Fissure
4,069 words · 14 min read
Quick Definition
A narrow groove or cleft in the chewing surface of a tooth, particularly molars and premolars. Fissures are common sites for cavity development because they trap food and bacteria.
Fissure: Understanding the Grooves That Matter for Your Dental Health
In the intricate landscape of your mouth, the surfaces of your teeth are not uniformly flat. Particularly on the back teeth, you'll find a series of tiny valleys, ridges, and grooves. Among these, some of the most critical to understand for your dental health are known as fissures. These narrow, deep crevices are natural anatomical features, but they also represent one of the primary battlegrounds against tooth decay.

A fissure is a narrow groove or cleft found predominantly on the chewing (occlusal) surfaces of your posterior teeth – the molars and premolars. While they are a normal part of tooth anatomy, their depth and intricate shape make them notorious for trapping food particles and harmful bacteria. This susceptibility to plaque accumulation makes fissures prime locations for the development of dental caries, commonly known as cavities. Understanding what fissures are, why they pose a risk, and how to protect them is fundamental to maintaining a healthy smile for life.
The prevalence of tooth decay originating in fissures is significant. Studies show that a substantial majority—often cited as 80-90%—of cavities in children and adolescents occur on the chewing surfaces of molars and premolars, largely due to the vulnerability of fissures. Even in adults, these areas remain susceptible. By delving into the nature of fissures, we empower ourselves with the knowledge to prevent costly and uncomfortable dental problems, ensuring our teeth remain strong and functional.
Key Takeaways:
- Fissures are natural, narrow grooves on the chewing surfaces of molars and premolars.
- Their intricate shape makes them highly susceptible to trapping food and bacteria, leading to plaque buildup.
- Fissures are the most common starting point for dental caries (cavities), especially in children and adolescents.
- Dental sealants are the primary and most effective preventive measure against fissure decay.
- Regular dental check-ups are crucial for early detection and intervention, whether preventive or restorative.
- Maintaining excellent oral hygiene, combined with professional care, significantly reduces the risk of fissure-related cavities.
Detailed Explanation
Types and Classifications of Fissures
Not all fissures are created equal. Their morphology – the specific shape and depth – significantly influences their susceptibility to decay. Dentists often classify fissures based on their cross-sectional appearance, which helps determine the risk level and the most appropriate preventive or restorative approach.
- V-shaped Fissures: These are relatively broad at the top and narrow down towards the base, resembling a "V." They are generally considered to be at a lower risk of decay because their wider opening allows for better self-cleansing by saliva and easier access for toothbrush bristles.
- U-shaped Fissures: Similar to V-shaped but with a broader, more rounded base. They still offer better access for cleaning than narrower types but can still harbor bacteria.
- I-shaped Fissures (or "Straight Drop"): These are narrow from top to bottom, with parallel walls. They are challenging to clean effectively due to their constricted opening, making them highly prone to decay. Bacteria and food particles can easily get trapped deep within, beyond the reach of a toothbrush.
- K-shaped Fissures: These are complex, often resembling a "K" or an "inverted Y," with multiple branches or accessory grooves extending from the main fissure. Their intricate network provides numerous hiding spots for plaque and are considered high-risk for decay.
- Inverted Y-shaped Fissures: Similar to K-shaped, these have a main groove with smaller, often deeper side branches, making them difficult to clean and highly retentive for debris.
The deeper and narrower the fissure, the greater its propensity to develop caries. Dentists use an explorer probe, sometimes with magnification, to assess the morphology of these grooves and determine the best course of action.
Causes and Risk Factors
The primary "cause" of fissures themselves is natural tooth development. However, several factors contribute to their vulnerability and the development of decay within them:
- Anatomical Structure: This is the most significant factor. Deep, narrow fissures naturally create microenvironments that are difficult to clean. Food particles and plaque can become entrapped, creating an acidic environment that demineralizes enamel.
- Poor Oral Hygiene: Inadequate brushing, especially with improper technique, means that toothbrush bristles cannot effectively reach into the depths of many fissures. This allows plaque to accumulate undisturbed.
- Dietary Habits: Frequent consumption of sugary and acidic foods and beverages fuels the bacteria responsible for producing acids that erode tooth enamel. These acids are particularly damaging when trapped within fissures.
- Inadequate Fluoride Exposure: Fluoride strengthens tooth enamel, making it more resistant to acid attacks. Insufficient exposure to fluoride (through fluoridated water, toothpaste, or professional treatments) can leave fissures more vulnerable.
- Newly Erupted Teeth: When permanent molars and premolars first erupt (typically between ages 6-7 for first molars and 11-13 for second molars), their enamel is not yet fully mature or "hardened" by fluoride. This makes them especially susceptible to decay, and why sealants are often recommended shortly after eruption.
- Xerostomia (Dry Mouth): Saliva plays a crucial role in neutralizing acids and washing away food particles. Reduced saliva flow increases the risk of decay in all areas, including fissures.
- Genetics/Heredity: The specific morphology of an individual's teeth, including the depth and complexity of their fissures, can be genetically influenced. Some people are simply born with more intricate and decay-prone fissure patterns.
Signs and Symptoms to Watch For
In their healthy state, fissures present no symptoms. However, once decay begins to develop within a fissure, certain signs may emerge. It's important to note that fissure decay can often progress significantly before symptoms become noticeable, highlighting the importance of regular dental check-ups.
- Visible Dark Lines or Spots: One of the earliest visual signs of fissure caries can be a dark brown or black line or spot within the fissure itself. This discoloration indicates bacterial activity and demineralization of the enamel. It's important to distinguish this from naturally pigmented grooves, which a dentist can do.
- "Sticky" Fissure: If a dental explorer catches or sticks within a fissure, it can be a sign that the enamel surface has softened or that a small cavity has formed, preventing the smooth passage of the instrument.
- Sensitivity: As decay progresses deeper into the tooth, it may cause sensitivity to hot, cold, or sweet foods and drinks. This is often a sign that the decay has breached the enamel and is approaching or has reached the dentin layer, which is more sensitive.
- Pain When Biting: If the decay is extensive enough to compromise the tooth's structure, or if food gets lodged deeply within an active cavity, you might experience pain when chewing on that tooth.
- Visible Hole or Cavity: In advanced stages, a clear hole or defect may be visible within the fissure, indicating a fully developed cavity.
Diagnosis Process — What Your Dentist Does
Detecting fissure caries can be challenging because of their narrow and deep nature. Often, decay can progress significantly beneath a seemingly intact enamel surface. Dentists employ a combination of methods:
- Visual Examination: The dentist will carefully examine the chewing surfaces of your molars and premolars, often using a dental mirror and good lighting. Magnification (e.g., through loupes) is frequently used to get a closer look at the intricate details of the fissures.
- Dental Explorer Probe: A thin, sharp dental instrument called an explorer is gently run along the fissures. If the explorer "catches" or resists removal, it can indicate a softened enamel surface or a cavity. However, this method is used with caution to avoid damaging remineralizing enamel or creating microfractures.
- Bitewing X-rays: These radiographs are excellent for detecting decay between teeth (interproximal caries) but are less reliable for early fissure decay. Because fissures run parallel to the X-ray beam, early lesions within them may not be visible until they are quite extensive. Still, they can help identify larger lesions or decay that has spread.
- Transillumination: A bright light is shone through the tooth. Areas of decay will absorb more light and appear as a shadow, providing an alternative visual cue.
- Dye Application: In some cases, a special dental dye is applied to the tooth. Decayed areas absorb the dye more readily, making the lesion more apparent.
- Laser Fluorescence Devices (e.g., DIAGNOdent): These modern devices emit a specific wavelength of light into the tooth and measure the fluorescence reflected back. Healthy enamel has a low fluorescence, while decayed enamel and bacteria produce a higher fluorescence. This allows for early, non-invasive detection of even subtle demineralization within fissures.
Early and accurate diagnosis is critical, as it allows for conservative treatment (like sealants for high-risk fissures or very small fillings) before the decay progresses.
Treatment Options with Pros, Cons, and Costs
Treatment for fissures depends on whether they are healthy but high-risk, or if decay has already initiated.
1. Prevention: Dental Sealants (For Healthy or Incipiently Decayed Fissures)
- What it is: A dental sealant is a thin, protective plastic coating painted onto the chewing surfaces of molars and premolars. It flows into the deep grooves and fissures, hardening to create a smooth surface that effectively "seals off" the fissure from food particles and bacteria.
- Pros:
- Highly effective: Reduces the risk of fissure caries by 80% for two years after application and continues to be effective for four years or more.
- Non-invasive: No drilling, no anesthetic required.
- Cost-effective: Significantly cheaper than treating a cavity.
- Painless: The procedure is quick and comfortable.
- Safe: Materials are proven safe.
- Cons:
- Can chip or wear over time: May require reapplication or repair.
- Not suitable for existing cavities: If decay has progressed beyond incipient stage, a sealant cannot be placed.
- Cost Range in the US: $30 - $60 per tooth. Many dental insurance plans cover sealants for children.
2. Restoration: Dental Fillings (For Fissures with Existing Decay)
If a fissure has developed a cavity, it needs to be treated with a dental filling. The type of filling material will depend on the extent of the decay, location, esthetic concerns, and patient preference.
| Treatment Option | Description | Pros | Cons | Average Cost (US) |
|---|---|---|---|---|
| Composite (Resin) Filling | Tooth-colored material made of a plastic resin and finely ground glass particles. Bonded directly to the tooth. | Aesthetically pleasing (matches tooth color). Bonds to tooth structure, requiring less tooth removal. Versatile. | Can be less durable than amalgam in very large restorations. Can stain over time. More technique-sensitive for placement. Slightly higher cost. | $150 - $350 |
| Amalgam (Silver) Filling | A mixture of mercury, silver, tin, and copper. Durable and long-lasting. | Very durable and strong, especially for posterior teeth. Less expensive. Easier to place in moisture-controlled environments. | Not aesthetically pleasing (silver color). Does not bond to tooth structure (requires mechanical retention). Contains mercury (though deemed safe by ADA). | $100 - $250 |
| Glass Ionomer Cement (GIC) | Tooth-colored material that releases fluoride. Used for small, superficial cavities or temporary fillings, often in areas under less stress. | Releases fluoride, which can help prevent further decay. Bonds to tooth structure. Good for young children or temporary restorations. | Less strong and durable than composite or amalgam. More prone to wear. Not ideal for chewing surfaces under heavy stress. | $100 - $200 |
| Inlays/Onlays | Indirect restorations (made in a lab from composite, porcelain, or gold) used when the decay is too extensive for a simple filling but not severe enough for a crown. An inlay fits within the cusps, an onlay covers one or more cusps. | Very durable and long-lasting. Excellent fit and aesthetics (especially porcelain). Preserves more tooth structure than a crown. | More expensive. Requires two dental visits. | $700 - $1,500+ |
Cost Ranges in the US (with/without insurance): The costs listed above are general averages.
- With insurance: Coverage varies widely. Many plans cover 80-100% of sealants for children. For fillings, coverage typically ranges from 50-80% for basic restorative procedures after your deductible.
- Without insurance: You will pay the full cash price. Many dental practices offer payment plans or in-house discount programs.
- It's always best to get a specific treatment plan and cost estimate from your dentist, as prices can vary by location, dentist's fees, and the complexity of the procedure.
Step-by-Step: What to Expect During Treatment
1. Dental Sealant Application:
- Cleaning: The tooth surface is thoroughly cleaned to remove any plaque or food debris from the fissures.
- Isolation & Drying: The tooth is isolated with cotton rolls or a rubber dam to keep it dry, as moisture can interfere with the bonding process.
- Etching: An acidic gel (etchant) is applied to the chewing surface for a few seconds. This creates microscopic pores in the enamel, improving the bond of the sealant.
- Rinsing & Drying: The etchant is thoroughly rinsed off, and the tooth is carefully dried. It will appear chalky white if properly etched.
- Sealant Application: The liquid sealant material is painted directly into the fissures.
- Curing: A special curing light (blue light) is used to harden the sealant within seconds.
- Check & Adjust: The dentist will check the occlusion (how your teeth bite together) and make any necessary adjustments to ensure comfort.
2. Dental Filling Procedure (for Fissure Caries):
- Local Anesthetic: The dentist will typically administer a local anesthetic to numb the tooth and surrounding tissues, ensuring a pain-free experience.
- Decay Removal: Using a dental handpiece (drill), the dentist carefully removes all decayed tooth structure from the fissure and surrounding areas. The goal is to preserve as much healthy tooth structure as possible.
- Preparation: The tooth is prepared for the filling material. For composite fillings, an etchant and bonding agent are applied.
- Filling Placement: The chosen filling material (composite, amalgam, GIC) is placed into the prepared cavity.
- Shaping & Curing: If using composite or GIC, the material is shaped to mimic the natural contours of the tooth and then hardened with a curing light. Amalgam hardens on its own over a few hours.
- Polishing & Adjustment: The filling is polished, and the dentist checks your bite (occlusion) to ensure the filling is not too high and feels comfortable. Adjustments are made as needed.
Recovery Timeline and Aftercare
- Dental Sealants: There is no recovery period. You can eat and drink normally immediately after the procedure. You'll just need to continue your regular oral hygiene practices.
- Dental Fillings:
- Numbness: The local anesthetic will wear off within a few hours. Avoid chewing on the treated side until the numbness subsides to prevent accidentally biting your lip or cheek.
- Sensitivity: It's common to experience some sensitivity to hot, cold, or pressure for a few days to a few weeks after a filling, especially with deeper fillings. This usually resolves on its own. If sensitivity persists or worsens, contact your dentist.
- Pain: Mild discomfort is normal. Over-the-counter pain relievers can help. If you experience severe pain, pain when biting, or swelling, contact your dentist immediately.
- Aftercare: Maintain excellent oral hygiene (brushing twice daily, flossing once daily). Avoid very hard or sticky foods initially if advised by your dentist. Regular dental check-ups are essential to monitor the filling and overall oral health.
Prevention Strategies
Preventing fissure caries is far more effective and less invasive than treating them.
- Dental Sealants: This is the cornerstone of fissure decay prevention, particularly for children and adolescents shortly after their permanent molars and premolars erupt. Ask your dentist if sealants are right for you or your child.
- Excellent Oral Hygiene:
- Brush Twice Daily: Use a fluoride toothpaste and a soft-bristled brush. Pay special attention to the chewing surfaces of your back teeth, using small, circular motions.
- Floss Daily: While flossing targets between teeth, good overall hygiene helps reduce the bacterial load throughout the mouth.
- Fluoride Exposure:
- Use fluoride toothpaste.
- Drink fluoridated tap water if available.
- Discuss professional fluoride applications with your dentist, especially if you're at high risk for cavities.
- Healthy Diet:
- Limit sugary snacks and beverages (sodas, juices, candies).
- Reduce consumption of acidic foods and drinks (citrus, sports drinks).
- Eat a balanced diet rich in fruits, vegetables, and whole grains.
- Avoid frequent snacking to give your teeth time to recover from acid attacks.
- Regular Dental Check-ups and Cleanings:
- Visit your dentist at least every six months for professional cleanings and examinations. This allows for early detection of potential issues, monitoring of existing sealants, and reapplication if necessary. Your dentist can also identify high-risk fissures before decay even starts.
For Parents / Pediatric Considerations
Fissures are a particularly important topic for parents because children are at the highest risk for developing cavities in these areas.
- Timing of Sealants: The American Dental Association (ADA) recommends applying dental sealants to the chewing surfaces of permanent molars and premolars as soon as they erupt. This typically occurs around age 6 for the first molars and age 12 for the second molars. Sealing these teeth shortly after eruption provides maximum protection when their enamel is still maturing and most vulnerable.
- High Incidence of Decay: As mentioned, 80-90% of cavities in children and adolescents occur on the chewing surfaces of back teeth. This statistic alone underscores the critical importance of sealants.
- Ease of Application: The sealant procedure is ideal for children as it is non-invasive, quick, and comfortable, requiring no needles or drilling. This can also help children have positive early experiences at the dentist.
- Long-Term Benefits: Protecting children's permanent teeth with sealants can lead to a lifetime of fewer cavities, less dental pain, and lower dental costs. Parents should proactively discuss sealants with their pediatric dentist.
Frequently Asked Questions
Is fissure treatment painful?
The pain level associated with fissure treatment depends entirely on whether it's a preventive measure (like a sealant) or a restorative procedure (like a filling for a cavity).
- Dental Sealants: The application of a sealant is completely painless. It involves cleaning, etching, and painting the sealant onto the tooth, with no drilling or needles required.
- Dental Fillings: If decay is present and requires a filling, the procedure is typically performed under local anesthetic to numb the tooth. While you might feel some pressure, you should not feel any sharp pain during the removal of decay. Some mild sensitivity or discomfort after the anesthetic wears off is common but usually manageable with over-the-counter pain relievers.
How long does a dental sealant last?
Dental sealants are quite durable but are not permanent. They can last for several years, often 5 to 10 years, with good care. The Centers for Disease Control and Prevention (CDC) notes that sealants reduce the risk of caries by 80% for two years and continue to be effective for four years. They can sometimes last even longer. During regular dental check-ups, your dentist will inspect the sealants for any chips, wear, or signs of detachment and can easily repair or reapply them as needed.

Can fissures heal naturally?
No, fissures themselves are anatomical structures and do not "heal" in the way a wound on your skin would. If a fissure is healthy, it remains a potential risk area. If incipient decay (very early demineralization) has begun within a fissure but has not yet broken through the enamel surface, it can sometimes be remineralized with intense fluoride exposure and excellent oral hygiene. However, once a true cavity (a hole in the enamel) has formed, it will not heal on its own and requires professional intervention (a filling) to prevent further progression and protect the tooth.
Are fissures always a problem?
No, not all fissures are problematic, but they are always considered at-risk areas. Healthy fissures, especially those that are shallower or more V-shaped, may not develop decay if they are cleaned effectively and exposed to adequate fluoride. However, deep, narrow, or complex fissures are inherently difficult to clean and are therefore highly susceptible to decay, making them a significant dental health concern if not protected. Proactive measures like sealants help prevent them from becoming a problem.
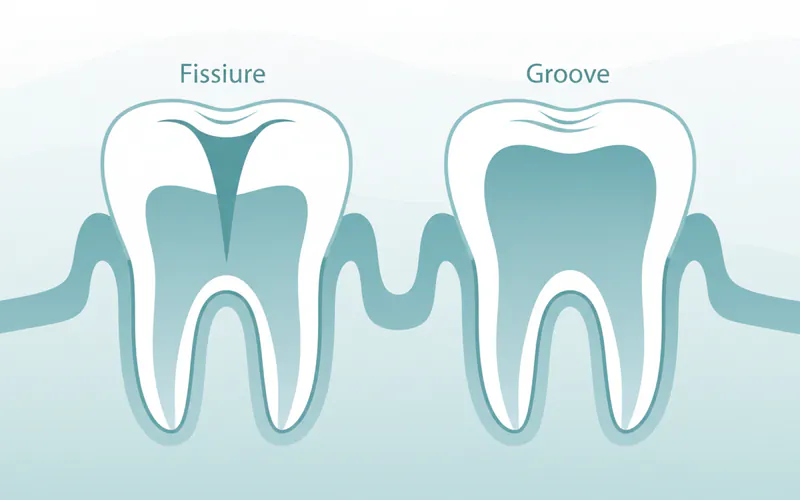
What is the difference between a fissure and a groove?
The terms "fissure" and "groove" are often used interchangeably, but in dentistry, they have distinct meanings that relate to their depth and clinical significance.
- Groove: A groove is a broader, shallower depression on the chewing surface of a tooth. Grooves are generally easier to clean with a toothbrush and are less prone to trapping food and bacteria, thus posing a lower risk for cavity development. They are a normal part of tooth anatomy.
- Fissure: A fissure is a very narrow, deep, and often intricate cleft or crevice. Their constricted opening and depth make them extremely difficult for toothbrush bristles to penetrate, leading to significant plaque retention and a high risk of caries. All teeth have grooves, but it's the specific morphology of a fissure that classifies it as high-risk.
Does insurance cover fissure sealants/fillings?
- Dental Sealants: Most dental insurance plans, particularly those for children, provide good coverage for dental sealants, often covering 80-100% of the cost. However, some plans may have age limits or frequency limitations. It's essential to check with your specific insurance provider.
- Dental Fillings: Dental insurance typically covers a portion of the cost of dental fillings, usually between 50-80%, depending on your plan's specifics, after your deductible is met. The coverage might also vary based on the type of filling material (e.g., some plans may cover amalgam fillings at a higher percentage than composite due to the latter being considered a "cosmetic" option, though this is changing). Always confirm your benefits with your insurance company before treatment.
What happens if a fissure cavity is left untreated?
Leaving a fissure cavity untreated allows the decay to progress unchecked.
- Enlargement of Cavity: The cavity will grow larger and deeper, destroying more tooth structure.
- Pain and Sensitivity: As decay reaches the dentin and then the pulp (the innermost part of the tooth containing nerves and blood vessels), you will likely experience increased pain, sensitivity to hot/cold, and pain when chewing.
- Infection: If decay reaches the pulp, it can lead to an infection (pulpitis), which can cause severe pain, swelling, and potentially an abscess (a pocket of pus).
- Root Canal Treatment: A severe infection might require root canal treatment to save the tooth.
- Tooth Loss: In the most severe cases, if the decay and infection are too extensive, the tooth may need to be extracted.
- Spread of Infection: An untreated dental infection can, in rare but serious cases, spread to other parts of the body, potentially leading to systemic health problems.
When to See a Dentist
Regular dental check-ups are the most crucial step in managing fissures and preventing related problems.
- Routine Care: Schedule regular dental examinations and cleanings at least every six months. This allows your dentist to monitor the health of your fissures, apply or repair sealants, and detect any early signs of caries before they become problematic.
- Signs of Decay: If you notice any of the signs of fissure decay, such as dark spots, visible holes, food trapping in a specific area, or new sensitivity to hot/cold/sweet, schedule an appointment promptly.
- Chipped or Lost Sealant: If you have sealants and notice that one has chipped, cracked, or completely come off, contact your dentist. It's important to repair or replace it to maintain protection.
- Pain or Discomfort: Any persistent tooth pain, especially when chewing or consuming hot/cold items, warrants a visit to the dentist. While not all pain indicates a fissure cavity, it always signals an underlying issue that needs professional evaluation.
By understanding the nature of fissures and taking proactive steps for prevention and early intervention, you can significantly safeguard your dental health and enjoy a lifetime of healthy, strong teeth.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.