Oral Cancer Roof of Mouth: Complete Guide

Key Takeaways
- Each year, thousands of Americans receive a life-altering diagnosis of oral cancer. While often associated with the tongue, lips, or throat, a lesser-known but equally critical form of this disease can manifest in an area you might overlook: the roof of your mouth. **Oral cancer on the roof of the m
Oral Cancer Roof of Mouth: Complete Guide
Each year, thousands of Americans receive a life-altering diagnosis of oral cancer. While often associated with the tongue, lips, or throat, a lesser-known but equally critical form of this disease can manifest in an area you might overlook: the roof of your mouth. Oral cancer on the roof of the mouth, specifically affecting the hard palate, demands our attention due to its potential for rapid progression and the serious implications it can have on your ability to speak, eat, and live comfortably. Early detection is paramount, yet many are unaware of the subtle signs and risk factors.

This comprehensive guide from SmilePedia.net aims to shed light on oral cancer of the hard palate, providing you with the knowledge needed to understand, identify, and proactively address this condition. We'll delve into what it is, what causes mouth cancer in this specific area, the tell-tale signs and symptoms, the range of available treatment options, and crucial prevention strategies including leukoplakia self-care. Our goal is to empower you with medically accurate information, enabling you to recognize potential issues early and seek timely professional care, ultimately improving outcomes and preserving your oral health.
Key Takeaways:
- Prevalence: Oral cancer of the roof of the mouth (hard palate) accounts for a smaller percentage of all oral cancers but can be aggressive. Overall, oral cancers affect over 54,000 Americans annually.
- Early Detection is Crucial: The 5-year survival rate significantly improves when detected in early stages (localized disease, ~85%) compared to late stages (distant metastasis, ~39%).
- Primary Causes: Tobacco use (smoking and smokeless) and excessive alcohol consumption are the leading risk factors for oral cancer, including those affecting the palate.
- Common Symptoms: Persistent red or white patches (leukoplakia, erythroplakia), non-healing sores, lumps, or pain on the roof of the mouth lasting more than two weeks warrant immediate dental evaluation.
- Treatment Pathways: Standard treatment involves surgery, often combined with radiation therapy, chemotherapy, or targeted therapies, tailored to the cancer's stage and type.
- Cost Implications: Oral cancer treatment can range from $25,000 to over $100,000 for comprehensive care, depending on stage, treatment modality, and location. Insurance typically covers a significant portion, but out-of-pocket costs can still be substantial, often in the thousands to tens of thousands.
- Prevention & Self-Care: Avoiding tobacco and excessive alcohol, maintaining a healthy diet, and regular dental check-ups (including oral cancer screenings) are vital. For precancerous lesions like leukoplakia, professional monitoring and elimination of risk factors are key aspects of leukoplakia self-care, but self-treatment is not advised.
What Is Oral Cancer of the Roof of the Mouth?
Oral cancer, also known as oral cavity cancer, refers to malignant (cancerous) growths that develop in any part of the mouth. When we specifically talk about oral cancer on the roof of the mouth, we are referring to cancers that originate on the hard palate, which is the bony front part of the roof of your mouth, separating your oral cavity from your nasal cavity. This area is covered by a specialized type of tissue known as stratified squamous epithelium.
Most oral cancers, including those on the hard palate, are squamous cell carcinomas (SCCs). These cancers arise from the flat, thin squamous cells that line the inside of the mouth. While the hard palate might seem like a less common site compared to the tongue or lips, it is a significant location because cancers here can invade underlying bone and spread to lymph nodes if not detected and treated early. The texture and appearance of the hard palate – often firm and ridged – can sometimes make subtle changes difficult to notice without careful examination. Recognizing what constitutes a normal oral palate is the first step in identifying potential abnormalities.
Types of Oral Cancer Affecting the Palate
While squamous cell carcinoma is the most prevalent form of oral cancer, other types can also affect the roof of the mouth. Understanding these variations is crucial for accurate diagnosis and effective treatment planning.
Squamous Cell Carcinoma (SCC)
This is by far the most common type, accounting for over 90% of all oral cancers. SCCs originate from the squamous cells that line the surface of the hard palate. They can appear as white patches (leukoplakia), red patches (erythroplakia), a mix of red and white, non-healing sores, or a lump. Its aggressive nature means it can quickly invade deeper tissues and spread to regional lymph nodes.
Minor Salivary Gland Cancers
The hard palate is home to numerous minor salivary glands. Cancers can arise from these glands, even though they are less common than SCCs. These include:
- Adenoid Cystic Carcinoma: A relatively rare type known for its tendency to spread along nerves (perineural invasion) and have a high recurrence rate, even years after initial treatment.
- Mucoepidermoid Carcinoma: The most common malignant salivary gland tumor, which can occur in minor salivary glands throughout the oral cavity, including the hard palate. Its aggressiveness varies, from low-grade to high-grade forms.
- Polymorphous Adenocarcinoma: Another type that originates in minor salivary glands, typically found in the palate. It often has a slow growth pattern but can metastasize over time.
Melanoma
Oral melanoma is exceedingly rare, representing less than 1% of all oral malignancies. However, it can appear on the hard palate. Like skin melanoma, oral melanoma arises from melanocytes (pigment-producing cells) and is highly aggressive, with a poor prognosis due to its tendency for early metastasis. It typically presents as a dark, discolored lesion (brown, black, blue), but can also be amelanotic (non-pigmented).
Lymphoma
Very rarely, lymphomas can manifest in the oral cavity, sometimes affecting the palate. These cancers originate from lymphocytes, a type of white blood cell, and are part of a broader category of blood cancers. Oral lymphomas may present as swellings or masses.
The specific type of cancer will dictate the exact treatment approach and influence the prognosis, underscoring the importance of a precise histopathological diagnosis through biopsy.
What Causes Mouth Cancer on the Roof of the Mouth?
Understanding what causes mouth cancer is the first step towards prevention. While some cases occur without clear risk factors, the vast majority are linked to specific lifestyle choices and environmental exposures. For oral cancer on the roof of the mouth, the primary culprits often parallel those for other oral cavity cancers.
Major Risk Factors
- Tobacco Use (All Forms): This is the single largest preventable risk factor.
- Smoking: Cigarettes, cigars, and pipes contain numerous carcinogens that directly irritate the oral tissues, including the palate. The heat from smoking also plays a role.
- Smokeless Tobacco: Products like chewing tobacco, snuff, and dip are particularly dangerous for the roof of the mouth and gums. Users often hold these products directly against the mucous membranes, leading to prolonged exposure to potent carcinogens. The prolonged irritation and chemical exposure significantly increase the risk of squamous cell carcinoma and precancerous lesions like leukoplakia.
- Excessive Alcohol Consumption: Heavy alcohol use is another significant risk factor. When combined with tobacco, the risk multiplies dramatically (synergistic effect). Alcohol acts as a solvent, allowing carcinogens from tobacco to penetrate oral tissues more easily.
- Human Papillomavirus (HPV) Infection: Certain high-risk strains of HPV, particularly HPV-16, are a growing cause of oropharyngeal cancers (back of the throat, base of tongue, tonsils). While less commonly associated with the hard palate directly compared to the oropharynx, HPV can still contribute to oral cancers in other areas of the mouth.
- Ultraviolet (UV) Light Exposure: While primarily a risk factor for lip cancer, prolonged sun exposure can also contribute to overall oral and head and neck cancer risk, especially for those with outdoor occupations.
- Poor Nutrition: A diet consistently low in fruits and vegetables, which are rich in antioxidants, may increase susceptibility to various cancers, including oral cancer.
- Compromised Immune System: Individuals with weakened immune systems (e.g., due to HIV/AIDS, organ transplant recipients on immunosuppressive drugs) have a higher risk of developing certain cancers, including some oral cancers.
- Chronic Irritation: While less direct than tobacco or alcohol, chronic irritation from ill-fitting dentures, sharp teeth, or constant rubbing might create an environment conducive to malignant changes over a very long period. However, this is not a primary direct cause, but rather a factor that warrants monitoring.
- Age: The risk of oral cancer generally increases with age, with most diagnoses occurring in individuals over 45.
- Gender: Historically, men have been diagnosed with oral cancer more frequently than women, largely due to higher rates of tobacco and alcohol use. However, this gap is narrowing.
Precancerous Conditions
Certain conditions on the roof of the mouth are not cancer but have the potential to become cancerous over time. Recognizing and managing these is a critical part of prevention.
- Leukoplakia: White patches or plaques on the mucous membranes that cannot be scraped off and cannot be classified as any other diagnosable disease. While many are benign, a significant percentage (5-10%, some sources state up to 17%) can undergo malignant transformation, especially if they show dysplastic changes on biopsy.
- Erythroplakia: Red patches on the mucous membranes. These are less common than leukoplakia but have a much higher rate of malignant transformation (up to 90% in some studies). They are considered highly suspicious.
- Erythroleukoplakia (Speckled Leukoplakia): A combination of red and white patches, carrying a significant risk of malignancy.
Pro Tip: If you have leukoplakia or erythroplakia, diligent monitoring by a dental professional is absolutely essential. Leukoplakia self-care primarily involves avoiding known risk factors like tobacco and alcohol, and strict adherence to your dentist's follow-up schedule. Never attempt to self-treat or ignore these lesions.
Signs and Symptoms of Oral Cancer on the Roof of the Mouth
Early detection of oral cancer on the roof of the mouth relies on your awareness of your own oral health and regular professional screenings. The symptoms can be subtle at first, often painless, which is why routine dental check-ups are so vital. Look for any of the following changes that persist for more than two weeks:
- Persistent Red or White Patches (Leukoplakia/Erythroplakia):
- Leukoplakia: A white or grayish patch that cannot be wiped away. While often benign, it can be precancerous. On the roof of the mouth, these might appear as flat, irregular areas.
- Erythroplakia: A bright red, velvety patch. This is less common than leukoplakia but much more likely to be precancerous or cancerous.
- Erythroleukoplakia: A lesion with both red and white areas, which is highly suspicious.
- A Sore or Ulcer That Doesn't Heal: Any sore on the roof of your mouth that doesn't improve or go away within two weeks, especially if it's painless, should be evaluated.
- A Lump, Thickening, or Swelling: Feeling a new bump, growth, or an area of thickening on the hard palate that wasn't there before. This might be firm to the touch.
- Persistent Pain or Tenderness: While often painless in early stages, some individuals may experience a persistent sore throat, pain in the mouth or ear, or difficulty swallowing. Pain on the roof of the mouth that doesn't resolve.
- Difficulty Chewing, Swallowing (Dysphagia), or Speaking (Dysarthria): As the tumor grows, it can interfere with the normal function of your mouth and throat.
- Numbness (Paresthesia) or Loss of Sensation: A feeling of numbness or a burning sensation in any area of the mouth or face.
- Loose Teeth or Dentures That No Longer Fit Well: If the cancer invades the underlying bone, it can lead to teeth becoming loose or make existing dentures uncomfortable or ill-fitting.
- Unexplained Bleeding in the Mouth: Any unusual or persistent bleeding from the roof of the mouth without an obvious cause.
- Persistent Bad Breath (Halitosis): While many factors cause bad breath, a persistent, foul odor that doesn't improve with oral hygiene could be a symptom of underlying pathology.
- Unexplained Weight Loss: In more advanced stages, difficulty eating or the metabolic demands of cancer can lead to unintentional weight loss.
- Swelling in the Jaw or Neck: Enlarged lymph nodes in the neck can indicate that the cancer has spread beyond the primary site.
Pro Tip: Perform a self-check monthly. Use a good light and a mirror. Feel the roof of your mouth with your tongue and finger. Look for any changes in color, texture, or the presence of lumps or sores. Early detection makes a significant difference in treatment outcomes.
Treatment Options for Oral Cancer of the Roof of the Mouth
The treatment plan for oral cancer on the roof of the mouth is highly individualized, depending on the type and stage of cancer, its exact location, your overall health, and personal preferences. A multidisciplinary team of specialists, including oral and maxillofacial surgeons, oncologists, radiation oncologists, dentists, and reconstructive surgeons, will typically collaborate to devise the most effective strategy.
1. Surgery
Surgery is often the primary treatment for oral cancer of the hard palate, especially in early stages.
- Resection: This involves surgically removing the tumor along with a margin of healthy tissue around it to ensure all cancerous cells are excised. For hard palate cancers, this may involve removing a portion of the palate bone.
- Pros: Can be curative for early-stage cancers; offers immediate tumor removal.
- Cons: Can be extensive and may require reconstructive surgery; potential for disfigurement, speech, and swallowing difficulties.
- Neck Dissection: If the cancer has spread or is suspected to have spread to the lymph nodes in the neck, these lymph nodes will be surgically removed.
- Pros: Prevents further spread of cancer; improves staging accuracy.
- Cons: Can lead to nerve damage, stiffness, and swelling in the neck (lymphedema).
- Reconstructive Surgery: After removing a significant portion of the palate or surrounding structures, reconstructive surgery may be necessary to restore function (eating, speaking) and aesthetics. This can involve using tissue flaps (e.g., from the arm or leg) or skin grafts. Dental prosthetics (obturators) can also be used to close defects in the palate.
- Pros: Improves quality of life; restores oral function.
- Cons: Complex procedures; requires specialized surgical expertise; additional recovery time.
2. Radiation Therapy
Radiation therapy uses high-energy X-rays or other particles to kill cancer cells or inhibit their growth. It can be used as a primary treatment for early-stage cancers, after surgery (adjuvant therapy) to kill remaining cancer cells, or in combination with chemotherapy for more advanced stages.
- External Beam Radiation Therapy (EBRT): The most common type, where radiation is delivered from a machine outside the body. Intensity-Modulated Radiation Therapy (IMRT) is a sophisticated form that targets the tumor more precisely while sparing healthy surrounding tissues.
- Pros: Non-invasive; can spare certain functions better than extensive surgery; effective for specific types of tumors.
- Cons: Side effects can include dry mouth (xerostomia), mucositis (sore mouth), taste changes, difficulty swallowing, skin reactions, and potential for osteoradionecrosis (bone death) in severe cases. These side effects can be long-lasting.
- Brachytherapy: Less common for the hard palate, this involves placing radioactive sources directly into or near the tumor.
- Pros: Delivers a high dose of radiation directly to the tumor with minimal exposure to surrounding healthy tissue.
- Cons: Invasive; not suitable for all tumor locations.
3. Chemotherapy
Chemotherapy uses drugs to kill cancer cells throughout the body. It is often used in combination with radiation therapy (chemoradiation) for more advanced oral cancers or as a palliative treatment to control symptoms and improve quality of life for metastatic disease.
- Pros: Systemic treatment, can target cancer cells wherever they are in the body.
- Cons: Significant side effects due to impact on healthy rapidly dividing cells (nausea, fatigue, hair loss, mouth sores, increased infection risk, nerve damage).
4. Targeted Therapy and Immunotherapy
These are newer treatment modalities that are becoming more common, especially for advanced or recurrent oral cancers, or when traditional treatments are not effective.
- Targeted Therapy: Drugs that specifically target molecular pathways involved in cancer growth and spread (e.g., EGFR inhibitors).
- Pros: Often has fewer generalized side effects than traditional chemotherapy; more precise.
- Cons: Only effective for cancers with specific molecular targets; can be expensive.
- Immunotherapy: Drugs that help your body's own immune system fight cancer (e.g., checkpoint inhibitors).
- Pros: Can lead to long-lasting responses in some patients; distinct side effect profile.
- Cons: Not effective for all patients; can cause immune-related side effects; very expensive.
The choice of treatment is a complex decision made in close consultation with your oncology team, weighing the potential for cure against the impact on your quality of life.
Step-by-Step Process: From Diagnosis to Treatment
Navigating an oral cancer diagnosis and treatment can feel overwhelming. Here’s a general step-by-step overview of what to expect:
Step 1: Initial Examination and Screening
Your journey usually begins with a routine dental check-up or a visit for a persistent symptom. Your dentist performs a visual and tactile examination of your mouth, looking for any suspicious lesions, lumps, or discolorations. This initial screening is crucial for identifying potential issues early.
Step 2: Diagnostic Evaluation and Biopsy
If a suspicious area is found, your dentist will refer you to an oral surgeon or an ENT (Ear, Nose, and Throat) specialist.
- Visual Inspection and Palpation: The specialist will conduct a thorough examination.
- Biopsy: This is the only definitive way to diagnose cancer. A small tissue sample is taken from the suspicious lesion and sent to a pathologist for microscopic analysis. This can be an incisional biopsy (removing a small piece) or an excisional biopsy (removing the entire lesion if small).
- Imaging: If cancer is confirmed, imaging tests are ordered to determine the extent of the cancer (stage) and if it has spread. This may include:
- CT Scan (Computed Tomography): Provides detailed cross-sectional images to show tumor size, location, and spread to nearby structures or lymph nodes.
- MRI (Magnetic Resonance Imaging): Offers excellent soft tissue contrast, helpful for evaluating tumor depth and perineural invasion.
- PET Scan (Positron Emission Tomography): Helps detect cancer cells that have spread to other parts of the body, especially lymph nodes or distant sites.
- Chest X-ray: To check for lung involvement.
Step 3: Staging and Treatment Planning
Once all diagnostic information is gathered, your oncology team will determine the cancer's stage using the TNM (Tumor, Node, Metastasis) staging system. This describes the size of the primary tumor (T), whether it has spread to lymph nodes (N), and whether it has metastasized to distant sites (M).
- Tumor Board Review: Your case will likely be presented to a multidisciplinary "tumor board" – a group of specialists who discuss the findings and recommend the best treatment approach based on established guidelines and their collective expertise.
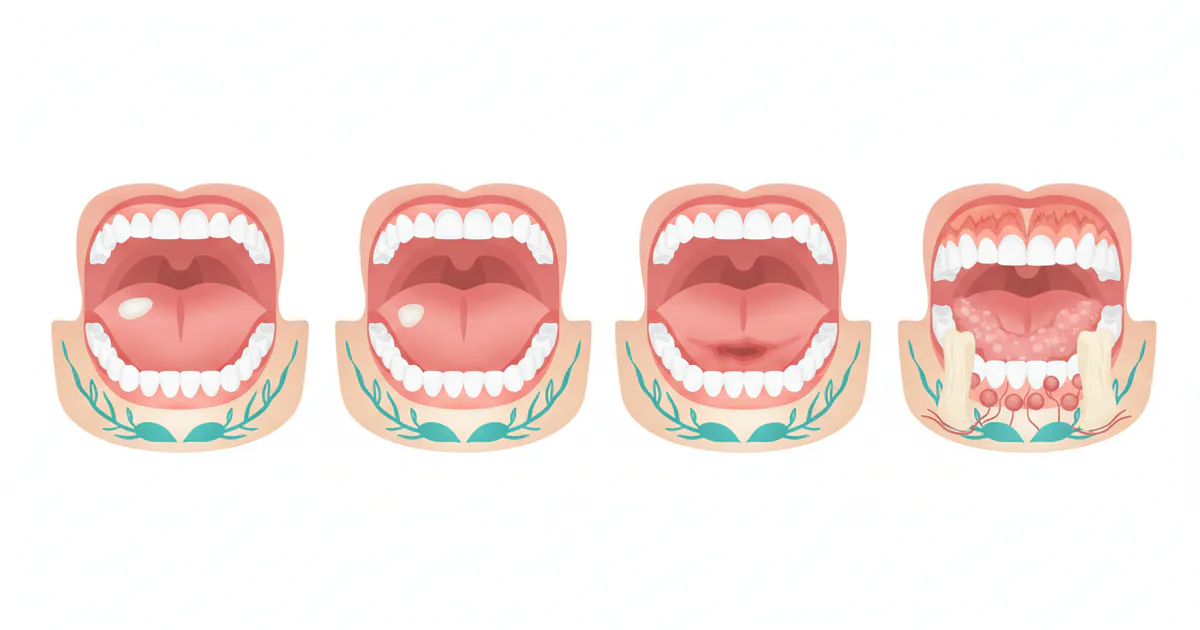
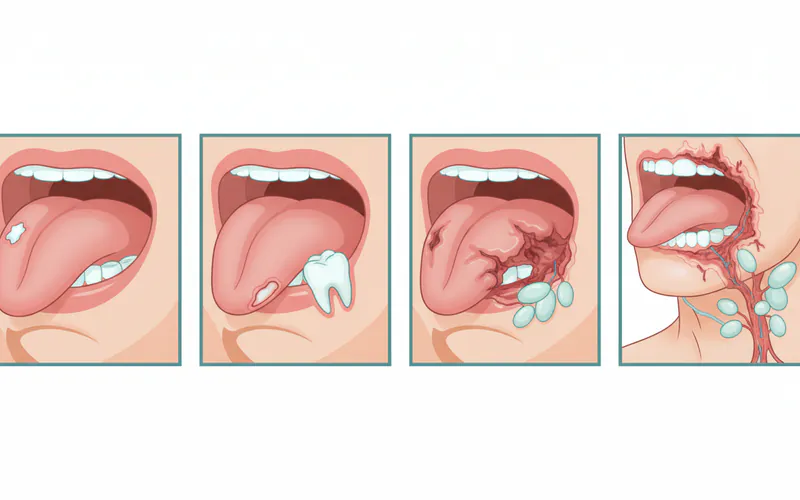 Image description: A series of four diagrams showing the progression of oral cancer on the hard palate. The first shows a small, localized lesion. The second shows a larger tumor beginning to invade deeper tissues. The third shows the tumor with involvement of nearby lymph nodes in the neck. The fourth shows a large tumor with distant metastasis depicted in other body areas.
Image description: A series of four diagrams showing the progression of oral cancer on the hard palate. The first shows a small, localized lesion. The second shows a larger tumor beginning to invade deeper tissues. The third shows the tumor with involvement of nearby lymph nodes in the neck. The fourth shows a large tumor with distant metastasis depicted in other body areas.
Step 4: Treatment Implementation
Based on the treatment plan:
- Surgery: If surgery is indicated, it will be scheduled. This may involve the primary tumor resection, potentially a neck dissection, and immediate reconstruction.
- Adjuvant Therapy: After surgery, you may undergo radiation therapy, chemotherapy, or both, to eliminate any remaining cancer cells and reduce the risk of recurrence. This typically begins several weeks after surgery to allow for initial healing.
- Non-Surgical Primary Treatment: In some cases (e.g., very early stage, or if surgery is not feasible), radiation therapy or chemoradiation may be the primary treatment.
Step 5: Recovery and Follow-up
The recovery process can be lengthy and involves several aspects:
- Post-Treatment Care: Managing pain, nutrition (often requiring a liquid or soft diet), and wound care.
- Rehabilitation: May include speech therapy, swallowing therapy, and physical therapy to help regain function.
- Dental Rehabilitation: Prosthetics (obturators) or dental implants may be needed to restore aesthetics and function.
- Surveillance: Regular follow-up appointments with your oncology team are crucial to monitor for recurrence or the development of second primary cancers. Initially, these may be every 1-3 months, gradually extending over several years.
Throughout this process, psychological and nutritional support are often integrated to help you cope with the challenges of cancer treatment.
Cost and Insurance for Oral Cancer Treatment
The financial burden of oral cancer treatment in the US can be substantial, varying widely based on the stage of cancer, chosen treatment modalities, geographical location, and whether you have insurance. It's important to be prepared for both direct medical costs and indirect expenses.
Estimated US Price Ranges (Without Insurance)
These are general ranges, and actual costs can be higher or lower.
- Initial Diagnosis & Staging:
- Dental Examination: $50 - $200
- Biopsy (including pathology fees): $300 - $1,500
- CT Scan: $500 - $3,000
- MRI Scan: $700 - $5,000
- PET Scan: $2,000 - $8,000
- Surgery:
- Tumor Resection (localized): $10,000 - $30,000
- Complex Resection with Neck Dissection: $25,000 - $70,000+
- Reconstructive Surgery: $15,000 - $100,000+ (depending on complexity and flap type)
- Radiation Therapy:
- Full Course (e.g., 6-7 weeks of IMRT): $20,000 - $60,000+
- Chemotherapy:
- Per Cycle (varies greatly by drug and regimen): $500 - $30,000+
- Full Course: $10,000 - $150,000+
- Targeted/Immunotherapy:
- Per Month: $10,000 - $20,000+ (can be for many months or years)
- Supportive Care & Rehabilitation:
- Speech/Swallowing Therapy: $100 - $300 per session
- Dental Prosthetics (Obturators): $2,000 - $15,000
Total Comprehensive Treatment (Early Stage): Can range from $25,000 - $75,000. Total Comprehensive Treatment (Advanced Stage with Reconstruction and Multiple Therapies): Can easily exceed $100,000 - $300,000.
Insurance Coverage Details
Most major medical insurance plans (PPO, HMO, EPO) will cover a significant portion of oral cancer treatment as it's considered a medical necessity. However, understanding your specific plan is crucial.
- Deductibles: The amount you must pay out-of-pocket before your insurance starts covering costs. These can range from a few hundred to several thousand dollars annually.
- Co-pays: A fixed amount you pay for a doctor's visit, prescription, or service.
- Co-insurance: The percentage of the cost you are responsible for after meeting your deductible (e.g., 20% co-insurance means your plan pays 80%, you pay 20%).
- Out-of-Pocket Maximum: The maximum amount you will have to pay for covered services in a plan year. Once you reach this limit, your insurance plan pays 100% of the cost for covered benefits. This is a crucial safety net for cancer treatment.
- Medicare/Medicaid:
- Medicare: Covers a large portion of cancer treatment for individuals 65 and older or those with certain disabilities. Part A covers hospital stays, Part B covers doctor's visits, outpatient care, and durable medical equipment, and Part D covers prescription drugs. Supplemental plans (Medigap) or Medicare Advantage plans can help cover out-of-pocket costs.
- Medicaid: Provides health coverage to low-income individuals and families. Coverage varies by state but generally covers essential health benefits, including cancer treatment.
Pro Tip: Before starting any extensive treatment, contact your insurance provider directly. Understand your deductible, co-insurance, out-of-pocket maximum, and any pre-authorization requirements for specific treatments or procedures. A financial counselor at the hospital or clinic can also help you navigate these complexities.
Table 1: Estimated Costs of Key Oral Cancer Treatment Components (US, without insurance)
| Treatment Component | Estimated Cost Range (USD) | Notes |
|---|---|---|
| Initial Diagnostic Tests | ||
| Dental Exam/Consultation | $50 - $200 | Varies by practitioner and region |
| Biopsy & Pathology | $300 - $1,500 | Includes specialist fees and lab analysis |
| CT/MRI/PET Scans | $500 - $8,000 per scan | PET scans are generally most expensive |
| Primary Treatments | ||
| Tumor Resection (Surgery) | $10,000 - $70,000+ | Depends on tumor size, location, and complexity |
| Neck Dissection (Surgery) | $15,000 - $50,000 | Often combined with primary tumor surgery |
| Reconstructive Surgery | $15,000 - $100,000+ | Varies widely based on tissue flap source and complexity |
| Radiation Therapy (Full Course) | $20,000 - $60,000+ | Typically 6-7 weeks, varies by technology (e.g., IMRT) |
| Chemotherapy (Per Cycle) | $500 - $30,000+ | Highly variable based on drug type, dosage, and duration |
| Targeted/Immunotherapy (Per Month) | $10,000 - $20,000+ | Newer therapies can be very costly, often long-term |
| Supportive Care | ||
| Speech/Swallowing Therapy | $100 - $300 per session | Multiple sessions often required |
| Dental Prosthetics (Obturator) | $2,000 - $15,000 | Custom-made device to close palatal defects |
Recovery and Aftercare
Recovery from oral cancer treatment, particularly for cancer on the roof of the mouth, is a multifaceted process that can be challenging but is crucial for regaining function and quality of life. The specific challenges depend on the extent of surgery, type of radiation, and whether chemotherapy was involved.
Immediate Post-Treatment
- Pain Management: You will experience pain, especially after surgery. Medications will be prescribed to manage this.
- Wound Care: If surgery involved grafts or flaps, meticulous wound care is essential to prevent infection and promote healing.
- Diet Modification: Swallowing can be difficult. You may need to start with a liquid diet, progressing to soft foods. In some cases, a feeding tube (nasogastric or gastrostomy) may be temporarily or permanently necessary.
- Oral Hygiene: Maintaining strict oral hygiene is vital, even with soreness. Special rinses may be prescribed, and careful brushing is recommended.
Rehabilitation and Long-Term Care
- Speech and Swallowing Therapy: Significant changes to the roof of the mouth can impact speech (articulation) and the ability to swallow effectively (dysphagia). A speech-language pathologist (SLP) will provide exercises and strategies to improve these functions. This may include exercises for jaw mobility, tongue strength, and swallowing techniques.
- Dental Rehabilitation:
- Prosthetics: If a portion of the hard palate was removed, a custom-made prosthetic device called an obturator can be fabricated by a prosthodontist. This closes the defect, restoring the ability to speak clearly and swallow without food or liquid entering the nasal cavity. Obturators require regular cleaning and adjustment.
- Dental Implants: After bone healing, dental implants may be an option to support new teeth, especially if teeth were lost during treatment.
- Managing Treatment Side Effects:
- Dry Mouth (Xerostomia): A common and often long-lasting side effect of radiation therapy. This can lead to increased risk of tooth decay, gum disease, and discomfort. Strategies include artificial saliva, fluoride treatments, frequent sips of water, and avoiding dry/spicy foods.
- Mucositis: Painful inflammation and ulceration of the mouth and throat lining, common during radiation and chemotherapy. Pain relief and special rinses are used.
- Taste Changes: Food may taste different or bland. This usually improves over time but can persist.
- Jaw Stiffness (Trismus): May occur after radiation or surgery. Jaw exercises can help maintain mobility.
- Lymphedema: Swelling in the face, neck, or jaw due to lymph node removal. Physical therapy and specialized massage can help.
- Osteoradionecrosis (ORN): A serious complication where bone in the radiated area dies. More common with higher radiation doses, smoking, and trauma. Requires specialized management.
- Nutritional Support: A registered dietitian can help you maintain adequate nutrition, which is crucial for healing and energy.
- Psychological Support: A cancer diagnosis and treatment can take a significant emotional toll. Support groups, counseling, and mental health professionals can provide invaluable assistance.
- Regular Follow-up: This is perhaps the most critical aspect of long-term care. You will have frequent appointments with your oncology team, oral surgeon, and dentist to monitor for recurrence and manage any late effects of treatment. These visits will typically involve thorough oral exams, palpation of lymph nodes, and potentially imaging. The American Dental Association (ADA) strongly recommends comprehensive oral exams at every recall appointment for all patients, emphasizing the visual and tactile inspection for any abnormalities.
Prevention of Oral Cancer on the Roof of the Mouth
Preventing oral cancer on the roof of the mouth largely involves eliminating or reducing exposure to known risk factors. While some factors are beyond our control, a significant portion of cases are preventable through lifestyle modifications and proactive health choices. This is where leukoplakia self-care and understanding what causes mouth cancer become incredibly powerful tools.
1. Eliminate Tobacco Use
This is the single most impactful preventive measure.
- Quit Smoking: Cease using cigarettes, cigars, and pipes. The risk of oral cancer decreases significantly within 5-10 years of quitting.
- Avoid Smokeless Tobacco: Discontinue use of chewing tobacco, snuff, and dip. These products are particularly damaging to the hard palate and gums.
- Avoid Vaping/E-cigarettes: While considered by some to be "safer" than traditional cigarettes, the long-term effects of vaping on oral tissues are still being studied, and they are not without potential harm.

2. Moderate Alcohol Consumption
- Limit Intake: If you drink alcohol, do so in moderation. For women, this means up to one drink per day; for men, up to two drinks per day.
- Avoid Concurrent Use: Never combine tobacco and alcohol, as their synergistic effect dramatically increases cancer risk.
3. Maintain a Healthy Diet
- Eat Plenty of Fruits and Vegetables: A diet rich in a variety of colorful fruits and vegetables provides antioxidants and essential nutrients that help protect against cancer. Aim for at least 5 servings daily.
- Limit Processed Foods and Sugary Drinks: These can contribute to inflammation and overall poor health.
4. Practice Excellent Oral Hygiene
- Brush and Floss Regularly: This helps remove plaque and bacteria, reducing inflammation and supporting overall oral health.
- Regular Dental Check-ups: The ADA recommends regular dental visits (typically every 6 months) for professional cleanings and comprehensive oral examinations, including oral cancer screenings. This is arguably the most vital step for early detection and prevention for the general population.
5. Get Screened Regularly
- Annual Oral Cancer Screenings: Your dentist or hygienist should perform a thorough oral cancer screening at every regular check-up. This involves visually inspecting your mouth and palpating your neck and jaw for lumps. Technologies like VELscope or Identafi may be used in some practices for enhanced visualization of suspicious lesions. Early detection of precancerous lesions (like leukoplakia) or early-stage cancers significantly improves prognosis.
6. Protect Against HPV
- HPV Vaccination: The HPV vaccine (Gardasil 9) is recommended for adolescents and young adults (typically ages 9-26) and can protect against the strains of HPV most commonly associated with oropharyngeal cancers. Discuss with your doctor if it's right for you or your children.
- Safe Sexual Practices: Reduces the risk of HPV transmission.
7. Leukoplakia Self-Care (and Professional Care)
It's crucial to understand that leukoplakia self-care is not about treating the lesion yourself, but rather about proactive monitoring and risk factor reduction in conjunction with professional oversight.
- Monitor Any White Patches: If you notice any persistent white patches on your roof of mouth or anywhere else, note their size, location, and persistence.
- Eliminate Irritants: If you smoke or use smokeless tobacco, stopping is the most critical step. If an ill-fitting denture or sharp tooth is causing chronic irritation, address it promptly with your dentist.
- Regular Professional Evaluation: Any lesion suspected to be leukoplakia must be evaluated by a dentist or oral surgeon. They may recommend a biopsy to determine if the cells are dysplastic (precancerous) or cancerous. Even if benign, regular follow-up is essential, as leukoplakia can transform into cancer over time. Do NOT ignore it.
Table 2: Characteristics of Precancerous Lesions (Leukoplakia vs. Erythroplakia)
| Feature | Leukoplakia (White Patch) | Erythroplakia (Red Patch) |
|---|---|---|
| Appearance | White or gray, flat, irregular, non-scrapable | Bright red, velvety, smooth or granular |
| Prevalence | More common | Less common |
| Malignant Transformation Rate | 5-17% (average) | Up to 90% (much higher risk) |
| Symptoms | Usually asymptomatic | Often asymptomatic, may be sensitive |
| Etiology | Often associated with tobacco/alcohol | Often associated with tobacco/alcohol |
| Management | Biopsy, regular monitoring, risk factor cessation | Urgent biopsy, often excision due to high risk |
| Self-Care Implication | Monitor, avoid irritants, professional evaluation mandatory | Monitor, avoid irritants, professional evaluation mandatory and urgent |
Risks and Complications
Oral cancer, particularly on the roof of the mouth, and its treatment carry various risks and potential complications. Awareness of these can help you and your care team manage them effectively.
From the Cancer Itself
- Local Invasion: The cancer can grow into adjacent structures like the nasal cavity, sinuses, underlying bone (palate, maxilla), or even the brain in advanced stages.
- Metastasis: Spread to regional lymph nodes in the neck is common, and from there, it can spread to distant organs (lungs, liver, bones), significantly worsening the prognosis.
- Functional Impairment: Difficulty eating, swallowing, and speaking due to tumor growth.
- Pain and Discomfort: As the tumor grows, it can cause significant pain.
From Treatment
- Surgical Complications:
- Infection and Bleeding: Standard surgical risks.
- Nerve Damage: Can lead to numbness, weakness, or paralysis of facial muscles, tongue, or jaw. This can be temporary or permanent.
- Fistula Formation: An abnormal connection between two organs or between an organ and the skin (e.g., oro-nasal fistula if the palate defect doesn't close completely).
- Disfigurement: Removal of tissue from the palate and surrounding areas can alter facial appearance and oral structures, even with reconstruction.
- Speech and Swallowing Difficulties: Post-surgical changes can profoundly affect these functions, sometimes requiring long-term therapy or dietary modifications.
- Radiation Therapy Complications:
- Xerostomia (Dry Mouth): Permanent damage to salivary glands, leading to chronic dry mouth, increased risk of dental decay, and discomfort.
- Mucositis: Severe inflammation and sores in the mouth and throat, causing intense pain and difficulty eating.
- Osteoradionecrosis (ORN): Death of bone tissue due to radiation, which can be extremely painful and debilitating, sometimes requiring surgical removal of the affected bone. This risk is particularly relevant for the hard palate.
- Trismus: Jaw stiffness due to fibrosis of muscles involved in chewing.
- Taste Changes: Often long-lasting.
- Skin Changes: Redness, peeling, and scarring in the radiated area.
- Chemotherapy Complications:
- Nausea, Vomiting, Fatigue, Hair Loss: Common systemic side effects.
- Myelosuppression: Reduced blood cell production, leading to increased risk of infection, anemia, and bleeding.
- Peripheral Neuropathy: Nerve damage, leading to numbness, tingling, or pain in extremities.
- Mouth Sores: Chemotherapy can also cause mucositis.
Long-Term Risks
- Cancer Recurrence: The cancer can return in the original site (local recurrence), in nearby lymph nodes (regional recurrence), or in distant parts of the body (distant metastasis).
- Second Primary Cancers: Individuals who have had one oral cancer are at a higher risk of developing a new, distinct cancer (second primary cancer) in the head and neck or other areas, especially if they continue to engage in high-risk behaviors like tobacco and alcohol use.
- Psychological Impact: Living with and surviving cancer can lead to anxiety, depression, fear of recurrence, and body image issues.
Children / Pediatric Considerations
Oral cancer of the roof of the mouth is exceedingly rare in children. When it does occur, it is often linked to different underlying causes compared to adults.
- Rarity: Unlike adults, where lifestyle factors like tobacco and alcohol are primary drivers, these are not typically relevant for pediatric oral cancers.
- Genetic Syndromes: Some rare genetic syndromes can predispose children to developing certain cancers, including those in the oral cavity.
- Specific Tumor Types: If a child develops an oral malignancy, it might be a different type than the squamous cell carcinoma common in adults, such as rhabdomyosarcoma (a type of soft tissue sarcoma), lymphoma, or specific types of salivary gland tumors.
- Diagnosis Challenges: Due to its rarity, diagnosis can sometimes be delayed as symptoms might be mistaken for more common childhood ailments.
- Parental Awareness: Parents should be vigilant for any persistent, unexplained lumps, sores, or abnormal growths on their child's palate or anywhere in the mouth. Any lesion that doesn't resolve within two weeks should be examined by a pediatric dentist or an oral pathologist.
- Treatment Approach: Treatment in children requires a highly specialized pediatric oncology team that understands the unique developmental considerations and potential long-term effects of surgery, radiation, and chemotherapy on a growing child. The focus is always on achieving a cure while minimizing developmental impact.
While pediatric oral cancer is a serious concern, its extreme rarity means that parents should focus more on general oral health, prevention of common issues, and seeking prompt dental care for any unusual or persistent oral abnormalities.
Cost Breakdown
Understanding the financial aspects of oral cancer treatment is vital for planning and seeking appropriate support. Beyond the overall ranges, here's a breakdown of how costs accumulate and options for managing them in the US.
Average US Costs (Low, Mid, High Estimates for an Entire Course of Treatment)
The total cost of treating oral cancer on the roof of the mouth can be highly variable.
- Low Estimate (Early Stage, Localized Surgery Only): $25,000 - $50,000
- This might include initial diagnostics, simple surgical resection, and short-term follow-up.
- Mid Estimate (Moderate Stage, Surgery + Radiation/Chemo): $75,000 - $150,000
- Includes more extensive surgery, a full course of radiation, possibly some chemotherapy, and initial rehabilitation.
- High Estimate (Advanced Stage, Complex Reconstruction, Multi-Modal Therapy, Recurrence): $150,000 - $300,000+
- Encompasses extensive surgery, complex reconstruction with microvascular free flaps, prolonged chemoradiation, targeted therapies, management of complications, and long-term rehabilitation.
With vs. Without Insurance
- With Insurance: Even with comprehensive insurance, you will likely be responsible for out-ofpocket costs including deductibles, co-pays, and co-insurance until you reach your annual out-of-pocket maximum. This can still amount to thousands to tens of thousands of dollars per year. However, insurance significantly mitigates the catastrophic financial impact.
- Without Insurance: Without insurance, the full cost of treatment falls on the patient, which can be financially devastating and lead to medical debt or delayed/foregone treatment. The costs outlined above for individual components would sum up to the total.
 Image description: A pie chart titled "Typical Oral Cancer Treatment Cost Breakdown" visually representing the proportional costs. Segments include: Surgery (40%), Radiation Therapy (30%), Chemotherapy/Targeted Therapy (15%), Diagnostics & Staging (10%), Rehabilitation & Follow-up Care (5%).
Image description: A pie chart titled "Typical Oral Cancer Treatment Cost Breakdown" visually representing the proportional costs. Segments include: Surgery (40%), Radiation Therapy (30%), Chemotherapy/Targeted Therapy (15%), Diagnostics & Staging (10%), Rehabilitation & Follow-up Care (5%).
Payment Plans and Financing Options
- Hospital Financial Assistance: Most hospitals have financial counselors who can help you understand your bills, negotiate payment plans, and identify assistance programs. Many offer discounted care or charity care for those who qualify based on income.
- Patient Assistance Programs: Pharmaceutical companies often have programs to help patients afford high-cost chemotherapy or targeted therapy drugs.
- Non-profit Organizations: Numerous organizations offer financial aid for cancer patients (e.g., CancerCare, The Leukemia & Lymphoma Society, specific oral cancer foundations).
- Medical Credit Cards: Options like CareCredit offer special financing for healthcare expenses, often with deferred interest periods.
- Clinical Trials: Participating in a clinical trial may cover the costs of experimental treatments, though standard care costs may still apply.
Cost-Saving Tips
- Verify Coverage: Always confirm what procedures and medications are covered by your insurance before treatment.
- Choose In-Network Providers: Stick to doctors and facilities that are in your insurance network to avoid higher out-of-network costs.
- Generic Medications: If available and appropriate, opt for generic versions of prescription drugs.
- Understand Your EOBs: Carefully review your Explanation of Benefits (EOBs) from your insurance company to ensure accuracy and catch any billing errors.
- Negotiate Prices: If you are uninsured or facing high out-of-pocket costs, you can sometimes negotiate prices with hospitals or providers for specific services.
Frequently Asked Questions
How long does oral cancer take to develop?
Oral cancer can develop over a period of months to several years. Precancerous lesions like leukoplakia or erythroplakia can exist for a long time before transforming into invasive cancer. The speed of progression varies greatly depending on the individual, risk factors, and cancer type.
Is oral cancer on the roof of the mouth painful?
In its early stages, oral cancer on the roof of the mouth is often painless. This is one reason why early detection can be challenging. As the cancer grows and invades deeper tissues or nerves, it can cause persistent pain, discomfort, or a burning sensation. Any persistent oral pain warrants investigation.
Can oral cancer be cured?
Yes, oral cancer is highly curable, especially when detected and treated in its early stages. The 5-year survival rate for localized oral cancer is around 85%. However, this rate decreases significantly if the cancer has spread to regional lymph nodes or distant sites.
What is the survival rate for oral cancer of the palate?
The 5-year survival rate for oral cavity cancers (including the palate) in the US is about 68%. For localized disease, it's approximately 85%; for regional spread, it drops to 69%; and for distant metastasis, it's about 39%. Early diagnosis is the most critical factor for improving these rates.
What are the early signs of oral cancer I can look for?
Look for any persistent white or red patches (leukoplakia or erythroplakia), a sore that doesn't heal within two weeks, a lump or thickening, or unexplained numbness or pain on the roof of your mouth or anywhere in your oral cavity. These signs should prompt an immediate dental visit.
Can dentures cause oral cancer?
Ill-fitting or poorly maintained dentures do not directly cause oral cancer. However, chronic irritation from a denture that constantly rubs against oral tissues can create an area of chronic inflammation, which might make the tissue more susceptible to malignant changes over a very long time, especially in individuals with other risk factors like tobacco use. Proper denture fit and hygiene are essential.
What is the difference between leukoplakia and oral cancer?
Leukoplakia is a white patch on the mucous membrane that cannot be scraped off and is not identifiable as any other disease. It is considered a potentially malignant disorder, meaning it can develop into cancer. Oral cancer is already an invasive malignancy where cells have become cancerous and are invading surrounding tissues. A biopsy is necessary to differentiate between them.
How often should I get screened for oral cancer?
The American Dental Association (ADA) recommends that all adults receive an oral cancer screening at least once a year as part of their routine dental check-up. Individuals with higher risk factors (e.g., tobacco/alcohol users) may benefit from more frequent screenings, such as every six months.
Are there alternative treatments for oral cancer?
While some complementary therapies (e.g., acupuncture for dry mouth, nutritional support) can help manage symptoms and improve quality of life during conventional treatment, there are no scientifically proven "alternative treatments" that can cure oral cancer independently. Relying solely on unproven alternative therapies can be dangerous and delay effective conventional treatment.
How long is recovery after oral cancer treatment?
Recovery varies significantly based on the stage of cancer and the extent of treatment. For minor surgery, recovery might be a few weeks. For extensive surgery with reconstruction and radiation/chemotherapy, recovery can take many months to over a year, involving ongoing rehabilitation for speech, swallowing, and dental function. Long-term follow-up is lifelong.
When to See a Dentist
Given the importance of early detection for oral cancer on the roof of the mouth, knowing when to seek professional dental attention is paramount. Do not delay if you observe any of the following:
- Persistent Oral Lesions: Any white patch (leukoplakia), red patch (erythroplakia), or a combined red and white patch on the roof of your mouth or elsewhere in your mouth that persists for more than two weeks without showing any signs of healing or resolution.
- Non-Healing Sores or Ulcers: A sore or ulcer on your palate, tongue, lips, or gums that does not heal within a two-week period. This is a critical warning sign, especially if it's painless.
- Unexplained Lumps or Swellings: The appearance of a new lump, thickening, or persistent swelling in your mouth, neck, or jaw. Palpate the roof of your mouth gently; if you feel something new or unusual, get it checked.
- Chronic Pain or Numbness: Persistent pain, tenderness, or numbness in any area of your mouth, face, or neck that cannot be attributed to a clear cause like a recent injury.
- Difficulty with Oral Functions: Any new or worsening difficulty in chewing, swallowing, speaking, or moving your tongue or jaw without an obvious explanation.
- Unexplained Bleeding: Frequent or persistent bleeding from your mouth that is not associated with an injury or brushing too hard.
- Changes in Denture Fit: If your dentures suddenly feel ill-fitting, loose, or uncomfortable, or if they start causing new sore spots that don't heal, it could indicate underlying changes in your oral tissues or bone structure.
Red Flags vs. Routine Care Guidance
- Red Flags (Immediate Action): Any of the persistent symptoms listed above, especially if accompanied by rapid growth, increasing pain, or constitutional symptoms like unexplained weight loss, warrant an urgent appointment with your dentist or an oral surgeon. Do not wait for your next routine check-up.
- Routine Care Guidance: Regular dental check-ups, ideally every six months, are crucial for comprehensive oral cancer screenings. Even if you have no symptoms, your dentist is trained to identify subtle changes you might miss. Adhere to the American Dental Association's guidelines for preventive care.
 Image description: A decision-tree flowchart titled "When to See Your Dentist for Oral Concerns." It starts with "Notice an Oral Concern?" and branches to "Does it last > 2 weeks?" (If No -> "Monitor or Routine Check-up"). If Yes -> "Is it painful/growing/bleeding/affecting function?" (If Yes -> "See Dentist Urgently"). If No -> "See Dentist for Evaluation (Non-Emergency)"). This leads to a final box "Professional Diagnosis & Treatment Plan."
Image description: A decision-tree flowchart titled "When to See Your Dentist for Oral Concerns." It starts with "Notice an Oral Concern?" and branches to "Does it last > 2 weeks?" (If No -> "Monitor or Routine Check-up"). If Yes -> "Is it painful/growing/bleeding/affecting function?" (If Yes -> "See Dentist Urgently"). If No -> "See Dentist for Evaluation (Non-Emergency)"). This leads to a final box "Professional Diagnosis & Treatment Plan."
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Floor of Mouth Cancer: Complete Guide
Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral c
February 23, 2026
Oral Cancer Stages Pictures: Complete Guide
Oral cancer, a serious and potentially life-threatening disease, affects thousands of Americans each year. According to the American Cancer Society, approximately 54,000 new cases of oral cavity or oropharyngeal cancer are diagnosed annually in the United States. While these numbers can be daunt
February 23, 2026
Can You Die From Mouth Cancer
Oral cancer is a formidable disease, often striking with insidious subtlety before revealing its devastating potential. It's a question that weighs heavily on the minds of those who receive a diagnosis or even those simply concerned about unusual oral symptoms: can you die from mouth cancer? The
February 23, 2026

Mouth Cancer Photos: Complete Guide
Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,23
February 23, 2026