Acid Reflux Teeth: Complete Guide

Key Takeaways
- Acid Reflux Teeth: Complete Guide
Acid Reflux Teeth: Complete Guide
Did you know that over 60 million Americans experience heartburn at least once a month, a key symptom of acid reflux? While many associate acid reflux with digestive discomfort, its impact often extends far beyond the esophagus, silently eroding one of your body's most resilient structures: your teeth. The constant wash of stomach acid can wreak havoc on your oral health, leading to sensitivity, decay, and even tooth loss if left unaddressed. Understanding the connection between acid reflux and your dental health is crucial for preserving your smile and preventing irreversible damage. This comprehensive guide will delve into what acid reflux teeth are, why they occur, how to identify the subtle yet significant signs of calcium deficiency in teeth caused by acid erosion, the available treatments, and, most importantly, how to protect your pearly whites from this silent attacker. We'll explore everything from lifestyle changes and medical interventions to advanced dental restorations, ensuring you have all the knowledge to safeguard your oral health.
Key Takeaways:
- Acid reflux (GERD) directly erodes tooth enamel: Stomach acid, with a pH as low as 1.5-3.5, can dissolve enamel, leading to sensitivity, cavities, and changes in tooth appearance.
- Early detection is key: Dental professionals often spot acid erosion before individuals are aware of their reflux, highlighting the importance of regular check-ups.
- Treatment costs vary widely: Minor erosion repairs (bonding) can range from $150-$600 per tooth, while extensive damage requiring crowns or veneers can cost $800-$2,500+ per tooth, often covered partially by dental insurance.
- Prevention is paramount: Lifestyle and dietary changes, alongside meticulous oral hygiene (e.g., waiting 30-60 minutes to brush after reflux), are crucial to halt progression.
- Long-term management: Effective management of acid reflux, medically and through lifestyle, is essential to prevent ongoing dental damage.
- Pediatric risk: Children with reflux are particularly vulnerable due to thinner enamel, requiring proactive monitoring and preventive care.
- Not just erosion: Severe, prolonged reflux can sometimes manifest as extreme calcium buildup on teeth (calculus) in less affected areas, paradoxically due to changes in saliva pH and mineral saturation, though erosion is the primary concern.
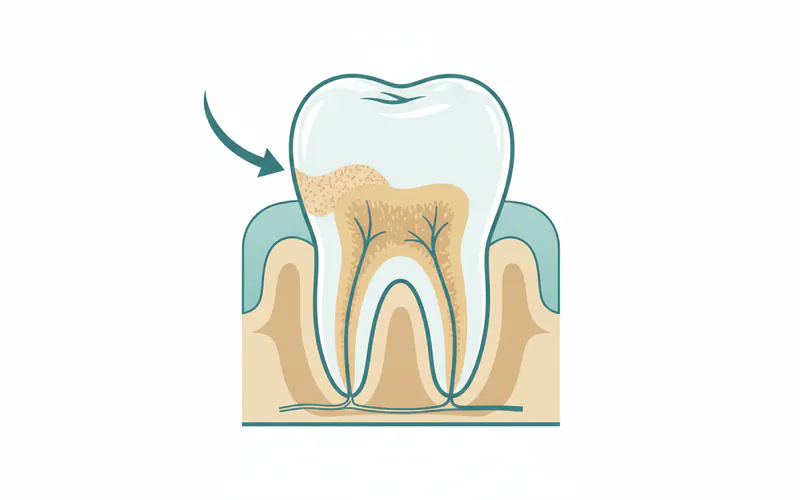
![A cross-section of a tooth showing enamel erosion on the lingual (tongue-facing) surface, with an arrow pointing to the thinning enamel and exposed dentin(/glossary/glossary-dentin). The image should also show an eroded molar with a distinct 'scooped-out' appearance.]
{kind=link}
What It Is / Overview
Acid reflux, medically known as Gastroesophageal Reflux Disease (GERD), occurs when stomach acid frequently flows back into the tube connecting your mouth and stomach (esophagus). This backward flow, called reflux, can irritate the lining of your esophagus. However, its corrosive power extends beyond the esophagus, reaching the oral cavity and directly impacting your teeth.

Acid reflux teeth refers to the dental damage, primarily enamel erosion, caused by repeated exposure to stomach acid. Enamel, the hardest substance in the human body, is designed to protect the softer, underlying dentin. While incredibly strong, enamel is highly susceptible to acid dissolution. Stomach acid is potent, with a pH typically ranging from 1.5 to 3.5, significantly more acidic than the critical pH of 5.5 at which tooth enamel begins to demineralize. When this acid washes over teeth, it strips away the protective enamel, leading to a host of dental problems.
This process is insidious because it's often painless in its early stages. Many individuals may not even realize they have acid reflux or that it's harming their teeth until significant damage has occurred. Dental professionals are frequently the first to identify the characteristic patterns of acid erosion, often on the lingual (tongue-facing) surfaces of upper teeth and the occlusal (biting) surfaces of molars, serving as a critical diagnostic clue for underlying reflux.
Types / Variations
The impact of acid reflux on teeth can vary depending on the specific type of reflux and its severity.
Gastroesophageal Reflux Disease (GERD)
GERD is the most common form of chronic acid reflux, characterized by frequent and persistent backward flow of stomach acid.
- Dental Impact: This type typically causes widespread erosion, especially on the lingual surfaces of the maxillary (upper) anterior teeth and the occlusal surfaces of posterior teeth. The pattern is often smooth and generalized, rather than localized to specific areas like typical cavities. Patients might also experience a constant sour taste.
Laryngopharyngeal Reflux (LPR)
Often called "silent reflux," LPR involves stomach acid traveling all the way up into the throat and even the nasal passages, without the typical heartburn symptoms associated with GERD.
- Dental Impact: While LPR primarily affects the throat (hoarseness, chronic cough, globus sensation), the aerosolized acid can still come into contact with teeth, leading to a more diffuse, generalized erosion pattern. Because symptoms are less overt, the dental damage from LPR might progress further before the underlying cause is identified.
Bulimia Nervosa
While not a type of acid reflux itself, bulimia nervosa involves self-induced vomiting, which is a significant source of highly acidic gastric contents.
- Dental Impact: The pattern of erosion in bulimia is strikingly similar to GERD, often severe on the lingual surfaces of the upper teeth due to the direct contact of vomitus. However, it can often be distinguished by other oral signs, such as trauma to the soft palate or knuckles (Russell's sign). This condition demands a multidisciplinary approach involving both medical and dental professionals.
Chronic Heartburn Without GERD Diagnosis
Some individuals experience occasional heartburn or regurgitation that doesn't meet the clinical criteria for GERD.
- Dental Impact: Even intermittent exposure to stomach acid can contribute to subtle enamel changes over time, increasing tooth sensitivity and susceptibility to decay. The damage might be less severe or widespread but still warrants attention.
Understanding these variations helps dentists identify the root cause of dental erosion and recommend appropriate management strategies, both for oral health and overall well-being.
Causes / Why It Happens
The primary cause of acid reflux teeth is the direct exposure of tooth enamel to stomach acid. This exposure leads to chemical dissolution of the enamel, a process distinct from bacterial decay.
Physiological Causes of Acid Reflux:
The mechanisms behind acid reflux itself are varied:
- Weak Lower Esophageal Sphincter (LES): The LES is a ring of muscle at the bottom of the esophagus that acts as a valve. When it relaxes inappropriately or weakens, stomach contents can flow back up. This is the most common cause of GERD.
- Hiatal Hernia: A condition where the upper part of the stomach pushes up through the diaphragm into the chest cavity. This can prevent the LES from closing properly, leading to reflux.
- Slow Stomach Emptying (Gastroparesis): If the stomach takes too long to empty its contents into the small intestine, pressure can build up, increasing the likelihood of reflux.
- Increased Abdominal Pressure: Conditions like obesity, pregnancy, and even tight clothing can put pressure on the abdomen, forcing stomach acid upwards.
Contributing Factors to Dental Erosion from Reflux:
Beyond the presence of reflux, several factors influence the severity of dental damage:
- Frequency and Duration of Reflux Episodes: More frequent and longer exposures to acid lead to greater enamel loss.
- Acidity (pH) of Refluxate: The lower the pH (more acidic), the more aggressive the erosion. Stomach acid is particularly destructive.
- Salivary Flow Rate and Buffering Capacity: Saliva is a natural defense mechanism. It neutralizes acids, washes away food debris, and helps remineralize enamel. Individuals with dry mouth (xerostomia) or reduced salivary flow are at higher risk of acid erosion. Saliva also contains calcium and phosphate ions that can help repair early enamel lesions.
- Dietary Habits: A diet high in acidic foods and drinks (citrus fruits, sodas, sports drinks, vinegar) can compound the damage from reflux. These external acids weaken enamel, making it even more susceptible to stomach acid.
- Bruxism (Teeth Grinding): Grinding or clenching teeth can accelerate the wear of already weakened enamel, causing more rapid tooth destruction when combined with acid erosion.
- Oral Hygiene Practices: While good oral hygiene is essential, improper brushing immediately after a reflux episode can actually worsen erosion by mechanically scrubbing away softened enamel.
- Medications: Certain medications can either contribute to acid reflux (e.g., NSAIDs, some blood pressure medications) or reduce salivary flow, indirectly exacerbating dental erosion.
Understanding these intertwined factors is critical for a comprehensive approach to managing both acid reflux and its dental consequences.
Signs and Symptoms
Recognizing the signs of calcium deficiency in teeth due to acid erosion is crucial for early intervention. Unlike traditional cavities caused by bacteria, acid erosion doesn't always present with pain until significant enamel is lost. Dental professionals are often the first to spot these subtle but telltale signs.
Common Dental Symptoms:
- Tooth Sensitivity: This is often one of the first and most common symptoms. As enamel erodes, the underlying dentin, which contains thousands of microscopic tubules leading to the tooth's nerve, becomes exposed. This leads to sharp pain or discomfort when consuming hot, cold, sweet, or acidic foods and drinks, or even when exposed to cold air.
- Changes in Tooth Appearance:
- Smooth, Shiny Surfaces: Eroded enamel often appears unnaturally smooth and shiny, sometimes described as having a "glazed" look, especially on the biting surfaces of back teeth and the tongue-side of front teeth.
- Discoloration: Teeth may appear more yellow or translucent. This happens because the white enamel is thinned or lost, revealing the naturally yellowish dentin beneath.
- Rounded Edges: The sharp edges of teeth, particularly incisors, can become rounded or worn down.
- "Scooped Out" or Cupped Surfaces: On the biting surfaces of molars, acid erosion often creates distinct, concave depressions or "cups" in the enamel, sometimes with fillings appearing to "stand proud" (elevated) because the surrounding tooth structure has eroded away.
- Increased Risk of Decay: While acid erosion isn't decay itself, the thinning of enamel makes teeth significantly more vulnerable to bacterial acid attacks, leading to cavities.
- Thinning or Shortening of Teeth: Over time, severe erosion can visibly shorten teeth, altering your bite and facial aesthetics.
- Cracks and Chips: Eroded enamel is weaker and more brittle, making teeth more prone to chipping or cracking, particularly on the edges of front teeth.
- Restoration Issues: Existing fillings, crowns, or veneers might appear to be "above" the tooth surface as the surrounding natural tooth structure erodes away. This can also lead to marginal leakage and recurrent decay.
Other Oral and General Symptoms (Indicating Reflux):
- Chronic Bad Breath (Halitosis): Acid reflux can contribute to persistent bad breath.
- Sour Taste in Mouth: A frequent metallic or sour taste, especially in the mornings.
- Dry Mouth (Xerostomia): While not directly caused by reflux, medications for reflux can sometimes cause dry mouth, which exacerbates dental erosion by reducing the protective effect of saliva.
- Difficulty Swallowing (Dysphagia): A sign of esophageal irritation.
- Hoarseness or Chronic Sore Throat: Common with LPR (silent reflux).
- Frequent Clearing of Throat or Chronic Cough: Also common with LPR.
- Chest Pain/Heartburn: The classic symptom of GERD.
Pro Tip: If you notice any of these dental changes, especially sensitivity or altered tooth appearance, schedule an appointment with your dentist promptly. They are skilled at diagnosing acid erosion and can help identify the underlying cause, potentially leading to an earlier diagnosis of reflux.
Treatment Options
Treating acid reflux teeth requires a dual approach: managing the underlying acid reflux and repairing the dental damage. Both aspects are crucial for long-term success.
A. Dental Treatment Options (Repairing Damage)
The choice of dental treatment depends on the severity and extent of enamel erosion.
-
Fluoride Therapy:
- What it is: Professional application of high-concentration fluoride varnish, gel, or foam. Prescription fluoride toothpastes or rinses for home use may also be recommended.
- Pros: Strengthens enamel, increases resistance to acid, reduces sensitivity. Non-invasive and relatively inexpensive.
- Cons: Not a restorative treatment; doesn't replace lost enamel. Needs regular reapplication.
- Cost: In-office fluoride applications typically range from $30-$70 per session. Prescription toothpaste can be $15-$30 per tube.
-
Dental Bonding (Composite Resin):
- What it is: A tooth-colored resin material is applied to the eroded areas, sculpted, and hardened with a special light.
- Pros: Minimally invasive, relatively quick (one appointment), matches tooth color well, cost-effective for minor to moderate erosion.
- Cons: Less durable than other restorations, can chip or stain over time, typically lasts 5-10 years.
- Cost: $150-$600 per tooth, depending on size and location of restoration.
-
Dental Veneers:
- What it is: Thin, custom-made shells (porcelain or composite) that cover the front surface of teeth.
- Pros: Excellent aesthetic results, very durable (porcelain), can correct severe erosion, discoloration, and minor alignment issues.
- Cons: More invasive (requires enamel removal), irreversible, higher cost, can be susceptible to chipping if not properly cared for.
- Cost: $800-$2,500+ per tooth for porcelain veneers; $250-$1,500 per tooth for composite veneers.
-
Dental Crowns (Caps):
- What it is: Full coverage caps placed over the entire tooth surface, custom-made from porcelain, ceramic, metal, or a combination.
- Pros: Provides maximum protection and strength for severely eroded or fractured teeth, restores function and aesthetics.
- Cons: More invasive (requires significant tooth reduction), higher cost, multiple appointments typically.
- Cost: $800-$2,500+ per tooth, depending on material and location.
-
Inlays and Onlays:
- What it is: Indirect restorations (made in a lab and cemented onto the tooth) used for moderate damage on the chewing surfaces of back teeth, when a filling isn't enough but a full crown isn't needed.
- Pros: More durable and longer-lasting than traditional fillings, conserve more natural tooth structure than crowns.
- Cons: Requires two appointments, higher cost than fillings.
- Cost: $600-$1,200 per tooth.
B. Medical Treatment Options (Managing Reflux)
Addressing the root cause of reflux is critical to prevent further dental damage. Consult a medical doctor or gastroenterologist for diagnosis and treatment.
-
Lifestyle and Dietary Modifications:
- What it is: Avoiding trigger foods (spicy, fatty, acidic), eating smaller meals, not eating close to bedtime, elevating the head during sleep, weight management, quitting smoking, reducing alcohol and caffeine intake.
- Pros: Non-pharmacological, can be highly effective, improves overall health, cost-free.
- Cons: Requires significant discipline and habit change.
-
Antacids:
- What it is: Over-the-counter medications (e.g., Tums, Rolaids) that neutralize stomach acid for quick, temporary relief.
- Pros: Fast-acting, readily available.
- Cons: Short-term relief only, not for chronic management, excessive use can have side effects (e.g., altered calcium levels).
-
H2 Blockers (Histamine-2 Receptor Blockers):
- What it is: Medications (e.g., Pepcid AC, Zantac 360) that reduce acid production in the stomach for a longer duration than antacids.
- Pros: Provides longer-lasting relief than antacids, available OTC and by prescription.
- Cons: May take longer to work than antacids, not as potent as PPIs for severe reflux.
-
Proton Pump Inhibitors (PPIs):
- What it is: Strongest class of acid-reducing medications (e.g., Prilosec, Nexium). They block the "pumps" in the stomach lining that produce acid.
- Pros: Highly effective for chronic GERD, provide long-term acid suppression.
- Cons: Prescription-strength versions, potential long-term side effects (e.g., nutrient deficiencies, increased risk of certain infections, bone density changes), should be used under medical supervision.
-
Surgery:
- What it is: Procedures like Nissen fundoplication or LINX device implantation aim to strengthen the LES or create a barrier to reflux.
- Pros: Can offer a long-term solution for severe, intractable GERD.
- Cons: Invasive, risks associated with surgery, not suitable for all patients.
Step-by-Step Process: Addressing Acid Reflux Teeth
Addressing dental erosion caused by acid reflux typically involves a multi-stage process, integrating both dental and medical management.
Step 1: Initial Dental Consultation and Diagnosis
- What to Expect: Your dentist will conduct a thorough oral examination, looking for characteristic signs of acid erosion (smooth, shiny surfaces, cupping, sensitivity, wear patterns, signs of calcium deficiency in teeth). They will inquire about your medical history, dietary habits, and any symptoms of acid reflux. X-rays may be taken to assess the internal health of the teeth and bone.
- Key Action: Be open and honest about any reflux symptoms, even mild ones, as this information is crucial for diagnosis.
Step 2: Confirmation of Acid Reflux (Medical Consultation)
- What to Expect: If dental erosion is strongly indicative of reflux, your dentist will likely recommend you consult a medical doctor or gastroenterologist. The medical doctor will assess your symptoms, medical history, and may perform diagnostic tests such as:
- Upper Endoscopy: A flexible tube with a camera is inserted down the throat to visualize the esophagus, stomach, and duodenum.
- pH Monitoring: A device measures acid levels in the esophagus over 24-48 hours.
- Esophageal Manometry: Measures the strength and coordination of esophageal muscle contractions.
- Key Action: Follow through with medical referrals. Effective management of reflux is paramount to prevent further dental damage.
Step 3: Dental Treatment Planning
- What to Expect: Once the extent of dental damage is assessed and reflux is being managed, your dentist will develop a personalized treatment plan. This plan considers:
- Severity of erosion
- Number of affected teeth
- Your aesthetic goals
- Your budget
- Treatment Phases:
- Phase 1: Stabilization & Prevention (Often first): This might include professional fluoride treatments, prescription fluoride toothpaste, and education on proper oral hygiene techniques (e.g., waiting to brush after reflux, using soft-bristled brushes). A custom nightguard may be recommended if bruxism is also present.
- Phase 2: Restoration (Repairing damage): This could involve:
- Dental Bonding for minor to moderate erosion.
- Inlays/Onlays for moderate posterior damage.
- Veneers for aesthetic and protective coverage of front teeth.
- Crowns for severely damaged or fractured teeth, or when significant tooth structure is lost.
- Key Action: Discuss all options, pros, cons, and costs thoroughly with your dentist.
Step 4: Dental Treatment Execution
- What to Expect: This is where the planned restorations are performed. The process varies depending on the chosen treatment:
- Bonding: Completed in one visit. Tooth prepared, resin applied, sculpted, hardened, and polished.
- Veneers/Crowns/Inlays/Onlays: Typically two visits.
- Visit 1: Tooth preparation (shaping), impressions taken, temporary restorations placed.
- Visit 2: Removal of temporaries, try-in of permanent restorations, final cementation.
- Key Action: Follow pre- and post-treatment instructions carefully.
Step 5: Ongoing Management and Maintenance
- What to Expect:
- Regular Dental Check-ups: Essential for monitoring existing restorations, detecting any new erosion, and reinforcing preventive measures. Your dentist will continue to assess your oral hygiene habits and may recommend additional fluoride applications.
- Continued Reflux Management: Consistently follow your medical doctor's advice regarding medication, lifestyle changes, and dietary restrictions to keep reflux under control.
- Dietary and Lifestyle Adjustments: Incorporate daily habits that protect your teeth (e.g., rinsing with water after reflux, chewing sugar-free gum to stimulate saliva).
- Key Action: Be proactive in both your dental and medical care. This is a long-term commitment for optimal health.


Cost and Insurance
The cost of treating acid reflux teeth can vary significantly based on the severity of the erosion, the type of dental restorations needed, your geographic location, and whether you have dental insurance.
Average US Price Ranges (Without Insurance):
| Treatment Type | Average Cost Range (Per Tooth) | Notes |
|---|---|---|
| Professional Fluoride | $30 - $70 | Often covered by insurance once or twice a year. |
| Dental Bonding | $150 - $600 | For minor to moderate erosion, direct composite resin. |
| Inlays / Onlays | $600 - $1,200 | For moderate posterior damage, indirect restoration. |
| Composite Veneers | $250 - $1,500 | Direct application, less durable than porcelain. |
| Porcelain Veneers | $800 - $2,500+ | Custom-made lab restoration, highly aesthetic and durable. |
| Dental Crowns | $800 - $2,500+ | For severe damage or fracture, covers entire tooth. |
| Root Canal (if needed) | $700 - $2,000+ | If erosion leads to nerve exposure/infection, followed by a crown. |
| Total Est. Severe Damage | $5,000 - $20,000+ | For full mouth reconstruction in extreme cases. |
These are general estimates. Costs can be higher in metropolitan areas or with specialist dentists.
Insurance Coverage Details:
Most dental insurance plans differentiate between "preventive," "basic," and "major" restorative services.
- Preventive: Fluoride treatments are usually covered at 80-100%. Regular check-ups are also fully covered.
- Basic Restorative: Dental bonding and some fillings (if erosion has led to decay) might be covered at 50-80%.
- Major Restorative: Veneers, crowns, inlays, onlays, and root canals are typically considered major procedures and are often covered at 20-50%, subject to deductibles and annual maximums (which often range from $1,000 to $2,000 per year).
Important Considerations:
- Pre-authorization: For major restorative work, your dentist may need to submit a pre-treatment estimate to your insurance company to determine exact coverage.
- Waiting Periods: Some insurance plans have waiting periods (e.g., 6-12 months) before major restorative procedures are covered.
- Medical vs. Dental: Treatments for the underlying acid reflux itself (medications, surgery) are typically covered by medical insurance, not dental. Ensure your medical plan is up-to-date.
Cost-Saving Tips:
- Early Detection: The most effective way to save money is to address acid reflux and dental erosion early. Minor bonding is far less expensive than crowns or veneers.
- Preventive Care: Regular dental check-ups and cleanings, along with meticulous home care, can prevent minor erosion from becoming major damage.
- Payment Plans: Many dental offices offer in-house payment plans or work with third-party financing options like CareCredit, which allows you to spread the cost over several months or years, often with low or no interest.
- Dental Schools: University dental schools often provide services at a reduced cost, with treatment performed by supervised students.
- Community Clinics: Look for community dental clinics or public health programs that offer services on a sliding scale or at lower costs.
- Discuss Options: Always discuss all available treatment options and their associated costs with your dentist. Sometimes, a less expensive, temporary solution can be used while you save for a more permanent one.
Recovery and Aftercare
Effective recovery and long-term aftercare for acid reflux teeth involve both maintaining your dental restorations and preventing further acid damage.
After Dental Restorations:
- Temporary Sensitivity: It's common to experience some temporary sensitivity to hot and cold after restorations like bonding, veneers, or crowns. This usually subsides within a few days to weeks. Your dentist may recommend a desensitizing toothpaste.
- Bite Adjustment: If you received crowns, inlays, or onlays, your bite might feel slightly off initially. Your dentist will adjust it to ensure proper occlusion and comfort.
- Avoid Staining Foods: For bonding, avoid highly staining foods and drinks (coffee, tea, red wine, berries) for the first 24-48 hours.
- Care for Restorations:
- Brush Gently: Use a soft-bristled toothbrush and non-abrasive toothpaste.
- Floss Daily: Continue to floss around your restorations to prevent plaque buildup.
- Avoid Hard/Sticky Foods: Be cautious with very hard foods (nuts, ice) or sticky candies, as they can dislodge or chip restorations.
- Regular Check-ups: Continue with your recommended schedule of dental check-ups (usually every 6 months) to allow your dentist to monitor the integrity of your restorations and overall oral health.
Preventing Further Acid Damage:
This is the most critical aspect of long-term aftercare and will directly impact the longevity of your dental work and the health of your remaining natural teeth.
-
Manage Your Acid Reflux:
- Adhere to Medical Treatment: Consistently follow your doctor's recommendations for medications (PPIs, H2 blockers) and scheduled follow-up appointments.
- Lifestyle Modifications: Continue to implement dietary changes (avoiding triggers like spicy, fatty, acidic foods, caffeine, alcohol), maintain a healthy weight, quit smoking, and avoid eating 2-3 hours before bedtime. Elevating your head while sleeping can also help.
-
Oral Hygiene Practices for Reflux Sufferers:
- DO NOT Brush Immediately After Reflux: Acid softens enamel, making it vulnerable to abrasive brushing. Wait at least 30-60 minutes after a reflux episode or vomiting before brushing. This allows saliva to naturally neutralize the acid and begin remineralizing the enamel.
- Rinse Immediately: After a reflux episode, rinse your mouth thoroughly with plain water or, even better, with a fluoride mouthwash or a baking soda solution (1 teaspoon baking soda in 8 ounces of water). Baking soda is alkaline and helps neutralize acid quickly.
- Use Fluoride Toothpaste: Opt for a toothpaste containing fluoride to strengthen enamel. Your dentist might prescribe a high-fluoride toothpaste.
- Chew Sugar-Free Gum: Chewing sugar-free gum after meals or reflux episodes stimulates saliva flow, which helps neutralize acids and wash them away, promoting remineralization.
- Use a Soft-Bristled Toothbrush: To minimize abrasion on already compromised enamel.
-
Dietary Considerations:
- Limit Acidic Foods & Drinks: Reduce consumption of sodas, sports drinks, fruit juices (especially citrus), vinegar-based dressings, and excessively sour candies.
- Stay Hydrated: Drink plenty of plain water throughout the day.
Pro Tip: Consider creating a "reflux toolkit" for your bathroom: a bottle of fluoride rinse or a container of baking soda solution readily available for immediate use after an episode.
Prevention
Preventing acid reflux teeth involves a two-pronged strategy: preventing acid reflux itself and protecting your teeth from acid exposure even if reflux occurs.
1. Medical and Lifestyle Management of Acid Reflux:
- Identify and Avoid Trigger Foods: Common triggers include fatty or fried foods, spicy foods, citrus fruits, tomatoes, chocolate, peppermint, garlic, onions, caffeine, and alcohol. Keep a food diary to pinpoint your specific triggers.
- Eat Smaller, More Frequent Meals: Large meals can put pressure on the stomach and LES.
- Avoid Eating Close to Bedtime: Allow at least 2-3 hours between your last meal and lying down.
- Elevate Your Head During Sleep: Use a wedge pillow or elevate the head of your bed by 6-8 inches to allow gravity to keep stomach acid down.
- Maintain a Healthy Weight: Excess abdominal fat can put pressure on your stomach, forcing acid upward.
- Quit Smoking: Nicotine relaxes the LES, making reflux more likely.
- Limit Alcohol and Caffeine: Both can relax the LES and increase stomach acid production.
- Review Medications: Discuss with your doctor if any of your current medications (e.g., NSAIDs, certain blood pressure medications, muscle relaxants) might be contributing to reflux.
- Stress Management: Stress can exacerbate reflux symptoms for some individuals. Techniques like yoga, meditation, or deep breathing can be beneficial.
- Wear Loose Clothing: Tight clothing around the waist can put pressure on your abdomen.
2. Dental Protection Strategies:
- Do Not Brush Immediately After Reflux/Vomiting: This is paramount. Acid softens enamel, and brushing immediately can mechanically abrade the softened surface. Wait at least 30-60 minutes.
- Rinse Your Mouth: Immediately after reflux or vomiting, rinse thoroughly with plain water, a fluoride mouthwash, or an alkaline solution (like a teaspoon of baking soda in 8 ounces of water). This neutralizes the acid and helps wash it away.
- Use Fluoride Regularly:
- Fluoride Toothpaste: Use a toothpaste with fluoride twice daily.
- Fluoride Mouthwash: Incorporate a daily over-the-counter fluoride mouthwash.
- Professional Fluoride Treatments: Your dentist may recommend in-office fluoride varnish applications, especially if you have ongoing erosion.
- Prescription Fluoride: For severe cases, a prescription-strength fluoride toothpaste or gel may be advised.
- Chew Sugar-Free Gum: Chewing stimulates saliva flow, which is your mouth's natural defense against acid. Saliva neutralizes acids, washes away food particles, and contains minerals that help remineralize enamel.
- Maintain Excellent Oral Hygiene: Brush twice a day with a soft-bristled toothbrush and floss daily to prevent plaque buildup and reduce the risk of cavities in areas where enamel might be compromised.
- Limit Dietary Acids: While managing reflux, also be mindful of external acidic foods and drinks like soft drinks, sports drinks, fruit juices, and sour candies. When consumed, drink them quickly, use a straw to minimize tooth contact, and rinse with water afterward.
- Regular Dental Check-ups: Inform your dentist about any reflux symptoms. Regular examinations allow your dentist to detect early signs of erosion and intervene before significant damage occurs.
- Consider a Nightguard (if bruxism is present): If you grind or clench your teeth (bruxism), it can accelerate the wear on already acid-weakened enamel. A custom nightguard can protect your teeth.
Pro Tip: Think of saliva as your mouth's natural "antacid." Anything that promotes healthy saliva flow (hydration, chewing sugar-free gum, avoiding dry mouth) will offer additional protection against acid erosion.
Risks and Complications
Failing to address acid reflux teeth and the underlying acid reflux itself can lead to a cascade of dental and general health complications.
Dental Complications:
- Severe Enamel Erosion: The most direct complication. Unchecked, acid will progressively dissolve enamel, leading to significant tooth structure loss. This manifests as severe sensitivity, changes in tooth shape, and a noticeably shorter smile.
- Increased Risk of Cavities (Dental Caries): Even though erosion is not decay, the loss of protective enamel makes teeth highly susceptible to bacterial acid attacks. Once dentin is exposed, cavities can progress much faster, potentially leading to widespread decay.
- Tooth Sensitivity: Persistent and often extreme sensitivity to hot, cold, sweet, and acidic foods and drinks can significantly impair quality of life and make eating uncomfortable.
- Dental Abscess and Infection: If erosion and subsequent decay reach the pulp (nerve) of the tooth, it can cause severe pain, infection, and potentially a dental abscess, requiring root canal treatment or even extraction.
- Tooth Fractures and Chipping: Eroded teeth are weaker and more brittle, making them prone to fracturing or chipping, especially under normal chewing forces. This can lead to sharp edges, injury to soft tissues, and further dental issues.
- Occlusal Instability (Bite Problems): Significant tooth loss from erosion can alter your bite, leading to issues with chewing, jaw pain (TMJ disorders), and headaches. This can sometimes necessitate complex and expensive full-mouth rehabilitation.
- Loss of Aesthetic Appearance: Discolored, shortened, or misshapen teeth can severely impact your self-confidence and appearance.
- Compromised Existing Restorations: Acid reflux can erode the natural tooth structure around existing fillings, crowns, or veneers, leading to leakage, recurrent decay, and premature failure of these restorations.
- Extreme Calcium Buildup on Teeth (Calculus): While enamel erosion is the primary concern, in some cases, chronic changes in oral pH due to reflux can paradoxically lead to altered saliva composition and increased calcification in specific areas, contributing to extreme calcium buildup on teeth (hard calculus or tartar) in areas not directly exposed to erosive forces, further complicating oral hygiene. This is less common than erosion but can occur.
General Health Complications (from untreated reflux):
The dental complications are often a symptom of larger underlying issues. Unmanaged GERD can lead to:
- Esophagitis: Inflammation of the esophagus.
- Esophageal Ulcers: Open sores in the esophageal lining, which can bleed and cause pain.
- Esophageal Stricture: Narrowing of the esophagus due to scar tissue, making swallowing difficult.
- Barrett's Esophagus: A serious complication where the cells lining the esophagus change to resemble the lining of the intestine. This condition increases the risk of esophageal cancer.
- Respiratory Problems: Acid can be aspirated into the lungs, leading to chronic cough, asthma, bronchitis, or even aspiration pneumonia.
- Sleep Disturbances: Reflux symptoms can disrupt sleep, leading to fatigue and reduced quality of life.
These risks underscore the importance of early diagnosis and comprehensive management of both the dental damage and the underlying acid reflux condition.
Comparison Tables
Table 1: Dental Restoration Options for Acid Erosion
| Restoration Type | Extent of Erosion | Durability | Cost Range (Per Tooth) | Pros | Cons |
|---|---|---|---|---|---|
| Fluoride Therapy | Minor | Temporary | $30 - $70 | Strengthens enamel, reduces sensitivity, non-invasive | Does not replace lost structure, requires reapplication |
| Dental Bonding | Mild to Moderate | 5-10 years | $150 - $600 | Minimally invasive, tooth-colored, single visit, cost-effective | Less durable than porcelain, can stain/chip, not for heavy wear |
| Inlay/Onlay | Moderate (molars) | 10-15+ years | $600 - $1,200 | Durable, preserves more tooth than a crown, good aesthetics | Two visits, higher cost than fillings |
| Porcelain Veneers | Moderate to Severe | 10-15+ years | $800 - $2,500+ | Excellent aesthetics, durable, covers front surface, long-lasting | Invasive (enamel removal), irreversible, higher cost |
| Dental Crowns | Severe | 15-20+ years | $800 - $2,500+ | Maximum protection, restores severely damaged teeth, strong | More invasive (significant tooth reduction), multiple visits, highest cost |
Table 2: US Cost Breakdown & Insurance Coverage for Acid Reflux Dental Treatments
| Procedure Category | Average Cost Range (Without Insurance) | Est. Insurance Coverage (Typical) | Out-of-Pocket Cost (With Insurance) | Notes |
|---|---|---|---|---|
| Preventive Care | ||||
| Routine Exam & Cleaning | $75 - $200 | 80-100% | $0 - $40 | Crucial for early detection. |
| Fluoride Treatment | $30 - $70 | 80-100% | $0 - $15 | Often included with cleanings. |
| Basic Restorative | ||||
| Dental Bonding (1 surface) | $150 - $350 | 50-80% | $30 - $175 | For minor erosions. |
| Major Restorative | Subject to deductible & annual maximum ($1k-$2k common). | |||
| Inlay/Onlay (Porcelain) | $800 - $1,200 | 20-50% | $400 - $960 | Durable, covers chewing surfaces. |
| Veneer (Porcelain) | $1,000 - $2,500 | 20-50% (sometimes cosmetic) | $500 - $2,000 | Highly aesthetic, for visible teeth. |
| Dental Crown (Porcelain) | $1,200 - $2,500 | 20-50% | $600 - $2,000 | For severely damaged teeth, full coverage. |
| Emergency Care | ||||
| Emergency Exam | $75 - $150 | 50-80% | $15 - $75 | For acute pain or fractured tooth. |
| Total Full Mouth | $5,000 - $20,000+ | Varies greatly | Varies greatly | For extensive damage, often requires multiple procedures. |
Note: All insurance figures are estimates. Actual coverage depends on your specific plan's details, deductibles, co-pays, and annual maximums. Always confirm with your insurance provider.
Children / Pediatric Considerations
Acid reflux can significantly impact children's dental health, often with more severe and rapid consequences due to their thinner, less mineralized enamel. Recognizing signs of calcium deficiency in teeth from reflux is especially critical in pediatric patients.
Why Children Are More Vulnerable:
- Thinner Enamel: Primary (baby) teeth have thinner enamel than permanent teeth, making them more susceptible to acid erosion.
- Developing Teeth: Erosion on primary teeth can affect the development and eruption of underlying permanent teeth.
- Difficulty Communicating Symptoms: Young children may not articulate their reflux symptoms or dental discomfort clearly, leading to delayed diagnosis.
- Common in Infants: Infantile reflux (GER) is common and usually resolves on its own, but persistent or severe cases (GERD) can cause significant dental issues.
- Dietary Factors: Many common children's foods and drinks (fruit juices, sodas, sugary snacks) are highly acidic, compounding the problem.
Signs of Acid Erosion in Children:
- Tooth Sensitivity: A child might wince or pull away from cold drinks or certain foods.
- Yellowish or Translucent Teeth: Enamel loss exposes the dentin, making teeth look yellow or see-through at the edges.
- Rounded or Worn Edges: Especially on the incisors and molars.
- "Cupped" Surfaces: Distinct depressions on the biting surfaces of molars.
- Increased Cavities: Erosion weakens enamel, making teeth prone to decay.
- Changes in Tooth Shape/Size: Noticeable shortening or alterations to the teeth.
Pediatric Management Strategies:
- Early Dental Screening: Regular dental check-ups, starting from the first tooth's eruption (around 6 months), are vital. Pediatric dentists are trained to spot early signs of erosion.
- Medical Diagnosis and Management: If erosion is suspected, prompt referral to a pediatrician or pediatric gastroenterologist is crucial to diagnose and manage the underlying reflux. This may involve dietary changes, medication, or in rare cases, surgery.
- Fluoride Application:
- In-office Fluoride Varnishes: Regular applications by the dentist are highly effective at strengthening enamel.
- Fluoride Toothpaste: Using a pea-sized amount of fluoride toothpaste (for children over 3) or a "smear" (for children under 3) twice daily, with parental supervision to prevent swallowing.
- Prescription Fluoride: For severe cases, a pediatric dentist might prescribe a high-fluoride rinse or gel.
- Sealants: Dental sealants can be applied to the chewing surfaces of molars, protecting them from both acid erosion and decay.
- Dietary Counseling: Educating parents and children on limiting acidic drinks (sodas, juices, sports drinks) and choosing water or milk instead. Avoid sugary snacks.
- Proper Oral Hygiene After Reflux: Teach older children (and parents of younger ones) to rinse their mouth with water or a baking soda solution immediately after reflux or vomiting, and to wait 30-60 minutes before brushing.
- Restorative Care: For significant erosion, bonding or stainless steel crowns (on baby teeth) might be necessary to protect the teeth and maintain space for permanent teeth.
- Parental Awareness: Parents should be aware of reflux symptoms (frequent spitting up, refusing to eat, arching back during feeding, chronic cough, poor weight gain) and discuss them with their pediatrician.

Pro Tip: For infants and toddlers, wipe their gums and any erupted teeth gently with a soft, damp cloth after reflux episodes, before brushing later. This helps remove acid safely without abrading softened enamel.
Cost Breakdown
A dedicated cost breakdown reinforces the financial aspects discussed earlier, offering a clearer picture for patients in the US.
Average US Costs for Acid Reflux Teeth Treatments (Without Insurance):
| Service Category | Average Low Range | Average Mid Range | Average High Range |
|---|---|---|---|
| Preventive Care | |||
| Fluoride Treatment | $30 | $50 | $70 |
| Dental Cleaning | $75 | $120 | $200 |
| Minor Restorative | |||
| Dental Bonding | $150 | $350 | $600 |
| Moderate Restorative | |||
| Inlay/Onlay | $600 | $900 | $1,200 |
| Composite Veneer | $250 | $800 | $1,500 |
| Major Restorative | |||
| Porcelain Veneer | $800 | $1,600 | $2,500+ |
| Dental Crown | $800 | $1,700 | $2,500+ |
| Comprehensive | |||
| Full Mouth Rehab | $5,000 | $12,000 | $20,000+ |
These ranges represent individual tooth costs where applicable, in an average US dental practice. Specialist fees or complex cases can exceed these highs.
With vs. Without Insurance:
- Without Insurance: You are responsible for 100% of the listed costs. Many dentists offer a cash discount for upfront payment or in-house discount plans.
- With Insurance: Dental insurance plans typically categorize procedures:
- Preventive (e.g., fluoride, cleanings): Often covered at 80-100%, minimizing your out-of-pocket expense.
- Basic (e.g., bonding, some fillings): Often covered at 50-80% after your deductible.
- Major (e.g., crowns, veneers, inlays/onlays): Typically covered at 20-50% after your deductible, and subject to your annual maximum benefit (commonly $1,000 - $2,000). Once you hit this maximum, you pay 100% of additional costs for that year.
- Medical Insurance: Remember that the medical treatment for acid reflux (e.g., doctor visits, prescriptions, endoscopy, surgery) falls under your medical insurance, not dental.
Payment Plans and Financing Options:
- In-Office Payment Plans: Many dental practices offer interest-free payment plans, allowing you to pay for treatment in installments over several months.
- Third-Party Financing (e.g., CareCredit, LendingClub): These companies provide healthcare-specific credit cards or loans that can be used for dental work. They often have promotional periods with 0% interest if the balance is paid within a certain timeframe (e.g., 6, 12, 18 months).
- Personal Loans: Banks and credit unions offer personal loans that can cover larger dental expenses.
- Health Savings Accounts (HSAs) / Flexible Spending Accounts (FSAs): If you have an HSA or FSA through your employer, you can use these tax-advantaged accounts to pay for qualified dental expenses.
Cost-Saving Tips:
- Prioritize Prevention: The least expensive treatment is prevention. Managing reflux and adopting good oral hygiene significantly reduces the need for costly restorations.
- Don't Delay Treatment: Small erosions are cheaper to fix with bonding than extensive damage requiring crowns.
- Get Multiple Quotes: For major procedures, it's acceptable to seek a second opinion and cost estimate from another reputable dentist.
- Inquire About Discounts: Ask your dentist if they offer any discounts for cash payments, senior citizens, or military personnel.
- Maximize Insurance Benefits: Understand your plan's annual maximums and waiting periods. Plan major treatments strategically across calendar years if needed to maximize benefits.
Frequently Asked Questions
What are "acid reflux teeth" exactly?
Acid reflux teeth refers to the dental damage, primarily enamel erosion, that occurs when stomach acid repeatedly washes over your teeth. This acid, which is highly corrosive, dissolves the protective outer layer of your teeth (enamel), leading to sensitivity, changes in tooth appearance, and increased vulnerability to decay.
How quickly can acid reflux damage teeth?
The speed of damage varies greatly depending on the frequency, duration, and acidity of reflux episodes, as well as your saliva's buffering capacity. Some individuals might see noticeable changes within a few months to a year of consistent, severe reflux, while for others, it may take several years. Early detection by a dentist is common before you even notice symptoms.
Are there specific parts of the mouth most affected by acid reflux?
Yes, acid erosion from reflux often presents in characteristic patterns. It commonly affects the lingual (tongue-facing) surfaces of your upper front teeth and the occlusal (biting) surfaces of your back teeth. This is because these areas are typically in direct contact with the acid as it flows up from the esophagus.
Can acid reflux cause extreme calcium buildup on teeth?
While acid reflux primarily causes enamel erosion (loss of calcium/minerals from teeth), in some specific and less common scenarios, chronic changes in oral pH and saliva composition can paradoxically lead to increased calcification in certain areas, contributing to extreme calcium buildup on teeth (calculus or tartar). However, erosion remains the dominant and more concerning dental manifestation of reflux.
What are the main signs of calcium deficiency in teeth due to acid erosion?
The primary signs of calcium deficiency in teeth from acid erosion include increased tooth sensitivity to hot, cold, or sweets; teeth appearing more yellow or translucent as enamel thins; smooth, shiny, or "scooped out" surfaces on teeth; and the appearance of fillings that seem to "stand proud" above the eroded tooth structure.
Is dental treatment for acid reflux teeth painful?
The pain level depends on the severity of the erosion and the type of treatment. Minor treatments like fluoride applications are painless. Dental bonding, veneers, or crowns typically involve local anesthesia to numb the area, so you should feel minimal to no pain during the procedure itself, though some post-treatment sensitivity is common. Your dentist will ensure your comfort.
How much does it cost to fix acid reflux teeth?
The cost varies significantly. Minor erosion treated with fluoride applications or dental bonding can range from $30 to $600 per tooth. More severe damage requiring veneers or crowns can cost $800 to $2,500+ per tooth. Extensive damage across multiple teeth can lead to total costs ranging from $5,000 to $20,000 or more for full mouth rehabilitation.
Does dental insurance cover the treatment for acid reflux teeth?
Dental insurance usually covers a portion of restorative treatments. Preventive care like fluoride is often covered 80-100%. Basic procedures like bonding might be covered 50-80%. Major procedures like crowns or veneers are typically covered 20-50%, often after a deductible and up to an annual maximum benefit (e.g., $1,000-$2,000). Always check with your specific insurance provider.
Can I brush my teeth immediately after an acid reflux episode or vomiting?
No, it's crucial not to brush immediately. Stomach acid softens your tooth enamel, making it highly susceptible to abrasion. Brushing too soon can actually scrub away softened enamel, worsening the erosion. Instead, rinse your mouth thoroughly with plain water, a fluoride mouthwash, or a baking soda solution (1 teaspoon baking soda in 8 ounces of water) and wait at least 30-60 minutes before brushing gently.
What can I do to prevent further dental damage from acid reflux?
Prevention involves managing your acid reflux medically and adopting specific oral hygiene habits. Avoid trigger foods, eat smaller meals, don't eat close to bedtime, and elevate your head when sleeping. For your teeth, use fluoride toothpaste and mouthwash, rinse your mouth with water or baking soda after reflux, wait to brush, and chew sugar-free gum to stimulate protective saliva. Regular dental check-ups are also essential.
When to See a Dentist
Given the silent and insidious nature of acid reflux's impact on dental health, knowing when to seek professional dental care is crucial.
Red Flags That Need Prompt Attention:
- Persistent Tooth Sensitivity: If you experience ongoing sharp or aching pain when consuming hot, cold, sweet, or acidic foods/drinks, or even with cold air, this is a strong indicator of enamel erosion and exposed dentin.
- Visible Changes in Tooth Appearance: Noticeable yellowing or translucency of teeth, smooth and shiny tooth surfaces (especially on the tongue-side of upper front teeth), "scooped out" depressions on biting surfaces, or teeth that appear shorter or more rounded at the edges.
- New or Worsening Cracks/Chips: Eroded teeth are weaker. If you start experiencing frequent chipping or cracking, it's a sign of significant structural compromise.
- Fillings That Seem to "Stick Up": If old fillings appear to be elevated above the surrounding tooth structure, it indicates that the natural tooth enamel has eroded around the restoration.
- Constant Sour or Acidic Taste: While a medical symptom, a persistent sour taste in your mouth could be a sign of ongoing reflux, directly impacting your teeth.
- Painful Chewing or Bite Changes: If significant erosion has occurred, it can alter your bite, leading to discomfort or difficulty chewing.
When to Schedule a Routine Check-up (and mention reflux):
- Every Six Months: Even if you don't have overt symptoms, regular dental check-ups are vital. Your dentist is often the first healthcare provider to identify early signs of acid erosion, even before you realize you have reflux.
- If You've Been Diagnosed with GERD/LPR: If a medical doctor has diagnosed you with acid reflux, inform your dentist immediately, even if your teeth currently look fine. This allows them to proactively monitor for erosion and recommend preventive measures.
- Considering Lifestyle Changes for Reflux: If you are actively trying to manage your reflux through diet and lifestyle, a dental check-up can help assess your baseline and monitor the effectiveness of your efforts on your oral health.
Emergency vs. Scheduled Appointment Guidance:
- Emergency (Call your dentist immediately): Severe, sudden tooth pain that doesn't subside; a fractured tooth with sharp edges; signs of a dental infection (swelling, fever, severe throbbing pain). These could be complications arising from severely eroded teeth.
- Scheduled Appointment (Book soon): Persistent sensitivity without acute pain; subtle changes in tooth color or shape; chronic sour taste; or if you've recently been diagnosed with acid reflux.
Never underestimate the silent damage acid reflux can inflict. Your dentist is a key partner in preserving your smile and can even be a first line of defense in identifying underlying health issues.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

What Are Calcium Deposits on Teeth
Are you one of the millions of Americans who notices a stubborn, yellowish buildup on your teeth despite regular brushing? You're likely experiencing what many refer to as "calcium deposits on teeth." This common dental concern, medically known as dental calculus or tartar, affects a vast ma
February 23, 2026

Calcium Good for Teeth: Complete Guide
More than 99% of your body's calcium resides in your bones and teeth, making it an undeniable cornerstone of skeletal and oral health. But did you know that an estimated 42% of American adults don't get enough calcium from their diet? This staggering statistic underscores a critical question
February 23, 2026

What Do Bulimia Teeth Look Like
"Bulimia teeth" refers to the specific and often severe damage that the self-induced vomiting characteristic of bulimia nervosa inflicts on a person's oral health. It's a critical issue, affecting approximately 1.5% of women and 0.5% of men in the US at some point in their lives, with many more
February 23, 2026

Erosion in Teeth: Complete Guide
Erosion in Teeth: Complete Guide
February 23, 2026