What Is Leukoplakia

Key Takeaways
- Imagine discovering a persistent white patch in your mouth that simply won't go away, no matter how much you brush or rinse. For many, this could be the first, often silent, sign of leukoplakia, a condition that, while usually painless, carries a significant and serious implication: it is consid
What Is Leukoplakia
Imagine discovering a persistent white patch in your mouth that simply won't go away, no matter how much you brush or rinse. For many, this could be the first, often silent, sign of leukoplakia, a condition that, while usually painless, carries a significant and serious implication: it is considered a potentially malignant disorder. With oral cancer affecting an estimated 54,000 Americans annually, understanding conditions like leukoplakia is not just important—it's critical for early detection and potentially life-saving intervention. This comprehensive guide from SmilePedia.net will delve deep into what is leukoplakia, explaining its various forms, underlying causes, and crucial symptoms. We'll explore the diagnostic process, available treatment options, associated costs, and most importantly, how to prevent this condition and what steps to take if you suspect you might have it. By arming yourself with this knowledge, you empower yourself to take proactive control of your oral health and recognize the subtle indicators that could signal an early stage cheek mouth cancer or other serious issues.
Key Takeaways:
- Definition: Leukoplakia is a persistent white or grayish patch in the mouth that cannot be rubbed off and is a "diagnosis of exclusion."
- Malignant Potential: Approximately 5-17% of leukoplakia cases can transform into oral cancer, making early detection and monitoring crucial.
- Primary Cause: Tobacco use (smoking, chewing) and heavy alcohol consumption are the leading risk factors.
- Diagnosis: A definitive diagnosis requires a biopsy to rule out other conditions and assess for dysplasia (precancerous changes).
- Treatment Costs: Biopsy costs range from $200-$800. Surgical excision can range from $500 to over $5,000, depending on size, location, and method (scalpel, laser).
- Monitoring: Even after treatment, lifelong follow-up appointments, often every 3-6 months initially, are essential due to high recurrence rates and the ongoing risk of malignant transformation.
- Prevention: Quitting tobacco and reducing alcohol intake are the most effective preventive measures, significantly reducing risk.
What It Is / Overview
Leukoplakia is medically defined as a predominantly white patch or plaque of the oral mucosa that cannot be characterized clinically or pathologically as any other definable lesion. In simpler terms, it's a persistent white spot or area inside your mouth that a dentist or doctor can't explain as something else, like a fungal infection (thrush), a burn, or a lichen planus lesion. It typically appears as a thick, white-to-grayish patch with an irregular or smooth surface. Unlike many other oral lesions, leukoplakia cannot be easily scraped off the surface.

The most significant aspect of leukoplakia is its status as a "potentially malignant disorder." This means that while it is not cancer itself, it has the potential to transform into oral squamous cell carcinoma, the most common type of oral cancer. The rate of malignant transformation varies depending on the type and specific characteristics of the lesion, but it underscores why vigilant monitoring and appropriate management are so vital. The World Health Organization (WHO) has recognized this potential, classifying leukoplakia as one of the most common premalignant oral lesions.
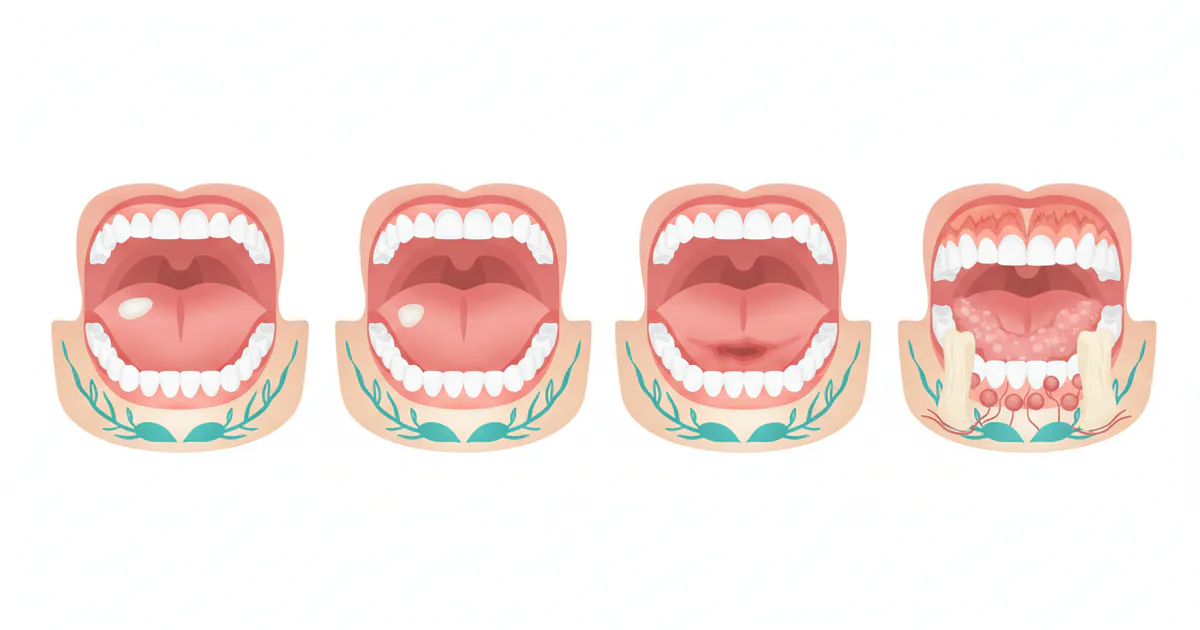
Leukoplakia can occur anywhere in the mouth, but common sites include the tongue, the floor of the mouth, the inside of the cheeks (buccal mucosa), and the gums. While often asymptomatic and discovered incidentally during a routine dental check-up, its presence necessitates immediate professional evaluation due to its potential to progress to malignancy. The prevalence of oral leukoplakia in the general adult population ranges from 0.5% to 10%, with higher rates observed in older individuals and those with specific risk factors.
Types / Variations
Leukoplakia isn't a single entity; it presents in various forms, each with different characteristics and varying degrees of malignant potential. Understanding these types is crucial for both diagnosis and prognosis.
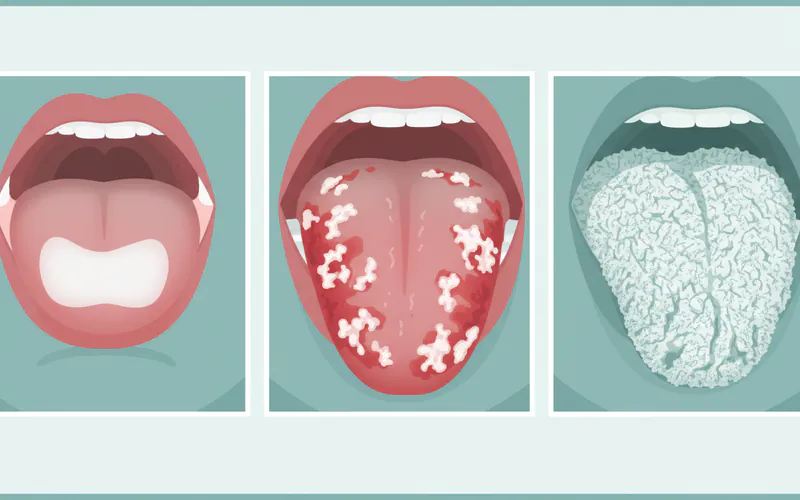
Homogeneous Leukoplakia
This is the most common and generally considered the least aggressive form. It appears as a uniformly flat, thin, white plaque with a smooth or finely wrinkled surface. The entire lesion is consistent in color and texture.
- Appearance: Evenly white, flat, or slightly raised.
- Malignant Potential: Relatively low, approximately 5% to 10% over a 10-year period.
- Common Locations: Buccal mucosa (inner cheek), tongue.
Non-Homogeneous Leukoplakia
This category encompasses lesions that are not uniform in appearance, signaling a higher risk of malignant transformation. They are often described based on their specific visual characteristics:
-
Speckled (or Erythroleukoplakia): This is a mixed red and white lesion. The red areas are often atrophic (thinned) and indicate a higher degree of inflammation and cellular changes.
- Appearance: Irregular white patches interspersed with red, often ulcerated or eroded areas.
- Malignant Potential: This is considered one of the highest-risk forms, with transformation rates reported as high as 30% to 50%.
- Common Locations: Floor of the mouth, lateral border of the tongue.
-
Nodular: Characterized by small, round, white nodules or bumps on a red or white background.
- Appearance: Nodular or pebble-like surface, can be white or mixed red and white.
- Malignant Potential: High, similar to speckled leukoplakia.
-
Verrucous: Features a wart-like, corrugated, or fissured surface, often very thick.
- Appearance: Exophytic, rough, wart-like growth with a white surface.
- Malignant Potential: High.
Proliferative Verrucous Leukoplakia (PVL)
PVL is a rare but highly aggressive form of non-homogeneous leukoplakia. It's characterized by its multifocal nature (appearing in multiple sites in the mouth), its tendency to recur after treatment, and its very high rate of malignant transformation, often into verrucous carcinoma or squamous cell carcinoma. PVL typically begins as a simple homogeneous lesion but progresses over time to become multifocal, exophytic, and increasingly verrucous.
- Appearance: Multiple, widespread, thick, wart-like lesions throughout the oral cavity.
- Malignant Potential: Extremely high, often exceeding 70-100% over the patient's lifetime.
- Characteristics: High recurrence rate, often resistant to treatment.
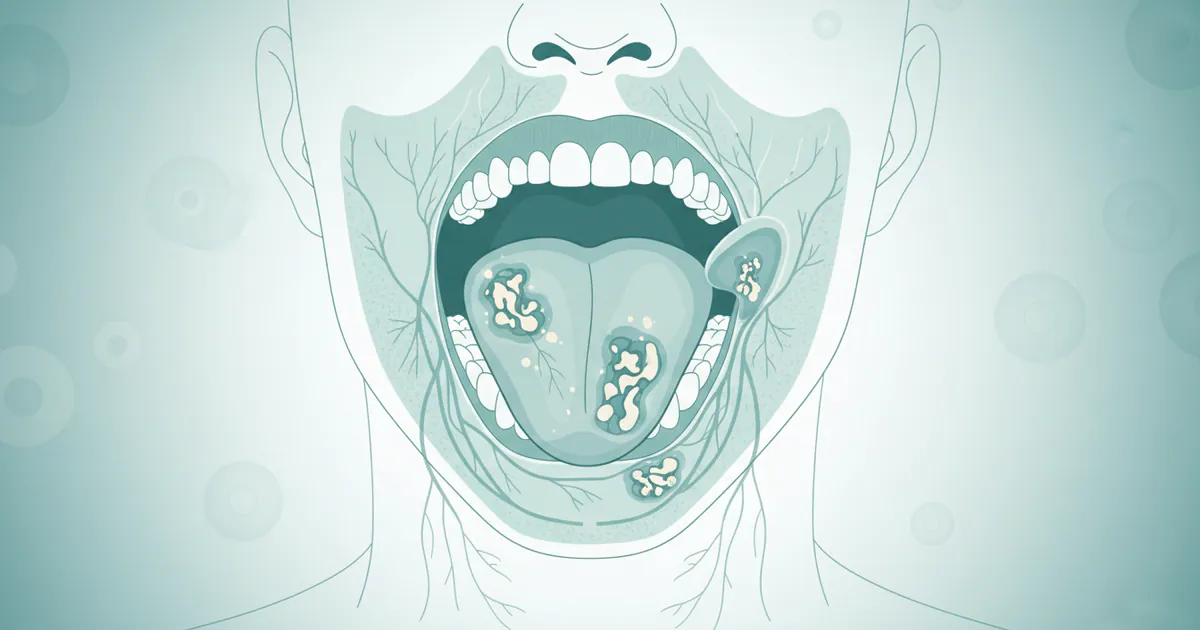
Oral Hairy Leukoplakia (OHL)
Unlike other forms of leukoplakia, OHL is specifically associated with the Epstein-Barr virus (EBV) and is almost exclusively seen in immunocompromised individuals, most commonly those with HIV/AIDS, or organ transplant recipients on immunosuppressive medications. It is not considered a precancerous lesion.
- Appearance: White, shaggy, or "hairy" corrugated patches, typically on the lateral borders of the tongue. It cannot be scraped off.
- Malignant Potential: None. It is benign.
- Distinguishing Feature: Presence of EBV.
Causes / Why It Happens
The exact etiology of leukoplakia isn't always clear, especially in cases with no obvious risk factors (idiopathic leukoplakia). However, strong associations have been identified with several key contributing factors:
Primary Risk Factors
-
Tobacco Use: This is by far the most significant risk factor. Whether smoked (cigarettes, cigars, pipes) or smokeless (chewing tobacco, snuff), tobacco introduces numerous carcinogens and irritants to the oral mucosa. The heat, chemicals, and mechanical irritation contribute to cellular changes that can lead to leukoplakia. The risk is dose-dependent, meaning the more you use, and the longer you use it, the higher the risk.
-
Alcohol Consumption: Heavy and chronic alcohol consumption is another major contributor. Alcohol acts as an irritant and a solvent, potentially enhancing the penetration of carcinogens from tobacco into the oral tissues. The synergistic effect of combining tobacco and alcohol is particularly potent, significantly multiplying the risk of leukoplakia and oral cancer.
Secondary and Contributing Factors
-
Chronic Irritation:
- Rough Teeth or Fillings: A persistently rough tooth surface or a jagged edge of a restoration can cause mechanical irritation to the adjacent soft tissues, leading to a localized white patch. While often benign, these lesions should still be monitored.
- Ill-Fitting Dentures: Dentures that rub or chafe against the oral mucosa can also cause chronic irritation.
- Trauma: Repetitive biting of the cheek or tongue can sometimes lead to localized leukoplakia-like lesions.
-
Human Papillomavirus (HPV) Infection: Certain high-risk strains of HPV, particularly HPV-16 and HPV-18, are increasingly linked to a subset of oral leukoplakia cases, especially those affecting the oropharynx and posterior tongue. HPV DNA has been detected in a significant percentage of oral leukoplakia lesions, suggesting its role in malignant transformation for some patients.
-
Ultraviolet (UV) Radiation: Exposure to sunlight is a known risk factor for lip cancer, and it can also cause actinic cheilitis (a precancerous condition of the lips) which presents as white patches on the vermilion border of the lip, essentially a form of leukoplakia.
-
Immunosuppression: As mentioned with Oral Hairy Leukoplakia (OHL), a compromised immune system (due to HIV, organ transplantation, etc.) can allow opportunistic viral infections like Epstein-Barr Virus (EBV) to manifest as white lesions. While OHL itself is benign, a weakened immune system can generally increase susceptibility to other oral issues.
-
Nutritional Deficiencies: While less common, severe deficiencies in certain vitamins, such as Vitamin A or B complex vitamins, have been theorized to play a role in altering epithelial health and potentially contributing to leukoplakia.
-
Genetic Predisposition: Some individuals may have a genetic susceptibility that makes them more prone to developing leukoplakia or more likely for their lesions to undergo malignant transformation, even in the absence of strong environmental risk factors.
It's important to remember that for a significant percentage of cases, especially homogeneous leukoplakia, the exact cause remains idiopathic (unknown). This underscores the need for regular dental check-ups, as even seemingly benign or unexplained white patches warrant investigation.
Signs and Symptoms
Leukoplakia is often insidious, meaning it develops slowly and often without noticeable symptoms in its early stages. This is why regular dental examinations are so crucial for early detection. However, when signs do appear, they are usually visual.
What to Look For:
- Appearance of a White or Grayish Patch: This is the hallmark symptom. The patch can be anywhere in the mouth—on the tongue, under the tongue, on the inside of the cheeks (buccal mucosa), on the gums, or on the floor of the mouth. The color can range from a milky white to a bright, chalky white.
- Non-Scrapable Nature: A key diagnostic feature is that the patch cannot be rubbed, scraped, or wiped away. This differentiates it from conditions like oral thrush (candidiasis), which typically can be scraped off, revealing inflamed tissue underneath.
- Texture Changes: The patch may feel rough, thickened, or hardened when touched with the tongue or finger. It might also have a wrinkled, fissured, or corrugated surface.
- Asymptomatic or Mild Discomfort: In most cases, leukoplakia is painless. However, some individuals might experience a mild burning sensation, especially if the lesion is non-homogeneous or inflamed. If the lesion becomes ulcerated or eroded, it can cause pain or discomfort, particularly when eating or drinking.
- Stiffness or Reduced Flexibility: If the lesion is extensive or thickened, it might lead to a feeling of stiffness in the affected area, potentially impacting speech or the ability to move the tongue or cheek normally.
Differentiating from Early Stage Cheek Mouth Cancer:
It's vital to understand that leukoplakia itself is not cancer, but it can be a precursor. However, some characteristics of leukoplakia, especially non-homogeneous types, can mimic early stage cheek mouth cancer or other mouth cancer symptoms pictures you might encounter. Therefore, it's crucial to report any of the following changes to your dentist immediately:
- Mixed Red and White Appearance (Erythroleukoplakia): Any red areas within or around the white patch are a significant warning sign and carry a much higher risk of malignancy.
- Presence of Ulcers or Sores: Non-healing sores or ulcers within or adjacent to the white patch, especially if they persist for more than two weeks, are highly suspicious.
- Hardness or Induration: A noticeably firm or hard feel to the patch or surrounding tissue, particularly at its base, can indicate deeper cellular changes.
- Rapid Growth or Change in Size/Shape: Any noticeable increase in the size of the patch or a change in its borders warrants immediate attention.
- Lumps or Bumps: The development of a raised lump or nodule within the white patch should be investigated promptly.
- Difficulty Swallowing or Speaking: If the lesion interferes with normal oral functions, it could indicate progression or a more advanced stage.
- Numbness or Tingling: Altered sensation in the area can be a sign of nerve involvement.
Pro Tip: Take a clear photo of any suspicious patch when you first notice it. This can help your dentist track any changes over time. Regularly inspect your mouth with a good light and mirror, especially if you have risk factors.
Treatment Options
The primary goal of treating leukoplakia is to prevent its progression to oral cancer. Treatment strategies depend heavily on the type of leukoplakia, the presence and degree of dysplasia (abnormal cell changes) identified on biopsy, the lesion's size and location, and the patient's overall health and risk factors.
1. Diagnosis and Risk Assessment
Before any definitive treatment, a thorough diagnostic process is essential.
- Clinical Examination: Your dentist will carefully examine your mouth, checking the size, location, color, and texture of the lesion. They will also feel the lesion to check for firmness or induration.
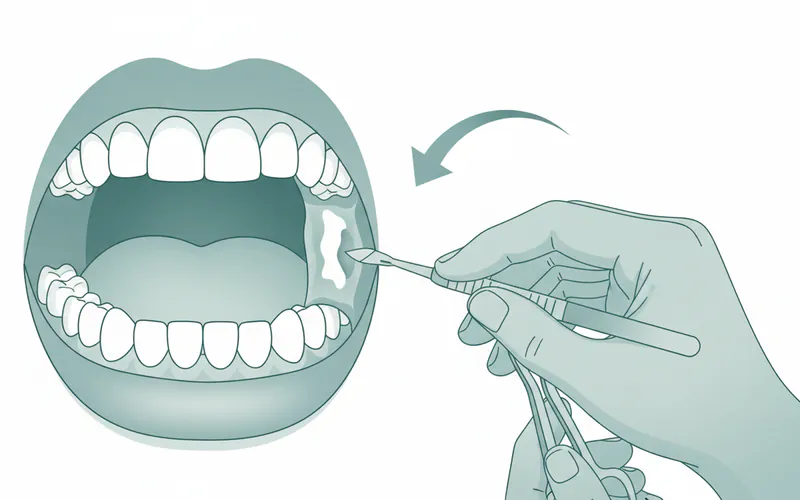
- Biopsy: This is the most crucial step for definitive diagnosis and risk assessment. A small tissue sample is taken from the suspicious area and sent to a pathologist for microscopic examination. The pathologist will determine if dysplasia is present and, if so, its grade (mild, moderate, severe), or if squamous cell carcinoma has already developed.
- Incisional Biopsy: A small wedge of tissue is removed from the most suspicious part of the lesion.
- Excisional Biopsy: The entire lesion is removed, typically for smaller lesions or those with clearly defined borders.
- Brush Cytology: While less invasive, a brush biopsy is less definitive than a scalpel biopsy as it only collects superficial cells. It can be used as a screening tool but a negative result does not definitively rule out dysplasia, and a positive or atypical result always requires a traditional biopsy.
2. Lifestyle Modifications
For all patients with leukoplakia, regardless of the biopsy results, the immediate recommendation is to eliminate or reduce known risk factors.
- Tobacco Cessation: Quitting all forms of tobacco (smoking, chewing) is paramount. This can lead to the regression of some lesions, especially homogeneous ones, and significantly reduces the risk of malignant transformation.
- Alcohol Reduction: Limiting or eliminating alcohol consumption, particularly heavy drinking, is also strongly advised due to its synergistic effect with tobacco.
- Address Chronic Irritation: If a sharp tooth, ill-fitting denture, or restorative material is causing irritation, it should be corrected promptly by your dentist.
3. Surgical Excision
This is the most common and effective treatment for dysplastic leukoplakia or lesions deemed high-risk. The goal is to completely remove the abnormal tissue.
- Scalpel Excision: Traditional surgical removal with a scalpel. This allows for clear margins and complete removal of the lesion, which is then sent for histopathological examination to ensure all abnormal cells are removed.
- Pros: High success rate for complete removal, excellent for histopathological assessment of margins.
- Cons: Requires local or general anesthesia, potential for scarring, discomfort, and temporary functional impairment.
- Laser Ablation/Excision: Using a CO2 laser to vaporize or precisely cut out the lesion. Lasers offer precision and can minimize bleeding.
- Pros: Less bleeding, often less postoperative pain, precise removal, can be done under local anesthesia.
- Cons: Higher cost, specialized equipment, precise histopathological margin assessment can be more challenging if vaporization is used.
- Cryotherapy: Freezing the lesion with liquid nitrogen. This destroys the abnormal cells by freezing and thawing.
- Pros: Minimally invasive, relatively quick.
- Cons: Can be difficult to control depth of penetration, less precise margin control, tissue not available for histopathological examination, higher recurrence rate than surgical excision.
- Electrocautery: Using heat to destroy the lesion. Similar pros and cons to cryotherapy.
4. Pharmacological and Adjunctive Therapies
These therapies are generally considered adjunctive (used in conjunction with other treatments) or for specific cases where surgery is not feasible or appropriate, or for lesions with mild dysplasia. Their efficacy is often limited compared to surgical excision.
- Retinoids (Vitamin A derivatives): Topical or systemic retinoids (e.g., isotretinoin, beta-carotene) have been explored to induce regression of leukoplakia. However, results are often temporary, and side effects (e.g., dry skin, liver toxicity with systemic use) can be significant.
- Pros: Non-invasive.
- Cons: Often temporary effect, potential for side effects, not a primary treatment for moderate-to-severe dysplasia.
- Anti-inflammatory Agents: Some studies have looked at the use of non-steroidal anti-inflammatory drugs (NSAIDs) or COX-2 inhibitors, given their role in carcinogenesis, but these are not standard treatments.
- Photodynamic Therapy (PDT): Involves administering a photosensitizing agent (e.g., aminolevulinic acid) which is absorbed by abnormal cells, followed by exposure to a specific wavelength of light. The light activates the drug, leading to the destruction of the target cells.
- Pros: Minimally invasive, precise targeting.
- Cons: Can be costly, requires specialized equipment, photosensitivity of the patient.
5. Surveillance (Watchful Waiting)
For small, homogeneous lesions with no or mild dysplasia, particularly in patients who have ceased tobacco and alcohol use, a "watchful waiting" approach with regular follow-up examinations (e.g., every 3-6 months) may be recommended. This involves careful monitoring for any changes in size, color, or texture. If the lesion progresses or shows signs of dysplasia, intervention becomes necessary.
Pro Tip: Always discuss all treatment options, including their risks and benefits, with your oral surgeon or oral medicine specialist. The best approach is highly individualized.
Step-by-Step Process: What to Expect During Treatment
Let's outline a typical process, focusing on the most common and definitive treatment: surgical excision following a biopsy.
Step 1: Initial Consultation and Examination
- Your Role: Report any persistent white patches or oral changes to your general dentist or hygienist.
- Dentist's Role: Your dentist will conduct a thorough oral examination, history taking (including tobacco and alcohol use), and possibly perform vital staining (e.g., with toluidine blue) to highlight suspicious areas. They will then refer you to an oral surgeon, oral medicine specialist, or periodontist experienced in managing oral lesions.
Step 2: Biopsy Procedure (Diagnostic Phase)
- Preparation: The specialist will explain the procedure, potential risks, and post-biopsy care. You might need to avoid certain medications (like blood thinners) beforehand.
- Anesthesia: Local anesthesia will be administered to numb the area. You will be awake but will not feel pain, though you might feel pressure.
- Tissue Sample Collection:
- Incisional Biopsy: A small piece of tissue, often wedge-shaped, will be carefully removed from the most suspicious part of the lesion, extending into healthy tissue for clear margins.
- Excisional Biopsy: For smaller, well-defined lesions, the entire lesion may be removed at this stage.
- Closure: The area may be closed with a few sutures, which might be dissolvable or require removal in 7-10 days.
- Post-Biopsy Care: You'll receive instructions on pain management (over-the-counter pain relievers), diet (soft foods), oral hygiene (gentle rinsing, avoiding the surgical site), and what to do if you experience excessive bleeding or swelling.
- Lab Analysis: The tissue sample is sent to an oral pathologist for microscopic examination to determine the presence and grade of dysplasia, or if cancer is present. This typically takes 7-14 days.
Step 3: Discussion of Biopsy Results and Treatment Planning
- Results Review: You will have a follow-up appointment with the specialist to discuss the biopsy results.
- Treatment Recommendations: Based on the pathology report (e.g., mild, moderate, severe dysplasia, or carcinoma), the specialist will recommend the most appropriate definitive treatment plan. If the excisional biopsy already removed the entire lesion with clear margins and no cancer, regular monitoring might be the primary recommendation.
Step 4: Definitive Treatment (Surgical Excision Example)
This step applies if further intervention is needed after biopsy.
- Preparation: Similar to the biopsy, you'll be prepped and given anesthesia (local, sedation, or general depending on complexity).
- Surgical Removal: The specialist will use a scalpel, laser, or other chosen method to remove the lesion entirely, ensuring a margin of healthy tissue is also removed to minimize recurrence. The excised tissue will again be sent for pathology to confirm complete removal and assess margins.
- Closure: The surgical site will be closed with sutures. For larger defects, a graft may be necessary, though this is rare for typical leukoplakia.
- Post-Operative Care: Detailed instructions will be provided, similar to biopsy aftercare but often more extensive:
- Pain Management: Prescription pain relievers or strong over-the-counter options.
- Diet: Soft, non-irritating foods for several days to weeks. Avoid hot, spicy, or acidic foods.
- Oral Hygiene: Gentle rinsing with prescribed antiseptic mouthwash (e.g., chlorhexidine) or warm salt water. Avoid vigorous brushing of the surgical site.
- Activity Restrictions: Avoid strenuous activity for a few days to a week.
- Follow-Up: Scheduled appointments to remove sutures (if non-dissolvable) and monitor healing.

Step 5: Long-Term Follow-Up and Surveillance
- Crucial Monitoring: Even after successful treatment, lifelong follow-up is essential. Leukoplakia has a significant recurrence rate (up to 30-50%) and the potential for new lesions to develop elsewhere in the mouth (field cancerization).
- Schedule: Initially, follow-up visits might be every 3-6 months, gradually extending to annually if stable. These appointments involve a thorough oral examination to detect any new or recurring lesions or signs of malignant transformation.
- Patient Vigilance: You will be educated on how to perform self-oral examinations and what signs to look for between appointments.
This step-by-step process emphasizes the continuous care required, from initial detection through long-term surveillance, to effectively manage leukoplakia and prevent the development of oral cancer.
Cost and Insurance
Understanding the financial aspect of leukoplakia diagnosis and treatment is crucial. Costs can vary significantly based on the region, the type of facility (dental office vs. hospital), the specialist's fees, and the specific procedures performed.
Diagnostic Costs
- Initial Consultation: A consultation with an oral surgeon or oral medicine specialist can range from $150 to $400.
- Biopsy:
- Incisional Biopsy: Typically ranges from $200 to $800. This includes the procedure itself, local anesthesia, and suture placement.
- Excisional Biopsy (simple): Can range from $400 to $1,500 if the entire lesion is removed in a simple office setting.
- Pathology Fee: The cost for the laboratory analysis of the tissue sample is usually separate and can range from $100 to $300.
Treatment Costs (Beyond Biopsy)
If definitive treatment beyond the initial biopsy is required, costs escalate:
- Surgical Excision (Scalpel): For moderate to large lesions requiring more complex removal, costs can range from $500 to $2,500. This generally covers the surgeon's fee, local anesthesia, and facility use.
- Laser Ablation/Excision: Laser treatments are often more expensive due to specialized equipment. Expect costs to range from $1,000 to $5,000 or more, depending on the size and number of lesions, and whether it's performed in an office or outpatient surgical center.
- Photodynamic Therapy: This is a less common treatment for leukoplakia and can be quite expensive, potentially ranging from $1,500 to $6,000 per session, often requiring multiple sessions.
- Follow-up Appointments: Regular surveillance visits post-treatment typically cost $50 to $250 per visit, depending on the scope of examination and any additional procedures (e.g., repeated brush cytology if used for monitoring).
Total Estimated Costs (without insurance):
- Mild/Single Lesion (Diagnosis + Simple Excision): $700 - $3,000
- Complex/Multiple Lesions (Diagnosis + Laser Excision/Advanced Surgery): $2,000 - $8,000+
Insurance Coverage
This is where it gets complex, as leukoplakia bridges dental and medical concerns.
- Dental Insurance: Typically, dental insurance covers routine check-ups and basic procedures. While some plans might cover a portion of diagnostic biopsies (especially if performed by an oral surgeon who accepts dental benefits for such procedures), they are less likely to cover extensive surgical treatments, especially if performed in a hospital setting. Diagnostic codes (CDT codes) are used for dental claims.
- Medical Insurance: Since leukoplakia is a potentially precancerous condition, medical insurance is often the primary payer for diagnosis and treatment. This includes consultations with specialists, biopsies, pathology fees, and surgical excisions.
- CPT Codes: Medical claims use Current Procedural Terminology (CPT) codes for procedures. For example, a biopsy might be coded as 41825, and an excision of a lesion could be 41116.
- Prior Authorization: Many medical insurance plans will require prior authorization for surgical procedures, especially for higher-cost treatments like laser surgery.
- Deductibles and Co-pays: You will be responsible for your plan's deductible before coverage kicks in, and then typically a co-pay or co-insurance percentage (e.g., 10-30% of the allowed amount) for covered services.
- Out-of-Pocket Maximum: Most medical plans have an annual out-of-pocket maximum, which limits how much you'll have to pay in a given year.
Pro Tip: Always verify your coverage with both your dental and medical insurance providers before any procedures are performed. Ask for a breakdown of estimated costs, CPT codes the provider plans to use, and what portion will be covered. Don't hesitate to ask the provider's office to assist with insurance verification and pre-authorization.
Payment Plans and Financing Options
If you face significant out-of-pocket costs, several options may be available:
- Payment Plans: Many oral surgery or dental offices offer in-house payment plans, allowing you to pay in installments.
- Healthcare Credit Cards: Services like CareCredit offer special financing options for healthcare expenses, often with deferred interest periods if paid in full within a certain timeframe.
- Health Savings Accounts (HSAs) / Flexible Spending Accounts (FSAs): If you have an HSA or FSA through your employer, you can use these tax-advantaged accounts to pay for qualified medical expenses, including leukoplakia treatment.
- Negotiation: In some cases, if you are paying entirely out-of-pocket, you may be able to negotiate a slightly reduced fee with the provider.
Recovery and Aftercare
Proper recovery and diligent aftercare are essential to ensure optimal healing, minimize complications, and facilitate successful long-term management of leukoplakia.
Immediate Post-Operative Period (First 24-72 Hours)
- Pain Management: Expect some discomfort as the local anesthesia wears off. Your specialist will recommend or prescribe pain medication. Over-the-counter options like ibuprofen or acetaminophen are often sufficient for mild pain. For more significant pain, prescription medication may be given.
- Bleeding: Minor oozing or spotting from the surgical site is normal. You may be advised to bite gently on a gauze pad for 30-60 minutes to control bleeding. Avoid spitting or rinsing vigorously, as this can dislodge the blood clot and prolong bleeding.
- Swelling: Some swelling is common. Applying a cold compress or ice pack to the outside of the face near the surgical area for 15-20 minutes at a time, with 20-minute breaks, can help reduce swelling in the first 24-48 hours.
- Diet: Stick to soft, bland, and cool foods for the first few days. Avoid hot, spicy, acidic, or crunchy foods that could irritate the wound or dislodge sutures. Examples include yogurt, applesauce, mashed potatoes, and soups.
- Oral Hygiene:
- Gentle Rinsing: Start rinsing gently with warm salt water (1/2 teaspoon salt in 8 ounces of warm water) or a prescribed antiseptic mouthwash (like chlorhexidine) 2-3 times a day, starting the day after surgery.
- Brushing: Brush your teeth gently, avoiding the surgical site. Do not use an electric toothbrush directly over the wound.
- Avoid: Do not use straws (suction can dislodge blood clots), smoke (severely impairs healing and increases risk of recurrence/new lesions), or consume alcohol.
Week 1-2 Post-Operative Period
- Suture Removal: If non-dissolvable sutures were used, they will typically be removed by your specialist at a follow-up appointment within 7-10 days.
- Healing: The surgical site will gradually heal. You might notice a white or yellowish film over the area, which is normal healing tissue (fibrin) and not pus.
- Diet Progression: Gradually introduce more solid foods as comfort allows.
- Oral Hygiene: Continue gentle oral hygiene. The goal is to keep the area clean without causing trauma.
Long-Term Aftercare and Surveillance
- Regular Follow-ups: This is perhaps the most critical aspect of long-term care. You will need routine follow-up examinations (e.g., every 3-6 months initially, then annually) with your oral medicine specialist or oral surgeon. These visits are vital to monitor for recurrence of leukoplakia or the development of new lesions, which can still occur even after successful treatment.
- Self-Examination: Your dentist will likely teach you how to perform monthly self-oral examinations to check for any new or changing white patches, red spots, or non-healing sores.
- Strict Risk Factor Avoidance: This cannot be stressed enough. Lifelong avoidance of tobacco and excessive alcohol is crucial to minimize the risk of recurrence and new lesions.
- Healthy Lifestyle: A balanced diet rich in fruits and vegetables, maintaining good general health, and regular dental check-ups (even with your general dentist) contribute to overall oral health and early detection of any new issues.
Potential Complications to Watch For
While rare, contact your specialist immediately if you experience:
- Excessive bleeding that doesn't stop with pressure.
- Increasing pain that isn't managed by prescribed medication.
- Signs of infection: fever, pus, severe swelling, spreading redness.
- Numbness or altered sensation that persists longer than expected.
- Difficulty swallowing, speaking, or opening your mouth that worsens.
Pro Tip: Keep a detailed record of your follow-up appointments and any instructions or observations from your specialist. This can be invaluable for continuous, informed care.
Prevention
Preventing leukoplakia, especially the types with malignant potential, largely revolves around eliminating or mitigating the identified risk factors. Proactive steps are your best defense against this potentially serious condition.
1. Eliminate Tobacco Use (Crucial!)
- Quit Smoking: Cigarettes, cigars, and pipes introduce thousands of toxic chemicals and carcinogens directly to the oral mucosa. Quitting smoking is the single most effective step you can take to prevent leukoplakia and oral cancer.
- Avoid Smokeless Tobacco: Chewing tobacco and snuff are particularly potent causes of leukoplakia and oral cancer, as they deliver high concentrations of carcinogens directly to the tissues for prolonged periods.
- Seek Support: Quitting tobacco can be challenging. Utilize resources like nicotine replacement therapies (patches, gum), prescription medications, counseling, and support groups. Your dentist or physician can offer guidance and referrals.
2. Limit Alcohol Consumption
- Moderation is Key: If you consume alcohol, do so in moderation. For women, this typically means no more than one drink per day, and for men, no more than two drinks per day.
- Avoid Binge Drinking: Excessive alcohol intake significantly increases risk.
- Synergistic Effect: Remember the potent combined risk of alcohol and tobacco. If you use tobacco, eliminating alcohol becomes even more critical.
3. Maintain Good Oral Hygiene and Regular Dental Check-ups
- Routine Examinations: Visit your dentist at least once a year, and ideally twice a year, for comprehensive oral examinations. Dentists are trained to spot subtle changes and lesions in their early stages, even before they cause symptoms.
- Self-Examination: Get into the habit of performing a quick self-oral examination once a month. Use a bright light and a mirror to check your tongue, cheeks, gums, lips, and floor of the mouth for any unusual white or red patches, lumps, or non-healing sores.
- Address Chronic Irritation: Promptly address any sources of chronic irritation, such as ill-fitting dentures, rough edges on teeth or restorations, or persistent cheek biting. Your dentist can adjust or repair these issues.
4. Healthy Diet
- Fruits and Vegetables: Consume a diet rich in fruits, vegetables, and whole grains. These foods are packed with antioxidants, vitamins, and minerals that can help protect cells from damage and support a healthy immune system.
- Limit Processed Foods: Reduce intake of highly processed foods, sugary drinks, and excessive red and processed meats.
5. Sun Protection for Lips
- Lip Balm with SPF: If you spend a lot of time outdoors, use a lip balm or lipstick that contains a broad-spectrum SPF of 15 or higher to protect your lips from UV radiation, which can contribute to actinic cheilitis (a form of lip leukoplakia) and lip cancer.
- Wear Hats: Broad-brimmed hats can provide additional sun protection for your face and lips.
6. HPV Vaccination
- Consider Vaccination: The HPV vaccine (Gardasil 9) protects against several high-risk HPV types, including those linked to oral cancers and potentially some forms of oral leukoplakia. While primarily known for preventing cervical cancer, its role in preventing head and neck cancers is increasingly recognized. Discuss this with your healthcare provider.
Pro Tip: Don't delay seeing a dentist for any oral concerns, even if they seem minor. Early detection is key to successful management of leukoplakia and oral cancer.
Risks and Complications
While leukoplakia itself is not cancer, its primary and most serious risk is the potential for malignant transformation. Understanding these risks and potential complications is vital for patient education and management.
1. Malignant Transformation (Oral Cancer Development)
- Primary Risk: This is the overarching concern with leukoplakia. A significant percentage of leukoplakia lesions, particularly the non-homogeneous types and Proliferative Verrucous Leukoplakia (PVL), will eventually transform into oral squamous cell carcinoma.
- Transformation Rates: The estimated malignant transformation rate for oral leukoplakia overall ranges from 5% to 17% over a 10-year period, but it can be much higher for specific types:
- Homogeneous Leukoplakia: ~5-10%
- Erythroleukoplakia (mixed red/white): Up to 30-50%
- Proliferative Verrucous Leukoplakia (PVL): Up to 70-100%
- Factors Influencing Transformation:
- Degree of Dysplasia: The higher the grade of dysplasia (severe dysplasia carries a higher risk than mild dysplasia).
- Clinical Type: Non-homogeneous lesions (speckled, verrucous, nodular) have a higher risk than homogeneous ones.
- Site: Lesions on the floor of the mouth and the lateral/ventral (underside) tongue have a higher risk.
- Size: Larger lesions may carry a higher risk.
- Persistence: Lesions that persist despite removal of risk factors.
2. Recurrence
- Even after successful surgical removal, leukoplakia has a substantial risk of recurring at the same site or developing new lesions elsewhere in the mouth. Recurrence rates can be as high as 30-50%, highlighting the need for continuous surveillance.
- This is due to the concept of "field cancerization," where the entire oral mucosa has been exposed to carcinogens, making other areas susceptible to developing new lesions.
3. Morbidity from Treatment
While necessary, treatments, especially surgical ones, can carry their own risks:
- Pain and Discomfort: Post-operative pain is common, though usually manageable.
- Bleeding: Risk of excessive bleeding during or after surgery.
- Infection: Any surgical site can become infected, requiring antibiotics.
- Scarring: Surgical removal can leave scars, which might be noticeable depending on the location and size of the lesion.
- Altered Sensation: If nerves are involved or affected during surgery, there might be temporary or, rarely, permanent numbness or altered sensation in the area.
- Functional Impairment: Extensive surgical removal, particularly on the tongue or floor of the mouth, can temporarily or even permanently impact speech, chewing, or swallowing.

4. Psychological Impact
Living with a potentially precancerous condition can cause significant anxiety and psychological stress for patients. Regular follow-ups and the uncertainty of malignant transformation can be a source of ongoing concern.
5. Progression to More Advanced Oral Cancer
If leukoplakia transforms into oral cancer and is not detected and treated early, the cancer can metastasize (spread) to other parts of the body, most commonly the lymph nodes in the neck, and then to distant organs. This significantly worsens the prognosis and necessitates more aggressive, complex, and debilitating treatments (e.g., extensive surgery, radiation therapy, chemotherapy).
Pro Tip: Understanding these risks should not cause panic, but rather reinforce the importance of adherence to follow-up schedules, risk factor elimination, and prompt reporting of any new oral changes to your dental professional.
Comparison Tables
Table 1: Types of Oral Leukoplakia Comparison
| Feature | Homogeneous Leukoplakia | Erythroleukoplakia (Speckled) | Proliferative Verrucous Leukoplakia (PVL) | Oral Hairy Leukoplakia (OHL) |
|---|---|---|---|---|
| Appearance | Uniformly white, flat, smooth/finely wrinkled | Mixed red and white, often irregular/eroded | Multiple, thick, wart-like, exophytic lesions | White, "hairy" or corrugated, non-scrapable |
| Malignant Potential | Low (~5-10% over 10 yrs) | High (~30-50%) | Extremely High (~70-100% lifetime) | None (Benign) |
| Common Location | Buccal mucosa, tongue | Floor of mouth, lateral tongue, soft palate | Anywhere in the oral cavity, often multifocal | Lateral borders of the tongue |
| Primary Causes/Assoc. | Tobacco, Alcohol | Tobacco, Alcohol | Idiopathic, aggressive form of non-homogeneous | Epstein-Barr Virus (EBV) |
| Patient Profile | Smokers, heavy drinkers | Heavy smokers, heavy drinkers | Older individuals, often females, non-smokers possible | Immunocompromised (HIV/AIDS, transplant pts) |
| Recurrence Rate | Moderate | High | Very High | May recur with immunosuppression |
Table 2: Treatment Options Comparison for Dysplastic Leukoplakia
| Treatment Method | Efficacy for Dysplasia Removal | Typical Cost Range (USD) | Recovery Time | Invasiveness | Pros | Cons |
|---|---|---|---|---|---|---|
| Scalpel Excision | High; allows for clear margin assessment | $500 - $2,500 (office) | 1-2 weeks | Moderate | Definitive, excellent for pathology, precise | Requires sutures, potential scarring, post-op discomfort |
| Laser Excision | High; precise tissue removal | $1,000 - $5,000+ (office/outpatient) | 1-2 weeks | Moderate | Less bleeding, often less pain, high precision | Higher cost, requires specialized equipment, potential for scarring |
| Cryotherapy | Moderate; tissue destruction | $300 - $1,500 | 1-2 weeks | Low | Minimally invasive, relatively quick | Less precise, no tissue for pathology, higher recurrence rate |
| Photodynamic Therapy | Moderate; targeted cell destruction | $1,500 - $6,000 per session | Few days (photosensitivity) | Low | Non-invasive, targets abnormal cells | High cost, multiple sessions, temporary photosensitivity |
| Retinoid Therapy | Limited/Temporary; often adjunctive | $50 - $200 per month (medication) | Ongoing | Very low | Non-surgical, potential for regression | Temporary effects, potential side effects, not definitive |
Children / Pediatric Considerations
Leukoplakia is exceedingly rare in children. When it does occur, it warrants immediate and thorough investigation due to its unusual presentation in this age group. Unlike adults, where tobacco and alcohol are the primary culprits, these factors are typically absent in children.
If a white, non-scrapable lesion is found in a child's mouth, dental and medical professionals will consider a broader differential diagnosis before labeling it as leukoplakia, which is a diagnosis of exclusion. Potential causes in children could include:
- Traumatic Lesions: Chronic irritation from habits like cheek biting, thumb sucking, or ill-fitting orthodontic appliances.
- Frictional Keratosis: Similar to leukoplakia but specifically caused by chronic mechanical irritation.
- Congenital Conditions: Certain genetic syndromes or hereditary diseases can manifest with white oral lesions.
- Infectious Causes: While oral hairy leukoplakia is rare in children, it can occur in immunocompromised children (e.g., those with HIV or undergoing chemotherapy/transplantation).
- Nutritional Deficiencies: Though less common, severe deficiencies could potentially play a role.
Guidance for Parents: If you notice any persistent white patch or unusual lesion in your child's mouth, even if it appears harmless and causes no pain, it is crucial to seek immediate evaluation from a pediatric dentist or an oral medicine specialist. They will conduct a comprehensive examination, take a detailed medical history, and determine if a biopsy or further diagnostic tests are necessary. Prompt evaluation is key to identifying the underlying cause and ensuring appropriate management, ruling out any potentially serious conditions.
Cost Breakdown (Consolidated)
To provide a clear picture, here's a consolidated overview of costs associated with leukoplakia management in the US, encompassing various stages and scenarios.
1. Diagnostic Phase
- Initial Specialist Consultation: $150 - $400
- Incisional Biopsy (Procedure): $200 - $800
- Pathology Report (Lab Analysis): $100 - $300
- Total Diagnostic Range (without insurance): $450 - $1,500
2. Treatment Phase (if needed after biopsy)
- Simple Excisional Biopsy (entire lesion removed during initial biopsy): Often falls within the higher end of the diagnostic range, $400 - $1,500.
- Scalpel Excision (Separate Procedure):
- Small lesion: $500 - $1,500
- Moderate to large lesion or complex location: $1,500 - $2,500
- Laser Ablation/Excision:
- Small lesion: $1,000 - $2,500
- Moderate to large lesion, or multiple sites: $2,500 - $5,000+
- Cryotherapy/Electrocautery: $300 - $1,500 (less common for dysplastic leukoplakia)
- Photodynamic Therapy (per session): $1,500 - $6,000 (multiple sessions possible)
3. Post-Treatment and Surveillance
- Follow-up Appointments: $50 - $250 per visit (typically 3-6 month intervals initially, then annually).
- Repeat Biopsy: If recurrence or new lesions are suspected, the cost of another biopsy would apply, $200 - $800.
Cost Examples:
- Low End (Mild Leukoplakia, Diagnosed, Simple Excision):
- Consultation: $150
- Excisional Biopsy (including lab): $700
- 2 Follow-up visits: $100
- Total: ~$950
- Mid-Range (Dysplastic Leukoplakia, Scalpel Excision):
- Consultation: $250
- Incisional Biopsy (including lab): $600
- Separate Scalpel Excision: $1,800
- 4 Follow-up visits: $200
- Total: ~$2,850
- High End (Complex Dysplastic/PVL, Laser Excision):
- Consultation: $350
- Incisional Biopsy (including lab): $800
- Laser Excision (large/multifocal): $4,000
- 6 Follow-up visits: $300
- Total: ~$5,450+
With vs. Without Insurance
- Without Insurance: You will be responsible for 100% of these costs.
- With Medical Insurance: Most medical insurance plans cover the majority of diagnostic and surgical costs for leukoplakia, as it's a medical condition with cancer potential.
- Patient Responsibility: You'll typically pay your annual deductible first (e.g., $500 - $5,000, depending on your plan). After the deductible is met, you'll pay a co-insurance percentage (e.g., 10-30%) up to your out-of-pocket maximum.
- Example: For a $2,850 mid-range case with a $1,000 deductible and 20% co-insurance: You pay $1,000 (deductible) + 20% of ($2,850 - $1,000) = 20% of $1,850 = $370. Total out-of-pocket: $1,370.
Payment Plans and Financing Options
- Provider Payment Plans: Many specialists' offices offer flexible payment schedules directly.
- CareCredit & Other Medical Credit Cards: These allow you to finance medical expenses, often with interest-free periods if paid in full within a certain timeframe (e.g., 6, 12, 18 months).
- Health Savings Accounts (HSAs) & Flexible Spending Accounts (FSAs): These tax-advantaged accounts are excellent for covering out-of-pocket medical costs. Maximize contributions if eligible.
Cost-Saving Tips:
- Verify Insurance Coverage: Contact your medical insurance before any procedures to confirm coverage, deductibles, and co-insurance for specific CPT codes.
- Ask for Estimates: Request a detailed written estimate from your provider for all anticipated costs (surgeon's fee, facility fee, anesthesia, pathology).
- Compare Providers (if possible): While specialist expertise is key, if multiple qualified providers are available, compare their fee schedules.
- In-Network Providers: Always choose in-network providers to maximize insurance benefits.
- Generic Prescriptions: For any post-operative medications, ask if a generic option is available.
Frequently Asked Questions
Is leukoplakia always cancer?
No, leukoplakia is not cancer, but it is classified as a "potentially malignant disorder." This means a percentage of these lesions can transform into oral squamous cell carcinoma over time. The risk varies depending on the type of leukoplakia and the presence and degree of cellular dysplasia found on biopsy.
Can leukoplakia go away on its own?
In some cases, especially homogeneous leukoplakia that is mild and related to identifiable irritants (like tobacco), the lesion may regress or disappear if the irritating factor is completely eliminated. However, most established leukoplakia lesions, particularly those with dysplasia, are unlikely to resolve spontaneously and require active management or close monitoring.
Is leukoplakia painful?
Typically, leukoplakia is asymptomatic and causes no pain. It's often discovered incidentally during routine dental examinations. However, if the lesion becomes inflamed, ulcerated, or progresses to cancer, it can cause discomfort, a burning sensation, or pain, particularly when eating or drinking.
How is leukoplakia diagnosed?
Leukoplakia is primarily diagnosed through a thorough clinical examination by a dental professional, followed by a biopsy. The biopsy involves removing a small tissue sample, which is then sent to a pathologist for microscopic examination to confirm the diagnosis and assess for any precancerous (dysplastic) changes or actual cancer cells.
What's the difference between leukoplakia and thrush?
The main difference is that thrush (oral candidiasis) is a fungal infection that appears as creamy white patches and can usually be wiped or scraped off, revealing red, tender tissue underneath. Leukoplakia, on the other hand, is a white patch that cannot be scraped off and is a potentially precancerous lesion, not an infection.
How long does it take for leukoplakia to turn into cancer?
The timeline for malignant transformation is highly variable and unpredictable. It can range from months to many years, or some lesions may never transform. Factors like the degree of dysplasia, type of lesion, and continued exposure to risk factors influence this progression. Regular monitoring is essential due to this uncertainty.
Can quitting smoking reverse leukoplakia?
Quitting smoking, along with reducing alcohol intake, is the most impactful step a patient can take. For some, particularly those with homogeneous leukoplakia and no severe dysplasia, the lesions may partially or completely regress. However, for others, especially those with established dysplasia or non-homogeneous types, the lesions may persist or require further intervention.
What are the chances of recurrence after treatment?
Even after successful treatment, leukoplakia has a significant recurrence rate, sometimes as high as 30-50%. This is partly due to "field cancerization," where other areas of the oral mucosa remain susceptible to developing new lesions. This high recurrence rate underscores the importance of lifelong follow-up and continued avoidance of risk factors.
Does insurance cover leukoplakia treatment?
Yes, medical insurance typically covers the diagnosis and treatment of leukoplakia. Because it is considered a potentially malignant medical condition, rather than a purely dental issue, medical insurance usually covers consultations, biopsies, pathology fees, and surgical excisions, subject to your plan's deductibles, co-pays, and out-of-pocket maximums. It's crucial to verify coverage with your insurer beforehand.
Can stress cause leukoplakia?
There is no direct scientific evidence linking stress as a primary cause of leukoplakia. However, chronic stress can weaken the immune system and exacerbate certain oral conditions. While not a direct cause, it's generally advisable to manage stress for overall health, which indirectly contributes to oral well-being.
When to See a Dentist
Given the potentially serious nature of leukoplakia, knowing when to seek professional dental attention is paramount. Early detection dramatically improves outcomes.
See a Dentist Immediately (Within 1-2 weeks) if you notice any of the following "Red Flags":
- Any persistent white or grayish patch or lesion in your mouth that you cannot scrape off and that doesn't disappear within two weeks. This is the primary sign of leukoplakia.
- A white patch that has changed in appearance: growing larger, becoming thicker, developing red areas (erythroleukoplakia), or becoming rougher or more nodular.
- A non-healing sore, ulcer, or lump anywhere in your mouth that persists for more than two weeks, regardless of color.
- Any area of unusual firmness or hardening within your oral tissues.
- Difficulty or pain with chewing, swallowing, or speaking that is new and unexplained.
- Persistent numbness or tingling in your tongue, lip, or other areas of your mouth.
- A persistent sore throat or hoarseness that doesn't resolve.
- A lump in your neck that you haven't noticed before.
Routine Care Guidance: Even without these "red flags," regular dental check-ups (at least once a year, preferably twice) are essential. Your dentist is trained to perform oral cancer screenings during these visits and can often spot subtle changes that you might miss. This proactive approach is your best defense against both leukoplakia and oral cancer.
Emergency vs. Scheduled Appointment:
- Scheduled Appointment: For a simple white patch that you've just noticed and is not causing pain or any other severe symptoms, a prompt scheduled appointment with your general dentist is appropriate.
- Emergency Appointment: If you experience sudden, severe pain, rapid swelling, significant bleeding that won't stop, or if a lesion is rapidly growing or interfering with your ability to breathe or swallow, seek immediate emergency dental care or go to an urgent care facility. While rare for initial leukoplakia, these symptoms could indicate an advanced problem.
Pro Tip: Don't self-diagnose or wait to see if a suspicious patch goes away. Procrastination is the biggest enemy when it comes to potentially malignant conditions. If in doubt, get it checked out by a dental professional.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Floor of Mouth Cancer: Complete Guide
Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral c
February 23, 2026
Oral Cancer Stages Pictures: Complete Guide
Oral cancer, a serious and potentially life-threatening disease, affects thousands of Americans each year. According to the American Cancer Society, approximately 54,000 new cases of oral cavity or oropharyngeal cancer are diagnosed annually in the United States. While these numbers can be daunt
February 23, 2026
Can You Die From Mouth Cancer
Oral cancer is a formidable disease, often striking with insidious subtlety before revealing its devastating potential. It's a question that weighs heavily on the minds of those who receive a diagnosis or even those simply concerned about unusual oral symptoms: can you die from mouth cancer? The
February 23, 2026

Mouth Cancer Photos: Complete Guide
Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,23
February 23, 2026