Calculus
4,542 words · 15 min read
Quick Definition
Hardened dental plaque that has mineralized on the tooth surface, also called tartar. Calculus cannot be removed by brushing and requires professional cleaning.
Understanding Dental Calculus: The Definitive Guide to Tartar and Your Oral Health
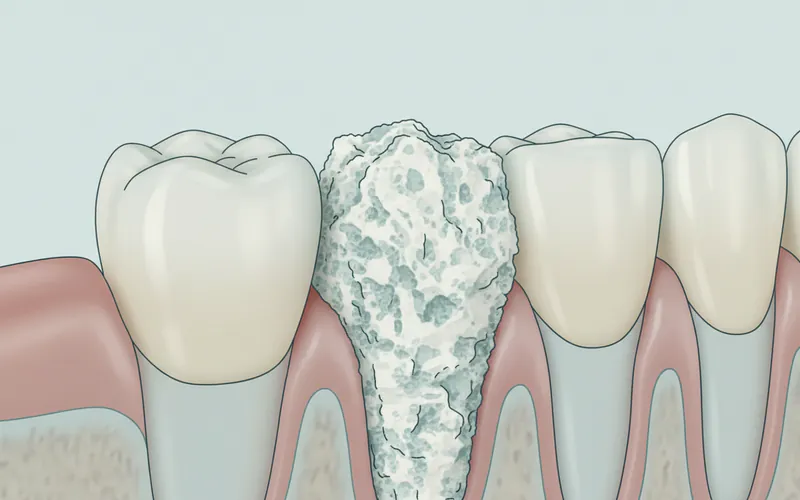
Dental calculus, commonly known as tartar, is a formidable foe in the battle for optimal oral health. It represents a significant step beyond ordinary plaque build-up, transforming into a hard, mineralized deposit that stubbornly adheres to the surfaces of your teeth and even beneath the gum line. Unlike its softer precursor, plaque, calculus cannot be removed by regular brushing and flossing at home, necessitating professional dental intervention.
Why does understanding calculus matter? Because its presence is a direct threat to the health of your gums and the integrity of your teeth. Left untreated, calculus serves as a rough, porous breeding ground for harmful bacteria, fueling a cycle of inflammation and infection that can lead to gingivitis (early gum disease) and progress to the more severe and potentially irreversible condition of periodontal disease. Globally, the prevalence of dental calculus varies widely, but it is incredibly common. Studies suggest that a vast majority of adults, especially those over 30, exhibit some level of calculus accumulation. In the United States, gum disease, often initiated or exacerbated by calculus, affects nearly half of adults aged 30 and older, representing over 64 million Americans. This makes calculus a widespread concern, affecting individuals across all demographics, though its severity can differ based on oral hygiene habits, genetics, and lifestyle factors.
The good news is that with proper understanding, diligent prevention, and timely professional care, the impact of dental calculus can be effectively managed, safeguarding your smile and overall well-being.
Key Takeaways:
- Calculus is hardened dental plaque, also known as tartar, that has mineralized.
- It cannot be removed by brushing or flossing at home.
- Calculus provides a rough surface for bacteria, leading to gingivitis and periodontal disease.
- It contributes to bad breath, tooth discoloration, and gum inflammation.
- Professional dental cleaning (scaling and root planing) is essential for its removal.
- Prevention involves consistent oral hygiene and regular dental check-ups.
Detailed Explanation
Types and Classifications of Dental Calculus
Dental calculus is primarily classified into two main types based on its location relative to the gum line:
- Supragingival Calculus: This type of calculus forms above the gum line (supra- meaning above, gingival- referring to the gums). It is often visible to the naked eye, appearing as a yellowish, brownish, or even black deposit on the visible surfaces of the teeth, especially near the gum line, behind the lower front teeth, and on the cheek side of the upper molars. Supragingival calculus typically derives its minerals from saliva, which is rich in calcium and phosphate. Its rough surface often traps extrinsic stains from coffee, tea, tobacco, and certain foods, contributing to tooth discoloration.
- Subgingival Calculus: More insidious and dangerous, subgingival calculus forms below the gum line (sub- meaning below). It is usually dark brown or black due in part to the presence of blood pigments from inflamed tissues. This type of calculus is harder to detect without a dental examination and instruments. Its mineral source comes from gingival crevicular fluid (fluid that oozes from the gums) and inflammatory exudates. Subgingival calculus is particularly problematic because it creates a pathway for bacteria to colonize the periodontal pockets (the spaces between the teeth and gums), actively contributing to the progression of periodontal disease by causing chronic inflammation, bone loss, and eventually tooth mobility and loss.
While both types are detrimental, subgingival calculus poses a greater risk due to its hidden nature and direct impact on the supporting structures of the teeth.
Causes and Risk Factors for Calculus Formation
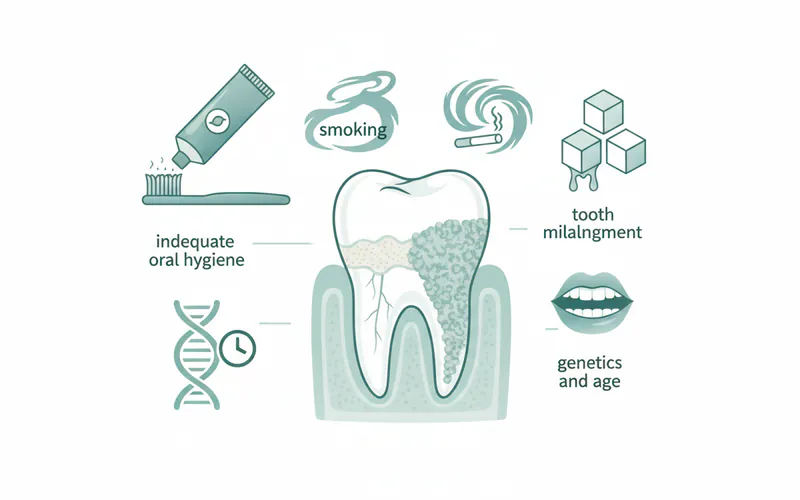
The formation of dental calculus is a direct consequence of inadequate oral hygiene, but several other factors can accelerate or exacerbate its development.
The primary cause is the persistent presence of plaque, a soft, sticky biofilm of bacteria that constantly forms on your teeth. If plaque isn't thoroughly removed through daily brushing and flossing, it begins to absorb minerals from your saliva (for supragingival calculus) or gingival crevicular fluid (for subgingival calculus). This mineralization process can start within 24-72 hours of plaque formation, transforming the soft film into hard calculus.
Key risk factors include:
- Poor Oral Hygiene: Infrequent or ineffective brushing and flossing are the leading culprits. If plaque isn't mechanically removed daily, it will inevitably harden into calculus.
- Diet: A diet high in sugars and refined carbohydrates promotes the growth of plaque-forming bacteria. Additionally, consuming acidic foods and drinks can slightly soften tooth enamel, potentially making it easier for plaque to adhere initially.
- Saliva Composition: Individuals with saliva naturally rich in calcium and phosphate can be more prone to rapid calculus formation. Saliva flow rate also plays a role; reduced saliva can lead to drier mouths where bacteria thrive.
- Smoking and Tobacco Use: Tobacco users are significantly more likely to develop calculus and more severe forms of periodontal disease. Tobacco chemicals disrupt normal gum function and blood flow, creating an environment conducive to calculus formation and hindering the body's ability to fight off bacterial infections.
- Age: As people age, they tend to accumulate more calculus due to cumulative exposure, longer periods of potential plaque build-up, and sometimes reduced dexterity for effective oral hygiene.
- Genetics: Some individuals may have a genetic predisposition to calculus formation or a heightened inflammatory response to its presence.
- Systemic Diseases and Medications: Certain health conditions, such as diabetes, and medications that cause dry mouth (xerostomia) can alter oral environments, making individuals more susceptible to calculus and gum disease.
- Rough Tooth Surfaces: Restorations with rough margins, chipped teeth, or crowded teeth can provide ideal surfaces for plaque and calculus to accumulate, as they are harder to clean effectively.
Understanding these causes and risk factors is crucial for developing effective prevention and management strategies.
Signs and Symptoms to Watch For
While only a dental professional can definitively diagnose calculus, there are several signs and symptoms you can look for that may indicate its presence:
- Rough Texture on Teeth: One of the most common signs is a rough, gritty feeling on the surface of your teeth, particularly near the gum line. This rough texture can be felt with your tongue and is a stark contrast to the smooth feel of clean enamel.
- Discoloration: Supragingival calculus often appears as a yellowish, brownish, or even black deposit. These stains can be intrinsic to the calculus itself or extrinsic stains absorbed into its porous surface from food, drinks, or tobacco.
- Bad Breath-everything-you-need-to-know "Complete Guide to Bad Breath (Halitosis): Everything You Need to Know") (Halitosis): Calculus provides a perfect environment for odor-producing bacteria to flourish. These bacteria release volatile sulfur compounds, leading to persistent bad breath that cannot be resolved with brushing alone.
- Swollen, Red, or Tender Gums: The bacteria harbored within calculus release toxins that irritate the gum tissues. This irritation leads to inflammation, causing the gums to become redder than normal, swollen, and sometimes tender to the touch. This is a classic sign of gingivitis.
- Bleeding Gums: Gums that bleed easily during brushing, flossing, or even when eating hard foods are a significant indicator of gum inflammation caused by plaque and calculus. Healthy gums should not bleed.
- Receding Gums: Over time, the chronic inflammation caused by calculus can lead to the gum tissue pulling away from the teeth, exposing more of the tooth root. This is a sign of advancing periodontal disease.
- Increased Tooth Sensitivity: Exposed tooth roots due to gum recession can lead to increased sensitivity to hot, cold, or sweet stimuli.
- Loose Teeth: In the advanced stages of periodontal disease, chronic inflammation and bone loss caused by calculus can weaken the support structures of the teeth, leading to tooth mobility.
If you observe any of these symptoms, it's a clear signal to schedule a dental appointment promptly.
Diagnosis Process — What Your Dentist Does
Diagnosing dental calculus is a routine part of a comprehensive dental examination. Your dentist or dental hygienist employs a combination of visual inspection and specialized tools to identify both supragingival and subgingival deposits.
- Visual Inspection: The most straightforward method involves a thorough visual examination of your teeth and gums. Your dental professional will use a dental mirror and good lighting to look for any visible signs of calculus, such as discoloration or rough surfaces, particularly along the gum line and in areas prone to accumulation (e.g., lingual surfaces of lower anterior teeth, buccal surfaces of upper molars).
- Dental Explorer (Periodontal Probe): This is a crucial instrument for detecting calculus. A dental explorer is a thin, sharp, curved tool that allows the dentist or hygienist to gently "feel" for rough spots or irregularities on the tooth surface, both above and, more importantly, below the gum line. When the explorer encounters calculus, it will feel gritty or catch, indicating the presence of hardened deposits. A periodontal probe is used to measure the depth of the gum pockets, which can indicate the presence and severity of subgingival calculus and periodontal disease. Healthy pockets are typically 1-3 millimeters deep; deeper pockets often signify inflammation and calculus.
- Dental X-rays: While calculus itself isn't always directly visible on standard X-rays, extensive subgingival calculus can sometimes appear as irregular projections on the tooth roots. More importantly, X-rays are vital for assessing the amount of bone loss around the teeth, which is a direct consequence of long-standing calculus and periodontal disease. The presence and pattern of bone loss can indirectly confirm the severity of the calculus problem.
- Air and Light: Sometimes, blowing a stream of air onto the teeth can help reveal calculus that might otherwise be obscured by saliva or the gums, especially in shallower pockets. Transillumination (shining a light through the teeth) can also highlight subtle deposits.
Based on the findings from these diagnostic steps, your dental professional can determine the extent and type of calculus present and recommend the appropriate treatment plan.
Treatment Options for Dental Calculus
The fundamental treatment for dental calculus is its professional removal, a process often referred to as scaling. The specific procedure recommended will depend on the amount and location of the calculus and the presence of periodontal disease.

1. Prophylaxis (Routine Dental Cleaning)
- Description: This is a standard cleaning for individuals with generally healthy gums and only supragingival calculus or mild gingivitis. It involves removing plaque, calculus, and stains from the tooth surfaces above the gum line.
- Pros: Prevents gum disease, maintains oral health, relatively quick and comfortable.
- Cons: Not sufficient for subgingival calculus or established periodontal disease.
- Cost Range in the US:
- Without Insurance: $75 - $200
- With Insurance: Typically covered at 80-100%, so out-of-pocket might be $0 - $50 (depending on plan, after deductible).
2. Scaling and Root Planing (Deep Cleaning)
- Description: This is the gold standard for treating subgingival calculus and early to moderate periodontal disease. It's a two-part procedure:
- Scaling: Involves meticulously removing plaque and calculus from above and below the gum line, down to the bottom of the periodontal pockets. This can be done using manual instruments (scalers and curettes) or ultrasonic devices that use high-frequency vibrations to break down calculus.
- Root Planing: After scaling, the root surfaces are smoothed to remove any remaining calculus, bacterial toxins, and irregular areas. This smooth surface makes it harder for plaque to reattach and allows the gum tissue to reattach more firmly to the tooth.
- Pros: Effectively removes subgingival calculus, reduces inflammation, halts the progression of periodontal disease, can prevent tooth loss, often reduces pocket depths.
- Cons: More involved and takes longer than a standard cleaning, may require local anesthesia, can cause temporary sensitivity. Multiple appointments might be needed (e.g., one quadrant at a time).
- Cost Range in the US (per quadrant):
- Without Insurance: $200 - $500 per quadrant (a full mouth treatment can range from $800 - $2,000+).
- With Insurance: Often covered at 50-80%, so out-of-pocket might be $50 - $250 per quadrant (after deductible).
3. Periodontal Maintenance
- Description: After scaling and root planing, patients with a history of periodontal disease typically require more frequent follow-up cleanings (every 3-4 months) to prevent the recurrence of calculus and manage the disease. These appointments are more thorough than routine prophylaxes but less intensive than initial scaling and root planing.
- Pros: Essential for long-term management of periodontal disease, prevents relapse.
- Cons: Ongoing commitment and cost.
- Cost Range in the US: Similar to prophylaxis, but insurance coverage may differ (some plans classify it differently than routine cleanings).
Comparison of Treatment Options
| Feature | Prophylaxis (Routine Cleaning) | Scaling and Root Planing (Deep Cleaning) |
|---|---|---|
| Purpose | Preventative; remove supragingival plaque & calculus | Therapeutic; remove subgingival calculus & bacterial toxins |
| Conditions Treated | Healthy gums, mild gingivitis | Gingivitis with subgingival calculus, mild to moderate periodontitis |
| Anesthesia | Generally not needed | Often recommended (local anesthetic) |
| Time | 30-60 minutes | 1-2 hours per quadrant (often 2-4 appointments) |
| Cost (US, avg) | $75 - $200 | $200 - $500 per quadrant |
| Insurance | High coverage (80-100%) | Moderate coverage (50-80%) |
| Follow-up | Every 6 months for most | Periodontal maintenance every 3-4 months |
Step-by-Step: What to Expect During Treatment
If you're undergoing scaling and root planing (deep cleaning), here's a general overview of what to expect:
- Anesthesia (if needed): Your dentist or hygienist will likely administer a local anesthetic to numb the areas being treated. This ensures your comfort during the procedure, especially since the work will be done below the gum line.
- Assessment and Mapping: Before starting, the dental professional may re-examine your gums, measuring pocket depths and identifying areas with significant calculus.
- Scaling:
- Ultrasonic Scaler: This device uses high-frequency vibrations combined with a stream of water to break up calculus and flush away debris. It's often used first to remove larger deposits efficiently. You'll hear a whirring sound and feel vibrations, along with the spray of water.
- Hand Instruments: Fine dental scalers and curettes are then used to meticulously scrape away smaller, more stubborn pieces of calculus from the tooth surfaces, both above and, critically, below the gum line. The curved tips of these instruments allow for thorough cleaning within the gum pockets.
- Root Planing: Once the calculus is removed, the instruments are used to smooth the root surfaces. This step is crucial for removing any embedded bacterial toxins and creating a clean, smooth surface that makes it difficult for bacteria to reattach and encourages gum reattachment.
- Irrigation and Rinsing: Throughout the procedure, water is used to rinse away debris. You'll be asked to rinse frequently.
- Polishing: After the main scaling and planing is complete, a polishing paste and rotating rubber cup are used to smooth the visible tooth surfaces and remove any remaining surface stains.
- Fluoride Treatment (Optional): Some dentists may apply a fluoride treatment to help reduce sensitivity and strengthen enamel.
- Antimicrobial Rinse (Optional): In some cases, an antimicrobial mouth rinse may be prescribed for use at home to further reduce bacteria.
Deep cleaning is often completed in multiple appointments, treating one or two quadrants of the mouth at a time, to ensure thoroughness and manage patient comfort.
Recovery Timeline and Aftercare
The recovery from a deep cleaning (scaling and root planing) is generally straightforward, but it's important to follow specific aftercare instructions to ensure proper healing and prevent recurrence.
- Immediate Aftermath (First 24-48 hours):
- Numbness: If local anesthesia was used, your mouth will remain numb for a few hours. Be cautious when eating or drinking to avoid biting your tongue or cheek.
- Soreness and Sensitivity: It's common to experience some gum soreness, tenderness, and increased tooth sensitivity to hot and cold. This should subside within a few days. Over-the-counter pain relievers like ibuprofen or acetaminophen can help manage discomfort.
- Bleeding: Slight bleeding from the gums may occur, especially during brushing. This is normal and usually resolves quickly.
- First Week:
- Diet: Stick to soft, easy-to-chew foods. Avoid extremely hot, cold, spicy, or acidic foods that might irritate sensitive gums.
- Oral Hygiene: Continue brushing gently with a soft-bristled toothbrush and flossing daily. Your dentist or hygienist might recommend a specific technique or a temporary antimicrobial mouthwash. Avoid aggressive brushing or flossing that could irritate healing gums.
- Smoking/Alcohol: It's highly advisable to avoid smoking and alcohol consumption, as they can impede healing and increase the risk of complications.
- Beyond One Week:
- Sensitivity: While initial soreness resolves, some sensitivity might linger for a few weeks, especially if root surfaces were exposed. Using desensitizing toothpaste can be beneficial.
- Gum Appearance: Your gums should gradually appear healthier—less red, less swollen, and firmer. The goal is for the gums to reattach more snugly to the tooth surfaces.
- Long-term Aftercare:
- Maintain Excellent Oral Hygiene: This is paramount. Brush at least twice a day for two minutes with a fluoride toothpaste, and floss daily. Consider an electric toothbrush for more effective plaque removal.
- Regular Dental Check-ups and Periodontal Maintenance: For those who have undergone deep cleaning, regular periodontal maintenance appointments (typically every 3-4 months) are crucial to prevent the re-accumulation of calculus and monitor gum health. This is more frequent than standard 6-month cleanings because you have a history of gum disease.
- Healthy Lifestyle: A balanced diet, avoidance of tobacco products, and managing systemic conditions like diabetes will significantly contribute to sustained oral health.
Adhering to these aftercare guidelines is essential for successful healing and preventing the progression of gum disease.
Prevention Strategies
Preventing dental calculus is largely about diligently preventing plaque buildup. While professional cleanings are essential for removing existing calculus, consistent daily habits are your first line of defense.

- Brush Twice Daily: Brush your teeth for at least two minutes, twice a day, using a soft-bristled toothbrush and a fluoride toothpaste. Pay close attention to the gum line, the back of your teeth, and around any fillings or crowns. An electric toothbrush can be particularly effective at disrupting plaque.
- Floss Daily: Flossing (or using interdental brushes) once a day is critical to remove plaque and food particles from between your teeth and under the gum line, areas your toothbrush can't reach. If plaque isn't removed from these areas, calculus will form.
- Use an Antimicrobial Mouthwash: While not a substitute for brushing and flossing, therapeutic mouthwashes containing active ingredients like cetylpyridinium chloride (CPC) or essential oils can help reduce bacteria and slow plaque formation. Discuss with your dentist if this is appropriate for you.
- Regular Dental Check-ups and Professional Cleanings: Schedule routine dental cleanings typically every six months, or more frequently if recommended by your dentist due to existing gum disease or rapid calculus formation. These appointments allow for the removal of any nascent calculus before it becomes a significant problem.
- Balanced Diet: Limit sugary and starchy foods and drinks, as these fuel the bacteria that produce plaque. Choose a diet rich in fruits, vegetables, and whole grains. Drinking water after meals can also help rinse away food particles.
- Avoid Tobacco Products: Smoking and chewing tobacco are significant risk factors for calculus and periodontal disease. Quitting tobacco is one of the most impactful steps you can take for your oral and overall health.
- Manage Systemic Health Conditions: If you have conditions like diabetes, ensure they are well-managed, as they can impact gum health.
- Identify and Address Risk Factors: If you have crowded teeth or rough restorations, discuss options with your dentist to address these areas that can trap plaque.
By consistently applying these preventive measures, you can significantly reduce your risk of calculus formation and maintain a healthier smile.
For Parents / Pediatric Considerations
While calculus is more commonly associated with adults, it can and does affect children and adolescents. Though less prevalent in very young children, its presence can increase with age, especially during the pre-teen and teenage years.
- Causes in Children: Similar to adults, the primary cause of calculus in children is inadequate oral hygiene. Children may not have the dexterity or discipline to brush and floss effectively, leading to plaque accumulation. Diet, particularly frequent consumption of sugary snacks and drinks, also plays a significant role.
- Signs to Watch For: Parents should look for yellowish or brownish deposits on their child's teeth, especially near the gum line of the lower front teeth. Swollen, red, or easily bleeding gums during brushing are also red flags for gingivitis, which often precedes or accompanies calculus.
- Early Intervention is Key: Teaching good oral hygiene habits from an early age is paramount.
- Supervise Brushing: Supervise and assist young children with brushing until they are around 7-8 years old to ensure thoroughness.
- Introduce Flossing Early: Start flossing your child's teeth as soon as two teeth touch.
- Regular Pediatric Dental Visits: Schedule regular check-ups and cleanings with a pediatric dentist starting by the first birthday or with the eruption of the first tooth. These visits are essential for monitoring oral health, educating parents, and removing any calculus that forms.
- Addressing Teenagers: Teenagers often face challenges with consistent oral hygiene due to busy schedules, dietary choices, and sometimes reduced emphasis on self-care. Hormonal changes during puberty can also make gums more susceptible to inflammation. Encouraging them to maintain excellent oral hygiene and attend regular dental appointments is crucial.
- Treatment: If calculus is found, a professional cleaning (prophylaxis) will be performed, similar to adults. In rare cases of more severe gingivitis, a deeper cleaning might be necessary.
Addressing calculus early in life helps set the foundation for a lifetime of good oral health and prevents the progression to more serious gum disease.
Frequently Asked Questions
Q1: Is removing dental calculus painful?
A: Routine dental cleanings (prophylaxis) to remove supragingival calculus are generally not painful, though some individuals may experience minor discomfort or sensitivity, especially if there's existing gum inflammation. For deep cleanings (scaling and root planing) that involve removing subgingival calculus, local anesthesia is frequently used to numb the area, making the procedure comfortable. You might feel pressure or vibrations, but significant pain should be avoided. Post-procedure, some soreness and sensitivity are common but manageable with over-the-counter pain relievers.
Q2: How long does it take to remove calculus?
A: The duration depends on the amount and type of calculus. A routine prophylaxis for minimal supragingival calculus usually takes 30 to 60 minutes. For extensive supragingival calculus or subgingival calculus requiring scaling and root planing, the procedure is more involved. It often takes 60 to 90 minutes per quadrant of the mouth, meaning a full deep cleaning can span two to four appointments, each focusing on a different section of your mouth.
Q3: Can I remove calculus at home with DIY methods?
A: Absolutely not. It is strongly advised against attempting to remove calculus at home. Calculus is extremely hard and firmly bonded to the tooth surface. DIY methods, such as scraping with sharp objects, can cause serious damage to your tooth enamel, lead to gum recession, introduce bacteria, and result in infection or even permanent tooth damage. Only trained dental professionals have the specialized instruments and expertise to safely and effectively remove calculus.
Q4: What are the long-term consequences of leaving calculus untreated?
A: Leaving calculus untreated has severe long-term consequences. It relentlessly irritates gum tissue, leading to chronic inflammation known as gingivitis. If ignored, gingivitis progresses to periodontal disease, where the infection spreads beneath the gum line, destroying the bone and ligaments that support your teeth. This can result in: receding gums, deep periodontal pockets, loose teeth, tooth loss, persistent bad breath, and even systemic health issues as oral bacteria can enter the bloodstream.
Q5: Will my dental insurance cover calculus removal?
A: Most dental insurance plans provide coverage for calculus removal, but the extent of coverage varies based on the type of procedure. Routine dental cleanings (prophylaxis) are typically covered at a high percentage, often 80-100%, as they are considered preventative care. Scaling and root planing (deep cleaning) for periodontal disease is usually classified as a basic or major restorative service and may be covered at 50-80% after a deductible. It's crucial to check with your specific insurance provider for details on your plan's coverage and any limitations.
Q6: Are there alternatives to scaling and root planing for calculus removal?
A: For established subgingival calculus and periodontal disease, scaling and root planing is the primary non-surgical treatment and considered the gold standard. While some adjunctive therapies like local antibiotic delivery (e.g., Arestin) or laser therapy might be used in conjunction with scaling and root planing, they are not standalone alternatives for comprehensive calculus removal. In advanced cases of periodontal disease with significant bone loss, surgical options performed by a periodontist may be necessary to access and clean deeper areas. However, these are typically considered when non-surgical methods are insufficient.
Q7: Does calculus always mean I have gum disease?
A: The presence of calculus, especially subgingival calculus, is a strong indicator of gum inflammation and is often a contributing factor to gum disease. If you have calculus, you almost certainly have some degree of gingivitis (inflammation of the gums). However, gingivitis is reversible. If calculus is removed and good oral hygiene is maintained, the gums can heal. If left untreated, calculus will likely lead to the progression of gingivitis into the more serious and irreversible condition of periodontal disease, which involves bone loss. So, while calculus is a major risk factor and sign of gum problems, early detection and treatment can prevent it from escalating to severe periodontal disease.
When to See a Dentist
Regular dental check-ups, ideally every six months, are your best defense against calculus and the problems it causes. These routine visits allow your dentist or hygienist to identify and remove calculus before it leads to significant issues.
However, certain signs warrant an immediate visit to your dentist, outside of your regular schedule:
- Persistent Bad Breath: If you experience chronic bad breath that doesn't improve with regular brushing and flossing.
- Red, Swollen, or Tender Gums: Gums that are consistently inflamed, painful, or bleed easily.
- Receding Gums or Visible Roots: If you notice your gums pulling away from your teeth, making your teeth appear longer.
- Loose or Shifting Teeth: Any change in how your teeth fit together or if they feel loose.
- Pus Between Teeth and Gums: A sign of active infection.
- Increased Sensitivity: Sudden or worsening tooth sensitivity, especially if accompanied by gum issues.
- Visible Deposits: If you can see hard, discolored deposits on your teeth that your toothbrush can't remove.
These symptoms could indicate the presence of significant calculus and advancing periodontal disease, requiring prompt professional evaluation and treatment to prevent further damage and potential tooth loss. Don't wait—early intervention is key to preserving your oral health.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.