of the tooth, dentin gives the tooth its basic shape and maintains its rigidity. It acts as a shock absorber for the more brittle enamel, preventing fractures from everyday chewing forces.
- Protection of the Pulp: Dentin serves as a critical barrier, shielding the delicate dental pulp (which contains nerves, blood vessels, and connective tissue) from external threats like bacteria, temperature changes, and physical trauma.
- Sensation Transmission: The dentinal tubules and the fluid within them are key to the tooth's ability to sense stimuli. The "hydrodynamic theory" of tooth sensitivity suggests that external stimuli (cold, heat, sugar, air) cause rapid fluid movement within these tubules. This movement stimulates nerve endings in the pulp, leading to the sensation of pain or sensitivity.
- Nutrition and Vitality: Odontoblasts, the cells lining the pulp and producing dentin, are responsible for its continued health and ability to form secondary and tertiary dentin. They receive nutrients from the pulp, maintaining the vitality of the dentin layer.
Causes and Risk Factors for Dentin Damage
Damage to dentin is a common dental problem, often resulting in pain, sensitivity, and the potential for more severe issues if left untreated. Several factors can compromise the integrity of this vital tissue.
- Dental Caries (Cavities): This is the most prevalent cause of dentin damage. When bacteria in plaque on the tooth surface produce acids, they first demineralize the enamel. If left unchecked, these acids penetrate the enamel and reach the dentin. Because dentin is softer and more porous than enamel, caries can spread much more rapidly once it reaches this layer, quickly advancing towards the dental pulp.
- Tooth Erosion: The loss of tooth structure due to chemical processes, typically acids not produced by bacteria. Common sources include acidic foods and drinks (soda, citrus fruits, sports drinks), gastric reflux (GERD), and certain medications. Erosion can wear away enamel and expose dentin, leading to severe sensitivity.
- Tooth Abrasion: Mechanical wear of tooth structure caused by external forces. This often occurs from aggressive or incorrect brushing techniques, using a hard-bristled toothbrush, or habitually chewing on non-food items (e.g., pen caps, fingernails). Abrasion commonly affects the gumline, exposing root dentin.
- Tooth Attrition: Wear of tooth structure from tooth-on-tooth contact, primarily due to grinding (bruxism) or clenching. Over time, attrition can wear down the chewing surfaces, exposing the underlying dentin.
- Gum Recession: When gums pull back from the teeth, they expose the root surfaces. The root dentin is normally covered by cementum, which is much thinner and softer than enamel and easily wears away, leaving the sensitive root dentin exposed to the oral environment. This is a very common cause of tooth sensitivity.
- Cracked or Fractured Teeth: Trauma, biting on hard objects, or large fillings can lead to cracks or fractures that extend into the dentin. These cracks can expose dentinal tubules, leading to pain and sensitivity, and providing pathways for bacteria to reach the pulp.
- Dental Procedures: Sometimes, certain dental procedures, such as aggressive scaling and root planing during deep cleanings, or over-preparation during cavity fillings, can inadvertently expose dentin or thin the existing enamel layer, contributing to sensitivity.
Signs and Symptoms to Watch For
Recognizing the signs of dentin damage is the first step toward effective treatment and preventing further complications. Pay close attention to these common indicators:
- Tooth Sensitivity: This is the hallmark symptom of exposed or compromised dentin. You may experience a sharp, sudden, and often temporary pain when your teeth are exposed to:
- Cold foods or drinks
- Hot foods or drinks
- Sweet or acidic foods
- Cold air
- Brushing or flossing
- Pain When Biting or Chewing: If the dentin is damaged by a crack, caries, or a loose filling, pressure from biting can stimulate the exposed nerve endings, causing pain.
- Visible Holes or Pits (Cavities): If caries has progressed through the enamel into the dentin, you may be able to see a discoloration, a soft spot, or an actual hole in your tooth. These can appear brown, black, or even chalky white initially.
- Yellowish or Brownish Discoloration: If the protective enamel layer is significantly worn away or eroded, the natural yellowish hue of the underlying dentin may become more prominent. This can lead to teeth appearing darker or duller.
- Bad Breath or Unpleasant Taste: Advanced caries involving dentin can harbor food particles and bacteria, leading to persistent bad breath (halitosis) or a foul taste in your mouth.
- Swelling Around the Tooth or Jaw: While less common for early dentin damage, if caries or a crack has progressed deeply enough to cause pulp infection, you might experience localized swelling, a pimple-like bump on the gums, or even facial swelling. This indicates a severe infection requiring immediate attention.
Diagnosis Process — What Your Dentist Does
If you experience any of the symptoms above, it's crucial to consult your dentist. A thorough diagnostic process helps pinpoint the cause and extent of dentin damage.
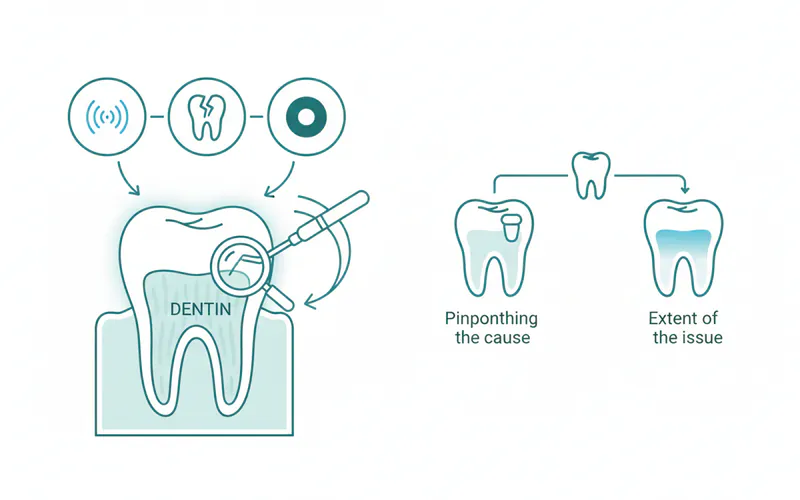
- Clinical Examination: Your dentist will visually inspect your teeth and gums for signs of caries, cracks, erosion, or gum recession. They will use a small instrument called an explorer to gently check tooth surfaces for soft spots or irregularities indicative of decay.
- Patient History: You'll be asked about your symptoms (when they started, what triggers them, how long they last), your oral hygiene habits, diet, and any relevant medical conditions. This information is vital for understanding potential risk factors.
- Sensitivity Tests: To confirm the presence and source of sensitivity, your dentist may apply cold air, a cold cotton pellet, or a dental probe to specific teeth. They might also tap on teeth to check for tenderness.
- Dental X-rays: Radiographs (X-rays) are indispensable for detecting caries that are hidden between teeth or under existing fillings, and to assess the depth of decay, its proximity to the pulp, and any signs of infection in the bone. Bitewing X-rays are common for detecting interproximal caries, while periapical X-rays show the entire tooth, including the root tip and surrounding bone.
- Transillumination: For suspected cracks, your dentist may shine a bright light through the tooth. Cracks will block the light, appearing as dark lines.
- Dye Application: In some cases, a special dental dye might be applied to a cracked tooth to make the fracture line more visible.
- Pulp Vitality Testing: If pulp involvement is suspected, electric pulp testers or thermal tests (hot or cold stimuli) may be used to assess the health and responsiveness of the pulp.
Treatment Options with Pros, Cons, and Costs
Treatment for dentin damage varies widely depending on the cause, severity, and location of the problem. Here's an overview of common approaches, including their typical cost ranges in the US (without insurance).
| Treatment Option | Best For | Pros | Cons | Est. Cost (US, without insurance) |
|---|---|---|---|---|
| Desensitizing Toothpaste | Mild to moderate sensitivity | Non-invasive, affordable, readily available OTC. | Requires consistent use (2-4 weeks for results), limited effectiveness for severe cases, temporary relief. | $5 - $20 |
| Fluoride Varnish/Gel | Mild sensitivity, early caries, erosion | Professional application, strengthens enamel, remineralizes dentin. | Temporary, requires reapplication every 3-6 months, can cause temporary discoloration. | $25 - $75 per application |
| Dental Bonding/Sealants | Exposed root dentin, surface erosion | Quick, non-invasive (for sealants), covers sensitive areas, good aesthetics. | May chip or wear over time (bonding), sealants are primarily for enamel but can protect exposed dentin from early decay. | $50 - $250 per tooth |
| Dental Fillings | Dental caries, minor chips/fractures | Restores tooth structure, stops decay progression, various material options. | Invasive (drilling required), potential post-operative sensitivity, limited lifespan (5-15 years). | $100 - $600 (Amalgam/Composite) |
| Dental Crowns | Extensive decay, large fractures, cracks | Provides full coverage and strength, protects weakened teeth, durable. | More invasive (significant tooth reduction), higher cost, multiple appointments, can lead to pulp irritation. | $800 - $2,500 |
| Gum Graft Surgery | Exposed root dentin due to recession | Covers roots, significantly reduces sensitivity, improves aesthetics. | Surgical procedure, higher cost, recovery time, potential discomfort post-op. | $600 - $2,500 per tooth |
| Root Canal Therapy | Pulp infection due to deep dentin damage | Saves the natural tooth, relieves severe pain. | Invasive, requires subsequent crown for protection, higher cost, can make tooth brittle. | $700 - $2,000 (plus crown) |
Insurance Coverage: Most dental insurance plans cover a portion of restorative treatments. Basic restorative care (fillings) is typically covered at 50-80%, while major restorative procedures (crowns, root canals, gum grafts) may be covered at 0-50%, often after a waiting period and subject to deductibles and annual maximums. Preventive treatments like fluoride are often covered at 80-100%.
Step-by-Step: What to Expect During Treatment (Dental Filling for Caries)
Let's walk through what you might expect if you need a dental filling, a common treatment for caries that has reached the dentin.
- Anesthesia: The first step is to numb the tooth and surrounding gum tissue. Your dentist will apply a topical anesthetic gel to the gum, followed by an injection of local anesthetic. You might feel a slight pinch, but the area will quickly become numb, ensuring a pain-free procedure.
- Removal of Decayed Tissue: Once the area is numb, your dentist will use a dental drill to carefully remove the decayed dentin and any remaining affected enamel. The goal is to remove all caries-infected tissue while preserving as much healthy tooth structure as possible. Water is used to keep the tooth cool and clear debris.
- Tooth Preparation: After removing the decay, the tooth cavity will be shaped to ensure the filling material has a secure and stable base. If the decay was very deep or close to the pulp, a protective liner or base material might be placed over the deepest part of the cavity to shield the pulp and encourage tertiary dentin formation.
- Application of Filling Material:
- Composite (Tooth-Colored) Fillings: If using composite resin, a bonding agent is applied to the prepared cavity. This agent helps the composite material adhere to the tooth structure. The composite resin, which is a paste-like material, is then applied in layers, with each layer cured (hardened) using a special blue light.
- Amalgam (Silver) Fillings: If using amalgam, the material is packed directly into the prepared cavity. It hardens quickly and requires no light curing.
- Shaping and Polishing: Once the filling material is in place, your dentist will carefully shape it to match the natural contours of your tooth and restore your bite. They will then polish the filling, making it smooth to prevent food accumulation and ensure comfort.
- Bite Check: You'll be asked to bite down gently to ensure the filling is not too high. Any adjustments needed are made immediately.
Recovery Timeline and Aftercare
After a dental procedure involving dentin (especially a filling or crown), a certain degree of sensitivity is normal, though it typically subsides within a few days to a few weeks.

- Temporary Sensitivity: You might experience sensitivity to hot, cold, or pressure for a few days or weeks, especially with composite fillings as the material settles. This is usually mild and can be managed with over-the-counter pain relievers (e.g., ibuprofen).
- Avoiding Hard/Sticky Foods: For the first 24 hours after a filling, it's wise to avoid very hard or sticky foods, especially if you had an amalgam filling, which takes longer to fully set. Even with composite, giving it time to bond properly is beneficial.
- Maintaining Good Oral Hygiene: Continue to brush twice daily and floss once daily to keep the treated tooth and surrounding areas clean. Use a soft-bristled toothbrush and fluoride toothpaste.
- Follow-up Appointments: Your dentist may schedule a follow-up appointment to check the filling or crown, especially if you experience persistent pain or discomfort.
If sensitivity worsens, persists beyond a few weeks, or if you develop severe pain, swelling, or signs of infection, contact your dentist immediately.
Prevention Strategies
Protecting your dentin is fundamentally about preventing enamel erosion, gum recession, and dental caries. Here are key strategies:
- Excellent Oral Hygiene:
- Brush your teeth twice a day for two minutes each time with a soft-bristled toothbrush and fluoride toothpaste.
- Floss daily to remove plaque and food particles from between teeth and under the gumline.
- Use Fluoride: Fluoride strengthens enamel and can help remineralize early lesions in dentin. Use fluoride toothpaste, and ask your dentist about fluoride rinses or in-office fluoride treatments.
- Limit Sugary and Acidic Foods/Drinks: Reduce your intake of sodas, sports drinks, fruit juices, and sugary snacks that fuel caries-causing bacteria. Minimize acidic foods like citrus fruits and vinegars that contribute to enamel erosion. When you do consume them, rinse your mouth with water afterward.
- Regular Dental Check-ups and Cleanings: Visit your dentist every six months for professional cleanings and examinations. Early detection of caries or enamel erosion can prevent dentin involvement and more complex treatments.
- Address Bruxism (Teeth Grinding): If you grind or clench your teeth (especially at night), your dentist may recommend a custom nightguard to protect your enamel and prevent attrition that can expose dentin.
- Protect Against Gum Recession: Practice proper brushing technique (gentle, circular motions) to avoid aggressive scrubbing that can lead to gum recession. If you have existing recession, discuss options with your dentist.
- Dental Sealants: While primarily for pits and fissures on chewing surfaces (to protect enamel), sealants can prevent bacteria from reaching areas vulnerable to decay, thereby safeguarding the underlying dentin.
For Parents / Pediatric Considerations
Dentin plays a particularly crucial role in the dental health of children. Understanding its characteristics in primary (baby) teeth is essential for parents.
- Thinner Enamel and Dentin: Primary teeth have thinner enamel and dentin layers compared to permanent teeth. This means that once caries starts, it can penetrate the enamel and reach the dentin more quickly, and then spread rapidly through the dentin to the pulp.
- Larger Pulp Chamber: The pulp chambers in primary teeth are proportionally larger than in permanent teeth. This makes the pulp more vulnerable to infection once caries reaches the dentin.
- Rapid Caries Progression: Due to the thinner layers and larger pulp, decay in baby teeth can progress very quickly from a small cavity to a pulp infection, potentially leading to pain, swelling, and early tooth loss. Early loss of baby teeth can affect speech development, chewing ability, and the proper alignment of permanent teeth.
- Importance of Prevention:
- Early Dental Visits: The American Academy of Pediatric Dentistry recommends a child's first dental visit by age one or when the first tooth erupts.
- Fluoride Varnish: Pediatric dentists frequently apply fluoride varnish to strengthen enamel and protect dentin.
- Dental Sealants: These are highly effective for preventing caries on the chewing surfaces of molars, both primary and permanent, protecting the dentin beneath.
- Dietary Habits: Limiting sugary drinks and snacks, and promoting a balanced diet, are critical for preventing early childhood caries.
- Good Oral Hygiene: Parents should brush their child's teeth twice a day with a small amount of fluoride toothpaste (rice-grain size for under 3, pea-size for 3-6 years old).
Frequently Asked Questions
Is dentin living tissue?
Yes, dentin is considered a living tissue. Unlike enamel, which is acellular, dentin contains microscopic tubules filled with fluid and extensions from odontoblast cells, which line the pulp chamber. These cells are vital for the formation of new dentin (secondary and tertiary) throughout life, making dentin responsive to stimuli and capable of some repair.
Can damaged dentin repair itself?
Dentin has a remarkable capacity for localized repair through the formation of tertiary dentin (also known as reparative or reactive dentin). In response to stimuli like caries, abrasion, or erosion, odontoblasts (or newly differentiated cells if the original odontoblasts are destroyed) can lay down new dentin to protect the pulp. This process walls off the insult and helps prevent pulp infection. However, dentin cannot regenerate large sections of lost tissue in the same way that bone can. Extensive damage still requires professional dental intervention.
Why is my tooth so sensitive when dentin is exposed?
Tooth sensitivity occurs when dentin is exposed to the oral environment, typically due to enamel erosion, gum recession, or caries. The exposed dentinal tubules contain fluid. When exposed to external stimuli (like cold air, hot liquids, or sweet foods), this fluid moves rapidly within the tubules, stimulating nerve endings in the underlying pulp. This rapid fluid movement is interpreted by the brain as a sharp, sudden pain, a phenomenon explained by the hydrodynamic theory of sensitivity.
What's the difference between enamel and dentin?
The key differences between enamel and dentin are:
- Location: Enamel is the outermost layer of the tooth crown; dentin is underneath it and forms the bulk of the tooth.
- Hardness: Enamel is the hardest substance in the human body (96% mineral); dentin is softer than enamel (70% mineral).
- Color: Enamel is translucent white; dentin is naturally yellowish and contributes to the tooth's overall color.
- Vitality: Enamel is non-living, acellular tissue; dentin is a living tissue with odontoblast cells and tubules.
- Sensation: Enamel has no nerve endings; dentin is sensitive due to its tubules connecting to the pulp.
- Repair: Enamel cannot repair itself; dentin can form secondary and tertiary dentin.
How much does it cost to treat dentin damage?
The cost of treating dentin damage in the US varies widely depending on the type and severity of the damage, the treatment required, geographic location, and whether you have dental insurance. Minor issues like sensitivity might be treated with a $5-20 desensitizing toothpaste or a $25-75 fluoride varnish. A dental filling for caries could range from $100-600. More extensive damage requiring a crown might be $800-2,500, and a root canal can cost $700-2,000 (plus the cost of a crown). Dental insurance often covers 50-80% of restorative procedures, but it's essential to check your specific plan.
Is treatment for dentin damage painful?
Most treatments for dentin damage, especially those involving dental procedures like fillings or crowns, are performed under local anesthesia. This means you should not feel any pain during the procedure itself, though you might feel pressure or vibrations. After the anesthetic wears off, it's common to experience some temporary sensitivity or mild discomfort for a few days to a few weeks, which can usually be managed with over-the-counter pain relievers. If you have severe anxiety about dental pain, discuss sedation options with your dentist.
How long do treatments for dentin damage last?
The longevity of treatments for dentin damage depends entirely on the type of treatment:
- Desensitizing toothpaste/varnishes: Provide temporary relief and require ongoing use or reapplication (every 3-6 months).
- Dental fillings: Can last 5-15 years or more, depending on the material and oral hygiene.
- Dental bonding/sealants: May last 5-10 years, but can chip or wear down.
- Dental crowns: Are designed to last 10-15 years or longer with proper care.
- Root canal therapy: If successful and followed by a crown, the treated tooth can last a lifetime. Maintaining excellent oral hygiene and regular dental check-ups are crucial for maximizing the lifespan of any dental restoration.
What are the alternatives to traditional fillings for dentin caries?
For very early stages of caries where damage is minimal and primarily in the enamel or superficial dentin, alternatives may include:
- Fluoride Varnish/Resin Infiltration: To remineralize the tooth and stop decay progression without drilling.
- Dental Sealants: For pits and fissures, preventing caries from forming in the first place.
- Strict Oral Hygiene & Dietary Changes: Can help arrest very early lesions. However, once caries has significantly progressed into the dentin, a traditional filling or more extensive restorative treatment (like a crown) is typically necessary to remove the decay and restore the tooth's integrity. There are generally no effective non-invasive alternatives for established dentin caries.
When to See a Dentist
Recognizing when to seek professional dental care is crucial for managing dentin damage and preventing more severe complications.
Emergency Signs (See a dentist immediately):
- Severe, throbbing, or constant tooth pain that interferes with sleep or daily activities. This could indicate a pulp infection (pulpitis) requiring urgent attention.
- Facial swelling, swelling around the tooth, or a "pimple" on the gums. These are signs of an acute infection or abscess.
- Fever accompanied by tooth pain or swelling.
- Pain when biting down on a tooth that recently had a filling or crown, or if a filling has fallen out.
- A tooth that has been knocked out or severely fractured.
Routine Care (Schedule an appointment soon):
- New or persistent tooth sensitivity to hot, cold, sweet, or air, even if it's mild. This often indicates exposed dentin or early caries.
- Visible changes in your teeth, such as dark spots, holes, or rough edges, which could be signs of caries or erosion.
- Any discomfort or pain when chewing that is not severe enough to be an emergency.
- Noticeable gum recession exposing tooth roots.
- Loose or damaged fillings or crowns.
- Regular dental check-ups and cleanings (ideally every six months) are vital for early detection and prevention of dentin damage.
Early intervention is key to preserving your natural teeth and avoiding more invasive, costly, and time-consuming treatments. Don't wait for pain to become unbearable – consult your dentist at the first sign of trouble.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.