Leukoplakia vs Thrush: Complete Comparison Guide
Key Takeaways
- Imagine finding a strange white patch in your mouth. Your immediate thought might be worry, and rightfully so. Oral lesions can range from harmless irritations to early indicators of serious health issues, including oral cancer. Distinguishing between conditions like leukoplakia and thrush is cr
Leukoplakia vs Thrush: Complete Comparison Guide
Imagine finding a strange white patch in your mouth. Your immediate thought might be worry, and rightfully so. Oral lesions can range from harmless irritations to early indicators of serious health issues, including oral cancer. Distinguishing between conditions like leukoplakia and thrush is critical for your health and peace of mind. While both can manifest as white patches in the mouth, their origins, implications, and treatments are vastly different. Misdiagnosis or delayed treatment for either condition, particularly leukoplakia vs thrush, can have significant consequences. This comprehensive guide from SmilePedia.net aims to provide a definitive comparison, arming you with the knowledge to understand these conditions, recognize their mouth cancer signs, and seek appropriate care.

We will delve into the distinct characteristics, underlying causes, symptoms, and treatment approaches for both leukoplakia and thrush. Understanding these differences is not just academic; it's a vital step in maintaining optimal oral health and ensuring timely intervention should a more serious condition arise.
Key Takeaways:
- Leukoplakia is a non-scrapable, potentially precancerous white patch, often linked to tobacco and alcohol use, with an estimated 5-17% risk of malignant transformation.
- Oral Thrush (candidiasis) is a scrapable, creamy-white fungal infection, common in infants, denture wearers, and individuals with weakened immune systems.
- Diagnosis is crucial: While thrush is typically diagnosed clinically, leukoplakia often requires a biopsy for definitive diagnosis and to rule out malignancy. A biopsy can cost $200-$800 without insurance.
- Treatment for Thrush usually involves antifungal medications (e.g., nystatin rinse, fluconazole tablets) and lifestyle changes, with symptoms often improving within 1-2 weeks.
- Leukoplakia management may involve lifestyle modification (cessation of tobacco/alcohol), surgical removal (costing $500-$3,000+), laser therapy, or cryotherapy, followed by lifelong monitoring.
- Regular dental check-ups (at least annually, ideally every six months) are vital for early detection of both conditions and for proactive oral cancer screening.
- Persistent oral white patches that do not resolve within two weeks should always be evaluated by a dental professional.
What It Is / Overview
Understanding the fundamental nature of leukoplakia and thrush is the first step in differentiating them. While both manifest as white patches in the mouth, their biological underpinnings are entirely distinct.
Leukoplakia: A Potentially Precancerous Oral Lesion
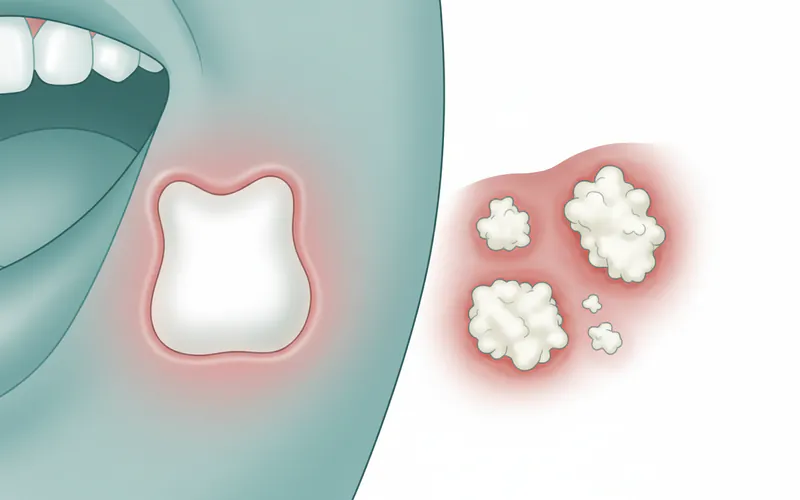
Leukoplakia (pronounced loo-koh-PLAY-kee-uh) is defined as a white patch or plaque on the oral mucous membrane that cannot be scraped off and cannot be characterized as any other diagnosable disease. It is a diagnosis of exclusion, meaning other more common white lesions must first be ruled out. The most significant aspect of leukoplakia is its precancerous potential. While not cancerous itself, it represents an abnormal growth of cells that has a recognized risk of developing into squamous cell carcinoma, the most common type of oral cancer.
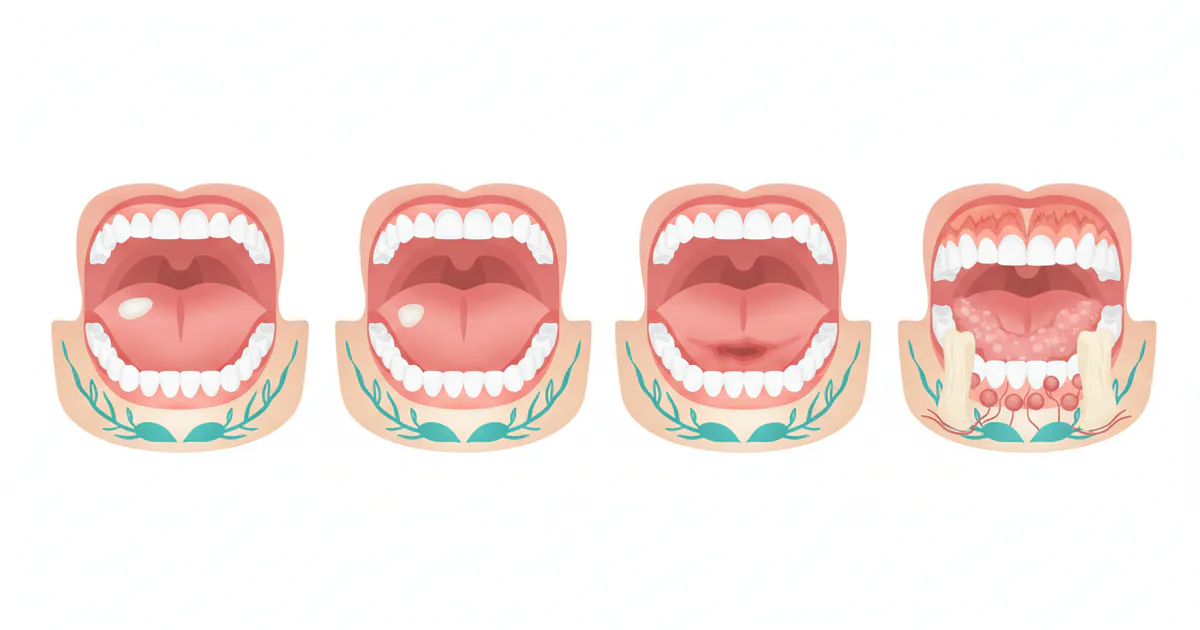
The patches typically appear as flat or slightly raised areas, ranging in color from milky white to grayish. They can be found anywhere in the mouth, but are most commonly seen on the tongue, the inside of the cheeks (buccal mucosa), and the floor of the mouth. The texture can vary from smooth to wrinkled or even nodular. Leukoplakia is more prevalent in older adults, particularly men, and its incidence increases with age.
Oral Thrush (Oral Candidiasis): A Fungal Infection
Oral Thrush, also known as oral candidiasis, is a fungal infection of the mouth caused by an overgrowth of Candida albicans, a yeast that is naturally present in small amounts in most people's mouths and digestive tracts. When conditions are favorable, Candida can multiply rapidly, leading to noticeable symptoms.
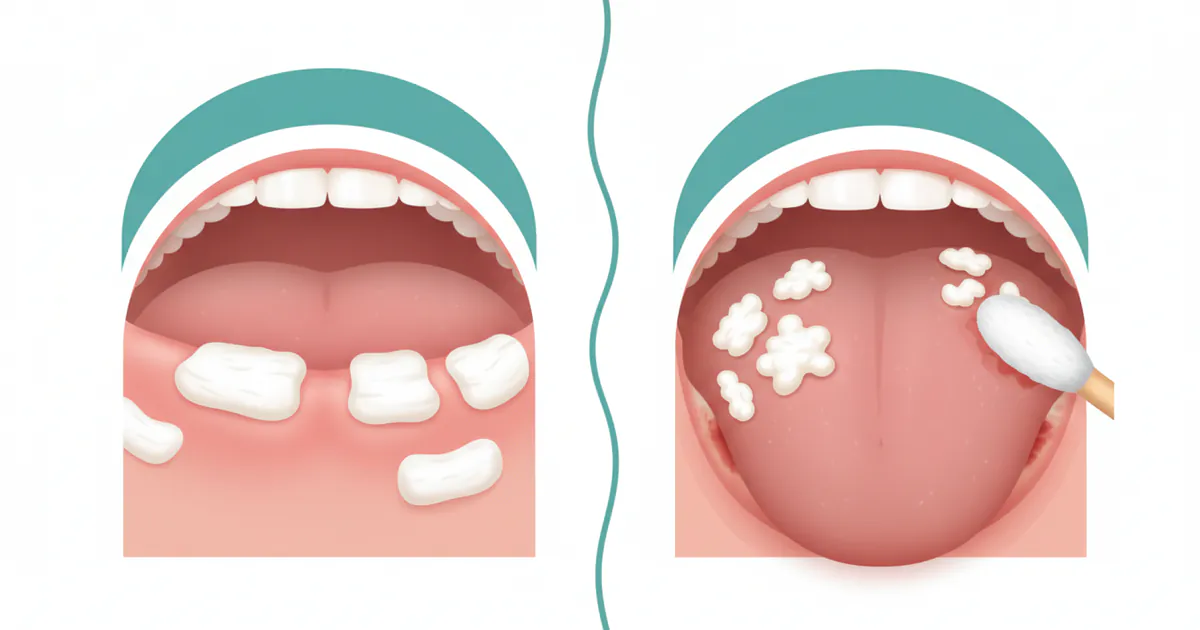
Thrush typically appears as creamy white lesions, often described as resembling cottage cheese, on the tongue, inner cheeks, roof of the mouth, gums, and tonsils. Unlike leukoplakia, these lesions can usually be scraped off, revealing red, inflamed, and sometimes bleeding tissue underneath. Thrush is a common condition, particularly in infants, the elderly, individuals with compromised immune systems, and those using certain medications. It is generally not considered a precancerous condition.
Types / Variations
Both leukoplakia and thrush present in several forms, each with its own characteristics and clinical implications.
Types of Leukoplakia
Leukoplakia is primarily categorized based on its clinical appearance, which can correlate with its malignant potential.
- Homogenous Leukoplakia: This is the most common and generally considered the least severe form. It presents as a uniformly white, relatively thin, non-elevated plaque with a smooth or finely wrinkled surface. These lesions have a lower, but still present, risk of malignant transformation.
- Non-homogenous Leukoplakia: This category includes lesions that are irregular in appearance and are associated with a higher risk of malignant transformation.
- Verrucous Leukoplakia: Characterized by a white, wart-like, corrugated, or shaggy surface. It has a significantly higher risk of malignant transformation than homogenous leukoplakia.
- Nodular Leukoplakia: Presents as white patches with small, rounded, or projecting nodules. This form also carries a higher risk.
- Erythroleukoplakia (Speckled Leukoplakia): This is a mixed red and white lesion, often considered the most concerning type. The red areas (erythroplakia) indicate significant epithelial dysplasia (abnormal cell growth) and have the highest malignant potential, often exceeding 50% likelihood of developing into invasive carcinoma. This is a critical mouth cancer sign.
- Proliferative Verrucous Leukoplakia (PVL): A rare but highly aggressive form characterized by multifocal, recurrent, and progressive white lesions. PVL has a very high rate of malignant transformation and can often develop into verrucous or squamous cell carcinoma. It tends to spread, involve multiple oral sites, and is resistant to conventional treatments.
Types of Oral Thrush (Oral Candidiasis)
Oral thrush also has various clinical presentations, often reflecting the underlying cause or location.
- Pseudomembranous Candidiasis (Classic Thrush): This is the most recognized form, characterized by the creamy white, cottage cheese-like patches that can be scraped off. It's common in infants, immunocompromised individuals, and those on antibiotics.
- Erythematous Candidiasis (Atrophic Candidiasis): Appears as red, inflamed areas, often without prominent white patches. It can be caused by antibiotic use, steroid inhalers, or ill-fitting dentures. The tongue may appear red and "bald" due to loss of papillae.
- Angular Cheilitis: This form of candidiasis affects the corners of the mouth, causing redness, cracking, and soreness. It's often seen in people with dentures, those who frequently lick their lips, or individuals with nutritional deficiencies.
- Denture Stomatitis: Characterized by redness and inflammation under a denture, typically on the palate. It's caused by Candida growth under the denture, often due to poor denture hygiene or continuous wear. White patches may or may not be present.
- Chronic Hyperplastic Candidiasis: A rarer form that presents as persistent, non-scrapable white patches, sometimes resembling leukoplakia. These lesions are more adherent and may have a speckled red appearance. A biopsy may be required to differentiate it from leukoplakia due to its fixed nature, although it is still a fungal infection.
Causes / Why It Happens
The root causes for leukoplakia and thrush are vastly different, which is a key factor in their diagnosis and management.
Causes of Leukoplakia
Leukoplakia is primarily associated with chronic irritation and exposure to carcinogens.
- Tobacco Use: This is by far the most significant risk factor. Smoking cigarettes, cigars, and pipes, as well as using smokeless tobacco (chewing tobacco, snuff), dramatically increases the risk. The chemicals in tobacco irritate the oral tissues and promote abnormal cell growth.
- Alcohol Consumption: Heavy and chronic alcohol use is another major contributing factor, especially when combined with tobacco. Alcohol can act as a solvent, allowing carcinogens to penetrate tissues more easily.
- Chronic Irritation: While less common than tobacco/alcohol, persistent irritation from rough teeth, ill-fitting dentures, or chronic cheek biting can sometimes contribute to localized leukoplakia. However, the ADA emphasizes that the majority of leukoplakia cases are linked to chemical irritants rather than purely mechanical ones.
- Human Papillomavirus (HPV): Certain high-risk strains of HPV (particularly HPV-16 and HPV-18) are known to be involved in a subset of oral cancers and can also be associated with some forms of leukoplakia, especially those occurring on the tonsils and base of the tongue.
- Sun Exposure: For leukoplakia on the lips (actinic cheilitis), prolonged exposure to ultraviolet (UV) radiation from the sun is a primary cause.
- Other Factors: Nutritional deficiencies (e.g., Vitamin A or B complex), genetic predisposition, and immune suppression may play a minor role, though they are not considered primary causes.
Causes of Oral Thrush
Thrush occurs when the Candida yeast, normally present in the mouth, overgrows. This usually happens when the balance of microorganisms in the mouth is disrupted or the body's immune defenses are weakened.
- Weakened Immune System: This is the most common underlying cause. Conditions that suppress the immune system include:
- HIV/AIDS: Individuals with HIV/AIDS are highly susceptible to recurrent oral thrush.
- Cancer: Chemotherapy and radiation therapy can severely compromise the immune system.
- Organ Transplants: Immunosuppressant drugs used to prevent organ rejection.
- Uncontrolled Diabetes: High sugar levels in saliva can promote Candida growth.
- Medications:
- Antibiotics: Broad-spectrum antibiotics kill beneficial bacteria in the mouth, allowing Candida to proliferate.
- Corticosteroids: Inhaled corticosteroids for asthma (e.g., fluticasone, budesonide) can suppress local immune responses in the mouth. Oral steroids also increase risk.
- Immunosuppressants: As mentioned above, for transplant patients or autoimmune conditions.
- Dentures: Ill-fitting or improperly cleaned dentures create moist, warm environments conducive to Candida growth.
- Dry Mouth (Xerostomia): Reduced saliva flow, often a side effect of medications or medical conditions, removes the natural cleansing action of saliva, allowing yeast to flourish.
- Infancy and Old Age: Infants have underdeveloped immune systems, and the elderly often have weakened immunity, chronic health conditions, or take multiple medications.
- Poor Oral Hygiene: Inadequate brushing and flossing can contribute to an environment where Candida can thrive.
Signs and Symptoms
Recognizing the distinct signs and symptoms is crucial for early detection and proper differentiation between leukoplakia and thrush.
Signs and Symptoms of Leukoplakia
Leukoplakia typically presents as a persistent lesion that may not cause pain initially, making early detection challenging without regular dental check-ups.
- Appearance: White or grayish patches on the tongue, gums, inner cheeks, or floor of the mouth. The color can be uniform or speckled.
- Texture: Can be flat, slightly raised, thickened, hardened, rough, wrinkled, or even nodular.
- Scrapability: Cannot be scraped off with a tongue depressor or toothbrush. This is a primary diagnostic differentiator.
- Sensation: Usually painless and asymptomatic in its early stages. Some individuals may report a slight burning sensation or discomfort, especially if the lesion is irritated.
- Persistence: The patches are persistent and do not disappear on their own within a couple of weeks.
- Location: Most commonly found on the lateral borders of the tongue, the floor of the mouth, the ventral surface of the tongue, and the soft palate.
Signs and Symptoms of Oral Thrush
Oral thrush, being an infection, often presents with more acute symptoms and a distinct appearance.
- Appearance: Creamy white, slightly raised lesions or patches on the tongue, inner cheeks, roof of the mouth, gums, and tonsils.
- Scrapability: Can typically be scraped off, revealing red, inflamed, and sometimes mildly bleeding tissue underneath.
- Sensation: May cause a cottony feeling in the mouth, soreness, or burning.
- Taste: Altered sense of taste or loss of taste.
- Eating/Swallowing: Difficulty or pain when eating or swallowing (dysphagia), especially if the infection extends to the esophagus.
- Cracked Corners of Mouth: Angular cheilitis (redness and cracking at the corners of the mouth) may accompany oral thrush.
- Bleeding: Minor bleeding can occur when the lesions are scraped or during vigorous brushing.
- Infants: Fussiness, difficulty feeding, and sometimes diaper rash (due to Candida spread) can be signs in babies.
Treatment Options
The treatment strategies for leukoplakia and thrush are fundamentally different, reflecting their distinct etiologies.
Treatment Options for Leukoplakia
Treatment for leukoplakia focuses on eliminating risk factors, removing the lesion, and preventing malignant transformation. The approach depends on the size, location, and severity of the lesion, as well as the presence of dysplasia (abnormal cells).
-
Lifestyle Modifications (First Line of Defense):
- Tobacco Cessation: For tobacco users, stopping all forms of tobacco is paramount. This can lead to the regression of homogenous leukoplakia in a significant number of cases.
- Alcohol Reduction/Cessation: Limiting or eliminating alcohol consumption, especially in combination with tobacco, is crucial.
- Sun Protection: For lip leukoplakia, using lip balm with SPF and avoiding prolonged sun exposure is important. Pro Tip: Your dentist can provide resources and referrals for tobacco cessation programs, which significantly improve your chances of quitting.
-
Surgical Excision: This is often the preferred method for definitive diagnosis and treatment, especially for lesions with moderate to severe dysplasia or those that persist after risk factor elimination.
- Traditional Scalpel Excision: The lesion is surgically cut out using a scalpel. This allows for clear margins and thorough histopathological analysis.
- Laser Ablation/Excision: Using a CO2 laser to vaporize or cut away the lesion. Offers precision, reduced bleeding, and potentially faster healing.
- Cryotherapy: Freezing the lesion with liquid nitrogen to destroy the abnormal cells.
- Electrocautery: Using an electric current to burn off the lesion.
- Pros of Surgical Removal: Provides a tissue sample for biopsy, high success rate for localized lesions.
- Cons: Potential for scarring, pain, swelling, and possible recurrence if margins are not clear.
- Cost: Varies significantly based on method and extent. Simple excisions can range from $500 to $1,500, while complex laser ablation or cryotherapy might be $1,500 to $3,000 or more. These costs typically do not include the biopsy.
-
Photodynamic Therapy (PDT): Involves administering a photosensitizing drug (e.g., aminolevulinic acid) which is absorbed by abnormal cells. The area is then exposed to a specific wavelength of light, activating the drug and selectively destroying the lesional cells.
- Pros: Minimally invasive, preserves surrounding healthy tissue, good for larger or multifocal lesions.
- Cons: Can cause photosensitivity, requires specialized equipment, potentially multiple sessions.
- Cost: PDT can be quite expensive, ranging from $1,000 to $5,000 per session, and may require multiple sessions.
-
Medications (Less Common, Often Adjunctive or Experimental):
- Retinoids (Vitamin A derivatives): Topical or systemic retinoids (e.g., tretinoin, isotretinoin) have shown some efficacy in reducing lesion size or preventing recurrence, but are often associated with side effects and have variable long-term success. They are generally not a first-line treatment.
- Beta-carotene: Antioxidant supplements are sometimes explored, but with limited conclusive evidence for direct treatment of leukoplakia.
-
Regular Monitoring: For small, homogenous lesions with no dysplasia, or in cases where complete removal is challenging, a "watch and wait" approach with very frequent follow-ups (every 3-6 months) may be chosen. This involves clinical examination and possibly repeat biopsies if changes are observed. The ADA emphasizes the importance of lifelong monitoring for all patients diagnosed with leukoplakia due to the risk of recurrence and new lesion formation.
Treatment Options for Oral Thrush
Treatment for oral thrush focuses on eliminating the Candida overgrowth and addressing the underlying predisposing factors.
-
Antifungal Medications (Primary Treatment):
- Topical Antifungals:
- Nystatin: Available as a mouth rinse (swish and swallow) or lozenges. Typically used several times a day for 7-14 days. Cost: Generic nystatin rinse can be $10-$30.
- Clotrimazole: Available as lozenges (troches) that dissolve slowly in the mouth, delivering the antifungal directly to the affected areas. Used 3-5 times a day for 7-14 days. Cost: Generic clotrimazole troches can be $20-$50.
- Systemic Antifungals:
- Fluconazole (Diflucan): An oral tablet taken once daily for 7-14 days. Often prescribed for more severe cases, when topical treatments are ineffective, or for immunocompromised individuals.
- Itraconazole, Posaconazole, Caspofungin: Other systemic antifungals used for resistant or widespread infections, often in hospital settings.
- Pros of Antifungals: Highly effective in clearing the infection, relatively quick relief of symptoms.
- Cons: Potential side effects (nausea, headache, liver issues for systemic drugs), drug interactions, recurrence if underlying cause isn't addressed.
- Cost: Generic fluconazole can range from $15-$100 for a course, depending on dosage and pharmacy.
- Topical Antifungals:
-
Oral Hygiene Improvements:
- Brushing and Flossing: Maintaining diligent oral hygiene helps reduce the fungal load.
- Denture Care: If you wear dentures, they must be removed nightly, thoroughly cleaned with a brush, and soaked in an antifungal or antiseptic solution (e.g., chlorhexidine or diluted bleach) overnight. Old dentures that harbor Candida may need to be replaced.
- Rinsing After Inhalers: If using corticosteroid inhalers, rinse your mouth thoroughly with water after each use to prevent residue from settling and promoting Candida growth.
-
Addressing Underlying Causes:
- Diabetes Management: Controlling blood sugar levels can significantly reduce the risk and recurrence of thrush.
- Immune System Support: For individuals with HIV/AIDS or cancer, managing their primary condition is key.
- Medication Review: Discuss with your doctor if any current medications might be contributing to dry mouth or immune suppression, and explore alternatives if possible.
Step-by-Step Process
Here's what you can expect during the diagnosis and treatment process for oral white lesions.
Diagnostic Pathway for Oral White Lesions
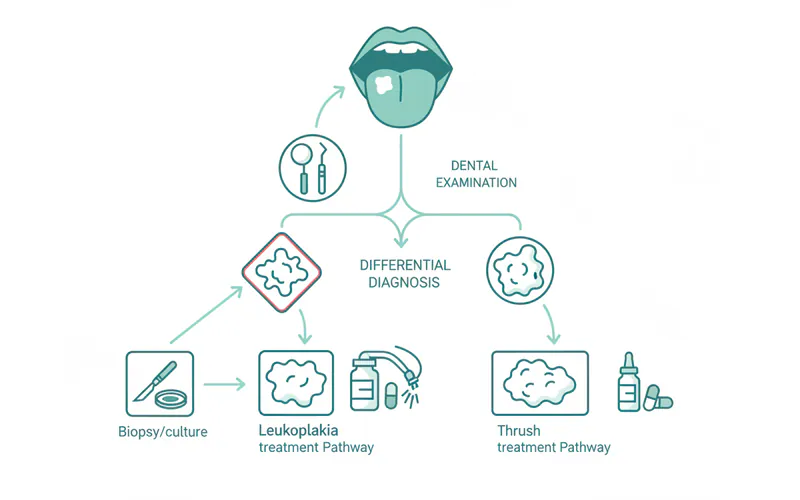
- Initial Dental Examination: Your dentist will visually inspect your mouth, checking for any white patches, redness, or other abnormalities. They will ask about your medical history, medications, and lifestyle habits (tobacco, alcohol).
- Palpation: The dentist will gently feel the lesion and surrounding tissues to check for any induration (hardening) or tenderness.
- Attempted Scraping: A key step for differentiation. The dentist will attempt to gently scrape the white patch with a tongue depressor or gauze.
- If it scrapes off: Highly suggestive of oral thrush or other removable deposits (e.g., food debris, materia alba). The scraped material might be sent for a fungal culture to confirm Candida presence.
- If it does NOT scrape off: Highly suggestive of leukoplakia or another fixed white lesion.
- Differential Diagnosis: Based on the clinical findings, your dentist will consider several possibilities, including leukoplakia, thrush, lichen planus, hyperkeratosis, or frictional keratosis.
- Biopsy (for non-scrapable lesions): If the lesion cannot be scraped off, or if it has characteristics suspicious of dysplasia or malignancy (e.g., erythroplakia, nodular texture, rapid growth), a biopsy is mandatory.
- Incisional Biopsy: A small portion of the suspicious tissue is removed for microscopic examination.
- Excisional Biopsy: The entire lesion is removed, along with a margin of healthy tissue, if it is small enough.
- The tissue sample is sent to an oral pathologist who examines it under a microscope to determine the precise diagnosis and rule out or confirm cancer.
- Pro Tip: Do not delay a recommended biopsy. Early detection of oral cancer significantly improves treatment outcomes and survival rates.
- Fungal Culture/Smear (for scrapable lesions): If thrush is suspected, a sample of the white material can be cultured in a lab to confirm Candida growth and identify the specific species. This is not always necessary as clinical diagnosis is often sufficient.

Step-by-Step Treatment for Leukoplakia (Post-Biopsy)
- Biopsy and Pathology Report: Once the biopsy results are back, confirming leukoplakia and indicating the presence (or absence) and grade of dysplasia, the definitive treatment plan is formulated.
- Risk Factor Elimination: Reinforce and guide the patient on strict tobacco and alcohol cessation. This is often the first step even before biopsy for homogenous lesions.
- Lesion Removal (if indicated):
- For lesions with dysplasia or those resistant to lifestyle changes, surgical excision (scalpel, laser, cryotherapy) is performed in a dental office or oral surgery clinic.
- The procedure is done under local anesthesia.
- Post-procedure instructions include pain management, wound care, and dietary recommendations.
- Follow-up and Monitoring: This is a lifelong commitment.
- Initial follow-up within 1-2 weeks to check healing.
- Regular follow-up examinations every 3-6 months for at least 5 years, and then annually, are crucial to monitor for recurrence or the development of new lesions.
Step-by-Step Treatment for Oral Thrush
- Clinical Diagnosis and Prescription: After a clinical diagnosis of thrush, your dentist or doctor will prescribe an appropriate antifungal medication.
- Medication Administration:
- Topical: If prescribed a rinse (e.g., nystatin), you will be instructed to swish it around your mouth for a specified time (e.g., 2 minutes) and then swallow it (especially important if the infection extends to the throat). For lozenges, allow them to dissolve slowly.
- Systemic: Oral tablets (e.g., fluconazole) are taken as directed.
- Improve Oral Hygiene: Implement enhanced oral hygiene practices:
- Brush teeth and tongue thoroughly.
- Clean dentures diligently, soaking them in appropriate solutions.
- Rinse mouth after using steroid inhalers.
- Address Underlying Factors: Work with your healthcare provider to manage conditions like diabetes, review medications, and bolster immune health.
- Monitoring and Follow-up: Symptoms typically improve within a few days, and the infection usually clears within 1-2 weeks. A follow-up appointment may be scheduled to ensure complete resolution and discuss long-term prevention strategies.
Cost and Insurance
Understanding the financial implications of diagnosis and treatment for these conditions in the US is important for planning your care.
Cost of Leukoplakia Diagnosis and Treatment
The costs associated with leukoplakia are primarily related to diagnostic biopsies and potential surgical removal.
- Initial Dental Exam: $50 - $150 (often covered by dental insurance).
- Biopsy (Incisional/Excisional):
- Without insurance: $200 - $800 (this covers the procedure by the dentist/oral surgeon and the pathology lab fee).
- With insurance: Dental insurance may cover a portion (e.g., 50-80% after deductible) as it's a diagnostic procedure. Medical insurance might cover it if referred by a physician and deemed medically necessary. Your out-of-pocket could range from $50 - $300.
- Surgical Removal (Post-biopsy):
- Scalpel Excision: $500 - $1,500 (simple lesion).
- Laser Ablation/Excision: $1,500 - $3,000+ (depending on size and complexity).
- Cryotherapy/Electrocautery: Similar to scalpel excision, $500 - $1,500.
- Photodynamic Therapy (PDT): $1,000 - $5,000 per session.
- Insurance Coverage: Surgical removal of precancerous lesions is often covered by medical insurance (as it prevents a more serious medical condition) or by a combination of medical and dental insurance. Patients should confirm coverage and potential out-of-pocket costs (deductibles, co-pays, co-insurance) with their providers.
- Follow-up Appointments: $50 - $200 per visit for clinical examinations. These are crucial and generally covered by dental insurance.
Cost of Oral Thrush Diagnosis and Treatment
Thrush treatment is generally less expensive, mainly involving the cost of antifungal medications and dental/medical visits.
- Initial Dental/Medical Exam: $50 - $150 (covered by dental or medical insurance).
- Fungal Culture/Smear: $50 - $150 (often covered by medical insurance if necessary).
- Antifungal Medications:
- Topical (Nystatin rinse, Clotrimazole troches): Generic forms typically cost $10 - $50 for a full course without insurance.
- Systemic (Fluconazole tablets): Generic fluconazole can range from $15 - $100 for a typical 7-14 day course without insurance. Brand-name drugs will be significantly higher.
- Insurance Coverage: Most prescription medications for thrush are covered by prescription drug plans associated with medical insurance, with co-pays ranging from $5 - $50 depending on the plan and whether generics are used.
Comparison Table: Estimated US Costs
| Service / Condition | Without Insurance (Avg. Range) | With Insurance (Avg. Out-of-Pocket) | Notes |
|---|---|---|---|
| Leukoplakia | |||
| Initial Exam | $50 - $150 | $10 - $50 | Often covered by dental or medical. |
| Oral Biopsy (Procedure + Path) | $200 - $800 | $50 - $300 | Critical for diagnosis, may be covered by medical. |
| Surgical Excision (Scalpel) | $500 - $1,500 | $100 - $500 | Covered by medical or dental/medical combo. |
| Laser Ablation / Cryotherapy | $1,500 - $3,000+ | $300 - $1,000+ | More advanced procedures. |
| Photodynamic Therapy (per session) | $1,000 - $5,000 | $500 - $2,000+ | Often less common, may require multiple sessions. |
| Follow-up Visits | $50 - $200 (per visit) | $10 - $50 (per visit) | Regular monitoring is crucial and ongoing. |
| Oral Thrush | |||
| Initial Exam | $50 - $150 | $10 - $50 | Often covered by dental or medical. |
| Fungal Culture (if needed) | $50 - $150 | $10 - $30 | Generally covered by medical. |
| Topical Antifungal Rx (e.g., Nystatin) | $10 - $50 | $5 - $20 | Generics are widely available and affordable. |
| Systemic Antifungal Rx (e.g., Fluconazole) | $15 - $100 | $5 - $50 | Generics are widely available and affordable. |
Recovery and Aftercare
Proper recovery and aftercare are vital for healing, preventing recurrence, and maintaining long-term oral health.
Recovery and Aftercare for Leukoplakia (Post-Treatment)
Recovery following surgical removal of leukoplakia generally involves managing discomfort and ensuring proper healing.
- Pain Management: Over-the-counter pain relievers (e.g., ibuprofen, acetaminophen) are usually sufficient. For more extensive surgeries, prescription pain medication may be provided for a few days.
- Oral Hygiene: Gentle brushing and rinsing with a mild saltwater solution (1/2 teaspoon salt in 8 ounces of warm water) can help keep the surgical site clean and promote healing. Avoid strong mouthwashes that contain alcohol.
- Diet: Stick to soft, bland foods for a few days to avoid irritating the healing tissue. Avoid spicy, acidic, or very hot foods.
- Avoid Irritants: Strictly avoid tobacco products, alcohol, and any other known irritants during the healing phase. This cessation should ideally be permanent.
- Follow-up Appointments: Adhere strictly to the schedule of follow-up visits with your oral surgeon or dentist. These visits are critical to monitor healing, check for complications, and screen for recurrence or new lesions.
- Lifelong Monitoring: Even after successful removal, patients with a history of leukoplakia are at an increased risk for developing new lesions or oral cancer. Regular, lifelong dental check-ups (every 3-6 months) are paramount, as recommended by the ADA.
Recovery and Aftercare for Oral Thrush
Recovery from oral thrush is usually straightforward once antifungal treatment is initiated and underlying causes are addressed.
- Complete Medication Course: It's crucial to finish the entire course of antifungal medication, even if symptoms improve quickly, to prevent recurrence.
- Enhanced Oral Hygiene: Continue diligent oral hygiene practices:
- Brush twice daily with a soft toothbrush, including the tongue.
- Floss daily.
- If using steroid inhalers, rinse your mouth thoroughly with water after each use.
- Clean dentures daily and soak them appropriately. Replace old or ill-fitting dentures.
- Address Predisposing Factors: Work with your healthcare provider to manage conditions like diabetes, dry mouth, or immune deficiencies. Review all medications with your doctor to identify and potentially modify those contributing to thrush.
- Diet: While not a primary treatment, some find avoiding sugary foods and yeast-containing products can help manage Candida overgrowth, though scientific evidence for this is mixed.
- Monitor for Recurrence: If thrush recurs frequently, it's a strong indicator that an underlying health issue or persistent risk factor needs further investigation.
Prevention
Preventing these conditions is always better than treating them. The prevention strategies are as distinct as their causes.
Prevention of Leukoplakia
Preventing leukoplakia largely revolves around minimizing exposure to irritants and carcinogens and regular screening.
- Eliminate Tobacco Use: This is the single most effective preventive measure. Quitting smoking and smokeless tobacco significantly reduces the risk of leukoplakia and oral cancer.
- Moderate Alcohol Consumption: Limit or avoid heavy alcohol intake.
- Regular Dental Check-ups and Screenings: Biannual (every 6 months) dental visits are crucial. Dentists are trained to perform oral cancer screenings, which include visually inspecting for any suspicious white or red patches. Early detection is key for better outcomes.
- Protect Lips from Sun: Use lip balm with SPF, especially if you spend a lot of time outdoors, to prevent actinic cheilitis.
- Maintain Good Oral Hygiene: While not a primary cause, a healthy oral environment is always beneficial.
- Address Chronic Irritation: Ensure dentures fit properly and address any rough tooth surfaces or sharp restorations that might cause constant irritation.
Prevention of Oral Thrush
Preventing oral thrush focuses on maintaining a balanced oral microbiome and addressing risk factors.
- Good Oral Hygiene: Brush your teeth and tongue at least twice a day and floss daily. This helps to reduce the microbial load in your mouth.
- Denture Care: If you wear dentures, remove them before sleeping, clean them thoroughly every day, and soak them in a denture cleaning solution. Follow your dentist's instructions for denture maintenance.
- Rinse After Inhalers: If you use corticosteroid inhalers, rinse your mouth thoroughly with water after each use to wash away medication residue.
- Manage Underlying Conditions: Work with your doctor to effectively manage diabetes, HIV, or other immune-compromising conditions.
- Prudent Antibiotic Use: Only take antibiotics when necessary and for the prescribed duration. Discuss potential alternatives or prophylactic measures with your doctor if you are prone to thrush after antibiotic courses.
- Address Dry Mouth: If you suffer from dry mouth, discuss strategies with your dentist, such as using artificial saliva, sugar-free gum, or prescription medications that stimulate saliva flow.
- Balanced Diet: A healthy, balanced diet supports overall immune function. Some individuals find that limiting sugar and refined carbohydrates can help, although this is not a universally accepted recommendation for Candida control.
Risks and Complications
Both conditions, if left untreated or unmanaged, can lead to significant health complications.
Risks and Complications of Leukoplakia
The primary and most serious complication of leukoplakia is its potential for malignant transformation.
- Malignant Transformation: The most significant risk is that leukoplakia can progress into oral squamous cell carcinoma. The rate of malignant transformation varies from 5% to 17% over 10-20 years, with some forms (e.g., erythroleukoplakia, PVL) having much higher rates. This is why vigilance and biopsy are critical mouth cancer signs.
- Recurrence: Even after successful surgical removal, leukoplakia can recur in the same location or develop in new areas, necessitating ongoing monitoring.
- Scarring and Functional Impairment: Extensive surgical removal can lead to scarring, which may affect speech, swallowing, or the aesthetic appearance of the mouth.
- Psychological Distress: The constant worry about a precancerous lesion can cause significant anxiety and stress.
Risks and Complications of Oral Thrush
While generally less severe than leukoplakia, untreated or recurrent thrush can lead to discomfort and spread.
- Spread of Infection: If left untreated, oral thrush can spread to other parts of the body, particularly in immunocompromised individuals. It can extend down the esophagus (esophageal candidiasis), causing pain and difficulty swallowing, or even spread systemically (invasive candidiasis), affecting organs like the lungs, liver, and brain, which can be life-threatening.
- Chronic Discomfort: Persistent thrush can cause ongoing pain, burning, and altered taste, significantly impacting quality of life and nutrition.
- Nutritional Deficiencies: Painful eating and difficulty swallowing can lead to inadequate food intake and subsequent nutritional deficiencies.
- Compromised Quality of Life: Persistent symptoms can interfere with daily activities, social interactions, and overall well-being.
Comparison Table: Leukoplakia vs. Oral Thrush at a Glance
| Feature | Leukoplakia | Oral Thrush (Oral Candidiasis) |
|---|---|---|
| Appearance | White/grayish patch/plaque | Creamy white, cottage cheese-like lesions |
| Scrapability | NON-SCRAPABLE | SCRAPABLE (reveals red, often bleeding tissue) |
| Underlying Cause | Chronic irritation, tobacco, alcohol, HPV | Fungal overgrowth (Candida albicans) |
| Malignant Potential | PRE-CANCEROUS (5-17% risk of transformation) | NOT CANCEROUS |
| Symptom Onset | Often asymptomatic, slow onset | Can be painful/sore, relatively quick onset |
| Primary Risk Factors | Tobacco, heavy alcohol, HPV, sun exposure | Weakened immune system, antibiotics, steroids, dentures, dry mouth, diabetes |
| Primary Treatment | Biopsy, surgical removal, lifestyle changes | Antifungal medications (topical/systemic), oral hygiene |
| Typical Duration | Persistent if untreated, requires ongoing monitoring | Resolves in 1-2 weeks with treatment |
| Recurrence Risk | High, even after treatment | Common if underlying cause not addressed |
Children / Pediatric Considerations
While both conditions can affect children, their prevalence and causes differ significantly from adults.
Oral Thrush in Children
Oral thrush is extremely common in infants, often appearing as white patches in their mouths during the first few months of life. This is due to their developing immune systems and the frequent use of bottles or pacifiers. It is generally harmless and easily treatable.
- Signs in Infants: Creamy white patches on the tongue and inner cheeks, fussiness during feeding, reluctance to feed, and sometimes a diaper rash if the yeast passes through the digestive system.
- Causes in Infants: Immature immune system, passage through the birth canal (exposure to Candida), antibiotic use in the infant or breastfeeding mother.
- Treatment: Pediatricians typically prescribe a topical antifungal solution (e.g., nystatin liquid) to be swabbed inside the baby's mouth. If breastfeeding, the mother may also need treatment for her nipples to prevent reinfection. Proper sterilization of bottles and pacifiers is also important.
- Prognosis: Infant thrush usually clears up quickly with treatment and rarely leads to serious complications.
Leukoplakia in Children
Leukoplakia is very rare in children and adolescents. When it does occur, it warrants thorough investigation due to its precancerous potential.

- Causes: Unlike adults, tobacco and alcohol are rarely factors. Causes in children might include chronic irritation from a sharp tooth or restoration, specific genetic syndromes, or, rarely, HPV infection.
- Diagnosis and Treatment: Any persistent white patch in a child's mouth that cannot be scraped off should be evaluated by a pediatric dentist or oral pathologist. A biopsy would likely be recommended due to the unusual presentation in this age group. Treatment would involve addressing the underlying cause and, if necessary, surgical removal, followed by close monitoring.
- Importance: Although rare, recognizing leukoplakia in children is vital as early diagnosis and intervention are critical given its potential for malignant transformation.
Cost Breakdown
A detailed look at the financial aspects for US patients.
Average US Costs (Low, Mid, High)
As seen in the comparison table, costs vary significantly:
- Leukoplakia Diagnosis (Biopsy):
- Low: $200 (simple incisional biopsy, lab fee included).
- Mid: $500 (more complex biopsy, specialist oral surgeon).
- High: $800+ (extensive biopsy, multiple sites, specialized pathology).
- Leukoplakia Treatment (Surgical Excision):
- Low: $500 (small lesion, scalpel excision in general dental office).
- Mid: $1,500 (moderate lesion, laser or cryotherapy in specialist office).
- High: $3,000+ (large or complex lesion, advanced laser, in-office surgical suite).
- Oral Thrush Treatment (Medication):
- Low: $10 (generic nystatin rinse with prescription drug coverage).
- Mid: $50 (generic fluconazole without prescription drug coverage, or brand-name topical).
- High: $200+ (multiple courses, different medications, or if compounded).
With vs. Without Insurance
- With Insurance: Dental insurance typically covers a portion of diagnostic procedures (exams, X-rays, biopsies) and basic treatments. Medical insurance is usually responsible for medically necessary procedures, including biopsies and surgical removal of precancerous lesions, especially if performed by an oral surgeon or physician. For thrush, medical insurance with a prescription drug plan will cover most of the cost of antifungals, usually with a co-pay. Out-of-pocket expenses (deductibles, co-pays, co-insurance) will still apply.
- Without Insurance: Patients without insurance will be responsible for the full cost of all procedures and medications. Negotiating cash discounts with providers or seeking care at community health clinics may offer some relief.
Payment Plans and Financing Options
Many dental and oral surgery offices offer:
- In-house payment plans: Often interest-free for a few months.
- Third-party medical/dental credit cards: Such as CareCredit, which offer deferred interest or low-interest financing options.
- Flexible Spending Accounts (FSAs) and Health Savings Accounts (HSAs): These tax-advantaged accounts can be used to pay for qualified medical and dental expenses.
Cost-Saving Tips
- Early Detection: Regular dental check-ups are the best cost-saving measure. Catching conditions like leukoplakia early can prevent costly and extensive treatments down the line.
- Generic Medications: Always ask your doctor or pharmacist if a generic version of your antifungal medication is available, as it will be significantly cheaper than brand-name drugs.
- Shop Around for Prescriptions: Use online tools or apps to compare prescription drug prices at different pharmacies.
- Community Health Clinics/Dental Schools: These institutions often provide care at reduced rates.
- Negotiate Cash Prices: If you are uninsured, ask your provider for a cash discount before treatment.
Frequently Asked Questions
Can leukoplakia turn into cancer?
Yes, leukoplakia is considered a potentially malignant disorder. While not all leukoplakia lesions transform into cancer, an estimated 5-17% can develop into oral squamous cell carcinoma over time. This risk underscores the critical importance of proper diagnosis and ongoing monitoring by a dental professional.
Is thrush contagious?
Oral thrush is generally not considered highly contagious for healthy individuals. While the Candida yeast can be transmitted through kissing or breastfeeding, a healthy immune system can typically keep the yeast in check. However, it can be transmitted from a baby to a breastfeeding mother or to another immunocompromised individual.
How long does it take to treat thrush?
With appropriate antifungal treatment, oral thrush typically resolves within 7 to 14 days. Symptoms often begin to improve within a few days of starting medication. It's crucial to complete the entire course of medication to ensure the infection is fully eradicated and to prevent recurrence.
What's the difference between leukoplakia and erythroplakia?
Leukoplakia refers to a white patch that cannot be scraped off. Erythroplakia, on the other hand, is a red patch in the mouth that also cannot be attributed to another condition. Erythroplakia is significantly more concerning than leukoplakia, as it has a much higher rate of malignant transformation, often exceeding 50%. A lesion with both red and white components is called erythroleukoplakia and also carries a very high risk.
Can I treat thrush at home?
While good oral hygiene and dietary changes might help manage mild cases or prevent recurrence, medically diagnosed oral thrush typically requires antifungal medication prescribed by a dentist or doctor. Over-the-counter remedies are generally not effective for treating an active fungal infection. Always consult a professional for diagnosis and treatment.
How often should I get checked for oral cancer?
The American Dental Association (ADA) recommends regular dental check-ups, ideally every six months. During these visits, your dentist performs a thorough oral cancer screening, looking for any suspicious lesions, including potential leukoplakia or other mouth cancer signs. For individuals with higher risk factors (e.g., tobacco/alcohol use, history of leukoplakia), more frequent screenings may be recommended.
Is leukoplakia painful?
In its early stages, leukoplakia is typically painless and asymptomatic. This lack of symptoms is precisely why many cases are discovered during routine dental exams. However, if the lesion becomes irritated, undergoes malignant transformation, or is associated with chronic inflammation, it can eventually cause discomfort, burning, or pain.
What increases my risk for leukoplakia?
The most significant risk factors for leukoplakia are tobacco use (smoking, chewing tobacco) and heavy alcohol consumption. Other contributing factors include chronic irritation, human papillomavirus (HPV) infection, and excessive sun exposure to the lips. Individuals with weakened immune systems may also be at a slightly increased risk.
Are there natural remedies for thrush?
Some natural remedies like yogurt with live cultures, probiotics, coconut oil pulling, or rinsing with diluted tea tree oil are sometimes explored for thrush. While these may support oral health, there is limited scientific evidence to support their effectiveness as primary treatments for an active thrush infection. They should not replace prescribed antifungal medications, especially for persistent or severe cases.
How is a biopsy for leukoplakia performed?
A biopsy for leukoplakia is usually performed by a dentist, oral surgeon, or periodontist. After administering local anesthesia to numb the area, a small piece of the suspicious tissue (incisional biopsy) or the entire lesion (excisional biopsy for smaller lesions) is removed. The tissue is then sent to an oral pathologist for microscopic examination to determine the definitive diagnosis and assess for any precancerous or cancerous changes.
When to See a Dentist
Prompt evaluation of any unusual oral changes is paramount for your oral and overall health.
You should see a dentist immediately if you notice:
- Any white patch in your mouth that does not rub off within two weeks. This is a primary indicator that requires professional evaluation for leukoplakia and oral cancer screening.
- Any red patch (erythroplakia), as these carry an even higher risk of malignancy.
- A sore or lesion in your mouth that does not heal within two weeks, regardless of color or appearance. This is a significant mouth cancer sign.
- Difficulty or pain when swallowing, chewing, or moving your tongue or jaw, especially if accompanied by a lesion.
- A persistent sore throat or hoarseness.
- Numbness or persistent tingling in any area of your mouth, face, or neck.
- A lump or thickening in your cheek, tongue, or neck.
- Significant weight loss without an apparent reason.
- White, creamy, cottage cheese-like lesions that persist for more than a few days, even if they scrape off, especially if accompanied by discomfort or fever. This indicates persistent oral thrush requiring treatment.
Red Flags vs. Routine Care Guidance:
- Red Flags (Urgent Care): Any of the symptoms listed above, especially persistent white or red patches, non-healing sores, or lumps, warrant an urgent appointment. Do not wait for your next routine check-up.
- Routine Care Guidance: Regular dental check-ups (every 6 months) are crucial for prevention and early detection of both leukoplakia and oral thrush, as well as general oral health. Your dentist can spot subtle changes you might miss.
Remember, early detection and timely intervention are key to successfully managing both leukoplakia and oral thrush. Empower yourself by being vigilant about your oral health and never hesitate to seek professional dental advice for any concerns.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Floor of Mouth Cancer: Complete Guide
Each year, over 54,000 Americans are diagnosed with oral cavity or oropharyngeal cancer, making it a significant public health concern. While often overlooked, floor of mouth cancer is a particularly aggressive and common form of oral cancer, accounting for a substantial percentage of all oral c
February 23, 2026
Oral Cancer Stages Pictures: Complete Guide
Oral cancer, a serious and potentially life-threatening disease, affects thousands of Americans each year. According to the American Cancer Society, approximately 54,000 new cases of oral cavity or oropharyngeal cancer are diagnosed annually in the United States. While these numbers can be daunt
February 23, 2026
Can You Die From Mouth Cancer
Oral cancer is a formidable disease, often striking with insidious subtlety before revealing its devastating potential. It's a question that weighs heavily on the minds of those who receive a diagnosis or even those simply concerned about unusual oral symptoms: can you die from mouth cancer? The
February 23, 2026

Mouth Cancer Photos: Complete Guide
Oral cancer is a formidable disease that affects tens of thousands of Americans each year, often with devastating consequences if not detected early. According to the Oral Cancer Foundation, approximately 54,000 Americans are diagnosed with oral or oropharyngeal cancer annually, and nearly 11,23
February 23, 2026