Pleural Cavity: Complete Guide
Key Takeaways
- Imagine a crucial, fluid-filled space within your chest that allows your lungs to expand and contract effortlessly with every breath. This vital anatomical area is the pleural cavity, and its proper functioning is indispensable for life. While primarily associated with respiratory medicine, unde
Pleural Cavity: Complete Guide
Imagine a crucial, fluid-filled space within your chest that allows your lungs to expand and contract effortlessly with every breath. This vital anatomical area is the pleural cavity, and its proper functioning is indispensable for life. While primarily associated with respiratory medicine, understanding the pleural cavity's role is crucial for overall systemic health, including implications that can, in rare or severe cases, be influenced by conditions originating elsewhere in the body, such as infections that might, in extreme scenarios, trace back to oral health concerns. For an authoritative dental health portal like SmilePedia.net, exploring this topic underscores the interconnectedness of our body's systems and the far-reaching impact of maintaining comprehensive health.
This comprehensive guide will delve deep into the pleural cavity, explaining its anatomy, physiological function, and the various conditions that can affect it. We'll explore causes, symptoms, diagnostic methods, and the full spectrum of treatment options available in the US, including cost considerations and recovery expectations. By the end of this article, you will have a clear understanding of this essential bodily component and how to recognize when medical attention is needed for pleural-related issues.
Key Takeaways:
- The pleural cavity is a critical, fluid-filled space surrounding the lungs, facilitating smooth respiration by reducing friction.
- Common conditions include pleural effusion (fluid buildup), pneumothorax (collapsed lung), and pleurisy (inflammation).
- Symptoms often involve chest pain, shortness of breath, and cough, necessitating prompt medical evaluation.
- Diagnosis typically involves imaging (X-ray, CT scan) and sometimes fluid analysis via thoracentesis.
- Treatment ranges from observation and medication to invasive procedures like chest tube drainage or surgery, with costs varying widely from $500 for a simple thoracentesis to over $30,000 for complex surgeries.
- While primarily a respiratory concern, severe infections from other body parts, including very rarely from uncontrolled dental sources, can indirectly impact the pleural cavity.
- Early intervention is key to preventing serious complications and improving outcomes for pleural conditions.
What It Is / Overview
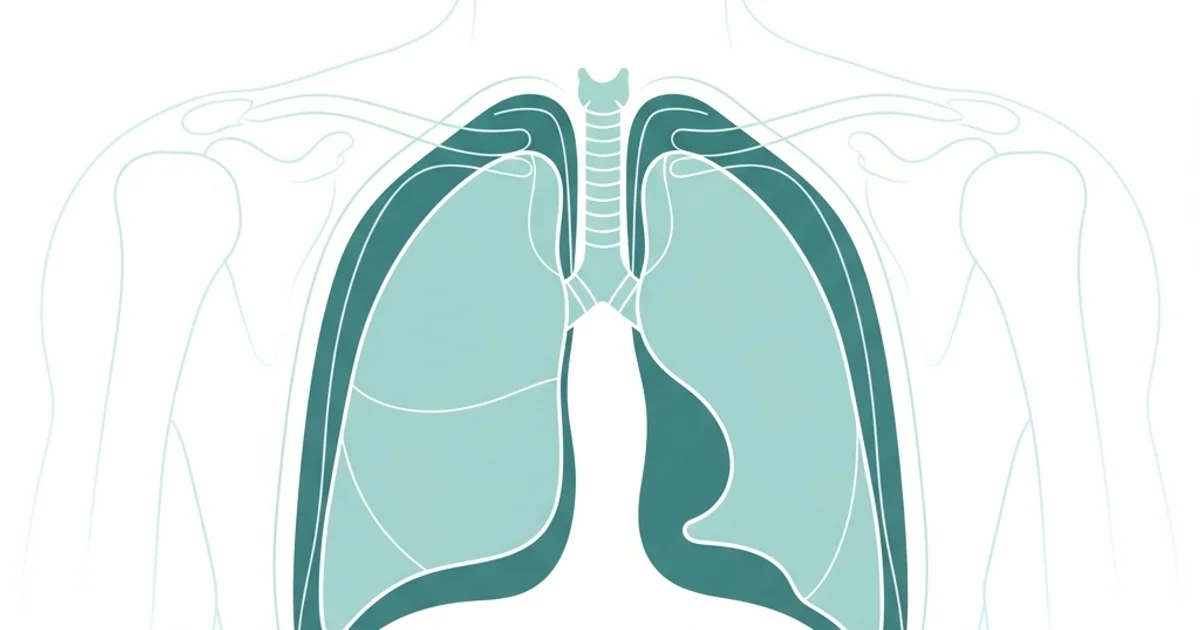
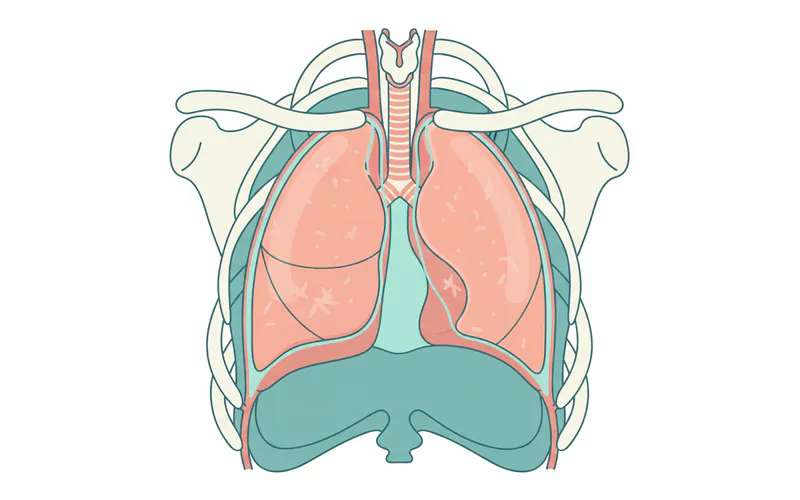
The pleural cavity is a potential space within the thoracic (chest) cavity that surrounds the lungs. It is not an empty space but rather a narrow, fluid-filled gap situated between two membranes known as the pleura. These membranes are crucial for respiratory function:
- Visceral Pleura: This inner layer directly covers the surface of each lung, dipping into the fissures that divide the lung lobes.
- Parietal Pleura: This outer layer lines the inside of the chest wall, the diaphragm, and the mediastinum (the central compartment of the chest containing the heart, great vessels, esophagus, and trachea).
Between these two layers lies the pleural cavity, containing a small amount (typically 10-20 mL) of serous, lubricating pleural fluid. This fluid serves two primary functions:
- Lubrication: It reduces friction between the visceral and parietal pleura, allowing the lungs to glide smoothly against the chest wall during inhalation and exhalation.
- Surface Tension: The fluid creates a strong adhesive force (like two wet glass slides sticking together) that keeps the visceral pleura (and thus the lung) closely apposed to the parietal pleura (and the chest wall). This adherence is vital because it allows the chest wall's expansion to pull the lungs outward, facilitating inflation. Without it, the lungs would collapse due to their natural elastic recoil.
The pressure within the pleural cavity, known as intrapleural pressure, is normally negative (sub-atmospheric). This negative pressure is essential for maintaining lung inflation. Any disruption to this delicate balance, whether by excess fluid, air, or inflammation, can significantly impair lung function.
Types / Variations (Conditions Affecting the Pleural Cavity)
Numerous conditions can affect the pleural cavity, leading to impaired breathing and other serious symptoms. These generally involve an accumulation of substances (fluid or air) or inflammation.
Pleural Effusion
This is the most common condition, characterized by the abnormal accumulation of fluid in the pleural cavity. The type of fluid determines the effusion's classification:
- Transudative Pleural Effusion: Caused by fluid leaking into the pleural space due to increased hydrostatic pressure or decreased oncotic pressure in the blood vessels, often without inflammation of the pleura itself.
- Common Causes: Congestive heart failure (most common), liver cirrhosis, nephrotic syndrome, peritoneal dialysis.
- Exudative Pleural Effusion: Caused by local inflammation, infection, or malignancy that increases the permeability of pleural capillaries, allowing protein-rich fluid, cells, and other substances to leak into the pleural space.
- Common Causes: Pneumonia, cancer (lung, breast, lymphoma), pulmonary embolism, autoimmune diseases (e.g., lupus, rheumatoid arthritis), pancreatitis, asbestos exposure.
- Hemothorax: The presence of blood in the pleural cavity.
- Common Causes: Trauma (e.g., rib fracture, penetrating chest injury), surgery, malignancy.
- Chylothorax: The presence of lymphatic fluid (chyle) in the pleural cavity, typically due to damage to the thoracic duct.
- Common Causes: Trauma, surgery (especially esophageal or cardiac), lymphoma.
- Empyema: The accumulation of pus in the pleural cavity, usually a complication of bacterial pneumonia. This is a severe form of exudative effusion.
- Common Causes: Bacterial pneumonia, lung abscess, chest trauma, thoracic surgery.
- Malignant Pleural Effusion: Fluid accumulation caused by cancer cells spreading to the pleura.
- Common Causes: Lung cancer, breast cancer, ovarian cancer, lymphoma, mesothelioma.
Pneumothorax (Collapsed Lung)
This condition involves the presence of air in the pleural cavity, which causes the lung to collapse partially or completely because the negative intrapleural pressure is lost.
- Spontaneous Pneumothorax: Occurs without any external injury.
- Primary Spontaneous Pneumothorax (PSP): Occurs in people without underlying lung disease, often tall, thin young men, possibly due to rupture of small air-filled sacs (blebs) on the lung surface. Smoking is a major risk factor.
- Secondary Spontaneous Pneumothorax (SSP): Occurs in individuals with underlying lung disease, such as COPD, asthma, cystic fibrosis, or pneumonia, which makes the lung more susceptible to rupture.
- Traumatic Pneumothorax: Results from an injury to the chest wall or lung.
- Causes: Stab wounds, gunshot wounds, blunt force trauma (e.g., car accident), iatrogenic (caused by medical procedures like central line insertion, lung biopsy, CPR).
- Tension Pneumothorax: A life-threatening condition where air enters the pleural cavity during inspiration but cannot escape during expiration, leading to a progressive buildup of pressure. This pressure pushes the mediastinum (heart, great vessels, trachea) to the opposite side, compromising cardiac output and respiratory function.
- Causes: Usually a complication of traumatic or iatrogenic pneumothorax, where a "one-way valve" effect allows air in but not out.
Pleurisy (Pleuritis)
Inflammation of the pleura, which causes sharp chest pain that worsens with deep breathing, coughing, or sneezing.
- Common Causes: Viral infections (most common), bacterial infections (e.g., pneumonia), pulmonary embolism, autoimmune diseases, cancer, rib fractures.
Mesothelioma
A rare but aggressive cancer of the pleura, primarily caused by asbestos exposure.
Causes / Why It Happens
The causes of pleural conditions are diverse, ranging from infections and systemic diseases to trauma and environmental exposures. Understanding the underlying mechanism is key to diagnosis and treatment.
Common Causes of Pleural Effusion:
- Heart Failure: Increased pressure in blood vessels causes fluid to leak into the pleural space (transudate).
- Pneumonia: Infection in the lung can spread to the pleura, causing inflammation and fluid accumulation (exudate, potentially empyema).
- Cancer: Malignant cells can invade the pleura, blocking lymphatic drainage or causing inflammation.
- Kidney Disease/Liver Cirrhosis: Leads to low protein levels in the blood, reducing oncotic pressure and allowing fluid to leak out.
- Pulmonary Embolism: Blood clots in the lungs can cause inflammation and fluid accumulation.
- Autoimmune Diseases: Conditions like rheumatoid arthritis or lupus can cause pleural inflammation.
- Trauma: Injuries to the chest can lead to hemothorax (blood) or chylothorax (lymphatic fluid).
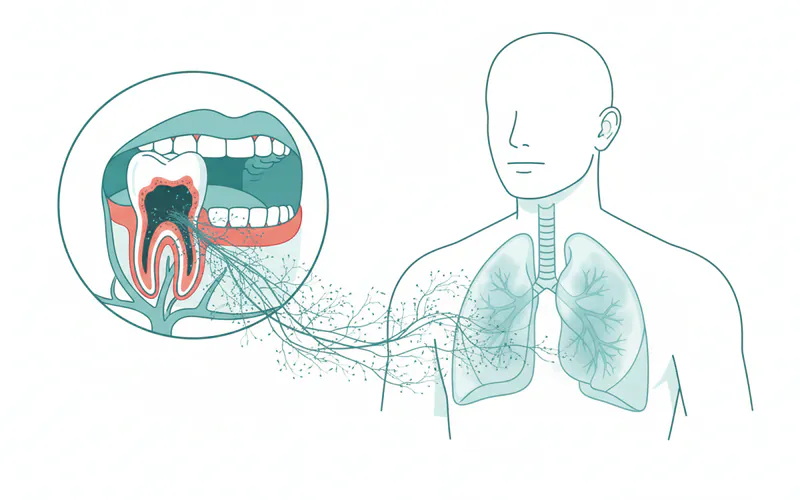
- Aspiration: While typically affecting the lungs, severe aspiration of stomach contents or oral bacteria can lead to aspiration pneumonia, which in turn can cause a complicated pleural effusion or empyema. This is where, in very rare and severe cases, untreated oral infections, including those stemming from a chipped tooth that harbors bacteria and impedes proper oral hygiene, could contribute to a higher bacterial load, increasing the risk of aspiration-related lung infections and their subsequent pleural complications. This link is indirect and represents an extreme scenario but highlights the systemic impact of oral health.
Common Causes of Pneumothorax:
- Trauma: Penetrating injuries (stabs, gunshot) or blunt force (car accidents) can directly puncture the lung or chest wall.
- Lung Diseases: COPD, cystic fibrosis, severe asthma, lung cancer, or infections can weaken lung tissue, making it prone to rupture.
- Medical Procedures: Biopsies, central line insertions, mechanical ventilation, or CPR can inadvertently injure the lung.
- Smoking: Increases the risk of bleb formation and rupture, particularly in spontaneous pneumothorax.
Common Causes of Pleurisy:
- Viral Infections: Often follows a cold or flu.
- Bacterial Infections: Pneumonia is a frequent cause.
- Pulmonary Embolism: As mentioned, clots can cause inflammation.
- Autoimmune Conditions: Systemic inflammatory diseases.
``
Signs and Symptoms
Recognizing the signs and symptoms of pleural conditions is crucial for timely medical intervention. While specific symptoms can vary depending on the underlying cause and severity, several common indicators should prompt medical evaluation.
- Chest Pain: This is often the most prominent symptom.
- Pleuritic Chest Pain: Sharp, stabbing pain that worsens with deep breathing, coughing, sneezing, or movement. It typically indicates inflammation of the pleura (pleurisy).
- Dull Aching Pain: May be present with large pleural effusions due to pressure on adjacent structures.
- Shortness of Breath (Dyspnea): Occurs when the fluid or air in the pleural cavity compresses the lung, reducing its ability to expand and exchange oxygen. Severity depends on the volume of fluid or air.
- Cough: A dry, non-productive cough is common, often triggered by irritation of the pleura or lung compression.
- Fever and Chills: Suggest an underlying infection, such as pneumonia leading to empyema.
- Rapid, Shallow Breathing: The body's attempt to minimize pleuritic pain or compensate for reduced lung capacity.
- Fatigue and Weakness: Can accompany chronic conditions or severe infections.
- Cyanosis: Bluish discoloration of the skin or lips, indicating severe oxygen deprivation, a critical sign in conditions like tension pneumothorax.
Pro Tip: Do not ignore persistent chest pain or unexplained shortness of breath. While a chipped tooth might cause discomfort, chest pain is a serious symptom that warrants immediate medical assessment to rule out cardiac, pulmonary, or pleural emergencies.
Diagnosis
Diagnosing pleural conditions involves a combination of medical history, physical examination, and various imaging and laboratory tests.
-
Medical History and Physical Exam:
- The doctor will ask about your symptoms, medical conditions, and lifestyle.
- During the physical exam, they will listen to your lungs with a stethoscope. Diminished or absent breath sounds over the affected area may indicate fluid or air accumulation. A pleural friction rub (a creaking sound) can be heard with pleurisy. Percussion (tapping on the chest) may reveal dullness (fluid) or hyper-resonance (air).
-
Imaging Studies:
- Chest X-ray: Often the first test. It can reveal pleural effusions (fluid appears as opacities, often blunting the costophrenic angles), pneumothorax (collapsed lung with visible visceral pleura line), or lung abnormalities.
- Computed Tomography (CT) Scan: Provides more detailed cross-sectional images, allowing for better characterization of fluid, air, masses, and underlying lung disease. It's excellent for identifying loculated (pocketed) effusions and differentiating between various types of pleural thickening.
- Ultrasound: Useful for detecting small effusions, guiding thoracentesis, and identifying septations (strands within the fluid) in complicated effusions or empyema.
- MRI: Less commonly used for primary pleural conditions but can be helpful in specific cases, especially for evaluating pleural tumors.
-
Pleural Fluid Analysis (Thoracentesis):
- If a significant pleural effusion is present, a procedure called thoracentesis is performed. This involves inserting a thin needle through the chest wall into the pleural cavity to withdraw a sample of pleural fluid.
- The fluid is then sent to a laboratory for analysis, which helps determine the cause of the effusion:
- Appearance: Clear, bloody, cloudy, milky.
- Cell Count and Differential: Presence of white blood cells (infection, inflammation), red blood cells (trauma, cancer).
- Protein and Lactate Dehydrogenase (LDH) Levels: Used to classify the effusion as transudative or exudative (Light's criteria).
- Glucose: Low levels suggest infection or malignancy.
- pH: Low pH suggests infection, cancer, or esophageal rupture.
- Microbiology: Gram stain, culture, and sensitivity to identify bacteria in empyema.
- Cytology: Examination for cancer cells.
- Other markers: Amylase (pancreatitis), triglycerides (chylothorax).
-
Pleural Biopsy:
- If fluid analysis is inconclusive, especially when cancer or tuberculosis is suspected, a small piece of the pleura may be biopsied. This can be done via needle biopsy or during a surgical procedure (thoracoscopy).
-
Bronchoscopy:
- If an underlying lung issue like a tumor or infection is suspected, a bronchoscope may be used to examine the airways and obtain samples.
Treatment Options
Treatment for pleural conditions varies widely depending on the specific diagnosis, its severity, and the patient's overall health. The primary goals are to relieve symptoms, remove fluid or air, and address the underlying cause.
A. For Pleural Effusion:
- Observation: Small, asymptomatic transudative effusions may not require specific treatment, especially if the underlying cause (e.g., mild heart failure) is being managed.
- Thoracentesis:
- Pros: Diagnostic (fluid analysis) and therapeutic (removes fluid to relieve symptoms). Relatively quick, minimally invasive.
- Cons: Temporary relief, risk of pneumothorax, bleeding, infection.
- Chest Tube Drainage (Tube Thoracostomy):
- Pros: Effective for large effusions, empyema, and hemothorax. Allows continuous drainage and medication instillation.
- Cons: Invasive, painful, requires hospitalization, risk of infection, tube dislodgement.
- Pleurodesis: A procedure to prevent recurrent pleural effusions (often malignant).
- Mechanism: A sclerosing agent (e.g., talc, doxycycline) is instilled into the pleural space via a chest tube, causing the two pleural layers to adhere to each other, thus obliterating the pleural cavity.
- Pros: Prevents fluid re-accumulation.
- Cons: Can be painful, may not be effective in all cases, requires chest tube.
- Indwelling Pleural Catheter (IPC):
- Mechanism: A small, flexible tube is surgically placed semi-permanently into the pleural space, allowing patients to drain fluid at home as needed.
- Pros: Good for recurrent effusions, especially in palliative care, improves quality of life, avoids repeated hospitalizations.
- Cons: Risk of infection, requires patient or caregiver training.
- Surgery (VATS or Thoracotomy):
- VATS (Video-Assisted Thoracoscopic Surgery): Minimally invasive. Used for complicated effusions (e.g., loculated empyema), biopsies, and talc pleurodesis.
- Thoracotomy: Open chest surgery. Reserved for complex cases, decortication (removal of thick, fibrous peel from the lung and pleura in chronic empyema), or extensive malignancy.
- Pros: Highly effective for specific indications, can resolve chronic issues.
- Cons: More invasive, longer recovery, higher risks (pain, infection, bleeding).
- Treating the Underlying Cause: Crucial for all effusions (e.g., diuretics for heart failure, antibiotics for pneumonia/empyema, chemotherapy/radiation for cancer).
B. For Pneumothorax:
- Observation: Small, stable spontaneous pneumothoraxes may resolve on their own with oxygen therapy.
- Needle Aspiration: For larger but stable pneumothoraxes, a small needle and syringe can be used to remove air.
- Chest Tube Drainage: Standard treatment for larger or symptomatic pneumothoraxes, and always for tension pneumothorax.
- Pleurodesis: Considered for recurrent pneumothorax.
- Surgery (VATS or Thoracotomy): For persistent air leaks, recurrent pneumothorax, or large blebs/bullae. Often involves pleurectomy (removal of pleura) or mechanical pleurodesis (abrasion of pleura).
C. For Pleurisy:
- Pain Management: NSAIDs (ibuprofen, naproxen) are often effective.
- Treating the Underlying Cause: Antibiotics for bacterial infections, antivirals for viral infections (if available), anticoagulants for pulmonary embolism.
``
Comparison Table: Common Pleural Procedures
| Procedure | Primary Use | Description | Average Recovery Time | Potential Risks |
|---|---|---|---|---|
| Thoracentesis | Diagnostic & therapeutic for pleural effusion | Needle inserted to remove fluid | 1-2 days (discomfort) | Pneumothorax, bleeding, infection, pain |
| Chest Tube Drainage | Large effusions, pneumothorax, empyema | Surgical insertion of a tube into the pleural space for continuous drainage | Days to weeks (hospital stay) | Infection, pain, tube dislodgement, lung injury |
| Pleurodesis | Recurrent effusions, recurrent pneumothorax | Instillation of a sclerosing agent (talc) or mechanical abrasion to fuse pleural layers | Days to weeks (hospital stay) | Pain, fever, acute respiratory distress, infection |
| VATS (Thoracoscopy) | Complicated effusions, biopsies, recurrent pneumothorax | Minimally invasive surgery with small incisions and a camera to view/treat the pleural space | 1-3 weeks | Bleeding, infection, air leak, nerve injury |
| Thoracotomy | Complex cases, decortication, extensive cancer | Open chest surgery with a larger incision to access the lungs and pleura | 4-8 weeks | Significant pain, longer recovery, infection, bleeding |
| Indwelling Pleural Catheter (IPC) | Recurrent malignant effusions | Semi-permanent catheter placed for intermittent home drainage | 1-2 weeks (placement healing) | Infection, blockage, pain around insertion site |
Step-by-Step Process: What to Expect During Chest Tube Insertion
A chest tube insertion (tube thoracostomy) is a common procedure for significant pleural effusions or pneumothorax. Here's what you can generally expect:
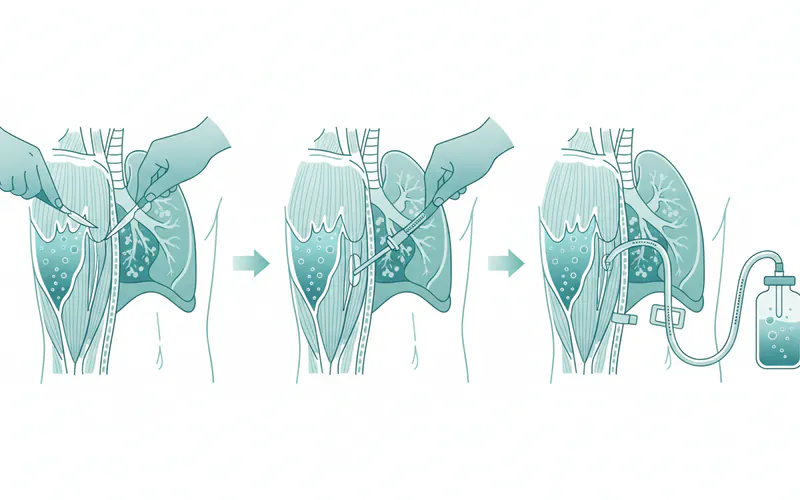
- Preparation: You will be positioned, usually semi-sitting or lying on your side with the arm on the affected side raised above your head. The area of insertion (typically between the ribs on the side of the chest) will be cleaned with an antiseptic solution and draped.
- Local Anesthesia: The doctor will inject a local anesthetic (like lidocaine) into the skin, muscle, and pleura. You will feel a sting and then numbness. It's crucial to inform the medical team if you feel any sharp pain during the procedure, despite the anesthetic.
- Incision: A small incision (typically 1-2 cm) is made in the skin.
- Dissection and Entry: The doctor will use a blunt instrument (or sometimes a finger) to carefully dissect through the muscle layers and create a pathway into the pleural cavity. You might feel pressure, but not sharp pain. This step is critical to avoid damaging the lung or other organs.
- Tube Insertion: A sterile chest tube (a flexible plastic tube) is then advanced through the incision and into the pleural space. The direction and depth depend on whether air or fluid is being drained. You might feel a sensation of pressure or discomfort as the tube is inserted.
- Securement and Connection: Once positioned, the tube is secured to your skin with sutures to prevent dislodgement. It is then connected to a drainage system, which typically includes a collection chamber, a water seal chamber (to prevent air from re-entering the chest), and sometimes a suction control chamber.
- Post-Procedure Checks: A chest X-ray will be performed immediately after insertion to confirm the tube's position and assess lung re-expansion.
- Management: While the tube is in place, nursing staff will monitor your vital signs, the amount and type of drainage, and look for air leaks. Pain medication will be administered as needed. The tube will remain until the lung has re-expanded and fluid/air drainage has ceased or significantly reduced, typically for a few days to a week or more.
- Removal: When criteria are met, the tube is removed, often after a final chest X-ray. The sutures are cut, and you'll be asked to take a deep breath and hold it (or exhale fully) as the tube is quickly pulled out. A sterile dressing is applied, and the site usually heals within a few days.
Cost and Insurance
The cost of diagnosing and treating pleural conditions in the US can vary significantly based on the specific condition, the procedures required, the healthcare facility (hospital vs. outpatient clinic), geographic location, and whether the patient has insurance.
Average US Price Ranges (Without Insurance):
| Procedure/Service | Low End (USD) | Mid Range (USD) | High End (USD) |
|---|---|---|---|
| Doctor Consultation | $150 | $300 | $600+ |
| Chest X-ray | $50 | $150 | $400+ |
| CT Scan (Chest) | $300 | $1,500 | $5,000+ |
| Chest Ultrasound | $100 | $400 | $1,000+ |
| Thoracentesis (Procedure Fee only) | $500 | $1,500 | $3,000+ |
| Pleural Fluid Analysis (Lab) | $200 | $800 | $2,000+ |
| Chest Tube Insertion (Hospital) | $5,000 | $15,000 | $30,000+ |
| VATS (Hospital/Surgeon Fees) | $15,000 | $30,000 | $75,000+ |
| Thoracotomy (Hospital/Surgeon Fees) | $30,000 | $60,000 | $150,000+ |
| Hospital Stay (per day) | $2,000 | $5,000 | $10,000+ |
| Indwelling Pleural Catheter (IPC) Placement | $5,000 | $10,000 | $20,000+ |
These are general ranges and can fluctuate wildly. They often do not include facility fees, anesthesia, pre/post-op care, or specialist consultations.
Insurance Coverage:
Most medical insurance plans (including employer-sponsored plans, ACA marketplace plans, Medicare, and Medicaid) cover medically necessary diagnostic tests and treatments for pleural conditions. However, coverage details will depend on your specific plan:
- Deductibles: The amount you must pay out-of-pocket before your insurance starts to cover costs.
- Copayments: A fixed amount you pay for a doctor's visit or prescription.
- Coinsurance: A percentage of the cost you are responsible for after meeting your deductible.
- Out-of-Pocket Maximum: The maximum amount you will have to pay for covered services in a plan year.
It's critical to verify your coverage with your insurance provider prior to any elective procedures. For emergency situations, most plans will cover the costs, though you will still be responsible for your plan's deductible and coinsurance. Always inquire about "in-network" vs. "out-of-network" providers, as using the latter can lead to significantly higher out-of-pocket costs.
Recovery and Aftercare
Recovery from pleural conditions and their treatments can vary greatly based on the underlying issue, the invasiveness of the procedure, and the individual's overall health.
General Recovery Principles:
- Pain Management: Expect some pain or discomfort, especially after invasive procedures like chest tube insertion or surgery. Your doctor will prescribe appropriate pain medication. It's important to manage pain effectively to allow for deep breathing and coughing, which are crucial for lung expansion and preventing complications.
- Activity Restrictions: Depending on the procedure, you may have activity restrictions for several weeks. After a pneumothorax, strenuous activities, heavy lifting, and even flying (due to pressure changes) may be restricted for a period.
- Wound Care: If you had a chest tube or surgery, you'll have an incision site that needs to be kept clean and dry. Follow specific instructions for dressing changes and watch for signs of infection (redness, swelling, pus, increasing pain).
- Breathing Exercises: Deep breathing exercises and incentive spirometry are often recommended to help re-expand the lungs and prevent atelectasis (partial lung collapse).
- Follow-up Appointments: Regular follow-up with your pulmonologist or surgeon is essential to monitor recovery, check for recurrence, and manage any ongoing symptoms. Chest X-rays or other imaging may be performed during these visits.
Specific Aftercare Notes:
- After Thoracentesis: You may have a small dressing over the insertion site. Avoid heavy lifting for a day or two. Report any sudden chest pain or shortness of breath.
- After Chest Tube Removal: A small dressing will cover the site. Keep it clean and dry. You might experience some localized pain or a "bubbling" sensation for a few days.
- After Pleurodesis: Pain management is crucial as the pleura adheres. This typically occurs in a hospital setting.
- After VATS/Thoracotomy: Expect more significant pain and a longer recovery period. Physical therapy may be recommended to regain strength and mobility.
Pro Tip: Adhere strictly to your post-treatment instructions. Early mobilization and deep breathing are key for recovery, but avoid overexertion. Discuss return-to-work or specific activity guidelines with your healthcare provider.
Prevention
Preventing pleural conditions often involves managing underlying health issues and adopting healthy lifestyle choices.
General Prevention Strategies:
- Manage Chronic Diseases: Effectively control conditions like heart failure, kidney disease, and autoimmune disorders to prevent transudative pleural effusions.
- Vaccinations: Get vaccinated against influenza and pneumococcal pneumonia, as these infections can lead to exudative effusions or empyema.
- Quit Smoking: Smoking is a major risk factor for spontaneous pneumothorax and COPD, which can predispose to pleural issues. It also increases the risk of lung cancer, a cause of malignant effusions.
- Avoid Asbestos Exposure: If you work in industries where asbestos is present, follow strict safety protocols to prevent exposure, which is the primary cause of mesothelioma.
- Treat Infections Promptly: Seek timely treatment for lung infections (pneumonia) to prevent complications like empyema.
- Prevent Trauma: Take precautions to avoid chest injuries, which can cause hemothorax or pneumothorax.
- Maintain Good Oral Hygiene: While not a direct cause, severe oral infections can increase the risk of aspiration pneumonia. Regularly visiting the dentist for cleanings and addressing issues like a chipped tooth can prevent bacterial overgrowth and reduce this highly indirect, but potential, risk pathway.
Risks and Complications
While treatments for pleural conditions are generally effective, like all medical interventions, they carry potential risks and complications.
- Pneumothorax: Can occur as a complication of thoracentesis or pleural biopsy, especially if the lung is accidentally punctured.
- Bleeding/Hemothorax: Injury to blood vessels during procedures can lead to bleeding into the pleural space.
- Infection: Introduction of bacteria during procedures can lead to empyema or wound infection.
- Pain: Post-procedure pain is common, and chronic pain (post-thoracotomy pain syndrome) can occur after surgery.
- Organ Injury: Rarely, procedures can inadvertently injure nearby organs like the liver, spleen, or diaphragm.
- Recurrence: Many pleural conditions, especially effusions and pneumothorax, have a risk of recurrence, necessitating further intervention.
- Acute Respiratory Distress Syndrome (ARDS): A severe, life-threatening lung injury that can occur as a complication of severe pleural infections or massive fluid removal.
- Trapped Lung: If a significant pleural effusion or empyema has been present for a long time, the lung may develop a fibrous peel that prevents it from fully re-expanding even after drainage. This may require surgery (decortication).
- Pleural Fibrosis/Thickening: Chronic inflammation or infection can lead to scarring and thickening of the pleura, potentially restricting lung movement.
Children / Pediatric Considerations
Pleural conditions in children, while less common than in adults, share many similarities but also present unique challenges and considerations.
- Pneumonia and Empyema: Bacterial pneumonia is the leading cause of pleural effusion and empyema in children. Streptococcus pneumoniae is a common culprit. Empyema in children often requires aggressive treatment, including antibiotics and chest tube drainage, and sometimes fibrinolytics or VATS to break up loculations.
- Spontaneous Pneumothorax: While rarer, it can occur in adolescents, particularly tall, thin boys, similar to adults. It can also be associated with underlying conditions like Marfan syndrome or cystic fibrosis.
- Traumatic Pneumothorax/Hemothorax: Children are susceptible to chest trauma, leading to these conditions, especially from falls, sports injuries, or accidents.
- Congenital Anomalies: Rarely, congenital lung or pleural abnormalities can predispose children to pleural issues.
- Symptoms in Children: May be less specific. Infants and young children may show irritability, feeding difficulties, or grunting in addition to fever, cough, and rapid breathing. Chest pain can be harder for them to localize or describe.
- Diagnosis and Treatment: Imaging (X-rays, ultrasound) is similar to adults, though radiation exposure is always a concern for CT scans. Thoracentesis and chest tube insertion are performed, often with smaller equipment. Surgical intervention (VATS) is often favored for complicated cases to minimize trauma and facilitate recovery.
- Importance of Early Diagnosis: Prompt recognition and treatment are critical in children to prevent long-term complications such as chronic lung disease or pleural fibrosis. Pediatric specialists (pulmonologists, thoracic surgeons) are often involved.
Cost Breakdown
Understanding the financial aspect of pleural care is essential for patients in the US. Costs are influenced by multiple factors, including the type of facility, geographical location, complexity of the condition, and insurance status.
Average US Costs:
- Low End (Conservative Management/Outpatient): For minor pleurisy or a very small, asymptomatic pleural effusion managed with medication and a few doctor visits, costs might range from $500 - $2,000. This would cover consultations, X-rays, and basic prescriptions.
- Mid-Range (Moderate Conditions/Inpatient): Conditions requiring procedures like thoracentesis, chest tube insertion, or a short hospital stay for a moderate pneumothorax or pleural effusion. Costs can range from $5,000 - $30,000. This would typically include diagnostic imaging, the procedure itself, professional fees, a few days of hospital stay, and follow-up care.
- High End (Severe Conditions/Surgery): Complex cases such as empyema requiring VATS or open thoracotomy, recurrent pneumothorax, or malignant effusions needing specialized interventions like pleurodesis or IPC. Costs can easily exceed $30,000 - $150,000+, encompassing extensive surgical fees, prolonged hospital stays, ICU care if needed, specialized medications, and intensive follow-up.
With vs. Without Insurance:
- With Insurance: After meeting your deductible (which can range from $500 to $10,000+ annually), your insurance will typically cover a significant portion of the remaining costs (e.g., 80% or more), up to your out-of-pocket maximum. Your actual out-of-pocket expense could be anywhere from a few hundred dollars to several thousand, depending on your plan's specifics and the total cost of care.
- Without Insurance: You will be responsible for 100% of the billed charges, which, as seen in the table above, can be financially devastating. Hospitals may offer uninsured patients discounted rates or payment plans if negotiated directly.
Payment Plans and Financing Options:
- Hospital Financial Aid: Many hospitals have financial assistance programs for uninsured or underinsured patients. Inquire with the hospital's billing department.
- Payment Plans: Hospitals and individual providers may offer interest-free payment plans to spread out the cost of care over several months or years.
- Medical Credit Cards: Services like CareCredit offer specialized credit lines for healthcare expenses. Be aware of interest rates and terms.
- Crowdfunding: For truly catastrophic costs, online crowdfunding platforms are an option, but success is not guaranteed.
Cost-Saving Tips:
- Verify Insurance Coverage: Always understand your benefits, deductibles, copayments, and out-of-pocket maximums before non-emergency procedures.
- In-Network Providers: Stick to healthcare providers and facilities that are in your insurance network to avoid higher "out-of-network" charges.
- Generic Medications: Opt for generic versions of prescribed medications when available.
- Negotiate: For uninsured patients, it's often possible to negotiate discounted rates with hospitals and providers. Don't hesitate to ask for the cash price before treatment.
- Itemized Bills: Request an itemized bill to review for any errors or duplicate charges.
- Telehealth Options: For initial consultations or follow-ups, telehealth might be a more cost-effective option than in-person visits.
Frequently Asked Questions
What is the main function of the pleural cavity?
The pleural cavity's main function is to facilitate smooth lung expansion and contraction during breathing. It achieves this by containing a small amount of lubricating fluid between the two pleural membranes, which reduces friction and maintains a negative pressure, essentially keeping the lungs "stuck" to the chest wall.
Can oral health impact lung health or the pleural cavity?
While the connection is indirect and uncommon, severe, uncontrolled oral infections (e.g., from a neglected chipped tooth or gum disease) can increase the bacterial load in the mouth. This can, in turn, heighten the risk of aspiration pneumonia in vulnerable individuals, especially those with impaired swallowing reflexes. Aspiration pneumonia, if severe, can lead to complicated pleural effusions or empyema, thus creating a rare, indirect pathway to pleural cavity issues.
What is the difference between the pleural cavity and the peritoneal cavity?
Both are serous cavities lined by membranes, but they are located in different parts of the body and serve distinct functions. The pleural cavity is in the chest, surrounding the lungs, and aids respiration. The peritoneal cavity is in the abdomen, surrounding most abdominal organs (stomach, intestines, liver, etc.), and allows for organ movement and contains peritoneal fluid.
How serious are conditions affecting the pleural cavity?
The seriousness varies widely. Simple pleurisy or a small, asymptomatic pleural effusion may resolve with minimal intervention. However, large pleural effusions, empyema, or a tension pneumothorax can be life-threatening emergencies requiring immediate medical attention and invasive procedures to prevent respiratory failure or cardiac collapse.
How is a collapsed lung (pneumothorax) treated?
Treatment depends on the size and cause of the collapse. Small, stable pneumothoraxes may be managed with observation and oxygen. Larger or symptomatic ones typically require needle aspiration or chest tube drainage to remove air and allow the lung to re-expand. Recurrent cases might need surgery or pleurodesis.
Is surgery always needed for pleural conditions?
No, surgery is not always needed. Many pleural conditions, such as small pleural effusions or mild pleurisy, can be managed with medication or less invasive procedures like thoracentesis. Surgery (VATS or thoracotomy) is reserved for more complex cases, such as persistent air leaks, complicated empyema, recurrent conditions, or malignant effusions that don't respond to other treatments.
How long does recovery take for pleural conditions?
Recovery time is highly variable. For a simple thoracentesis or mild pleurisy, recovery might be a few days. For chest tube insertion, it could be a week or more, including hospital stay. More invasive surgeries like VATS typically require 1-3 weeks for recovery, while an open thoracotomy can take 4-8 weeks or longer, with full strength returning gradually.
What causes the sharp pain associated with pleurisy?
The sharp, stabbing chest pain of pleurisy is caused by the inflamed layers of the pleura rubbing against each other during breathing. Normally, the pleural fluid acts as a lubricant, allowing these layers to glide smoothly. When inflamed, this lubrication is compromised, leading to friction and pain, especially with deep breaths, coughs, or movements.
What are the main risks of having a chest tube?
The main risks associated with chest tube insertion include pain at the insertion site, infection of the wound or pleural space, accidental puncture of the lung or other organs, bleeding, and accidental dislodgement of the tube. While rare, more severe complications like a persistent air leak or nerve damage can also occur.
Can pleural conditions recur?
Yes, many pleural conditions have a risk of recurrence. For example, spontaneous pneumothorax has a significant recurrence rate, particularly in smokers. Malignant pleural effusions are also prone to recurring after drainage. Procedures like pleurodesis or surgery are often performed to reduce the chances of recurrence for these specific conditions.
When to See a Doctor
Given the critical role of the pleural cavity in breathing, certain symptoms warrant immediate medical attention, while others require scheduled evaluation.
Emergency Medical Attention (Call 911 or go to the nearest ER):
- Sudden, Severe Chest Pain: Especially if it's crushing, squeezing, or accompanied by shortness of breath, radiating pain to the arm or jaw, or sweating. This could indicate a heart attack, but also a serious pleural event like a tension pneumothorax.
- Acute Shortness of Breath: Difficulty breathing that comes on suddenly, worsens rapidly, or makes it hard to speak.
- Rapid Breathing and Heart Rate: Especially if accompanied by dizziness or confusion.
- Bluish Discoloration (Cyanosis): Of the lips, fingers, or skin, indicating severe oxygen deprivation.
- Sudden Weakness or Collapse:
- Signs of Tension Pneumothorax: Severe shortness of breath, tracheal deviation (windpipe pushed to one side), distended neck veins, and dangerously low blood pressure.
Urgent Medical Consultation (See a doctor within 24-48 hours):
- Persistent Chest Pain: If pleuritic pain (sharp, worsening with breathing) continues for more than a day or two and is not relieved by over-the-counter pain relievers.
- New or Worsening Cough with Fever: Especially if accompanied by chills or production of colored sputum, suggesting a lung infection that could affect the pleura.
- Mild to Moderate Shortness of Breath: That is new, unexplained, or worsening over a few days.
- Unexplained Fatigue, Weight Loss, or Night Sweats: These can be signs of chronic underlying conditions, including some that affect the pleura (e.g., cancer, tuberculosis).
Routine Care Guidance:
- If you have a chronic medical condition (e.g., heart failure, COPD) that puts you at risk for pleural effusions, follow your doctor's management plan diligently and report any new or worsening symptoms during your regular check-ups.
- Maintain open communication with your primary care physician about any persistent or concerning symptoms, even if they seem mild.
Remember, prompt diagnosis and treatment are vital for managing pleural conditions effectively and preventing serious complications. Don't hesitate to seek medical advice if you are concerned about your breathing or chest symptoms.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

What Is an Abscess
Imagine a throbbing pain deep within your jaw, a persistent ache that keeps you awake at night and makes even the softest foods unbearable. This isn't just a bad toothache; it could be a sign of something much more serious: a dental abscess. Affecting millions of Americans annually, an abscess is an
February 22, 2026

Cracked Tooth Syndrome: Complete Guide
Cracked Tooth Syndrome: Complete Guide Category: Dental Conditions & Diseases
February 22, 2026
Dentinogenesis Imperfecta: Complete Guide
Imagine a world where your teeth, fundamental to chewing, speaking, and even smiling confidently, are inherently fragile, discolored, and prone to rapid wear from the moment they emerge. For individuals affected by dentinogenesis imperfecta (DI), this is a reality. While relatively rare, affecti
February 22, 2026

Stage 1 Early Cavity: Complete Guide
Did you know that dental cavities are one of the most common chronic diseases globally, affecting both children and adults? In the United States, over 90% of adults have had a cavity, and a significant portion of these begin as a stage 1 early cavity. Often invisible and painless in its nasc
February 22, 2026