1st Oral Cancer Stages: Complete Guide
Key Takeaways
- Detecting oral cancer in its earliest stages is not just beneficial; it can be life-saving. Each year, thousands of Americans receive an oral cancer diagnosis, and tragically, the 5-year survival rate for late-stage oral cancer drops significantly compared to cases caught early. Understanding the **
1st Oral Cancer Stages: Complete Guide
Detecting oral cancer in its earliest stages is not just beneficial; it can be life-saving. Each year, thousands of Americans receive an oral cancer diagnosis, and tragically, the 5-year survival rate for late-stage oral cancer drops significantly compared to cases caught early. Understanding the 1st oral cancer stages – often referred to as Stage 0 or Stage I – is paramount because early detection drastically improves treatment outcomes, leading to a much higher chance of successful recovery and a better quality of life. This comprehensive guide will equip you with vital knowledge about what early oral cancer looks like, its common causes, how it's diagnosed, and the most effective treatment strategies, empowering you to advocate for your oral and overall health. We'll delve into the specific characteristics of these initial stages, the importance of regular screenings, and what you can do to minimize your risk.
Key Takeaways:
- Early Detection is Crucial: Oral cancer caught in Stage 0 or Stage I has an 85% or higher 5-year survival rate, significantly better than later stages.
- Common Signs: Look for persistent sores, red or white patches (erythroplakia/leukoplakia), lumps, or numbness in the mouth that don't heal within two weeks.
- Diagnosis: A definitive diagnosis involves a biopsy, which typically costs $250 - $1,500 without insurance, depending on complexity and location.
- Primary Treatments: Early stage oral cancer is often treated successfully with surgery (excision) and sometimes radiation therapy.
- Treatment Costs: Initial surgery for Stage I oral cancer can range from $5,000 - $30,000, with radiation therapy adding another $10,000 - $50,000 for a full course, depending on facility and specific techniques.
- Prevention: Quitting smoking/vaping, reducing alcohol consumption, practicing safe sex (to prevent HPV), and regular dental check-ups are key preventive measures.
- Recovery Timeline: Most patients can expect a recovery period of 2-6 weeks post-surgery for early stages, with follow-up care extending for years.
What It Is / Overview: Understanding Oral Cancer Staging
Oral cancer refers to any cancerous growth that develops in the oral cavity. This includes the lips, tongue, cheeks, floor of the mouth, hard and soft palate, sinuses, and pharynx (throat). Like other cancers, oral cancer is classified into stages using the TNM staging system developed by the American Joint Committee on Cancer (AJCC). TNM stands for:
- T (Tumor): Describes the size of the original tumor and whether it has grown into nearby areas.
- N (Nodes): Indicates whether the cancer has spread to nearby lymph nodes.
- M (Metastasis): Refers to whether the cancer has spread to distant parts of the body.
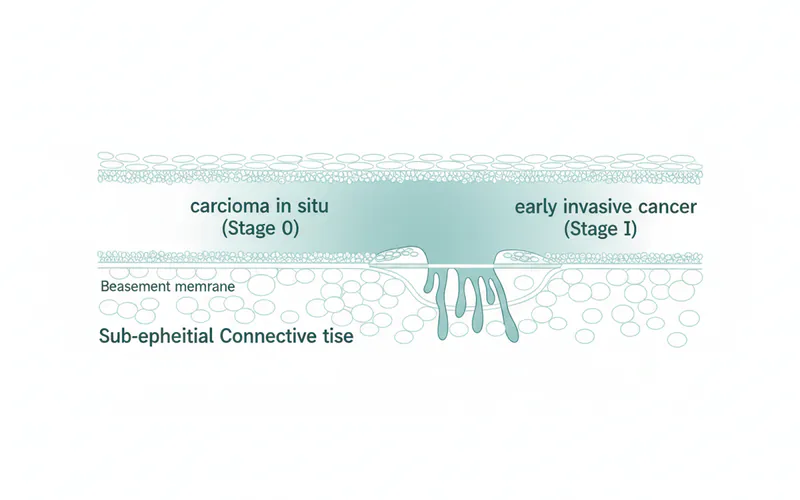
Understanding the 1st oral cancer stages specifically means focusing on Stage 0 and Stage I. These represent the earliest, most localized forms of the disease, making them highly curable.
- Stage 0 (Carcinoma In Situ): This is the earliest form of oral cancer. In this stage, abnormal cells are found only in the outermost layer of the lining of the oral cavity (the epithelium) and have not invaded deeper tissues. It's often referred to as "pre-cancer" because, if left untreated, it has the potential to develop into invasive cancer. At this stage, it doesn't meet the criteria for Stage I because it hasn't broken through the basement membrane.
- Stage I: At this stage, the cancer is still relatively small and has not spread significantly. Specifically, a Stage I oral cancer tumor is typically 2 centimeters (about 0.8 inches) or less in its greatest dimension, and it has not spread to any lymph nodes or distant sites in the body. The cancer cells have invaded beyond the superficial layer but are still contained within a small, localized area.
Catching oral cancer at Stage 0 or Stage I is crucial because the cancer is contained, making complete removal much more straightforward and successful. The primary goal at these stages is to eliminate all cancerous cells before they have the opportunity to grow larger, spread to lymph nodes (N), or metastasize to other organs (M).
Types / Variations of Oral Cancer
While various types of cancer can occur in the mouth, the vast majority of oral cancers fall under one main category, especially in the early stages.
Squamous Cell Carcinoma (SCC)
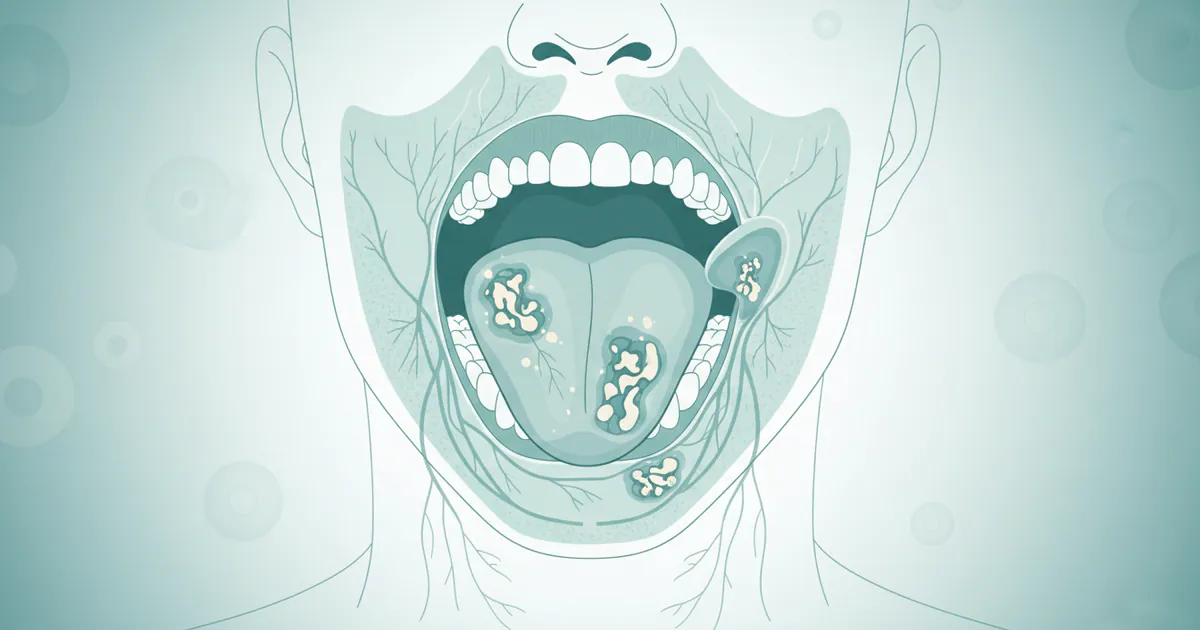
Squamous cell carcinoma accounts for over 90% of all oral cancers. It originates in the squamous cells, which are flat, thin cells that line the moist surfaces inside the mouth, nose, throat, and lungs. SCC can appear in any part of the oral cavity, but it is most commonly found on the:
- Sides and underside of the tongue
- Floor of the mouth
- Soft palate
- Lips
- Gums
In Stage 0 (carcinoma in situ), these squamous cells show severe dysplasia (abnormal growth) but have not yet become invasive. In Stage I, they have just begun to invade the deeper tissues.
Less Common Types
While rare, other types of cancer can occur in the oral cavity, though they are less likely to be diagnosed in Stage 0 or Stage I:
- Verrucous Carcinoma: A slow-growing, low-grade variant of squamous cell carcinoma, often associated with smokeless tobacco use. It appears as a warty growth.
- Minor Salivary Gland Cancers: These cancers develop in the small salivary glands located throughout the mouth lining. Examples include mucoepidermoid carcinoma and adenoid cystic carcinoma.
- Lymphoma: Cancers of the lymphatic system that can sometimes appear in the tonsils or base of the tongue.
- Melanoma: Though rare, melanoma can develop in the mouth, particularly on the palate or gums, originating from pigment-producing cells.
For the purpose of discussing 1st oral cancer stages, the focus almost exclusively remains on squamous cell carcinoma due to its prevalence and the distinct appearance of its early forms.
Causes / Why It Happens: Risk Factors for Oral Cancer
Oral cancer develops when DNA mutations occur in the cells of the mouth or throat, causing them to grow uncontrollably and form a tumor. While some cases occur without clear cause, several risk factors significantly increase the likelihood of developing oral cancer, even in its earliest stages.
Tobacco Use (Smoking and Smokeless Tobacco)
This is by far the leading risk factor.
- Smoking: Cigarettes, cigars, and pipes introduce harmful carcinogens directly into the mouth. The longer and more heavily a person smokes, the higher their risk. Smokers are up to 10 times more likely to develop oral cancer than non-smokers.
- Smokeless Tobacco: Products like chewing tobacco, snuff, and dissolvable tobacco are strongly linked to oral cancer, particularly affecting the gums, cheeks, and inner lips where the tobacco is held.
- Vaping/E-cigarettes: Regarding the question, "does zyn cause mouth cancer" or other nicotine pouches and e-cigarettes, the scientific community is still gathering long-term data. However, emerging research suggests that e-cigarettes and nicotine pouches like Zyn are NOT harmless. While they may contain fewer carcinogens than traditional cigarettes, they often contain:
- Nicotine: A highly addictive substance that can promote cell proliferation and inhibit apoptosis (programmed cell death), potentially contributing to cancer development and progression.
- Flavoring Agents: Many flavorings (e.g., diacetyl, cinnamaldehyde) are known irritants and can cause inflammation and damage to oral tissues.
- Formaldehyde and Acrolein: These are sometimes produced when e-liquids are heated, and both are known carcinogens.
- Other Toxins: Heavy metals and other volatile organic compounds have been found in e-cigarette aerosols.
- Conclusion on Zyn/Vaping: While direct, conclusive long-term evidence specifically linking Zyn to mouth cancer is still developing, the presence of nicotine and various chemicals that can damage oral tissue and potentially promote cancerous changes means that using Zyn and similar nicotine pouches or e-cigarettes should be considered a risk factor for oral health issues, including potentially increasing the risk of oral cancer. The ADA and other health organizations caution against the use of these products due to insufficient safety data and known harmful ingredients.
Alcohol Consumption
Heavy and regular alcohol consumption significantly increases oral cancer risk. The risk is particularly high when alcohol is combined with tobacco use, creating a synergistic effect that amplifies the damage to oral tissues. Individuals who drink 3.5 or more alcoholic drinks per day are 2-6 times more likely to develop oral cancer than non-drinkers.
Human Papillomavirus (HPV) Infection
Certain strains of HPV, particularly HPV-16, are a growing cause of oral (specifically oropharyngeal) cancers, especially in younger, non-smoking individuals. HPV is a sexually transmitted infection, and oral HPV infections can be transmitted through oral sex. The HPV vaccine can prevent infection with the strains most commonly associated with cancer.
Sun Exposure
Prolonged and unprotected exposure to the sun's ultraviolet (UV) rays can cause cancer of the lips, particularly the lower lip. This is similar to skin cancer development.
Other Contributing Factors
- Age: The risk of oral cancer increases with age, with most diagnoses occurring in people over 55, though HPV-related cases can occur earlier.
- Gender: Men are about twice as likely to develop oral cancer as women.
- Poor Nutrition: A diet low in fruits and vegetables and high in processed foods may increase risk.
- Weakened Immune System: Individuals with compromised immune systems (e.g., organ transplant recipients, HIV/AIDS patients) have a higher risk.
- Genetics: A family history of oral cancer or other head and neck cancers might indicate a slightly increased risk, though it's less of a factor than tobacco/alcohol.
- Chronic Irritation: While not a direct cause, chronic irritation from ill-fitting dentures, jagged teeth, or poor oral hygiene can create an environment where cells are more susceptible to cancerous changes, especially in the presence of other risk factors.
Signs and Symptoms: What to Look For
Recognizing the first signs of mouth cancer is crucial for early detection. Many early signs are subtle and can mimic less serious conditions, making vigilance and professional examination critical. If any of these symptoms persist for more than two weeks, it warrants immediate attention from a dentist or oral surgeon.
Visual and Palpable Changes
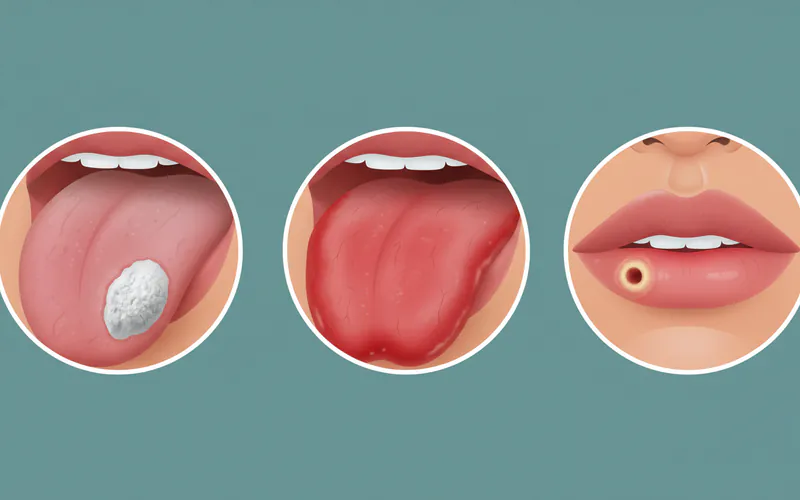
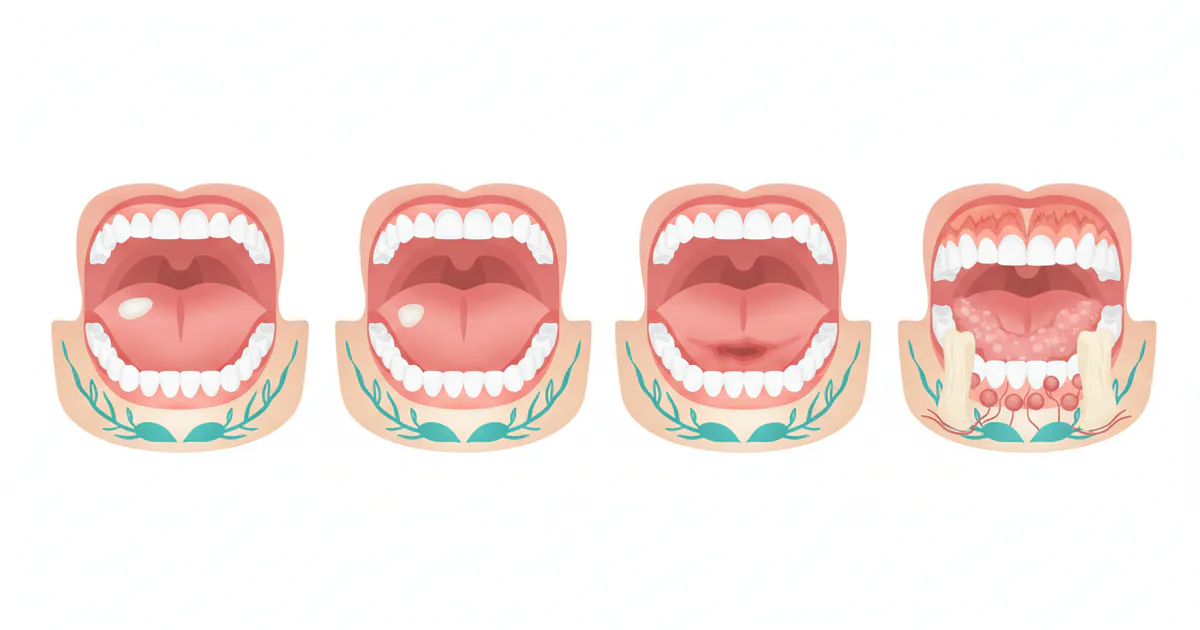
- Persistent Sore or Ulcer: A sore or ulcer in the mouth, on the lips, or on the tongue that does not heal within two weeks is the most common early sign. Unlike typical canker sores which heal quickly, a cancerous sore tends to persist, may be painless initially, and can have raised or rolled edges.
- Red or White Patches (Leukoplakia and Erythroplakia):
- Leukoplakia: These are white or grayish patches that appear on the tongue, gums, or inside of the cheeks. They are often rough or thick and cannot be scraped off. While many are benign, some (especially speckled leukoplakia) can be precancerous (dysplastic) and develop into cancer (Stage 0 or Stage I).
- Erythroplakia: These are bright red, velvety patches in the mouth. Erythroplakia is far less common than leukoplakia but has a much higher potential (up to 75-90%) of being or becoming cancerous. Any red patch in the mouth should be viewed with suspicion.
- Lumps, Bumps, or Thickening: A new lump, thickening, or hardened area on the lip, gum, cheek, or tongue. These can be painless at first and may be difficult to feel unless you specifically perform a self-exam.
- Numbness or Tingling: An unexplained numbness, tingling, or loss of feeling in any area of the mouth, face, or neck.
- Rough Spots or Crusting: Areas that feel rough, crusted, or eroded on the lips or inside the mouth.
Functional Symptoms
- Difficulty Chewing or Swallowing (Dysphagia): As a tumor grows, even slightly, it can interfere with normal mouth function.
- Difficulty Moving the Jaw or Tongue: Stiffness or pain when trying to open the mouth, chew, or move the tongue.
- Changes in Voice: Persistent hoarseness, a change in voice quality, or a feeling that something is caught in the throat.
- Unexplained Bleeding: Any unusual bleeding from the mouth or throat.
- Loose Teeth or Dentures: Teeth that become loose without a clear dental reason, or dentures that no longer fit properly.
- Persistent Sore Throat: A sore throat that doesn't go away, especially if accompanied by other symptoms.
- Unexplained Weight Loss: While more common in later stages, unexplained weight loss can sometimes be an early indicator.
Pro Tip: Perform a monthly self-examination of your mouth. Stand in front of a mirror with good lighting, examine your lips, cheeks, gums, tongue, and the floor and roof of your mouth. Look for any changes in color, texture, or the presence of any sores or lumps. If you find anything suspicious, schedule an appointment with your dentist promptly.
Treatment Options for 1st Oral Cancer Stages
Treatment for Stage 0 and Stage I oral cancer is typically highly successful due to the localized nature of the disease. The primary goal is complete eradication of the cancerous cells while preserving as much oral function and aesthetics as possible. Treatment often involves a multidisciplinary approach, with a team of specialists including oral surgeons, oncologists, radiation oncologists, and reconstructive surgeons.
1. Surgery (Primary Treatment)
For most Stage 0 and Stage I oral cancers, surgery is the initial and often curative treatment. The goal is to remove the tumor with clear margins (a rim of healthy tissue around the tumor).
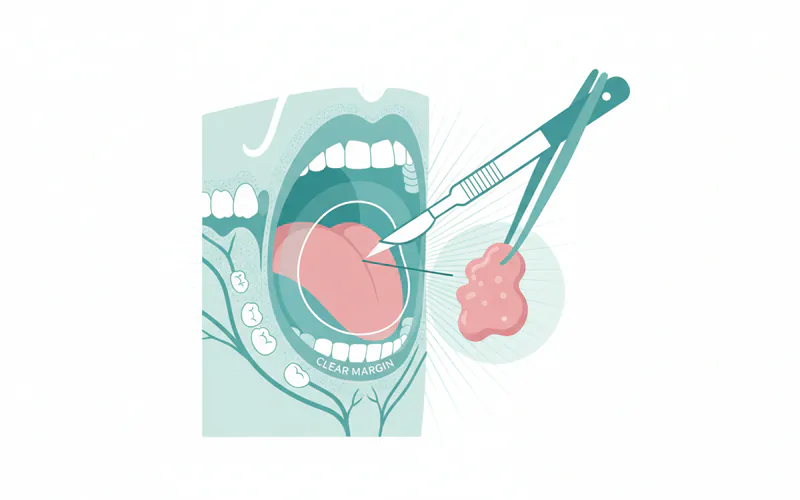
- Local Excision (Wide Local Excision): This is the most common surgical procedure for early-stage oral cancer. The surgeon carefully removes the tumor along with a surrounding margin of healthy tissue to ensure all cancerous cells are removed. The size of the margin depends on the tumor size and location.
- Pros: Often curative for early stages, preserves surrounding tissue, quicker recovery than more extensive surgeries.
- Cons: Potential for minor disfigurement depending on location, risk of infection, bleeding, or nerve damage.
- Mohs Micrographic Surgery: Less common for oral cancer but sometimes used for lip cancers. This specialized technique involves removing thin layers of cancerous tissue one at a time and examining each layer under a microscope until only cancer-free tissue remains.
- Pros: Maximizes preservation of healthy tissue, very high cure rates.
- Cons: Time-consuming, requires specialized training.
- Neck Dissection (Elective Neck Dissection): Even in Stage I, if there's a higher risk of microscopic spread to lymph nodes (e.g., depending on tumor depth or location), a surgeon might recommend removing a few lymph nodes in the neck (a "sentinel lymph node biopsy" or "elective neck dissection"). This is less common for pure Stage I and more for higher-risk early-stage cases or if the initial biopsy indicates aggressive features.
- Pros: Provides important staging information, removes potential hidden spread.
- Cons: More invasive, risk of nerve damage in the neck, longer recovery.
2. Radiation Therapy
Radiation therapy uses high-energy X-rays or other particles to kill cancer cells or keep them from growing. For early-stage oral cancer, radiation may be used:
- As a Primary Treatment (less common for Stage I, more for Stage 0 or if surgery is not feasible): Sometimes used instead of surgery for very small lesions, especially if surgery would result in significant cosmetic or functional impairment, or if the patient is not a surgical candidate.
- Adjuvant Therapy: After surgery, if pathology reports indicate high-risk features (e.g., positive margins, perineural invasion, lymphovascular invasion), radiation may be given to destroy any remaining cancer cells and reduce the risk of recurrence.
- Pros: Non-invasive (external beam), can effectively kill cancer cells.
- Cons: Side effects include dry mouth (xerostomia), difficulty swallowing, mucositis (mouth sores), taste changes, fatigue, skin irritation, and potential long-term jaw bone issues (osteoradionecrosis) or damage to salivary glands.
3. Chemotherapy and Targeted Therapy
Chemotherapy and targeted therapy are generally NOT primary treatments for Stage 0 or Stage I oral cancer. These therapies are typically reserved for:
- More advanced stages (Stage II or higher).
- Recurrent cancer.
- Cases where cancer has spread to lymph nodes or distant sites.
- As an adjunct to radiation in more complex cases (chemoradiation).
Pro Tip: Discuss all treatment options thoroughly with your multidisciplinary team. Understand the pros and cons of each, including potential side effects and their impact on your quality of life. Don't hesitate to seek a second opinion.
Step-by-Step Process: What to Expect
Navigating an oral cancer diagnosis and treatment can be daunting. Here’s a typical step-by-step process you can expect when dealing with 1st oral cancer stages:
-
Initial Consultation & Examination (Weeks 1-2):
- Your journey often begins with a routine dental check-up or an appointment due to a persistent symptom.
- Your dentist or doctor performs a thorough visual and tactile examination of your mouth and neck. They may use special lights (e.g., VELscope, Identafi) or rinses to highlight abnormal tissues.
- If a suspicious area is found, you'll likely be referred to an oral surgeon, ENT (Ear, Nose, and Throat) specialist, or periodontist for further evaluation.
-
Biopsy (Week 2-3):
- The definitive diagnostic step. A small tissue sample from the suspicious area is removed. This can be an incisional biopsy (part of the lesion) or an excisional biopsy (entire lesion for very small ones).
- The procedure is usually done under local anesthesia in an office setting.
- The tissue is sent to a pathologist who examines it under a microscope for cancer cells. Results typically take 3-7 business days.
- Cost: Biopsy procedures can range from $250 to $1,500 depending on the complexity, type of anesthesia, and facility fees.
-
Diagnosis Confirmation & Staging (Week 3-4):
- If the biopsy confirms cancer, the pathologist will identify the type and grade of cancer.
- To determine the exact stage (e.g., Stage 0 or Stage I), further imaging tests may be ordered to assess the tumor's size and check for spread:
- CT scan (Computed Tomography): Provides detailed cross-sectional images.
- MRI scan (Magnetic Resonance Imaging): Excellent for soft tissue detail, can show tumor extent.
- PET scan (Positron Emission Tomography): Can detect metabolically active cancer cells, useful for distant spread (less common for Stage 0/I).
- Endoscopy: Flexible tube with a camera to examine the throat and voice box.
- These tests help confirm the tumor (T) size and ensure no spread to lymph nodes (N) or distant sites (M), confirming the 1st oral cancer stages diagnosis.
-
Treatment Planning (Week 4-5):
- Once staging is complete, a multidisciplinary team (oral surgeon, oncologist, radiation oncologist, etc.) will meet to discuss your case and formulate a personalized treatment plan.
- For Stage 0 and Stage I, surgery (local excision) is typically the primary recommendation. Radiation might be discussed as an alternative or adjuvant therapy depending on specific factors.
-
Treatment Implementation (Weeks 5-8 onwards):
- Surgery: If surgery is chosen, it will be scheduled. This may be an outpatient procedure or require a short hospital stay, depending on the extent.
- Radiation Therapy: If radiation is necessary, it typically involves daily treatments (5 days a week) for several weeks (e.g., 5-7 weeks).
- During this phase, you will have regular appointments with your care team to monitor progress and manage side effects.
-
Recovery and Follow-up (Ongoing):
- After treatment, a period of recovery is necessary. This includes managing pain, nutritional support, and potentially speech or physical therapy.
- Regular follow-up appointments are critical to monitor for recurrence and manage long-term side effects. These often start every 1-3 months and gradually decrease in frequency over several years.
Cost and Insurance: US Price Ranges
The cost of diagnosing and treating oral cancer, even in its early stages, can vary significantly across the United States due to factors like geographic location, facility type (hospital vs. outpatient clinic), specific treatments chosen, and insurance coverage.
Diagnostic Costs (Without Insurance)
- Initial Consultation with Specialist: $150 - $600
- Biopsy (Incisional/Excisional): $250 - $1,500 (includes pathologist's fee)
- Imaging Scans (CT, MRI, PET):
- CT Scan: $300 - $3,000
- MRI Scan: $500 - $5,000
- PET Scan: $1,500 - $7,000 (often bundled with CT)
Treatment Costs (Without Insurance)
- Surgery (Local Excision for Stage I):
- Outpatient/Minor procedure: $5,000 - $15,000
- Hospital-based procedure (more complex, or with sentinel node biopsy): $15,000 - $30,000+
- This includes surgeon's fees, anesthesia, facility fees, and post-op care.
- Radiation Therapy (Full Course for Early Stage):
- $10,000 - $50,000+ for 5-7 weeks of daily treatments. This varies greatly based on technology (e.g., IMRT, proton therapy).
Total Estimated Costs for Early Stage Oral Cancer (Without Insurance)
A patient diagnosed and treated for Stage 0 or Stage I oral cancer might face total costs ranging from $15,000 on the low end (e.g., simple excision and no radiation) to $80,000+ on the high end (e.g., complex surgery, comprehensive staging, full course of advanced radiation).
Insurance Coverage
Most major health insurance plans (PPO, HMO, EPO, POS) in the US, as well as Medicare and Medicaid, typically cover a significant portion of oral cancer diagnosis and treatment. However, the extent of coverage depends on your specific plan:
- Deductibles: The amount you must pay out-of-pocket before your insurance starts to cover costs (can range from $500 to $10,000+ annually).
- Copayments: A fixed amount you pay for a doctor's visit or prescription.
- Coinsurance: The percentage of the cost you're responsible for after meeting your deductible (e.g., 10-30%).
- Out-of-Pocket Maximum: The most you'll have to pay for covered services in a plan year. Once you reach this limit, your insurance pays 100% of covered costs. These can range from $2,000 to $10,000+ for individuals, and higher for families.
Medicare: Generally covers medically necessary cancer treatments, including hospital stays, doctor fees, radiation, and diagnostic tests under Part A (hospital) and Part B (medical). Part D helps with prescription drugs. Medicaid: Covers low-income individuals and families, providing comprehensive coverage for cancer care, often with very low or no out-of-pocket costs. Private Insurance: Coverage details vary widely. It is essential to contact your insurance provider directly and understand your benefits, network providers, and pre-authorization requirements for procedures and medications.
Pro Tip: Before undergoing any major procedure, ask your healthcare provider for an estimate of costs and verify coverage with your insurance company. Many hospitals have financial counselors who can help you understand your benefits and explore payment plans.
Recovery and Aftercare
Recovery from early-stage oral cancer treatment focuses on healing, managing side effects, and restoring function. The specific aftercare depends on the treatment received (primarily surgery, sometimes radiation).
Immediate Post-Treatment (First 2-6 Weeks)
- Pain Management: You will likely experience pain after surgery. Your doctor will prescribe pain medication. Follow instructions carefully.
- Wound Care: If you had surgery, you'll receive instructions on how to care for the surgical site in your mouth or on your neck. This includes keeping the area clean and avoiding anything that might irritate it.
- Dietary Modifications: Soft foods will be recommended initially. Avoid spicy, acidic, crunchy, or hot foods that can irritate healing tissues. A diet rich in protein and nutrients is important for healing.
- Oral Hygiene: Gentle but thorough oral hygiene is crucial. Your dental team will guide you on appropriate techniques and products (e.g., non-alcoholic mouthwashes).
- Managing Side Effects of Radiation (if applicable):
- Mucositis: Painful mouth sores. Management includes special rinses, pain medication, and dietary adjustments.
- Dry Mouth (Xerostomia): Use saliva substitutes, drink plenty of water, and avoid caffeine and alcohol.
- Taste Changes: Foods may taste different or bland. Experiment with different seasonings and flavors.
- Skin Reactions: Redness, peeling, or soreness on the skin of the neck. Use gentle, non-irritating lotions as recommended.
- Fatigue: Rest is essential. Cancer treatment can be physically draining.
Long-Term Recovery and Follow-up (Months to Years)
- Regular Follow-up Appointments: This is paramount. For the first year or two, you'll likely see your oncologist or oral surgeon every 1-3 months. The frequency will gradually decrease to every 6 months, then annually, for at least 5 years. These appointments involve thorough oral examinations and sometimes imaging to monitor for recurrence.
- Dental Care: Continue regular dental check-ups and cleanings. Your dentist will be a key part of your surveillance team, looking for any new suspicious lesions.
- Speech and Swallowing Therapy: Depending on the location and extent of the cancer and treatment, you might need therapy to help regain normal speech and swallowing function.
- Nutritional Counseling: Ongoing support may be needed to maintain a healthy diet, especially if you experience persistent dry mouth or taste changes.
- Psychological Support: A cancer diagnosis and treatment can take a toll emotionally. Support groups, counseling, or therapy can be very beneficial.
- Lifestyle Changes: Reinforce preventive measures like quitting smoking/vaping and limiting alcohol to reduce the risk of secondary cancers.
Pro Tip: Maintain open communication with your entire healthcare team. Report any new or worsening symptoms immediately, even if they seem minor. Early detection of recurrence is as important as the initial diagnosis.
Prevention: How to Reduce Your Risk
Preventing oral cancer, especially minimizing the risk of developing the 1st oral cancer stages, involves a combination of lifestyle choices and regular medical vigilance.
- Avoid All Tobacco Products: This is the single most impactful step. Quit smoking cigarettes, cigars, pipes, and stop using all forms of smokeless tobacco, including chewing tobacco, snuff, and nicotine pouches like Zyn. The benefits of quitting begin immediately, and your risk significantly decreases over time.
- Moderate Alcohol Consumption: If you drink alcohol, do so in moderation. The American Dental Association (ADA) recommends limiting alcohol intake to no more than one drink per day for women and two drinks per day for men. Combining alcohol and tobacco creates a much higher risk than either substance alone.
- HPV Vaccination: The Human Papillomavirus (HPV) vaccine is highly effective in preventing infections from the strains of HPV most commonly associated with oral and oropharyngeal cancers (HPV-16, HPV-18). It is recommended for adolescents (typically around age 11-12) and can be given up to age 45, depending on individual risk factors and consultation with a doctor.
- Protect Your Lips from Sun Exposure: Use lip balm with SPF 30 or higher, and wear wide-brimmed hats when spending extended time outdoors to prevent lip cancer.
- Eat a Healthy, Balanced Diet: A diet rich in fruits and vegetables, which are high in antioxidants, may help reduce cancer risk. Limit processed foods and red meats.
- Maintain Excellent Oral Hygiene: Regular brushing, flossing, and using an antimicrobial mouthwash can help keep your mouth healthy and allow you to notice any changes more readily.
- Regular Dental Check-ups and Oral Cancer Screenings: Visit your dentist at least once a year, and ideally twice, for comprehensive oral exams. During these check-ups, your dentist performs a visual and tactile screening for signs of oral cancer. Early detection through these screenings is incredibly important.
- Perform Monthly Self-Exams: Get into the habit of performing a quick self-check of your mouth. Use a mirror to look at your lips, gums, tongue (top and bottom), cheeks, and the roof and floor of your mouth. Feel for any lumps or tender areas. If you notice any persistent changes, see your dentist immediately.
Risks and Complications
Even with early-stage oral cancer, there are potential risks and complications associated with the disease itself and its treatment.
Risks Related to the Cancer Itself
- Recurrence: Even after successful treatment of Stage 0 or Stage I cancer, there's a risk the cancer could return in the same area (local recurrence) or develop a new primary tumor in another part of the oral cavity or throat (field cancerization). This risk is highest in the first 2-5 years.
- Progression: If not detected and treated early, Stage 0 or Stage I cancer will progress to more advanced stages, making treatment more complex and less successful, and increasing the risk of spread to lymph nodes and distant organs.
Risks and Complications of Treatment
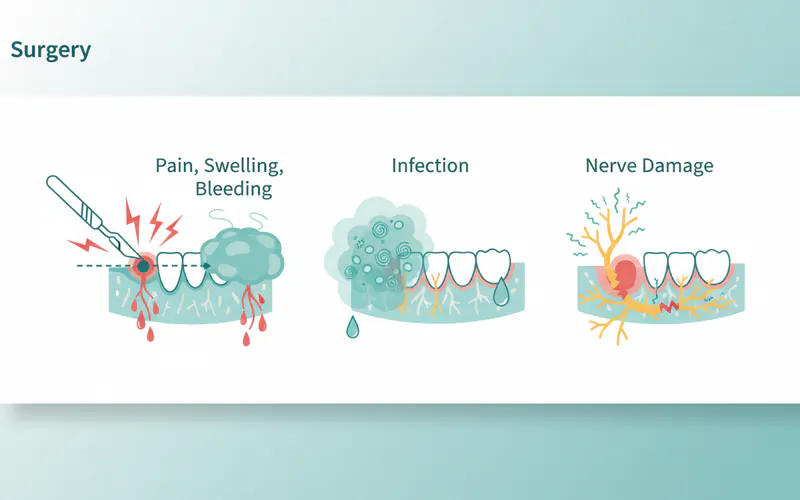
- Surgery:
- Pain, Swelling, Bleeding: Common post-operative issues.
- Infection: Risk at the surgical site.
- Nerve Damage: Depending on the tumor location, surgery can cause temporary or permanent numbness (e.g., tongue, lip) or weakness/paralysis of facial muscles.
- Functional Impairment: Difficulty with speech, chewing, or swallowing if significant tissue is removed.
- Cosmetic Changes: Scars or changes in facial appearance, especially for lip or external mouth surgeries.
- Radiation Therapy:
- Dry Mouth (Xerostomia): Can be temporary or permanent, leading to discomfort, difficulty eating, and increased risk of dental decay.
- Mucositis: Painful inflammation and sores in the mouth and throat.
- Taste Changes: Often temporary, but can persist.
- Difficulty Swallowing (Dysphagia): Due to inflammation or scarring.
- Fatigue: Common during and after treatment.
- Skin Changes: Redness, peeling, or tenderness in the treated area.
- Osteoradionecrosis (ORN): A serious long-term complication where radiation damages the jaw bone, leading to bone death and potential infection. This risk is low with modern radiation techniques but can be exacerbated by extractions or trauma in the irradiated area.
- Trismus: Jaw stiffness due to muscle scarring, making it difficult to open the mouth.
- Thyroid Problems: Radiation to the neck can affect thyroid function.
- Second Primary Cancers: Individuals who have had one oral cancer are at a higher risk of developing a new, second primary cancer in the head and neck region due to continued exposure to risk factors (e.g., tobacco, alcohol). This underscores the importance of continued prevention.
Comparison Table: Diagnostic vs. Biopsy
| Feature | Visual/Tactile Oral Exam | Biopsy (Incisional/Excisional) |
|---|---|---|
| Purpose | Screening, identify suspicious areas | Definitive diagnosis, determine cell type & malignancy |
| Method | Doctor/Dentist visually inspects, palpates mouth/neck | Small tissue sample surgically removed |
| Pain Level | None | Minimal (local anesthetic) |
| Duration | 5-10 minutes (part of routine exam) | 15-30 minutes (procedure) |
| Results | Immediate (suspicious findings) | 3-7 business days (pathology report) |
| Cost (No Ins.) | Included in exam (e.g., $50-$250) | $250 - $1,500 |
| Accuracy | High for identifying suspicion, low for definitive diagnosis | 100% for definitive diagnosis (if sample is adequate) |
| Key Advantage | Non-invasive, quick, first line of defense | Gold standard for cancer diagnosis and staging |
Comparison Table: Early Stage Treatment Options
| Treatment Option | Primary Use (1st Stages) | Typical Duration | Side Effects (Common) | Cost Range (No Ins.) | Recovery Time (Typical) |
|---|---|---|---|---|---|
| Local Excision (Surgery) | Primary for Stage 0 & I (removes tumor) | Single procedure (1-2 hours) | Pain, swelling, bleeding, temporary numbness, potential minor scarring | $5,000 - $30,000 | 2-6 weeks |
| Radiation Therapy (External Beam) | Adjuvant after surgery; rarely primary for small lesions (Stage 0) | 5-7 weeks (daily, 5x/week) | Dry mouth, mucositis, taste changes, fatigue, skin irritation | $10,000 - $50,000 | Weeks to months (side effects) |
Children / Pediatric Considerations
Oral cancer, particularly squamous cell carcinoma, is exceedingly rare in children. When oral malignancies do occur in pediatric populations, they are more commonly other types of cancer, such as:
- Rhabdomyosarcoma: A cancer of soft tissue, often found in the head and neck.
- Lymphoma: Can occur in the oral cavity.
- Leukemia: Manifestations can sometimes be seen in the oral cavity (e.g., gum swelling).
Risk factors commonly associated with adult oral cancer, like tobacco and alcohol use or extensive sun exposure, are generally not applicable to children. If a child develops suspicious oral lesions, especially those that are persistent or rapidly growing, it warrants immediate investigation by a pediatric dentist or an oral and maxillofacial surgeon. Diagnosis would still involve a biopsy, but the approach and differential diagnosis would be tailored to pediatric pathology. Parents should ensure children receive regular dental check-ups, and any unusual sores, lumps, or discolorations that don't resolve within a week or two should be evaluated by a dental professional.
Frequently Asked Questions
How painful is oral cancer detection and treatment?
The initial detection of oral cancer via a visual exam is painless. A biopsy is performed under local anesthesia, so you'll feel minimal pain during the procedure, similar to a dental filling. Post-biopsy discomfort is usually mild and managed with over-the-counter pain relievers. Early-stage surgical treatment involves pain, which is managed with prescription medication and typically subsides significantly within a few days to weeks. Radiation therapy can cause painful side effects like mucositis, but these are actively managed by your care team.
What is the survival rate for Stage 1 oral cancer?
The 5-year survival rate for Stage I oral cancer is excellent, generally 85% or higher. This means that 85% or more of individuals diagnosed with Stage I oral cancer are still alive five years after their diagnosis. This significantly higher rate underscores the critical importance of early detection compared to later stages.
How long does treatment for early oral cancer take?
For Stage 0 or Stage I oral cancer, treatment is often relatively quick. If surgery is the only treatment, it's typically a single procedure, with recovery taking 2-6 weeks. If adjuvant radiation therapy is needed, it adds another 5-7 weeks of daily treatments. Overall, the active treatment phase usually concludes within 2-3 months, followed by ongoing surveillance.
Can oral cancer be misdiagnosed?
While dentists and specialists are trained to identify suspicious lesions, some early signs of oral cancer can mimic benign conditions like canker sores, fungal infections, or benign fibromas. This is why persistence (not healing within two weeks) is a critical red flag, and a biopsy is the only definitive diagnostic tool to avoid misdiagnosis. Always advocate for a biopsy if a lesion is highly suspicious and doesn't resolve.
Are there non-surgical alternatives for early oral cancer?
For Stage I oral cancer, surgery (local excision) is generally the preferred and most effective treatment. Radiation therapy can sometimes be used as a primary treatment for very small or superficial lesions, especially if surgery would cause significant functional or cosmetic issues, or if the patient has other health conditions that make surgery risky. However, radiation may have its own set of side effects.
Does dental insurance cover oral cancer treatment?
Traditional dental insurance primarily covers routine dental care and restorative procedures. While it might cover the initial biopsy or some dental prosthetics after treatment, major oral cancer treatments like surgery and radiation therapy are typically covered by your medical health insurance plan. It's crucial to understand your medical insurance benefits regarding cancer care.
How often should I get screened for oral cancer?
The American Dental Association (ADA) recommends that all adults receive a visual and tactile oral cancer screening at least once a year as part of their routine dental check-up. Individuals with higher risk factors (e.g., tobacco users, heavy alcohol drinkers, history of HPV) may benefit from more frequent screenings.
What happens if oral cancer comes back after early treatment?
If oral cancer recurs after early-stage treatment, the approach depends on the location of the recurrence, its size, and whether it has spread. Treatment may involve repeat surgery, radiation therapy (if not used previously or if appropriate), chemotherapy, or targeted therapy. Regular follow-up appointments are vital for detecting recurrence early.
Can I get oral cancer even if I don't smoke or drink?
Yes, you can. While tobacco and alcohol are major risk factors, about 25% of oral cancer cases occur in people who do not smoke or drink. HPV infection is an increasingly common cause, and factors like genetics, sun exposure (for lip cancer), and unexplained causes can also contribute. Therefore, regular screenings are important for everyone.
What should I do if I find a suspicious spot in my mouth?
If you find a sore, lump, red or white patch, or any other unusual change in your mouth that persists for more than two weeks, schedule an appointment with your dentist or an oral surgeon immediately. Do not delay, as early diagnosis is key to successful treatment of the 1st oral cancer stages.
When to See a Dentist
Given the critical importance of early detection for 1st oral cancer stages, knowing when to seek professional dental attention is paramount. Do not delay if you notice any of the following warning signs:
- Persistent Sore or Ulcer: Any sore, ulcer, or irritation in your mouth, on your tongue, lips, or gums that does not heal within two weeks. Unlike a typical canker sore, a cancerous lesion often won't hurt initially and won't go away.
- Red or White Patches: The appearance of a new, unexplained red (erythroplakia) or white (leukoplakia) patch on the lining of your mouth or tongue. Remember that red patches have a particularly high risk of being or becoming cancerous.
- Lumps, Bumps, or Thickening: Any new lump, thickening, or hard spot in your mouth, on your lip, cheek, or neck that you can feel or see.
- Unexplained Numbness: A sudden or persistent feeling of numbness, tingling, or loss of sensation in any area of your mouth or face.
- Difficulty with Oral Functions: Persistent trouble chewing, swallowing, speaking, or moving your tongue or jaw.
- Loose Teeth or Ill-fitting Dentures: If your teeth suddenly become loose without an obvious dental reason, or if your dentures no longer fit comfortably.
- Persistent Sore Throat or Hoarseness: A chronic sore throat or voice change that doesn't resolve within a couple of weeks.
Red Flags vs. Routine Care: While routine dental check-ups (every 6-12 months) are essential for general oral health and early oral cancer screenings, the persistent symptoms listed above are red flags that warrant an immediate, dedicated appointment. Do not wait for your next scheduled check-up.
Emergency vs. Scheduled Appointment: Most early oral cancer symptoms do not constitute a dental emergency requiring an emergency room visit unless they are accompanied by severe pain, uncontrollable bleeding, or airway obstruction. However, they do require a prompt scheduled appointment with your dentist or an oral surgeon (within a few days to a week). Be clear with the dental office about your symptoms and concerns when you call to schedule, as this may help them prioritize your visit. Early action dramatically improves outcomes for the 1st oral cancer stages.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Floor of Mouth Cancer: Complete Guide
Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral c
February 23, 2026
Oral Cancer Stages Pictures: Complete Guide
Oral cancer, a serious and potentially life-threatening disease, affects thousands of Americans each year. According to the American Cancer Society, approximately 54,000 new cases of oral cavity or oropharyngeal cancer are diagnosed annually in the United States. While these numbers can be daunt
February 23, 2026
Can You Die From Mouth Cancer
Oral cancer is a formidable disease, often striking with insidious subtlety before revealing its devastating potential. It's a question that weighs heavily on the minds of those who receive a diagnosis or even those simply concerned about unusual oral symptoms: can you die from mouth cancer? The
February 23, 2026

Mouth Cancer Photos: Complete Guide
Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,23
February 23, 2026