Calcium Deposit Teeth: Complete Guide
Key Takeaways
- Did you know that 70% of adults aged 30 or older in the United States have some form of gum disease? Often, a primary contributing factor to this widespread issue is the accumulation of what many refer to as "calcium deposit teeth" – medically known as dental calculus or tartar. This hardened bu
Calcium Deposit Teeth: Complete Guide
Did you know that 70% of adults aged 30 or older in the United States have some form of gum disease? Often, a primary contributing factor to this widespread issue is the accumulation of what many refer to as "calcium deposit teeth" – medically known as dental calculus or tartar. This hardened buildup, far from being just a cosmetic nuisance, acts as a breeding ground for bacteria, relentlessly attacking your gums and teeth. If left unaddressed, these mineralized deposits can pave the way for serious oral health problems, including painful gum inflammation, persistent bad breath, and even tooth loss. Understanding the nature of these stubborn deposits, how they form, and crucially, how to prevent and remove them is paramount to maintaining a healthy smile and preventing more severe conditions like acid erosion of teeth from compounding the damage. This comprehensive guide will illuminate every facet of calcium deposits on your teeth, from their formation and identification to advanced treatment options, cost considerations, and essential preventive strategies, empowering you to safeguard your dental health.

Key Takeaways:
- What it is: "Calcium deposit teeth" primarily refers to dental calculus (tartar), hardened plaque made of mineralized bacteria and food debris. It cannot be removed by brushing or flossing alone.
- Causes: Poor oral hygiene, infrequent dental cleanings, specific dietary habits (sugary/acidic foods contributing to plaque), smoking, and individual saliva composition are key factors.
- Treatment: Professional dental scaling (manual or ultrasonic) is the only effective treatment. For subgingival deposits, root planing may also be necessary.
- Cost: A routine dental cleaning (prophylaxis) to remove supragingival calculus typically costs $75 - $200 without insurance. Scaling and root planing for deeper deposits can range from $200 - $600 per quadrant, totaling $800 - $2,400 for a full mouth.
- Prevention: Maintain diligent oral hygiene (brushing twice daily, flossing daily), use ADA-approved fluoride toothpaste, limit sugary and acidic foods, and schedule professional cleanings every 6 months.
- Timeline: Calculus can form within 24-72 hours if plaque is not removed. Once hardened, it requires professional intervention. Regular cleanings take 30-60 minutes. Scaling and root planing can take 1-2 hours per quadrant over multiple appointments.
What It Is / Overview
When people refer to "calcium deposit teeth," they are almost invariably talking about dental calculus, commonly known as tartar. This is a hard, calcified deposit that forms on the teeth and along the gum line. It's not the same calcium that strengthens your bones; rather, it's a hardened, mineralized form of dental plaque.
Dental plaque is a sticky, colorless film of bacteria that constantly forms on your teeth. It consists of bacteria, food particles, and saliva. If plaque isn't removed daily through effective brushing and flossing, it absorbs minerals from your saliva – primarily calcium and phosphate – and begins to harden. This hardening process, known as mineralization, transforms soft plaque into rigid calculus.
Once calculus forms, its porous, rough surface creates an ideal environment for more plaque to accumulate and flourish. This sticky plaque adheres more readily to calculus than to smooth enamel, creating a vicious cycle. The bacteria within the plaque and calculus release toxins that irritate the gums, leading to inflammation (gingivitis) and, if left untreated, more severe periodontal disease.
It's important to differentiate dental calculus from other, less common types of internal calcifications, such as pulp stones (denticles) which are small, calcified masses within the pulp chamber of a tooth. While these are also "calcium deposits," they are internal and typically not visible or directly related to the external deposits patients usually refer to. Our focus here will be on the external, problematic dental calculus.
Types / Variations
Dental calculus isn't a monolithic substance; its characteristics and location determine its classification and the approach to its removal. The two primary types are:
-
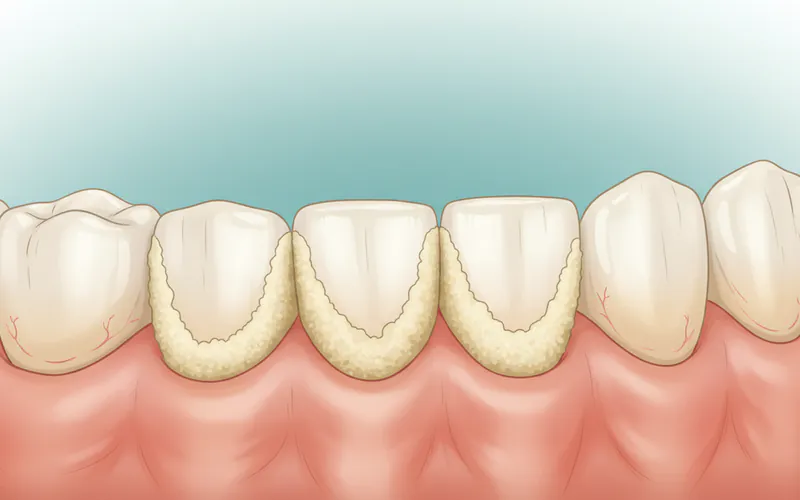
Supragingival Calculus:
- Location: This type forms above the gum line (supra-gingival). It's typically visible to the naked eye, though often mistaken for severe staining.
- Appearance: It can vary in color from white or creamy to yellow, brown, or even black. The darker colors are often due to staining from coffee, tea, tobacco, and certain foods, as well as chromogenic bacteria.
- Composition: Primarily consists of calcium phosphate, calcium carbonate, and magnesium phosphate, along with bacterial cells, salivary proteins, and food debris.
- Texture: Hard and rough, providing a retentive surface for more plaque to attach.
- Detection: Easily detected by dentists during a routine examination using an explorer tool.
- Impact: Contributes to gingivitis, bad breath (halitosis), and can progress to subgingival calculus if left untreated.
-
Subgingival Calculus:
- Location: This type forms below the gum line (sub-gingival), within the periodontal pockets that develop as gums pull away from the teeth due to inflammation.
- Appearance: Typically dark brown or black due to the presence of blood pigments from bleeding gums and degraded blood products. It's often denser and harder than supragingival calculus.
- Composition: Similar to supragingival calculus but with a higher proportion of calcium phosphate and magnesium phosphate, and less calcium carbonate. It also contains bacterial endotoxins.
- Texture: Very hard and firmly attached to the root surface.
- Detection: Cannot be seen directly but is detected by a dentist or dental hygienist using a periodontal probe and explorer, which can feel the roughness below the gum line. X-rays can also reveal larger subgingival deposits.
- Impact: This is the more dangerous type of calculus. Its presence irritates the gum tissue, perpetuates inflammation, and prevents the gums from reattaching properly to the tooth surface. It significantly contributes to the progression of periodontitis (advanced gum disease), leading to bone loss, gum recession, and eventually tooth mobility and loss.
While both types are mineralized plaque, their location and the specific challenges they present for removal are critical distinctions. Supragingival calculus is a precursor to subgingival calculus, highlighting the importance of early intervention and consistent oral hygiene.
Causes / Why It Happens
The formation of calcium deposit on tooth surfaces is a complex process influenced by a combination of oral hygiene practices, dietary choices, individual biology, and lifestyle factors. Understanding these causes is key to effective prevention.
-
Poor Oral Hygiene: This is the most significant contributing factor. When plaque isn't thoroughly removed from tooth surfaces and along the gum line through daily brushing and flossing, it remains undisturbed. Within 24 to 72 hours, if plaque isn't removed, it can start to absorb minerals from saliva and harden into calculus. Inadequate brushing technique, infrequent brushing, or neglecting to floss allows plaque to accumulate and mature into calculus.
-
Infrequent Dental Cleanings: Even with diligent home care, some plaque can be missed, particularly in hard-to-reach areas or tight spaces between teeth. Regular professional cleanings (typically every 6 months) are essential to remove any accumulated plaque and early calculus before it becomes extensive. If these cleanings are skipped, calculus will inevitably build up.
-
Dietary Habits:
- Sugary and Starchy Foods: A diet high in sugars and refined carbohydrates provides a feast for oral bacteria. These bacteria metabolize the sugars, producing acids and forming more plaque. The increased plaque then serves as the foundation for calculus formation.
- Acidic Foods and Drinks (Link to Acid Erosion of Teeth): While distinct from calculus formation, acid erosion of teeth can indirectly contribute. Frequent consumption of acidic beverages (soda, fruit juices, sports drinks) and acidic foods (citrus fruits, vinegar) softens and erodes tooth enamel. This creates a slightly rougher or demineralized surface on the enamel, which can make it easier for plaque to adhere more tenaciously. While acid doesn't directly cause calculus, the weakened, rougher enamel might become a more hospitable surface for initial plaque accumulation that subsequently calcifies. Additionally, a diet high in fermentable carbohydrates and acids can lead to a more acidic oral environment, which may alter the saliva composition in ways that influence plaque formation and calcification.
-
Saliva Composition: The unique mineral content and pH of an individual's saliva play a crucial role. Saliva is naturally supersaturated with calcium and phosphate ions, which are essential for remineralizing enamel. However, in some individuals, the concentration of these minerals is higher, or the pH makes them more readily available for plaque mineralization. People with naturally higher salivary pH tend to form calculus faster. Saliva can also contain proteins that promote bacterial aggregation and attachment, fostering plaque growth.
-
Genetics: Some individuals may be genetically predisposed to forming calculus more rapidly or having a more acidic oral environment. Research indicates that certain genetic markers might influence susceptibility to periodontal disease, which is directly linked to calculus.
-
Smoking and Tobacco Use: Tobacco products significantly increase the risk of plaque and calculus formation. Smoking impairs the immune system, reduces blood flow to the gums, and can alter saliva flow and composition. Smokers tend to have more subgingival calculus and are more prone to developing severe periodontal disease.
-
Certain Medications: Some medications can cause dry mouth (xerostomia) as a side effect. Reduced saliva flow means less natural rinsing action and buffering capacity, allowing plaque to accumulate more easily and potentially accelerate calculus formation.
-
Dental Anatomy and Restorations: Crowded teeth, misaligned teeth, or the presence of rough fillings, ill-fitting crowns, or partial dentures can create areas that are difficult to clean. These "plaque traps" become prime locations for calculus accumulation.
Pro Tip: Even if you brush regularly, pay close attention to the areas most prone to calculus buildup: the lingual (tongue side) surfaces of your lower front teeth and the buccal (cheek side) surfaces of your upper molars, as these areas are closest to your major salivary gland ducts.
Signs and Symptoms
Recognizing the signs of calcium deposit on tooth surfaces is crucial for early intervention. While some signs might be subtle, others are quite noticeable.
- Roughness on Tooth Surfaces: One of the most common initial signs you might feel with your tongue is a rough or grainy texture on your teeth, especially along the gum line. This indicates the presence of developing plaque or early calculus.
- Visible Deposits: As calculus hardens and accumulates, it becomes visibly noticeable. It can appear as white, yellow, brown, or even black deposits on the teeth, particularly along the gum line or between teeth.
- Persistent Bad Breath (Halitosis): The porous surface of calculus harbors millions of bacteria that release foul-smelling gases. If you notice chronic bad breath that doesn't resolve with brushing, calculus could be a major culprit.
- Inflamed, Swollen, or Red Gums: Calculus acts as a constant irritant to the gum tissue. This irritation leads to gingivitis, characterized by gums that are redder than usual, swollen, and tender to the touch. Healthy gums should be pink and firm.
- Bleeding Gums: Gums that bleed easily when you brush, floss, or even eat hard foods are a significant sign of gingivitis, almost always exacerbated by the presence of calculus. Healthy gums should not bleed.
- Gum Recession: Over time, the chronic inflammation caused by calculus can lead to the gums pulling away or receding from the teeth, exposing more of the tooth root. This makes teeth appear longer.
- Increased Tooth Sensitivity: Exposed tooth roots due to gum recession can lead to sensitivity to hot, cold, or sweet stimuli.
- Spaces Developing Between Teeth: As gum disease progresses due to calculus, bone loss can occur, leading to shifting teeth and new spaces or gaps.
- Loose Teeth: In advanced stages of periodontal disease, the bone supporting the teeth is severely compromised, causing teeth to become loose. This is a critical sign requiring immediate dental attention.
It's important to remember that early calculus may not cause pain, which is why regular dental check-ups are so important. By the time pain or severe sensitivity sets in, the condition may have advanced significantly.
Treatment Options
Once calcium deposit teeth (calculus) have formed, they cannot be removed by regular brushing or flossing. Professional dental intervention is necessary. The primary treatment revolves around various forms of dental scaling.
-
Professional Dental Cleaning (Prophylaxis):
- Description: This is the standard procedure for removing supragingival calculus and plaque from healthy gums or gums with mild gingivitis. It's typically performed by a dental hygienist.
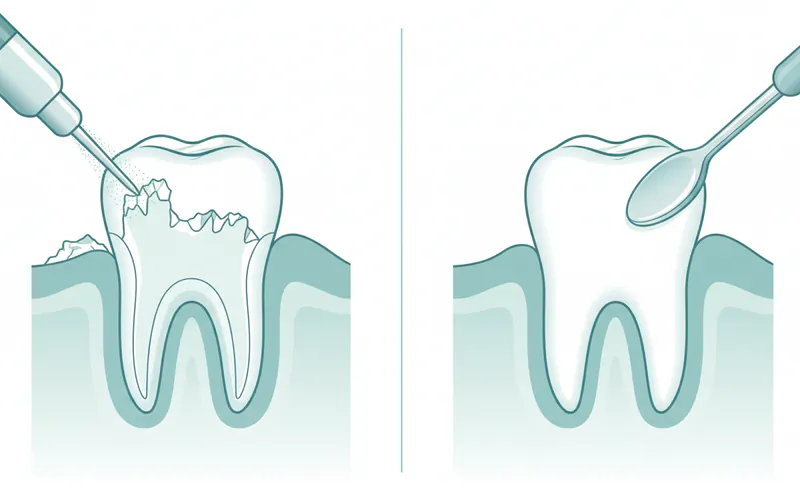
- Process: The hygienist uses specialized hand instruments (scalers and curettes) and/or ultrasonic scaling devices to dislodge and remove calculus from the tooth surfaces above the gum line. Following scaling, the teeth are polished to remove surface stains and smooth the enamel, making it harder for plaque to adhere.
- Pros: Non-invasive, relatively quick (30-60 minutes), prevents progression of gum disease, leaves teeth feeling clean and smooth.
- Cons: Only effective for supragingival calculus; does not address subgingival deposits or deep periodontal pockets.
- Anesthesia: Usually not required, though local anesthetic gel can be used for sensitive areas.
-
Scaling and Root Planing (Deep Cleaning):
- Description: This is a more intensive, non-surgical procedure for individuals with moderate to severe periodontitis, where subgingival calculus and inflammation are present, and periodontal pockets have formed.
- Process:
- Scaling: Involves meticulous removal of plaque, calculus, and bacterial toxins from tooth surfaces above and below the gum line, extending into the periodontal pockets. Both ultrasonic devices and hand scalers are used.
- Root Planing: After scaling, the root surfaces are smoothed (planed) to remove any remaining calculus, bacterial endotoxins, and to create a clean, smooth surface that discourages further bacterial attachment and allows the gum tissue to reattach more firmly.
- Pros: Effectively removes subgingival calculus, reduces gum inflammation, helps shrink periodontal pockets, and can halt the progression of gum disease. Often performed in quadrants over multiple appointments.
- Cons: More invasive than a routine cleaning, can cause temporary sensitivity, may require local anesthesia, and might be followed by some gum soreness.
- Anesthesia: Local anesthetic (injected numbing agent) is typically used to ensure patient comfort, especially for root planing, as it can reach sensitive areas.
-
Adjunctive Therapies (Often with Scaling and Root Planing):
- Antibiotics: For persistent infections or aggressive periodontitis, your dentist might prescribe oral antibiotics or apply localized antibiotic gels or chips directly into deep periodontal pockets after scaling and root planing.
- Antimicrobial Rinses: Prescription-strength antimicrobial mouthwashes (e.g., chlorhexidine) may be recommended for a short period to reduce bacterial load and promote healing.
- Laser Therapy: While not a primary treatment for calculus removal, dental lasers can sometimes be used as an adjunct to traditional scaling and root planing. They can help remove diseased tissue, sterilize pockets, and reduce inflammation. However, current ADA guidelines emphasize that lasers should not replace conventional scaling and root planing for calculus removal.
- Air Polishing (e.g., EMS Airflow): Uses a fine spray of air, water, and specialized powder (like erythritol or glycine) to remove biofilm, stains, and light, newly formed calculus, even in subgingival areas. It's very effective for biofilm management and can be less abrasive than traditional polishing.
-
Periodontal Surgery (for advanced cases):
- Description: If non-surgical treatments like scaling and root planing are insufficient to manage severe periodontitis with extensive bone loss and very deep pockets, surgical intervention may be necessary.
- Types: Procedures like flap surgery (gingival flap surgery), bone grafts, or guided tissue regeneration aim to access deeper calculus, reshape bone, or regenerate lost tissue.
- Pros: Can effectively treat advanced gum disease, reduce pocket depth, and potentially save teeth that would otherwise be lost.
- Cons: Invasive, longer recovery time, higher cost, potential for post-operative pain and sensitivity.
- Anesthesia: Local anesthetic, sometimes with sedation.
Comparison of Treatment Options for Calculus Removal
| Treatment Option | Primary Goal | Type of Calculus Addressed | Invasiveness | Anesthesia Required | Typical Duration (per session) |
|---|---|---|---|---|---|
| Professional Cleaning (Prophylaxis) | Remove plaque, supragingival calculus, stains | Supragingival (above gum line) | Low | Rarely | 30-60 minutes |
| Scaling & Root Planing (Deep Cleaning) | Remove plaque, subgingival calculus, endotoxins, smooth roots | Supragingival & Subgingival (below gum line) | Moderate | Yes (Local Anesthetic) | 1-2 hours (per quadrant) |
| Antibiotics / Antimicrobial Rinses | Reduce bacterial load, aid healing (adjunctive) | N/A (Targets bacteria, not calculus) | Low (Oral/Topical) | No | N/A (Prescription course) |
| Laser Therapy (Adjunctive) | Sterilize, remove diseased tissue, reduce inflammation | N/A (Assists SRP, doesn't remove calculus directly) | Low-Moderate | Often local anesthetic | Varies |
| Periodontal Surgery | Access deep calculus, reshape bone, regenerate tissue | Severe subgingival, bone defects | High | Yes (Local + Sedation) | Varies (1-Several hours) |
Step-by-Step Process: What to Expect During Treatment
Let's walk through what typically happens during a professional dental cleaning or a deep cleaning (scaling and root planing) to remove calcium deposit teeth.
For a Routine Dental Cleaning (Prophylaxis):
- Initial Examination: Your dental hygienist or dentist will first examine your mouth, checking for signs of gum inflammation, visible calculus, and assessing your overall oral health. They might use a small mirror and an explorer tool.
- Ultrasonic Scaling: An ultrasonic scaler, a device that emits high-frequency vibrations and a fine mist of water, is often used first. The vibrations gently break apart larger pieces of calculus, while the water spray flushes away debris. This process is generally comfortable, though you'll hear a buzzing sound and feel a cool mist.
- Hand Scaling: Following ultrasonic scaling, the hygienist will use specialized hand instruments (metal scalers and curettes) to meticulously remove any remaining smaller calculus deposits, particularly in tight spaces between teeth or just under the gum line, ensuring all surfaces are smooth.
- Polishing: Once all calculus is removed, a small, motorized brush with a gritty, fluoride-containing paste is used to polish your teeth. This removes surface stains and leaves your teeth feeling smooth and clean.
- Flossing: The hygienist will floss your teeth to remove any remaining polishing paste and check that all interdental areas are clean.
- Fluoride Treatment (Optional): Many routine cleanings conclude with a fluoride treatment (gel, foam, or varnish) to help strengthen enamel and prevent cavities.
- Final Check: Your dentist will often perform a final check of your teeth and gums, discuss any findings, and provide personalized oral hygiene advice.
For Scaling and Root Planing (Deep Cleaning):
- Local Anesthesia: Before starting, the dentist or hygienist will administer a local anesthetic to numb the specific areas of your mouth that will be treated. This ensures your comfort during the deeper cleaning procedure. They typically divide the mouth into quadrants (upper right, upper left, lower right, lower left) and treat one or two quadrants per appointment.
- Periodontal Probing: The hygienist will use a periodontal probe to measure the depth of your gum pockets around each tooth. This helps assess the severity of gum disease and guides the treatment.
- Ultrasonic Scaling (Subgingival): Similar to a routine cleaning, an ultrasonic scaler is used, but with a finer tip that can reach deeper into the periodontal pockets to break up and remove subgingival calculus. The water spray helps flush out bacteria and debris from these pockets.
- Hand Scaling (Subgingival): Specialized, curved hand scalers and curettes are then meticulously used to access and remove all remaining calculus and plaque from the root surfaces, deep within the gum pockets. This is a crucial and precise step.
- Root Planing: Once the calculus is removed, the root surfaces are carefully smoothed or "planed." This removes microscopic bacterial toxins and creates a clean, smooth surface that discourages bacteria from reattaching and promotes the reattachment of healthy gum tissue.
- Irrigation (Optional): Some practitioners may irrigate the pockets with an antimicrobial solution after scaling and root planing to further reduce bacterial load.
- Post-Treatment Instructions: You'll receive detailed instructions for aftercare, including managing sensitivity, medication if prescribed, and future follow-up appointments.
- Follow-up Appointments: Several weeks after scaling and root planing, you'll have a follow-up appointment to assess the healing of your gums and monitor pocket depths. Depending on your response, further treatment or a more frequent recall schedule (e.g., 3-4 month "perio maintenance" cleanings) may be recommended.
Cost and Insurance
Understanding the cost of treating calcium deposit teeth is essential, as prices can vary significantly based on the type of treatment, the severity of the condition, geographic location, and whether you have dental insurance. All prices listed are average ranges in the US and can fluctuate.
Routine Dental Cleaning (Prophylaxis)
- Average Cost (without insurance): $75 - $200.
- Low End: ~$75-$100 (Rural areas, dental schools, some corporate clinics).
- Mid-Range: ~$100-$150 (Most general dental practices in suburban areas).
- High End: ~$150-$200+ (Major metropolitan areas, specialist offices).
- Insurance Coverage: Most dental insurance plans cover 100% of routine cleanings (typically two per year) as a preventive service. This is often the most covered dental procedure.
Scaling and Root Planing (Deep Cleaning)
This procedure is typically billed per quadrant of the mouth. There are four quadrants: upper right, upper left, lower right, lower left.
- Average Cost (without insurance) per Quadrant: $200 - $600.
- Low End (per quadrant): ~$200-$300.
- Mid-Range (per quadrant): ~$300-$450.
- High End (per quadrant): ~$450-$600+.
- Total Cost for Full Mouth (4 Quadrants): $800 - $2,400.
- Insurance Coverage: Most dental insurance plans cover a significant portion of scaling and root planing, usually 50% to 80% after your deductible is met. However, there may be waiting periods or limitations on how often it's covered.
Other Potential Costs (Adjunctive Therapies)
- Localized Antibiotic Placement (e.g., Arestin): $50 - $100 per site (a "site" refers to an individual deep pocket). Insurance coverage varies.
- Antimicrobial Mouthrinses (Prescription): $20 - $50 per bottle. Usually not covered by dental insurance, may be by medical.
- Periodontal Maintenance Cleanings: After scaling and root planing, patients often require more frequent cleanings (every 3-4 months). These may be billed differently than a standard prophylaxis, often $120 - $300 per visit, and insurance coverage can vary between 50-80%.
Cost Variation Factors:
- Location: Major cities typically have higher costs due to overhead.
- Dentist vs. Specialist: Periodontists (gum specialists) may charge slightly more than general dentists for deep cleanings, but their expertise can be invaluable for complex cases.
- Technology Used: Use of advanced lasers or specific air polishing systems might slightly increase costs.
- Severity of Buildup: More extensive or stubborn calculus will require more time and effort, potentially impacting the final bill.
Insurance Details:
- Deductibles: Many plans have an annual deductible (e.g., $50-$100) that you must pay before your insurance starts covering services.
- Annual Maximums: Most dental insurance plans have an annual maximum benefit (e.g., $1,000 - $2,000) that they will pay out per year. If your treatment costs exceed this, you are responsible for the remainder.
- Waiting Periods: Some plans have waiting periods (e.g., 3-6 months) for major procedures like scaling and root planing.
- Pre-authorization: For more extensive treatments like scaling and root planing, your dentist may submit a pre-treatment estimate to your insurance company to clarify coverage beforehand.
Pro Tip: Always clarify with your dental office and your insurance provider exactly what procedures will be performed and what your out-of-pocket costs will be before starting treatment. Many offices offer payment plans or third-party financing options (like CareCredit) to help manage costs.
Recovery and Aftercare
After having calcium deposit teeth removed, especially after a deep cleaning (scaling and root planing), proper recovery and diligent aftercare are essential for healing and preventing recurrence.

Immediate Post-Treatment (First 24-48 hours):
- Sensitivity: It's common to experience increased tooth sensitivity to hot, cold, or pressure, particularly after root planing where root surfaces are exposed. This usually subsides within a few days to weeks.
- Management: Use toothpaste for sensitive teeth, avoid very hot or cold foods/drinks, and avoid aggressive brushing.
- Gum Soreness/Tenderness: Your gums may feel sore, tender, or even slightly swollen. This is normal as the tissues heal from inflammation and the procedure.
- Management: Over-the-counter pain relievers (e.g., ibuprofen, acetaminophen) can help. A warm salt water rinse (1/2 tsp salt in 8 oz warm water) 2-3 times a day can soothe gums and promote healing.
- Bleeding: Minor bleeding from the gums might occur for a few hours.
- Management: Avoid vigorous rinsing or spitting immediately after the procedure. If bleeding persists, apply firm but gentle pressure with a clean piece of gauze.
- Numbness: If local anesthesia was used, your mouth will be numb for several hours. Be careful not to bite your cheek or tongue, and avoid eating until the numbness wears off.
- Diet: Stick to soft, non-acidic foods for the first day or two. Avoid crunchy, sticky, spicy, or extremely hot/cold foods.
Ongoing Aftercare and Long-Term Maintenance:
- Excellent Oral Hygiene: This is the most critical aspect of preventing calculus from returning.
- Brushing: Brush thoroughly twice a day for at least two minutes with a soft-bristled brush and an ADA-approved fluoride toothpaste. Focus on cleaning along the gum line. Consider an electric toothbrush for enhanced plaque removal.
- Flossing: Floss daily to remove plaque and food particles from between your teeth and under the gum line, areas your toothbrush can't reach.
- Mouthwash: An antiseptic mouthwash (e.g., chlorhexidine, if prescribed, or an over-the-counter therapeutic rinse) can help reduce bacteria, but it's not a substitute for brushing and flossing.
- Regular Dental Visits: Adhere to your dentist's recommended schedule for follow-up appointments. After a deep cleaning, you will likely need more frequent "periodontal maintenance" cleanings (e.g., every 3-4 months) to monitor gum health, remove new plaque/calculus, and prevent recurrence of gum disease.
- Dietary Choices: Limit your intake of sugary and starchy foods and drinks, which feed plaque-forming bacteria. Reduce consumption of acidic beverages and foods, which can contribute to acid erosion of teeth and make enamel rougher, potentially accelerating plaque accumulation.
- Avoid Tobacco Products: Smoking and chewing tobacco significantly increase the risk of calculus formation and gum disease progression. Quitting tobacco is one of the best things you can do for your oral health.
- Monitor for Symptoms: Be vigilant for any signs of returning gum inflammation, sensitivity, or bad breath, and report them to your dentist promptly.
By diligently following these aftercare instructions, you can significantly prolong the positive effects of your dental treatment and maintain healthy gums and teeth.
Prevention
Preventing calcium deposit teeth is largely about consistent, effective oral hygiene and healthy lifestyle choices. Since calculus forms from hardened plaque, the goal is to remove plaque before it can mineralize.
-
Brush Twice Daily with Fluoride Toothpaste:
- Technique: Use a soft-bristled toothbrush (manual or electric) and angle the bristles at a 45-degree angle to the gum line. Use gentle, circular motions, covering all tooth surfaces – outer, inner, and chewing surfaces.
- Duration: Brush for at least two minutes each time. Many electric toothbrushes have built-in timers.
- Fluoride: Use an ADA-approved fluoride toothpaste. Fluoride strengthens enamel, making it more resistant to acid attacks and decay, and helps in the remineralization process.
- Replace Brush: Change your toothbrush or brush head every 3-4 months, or sooner if the bristles are frayed.
-
Floss Daily:
- Purpose: Flossing is crucial for removing plaque and food particles from between your teeth and beneath the gum line, areas your toothbrush cannot effectively reach. These are prime spots for calculus formation.
- Technique: Use about 18 inches of floss, winding most of it around your middle fingers. Guide the floss between your teeth, curving it into a C-shape against each tooth surface, and gently slide it under the gum line. Move the floss up and down several times before moving to the next tooth.
-
Use an Antimicrobial Mouthwash (Optional but Recommended):
- An ADA-accepted therapeutic mouthwash can help reduce plaque and gingivitis-causing bacteria. Look for rinses containing ingredients like cetylpyridinium chloride (CPC) or essential oils.
- Note: Mouthwash is an adjunct, not a substitute for brushing and flossing.
-
Limit Sugary and Starchy Foods and Drinks:
- Sugars and refined carbohydrates are the primary food source for plaque-forming bacteria. Reducing their intake means less plaque production.
- Pro Tip: If you do consume sugary snacks or drinks, rinse your mouth with water afterward to help wash away sugars and acids.
-
Be Mindful of Acidic Foods and Beverages (Prevent Acid Erosion of Teeth):
- While not directly causing calculus, frequent consumption of acidic items (sodas, fruit juices, sports drinks, citrus fruits, vinegar) can soften enamel, leading to acid erosion of teeth. This roughens the tooth surface, potentially making it easier for plaque to adhere and subsequently calcify.
- Prevention: Consume acidic items in moderation, preferably with meals. Use a straw for acidic drinks to minimize contact with teeth. Wait at least 30 minutes after consuming acidic foods before brushing, as enamel is temporarily softened and more susceptible to abrasion.
-
Regular Professional Dental Cleanings:
- Schedule professional cleanings and check-ups every six months, or more frequently if recommended by your dentist (e.g., 3-4 months for those prone to calculus or with a history of gum disease).
- Dental professionals can remove plaque and calculus you've missed, identify early signs of problems, and provide personalized advice.
-
Avoid Tobacco Products:
- Smoking and other tobacco use dramatically increase the risk of calculus formation and gum disease. Quitting tobacco is one of the most impactful steps you can take for your oral and overall health.
-
Drink Plenty of Water:
- Water helps rinse away food particles and bacteria, especially after meals, and supports healthy saliva flow.
By integrating these preventive measures into your daily routine, you can significantly reduce the risk of developing calcium deposit teeth and maintain optimal oral health.
Risks and Complications
Failing to address calcium deposit teeth can lead to a cascade of increasingly severe oral health problems, often impacting overall systemic health as well.
- Gingivitis: This is the earliest and mildest form of gum disease. Calculus accumulation along the gum line irritates the gum tissue, leading to inflammation characterized by redness, swelling, and bleeding during brushing or flossing. Gingivitis is reversible with professional cleaning and improved oral hygiene.
- Periodontitis (Gum Disease): If gingivitis is left untreated, the inflammation progresses, and the calculus spreads below the gum line (subgingival calculus). The bacteria and toxins trapped in these deposits cause the gums to pull away from the teeth, forming "periodontal pockets." The immune system's response to this chronic infection starts to break down the bone and connective tissue that support the teeth.
- Consequences: Deepening pockets, chronic inflammation, bone loss, gum recession, increased tooth sensitivity, persistent bad breath.
- Tooth Decay (Cavities): While calculus itself doesn't directly cause cavities, its porous surface creates an ideal environment for plaque bacteria to thrive. These bacteria produce acids that demineralize tooth enamel, leading to cavities. Calculus also makes it harder to clean tooth surfaces effectively, increasing decay risk.
- Tooth Mobility and Loss: In advanced periodontitis, significant bone loss occurs around the teeth, weakening their support structure. This can lead to teeth becoming loose, shifting, and eventually falling out or requiring extraction.
- Halitosis (Persistent Bad Breath): The bacteria within calculus produce volatile sulfur compounds (VSCs) that are the primary cause of chronic bad breath. This can significantly impact social interactions and self-confidence.
- Aesthetic Concerns: Visible calculus deposits can be unsightly, discolored, and detract from the appearance of your smile.
- Systemic Health Connections: The chronic inflammation and bacterial load associated with gum disease (fueled by calculus) are linked to several serious systemic health conditions.
- Cardiovascular Disease: Bacteria from infected gums can enter the bloodstream, contributing to inflammation and plaque buildup in arteries.
- Diabetes: There's a bidirectional relationship; gum disease can make it harder to control blood sugar, and poorly controlled diabetes can worsen gum disease.
- Respiratory Diseases: Inhaling bacteria from infected gums can exacerbate conditions like pneumonia.
- Adverse Pregnancy Outcomes: Gum disease has been linked to preterm birth and low birth weight.
- Other Conditions: Links have also been suggested with rheumatoid arthritis, certain cancers, and cognitive decline.
These risks underscore why timely removal of calculus and ongoing preventive measures are not merely cosmetic but are fundamental to maintaining not just your oral health, but your overall well-being.
Children / Pediatric Considerations
While calculus is more prevalent in adults, calcium deposit on tooth surfaces can certainly occur in children, sometimes even as early as toddlerhood. Pediatric dentists are keenly aware of these issues, and parents play a vital role in prevention and early detection.
Why Calculus Forms in Children:
- Inadequate Brushing and Flossing: Children may lack the dexterity or motivation for thorough oral hygiene. Areas often missed include the inner surfaces of lower front teeth and the chewing surfaces of molars.
- Dietary Habits: Frequent consumption of sugary snacks, juices, and soft drinks, common in childhood, provides ample fuel for plaque bacteria.
- Saliva Composition: Some children naturally have saliva with a higher mineral content, making them more prone to calculus formation.
- Orthodontic Appliances: Braces, retainers, and other orthodontic devices create more surfaces and traps for plaque, making meticulous cleaning crucial.
- Developing Habits: The early years are critical for establishing good oral hygiene habits. If not instilled early, calculus can become a recurring problem.
Signs to Look For in Children:
- Visible white, yellow, or brown deposits on the teeth, especially near the gum line.
- Red, swollen, or bleeding gums when brushing.
- Persistent bad breath.
- Reluctance to brush due to gum tenderness.
Age-Specific Guidance for Parents:
- Infants (0-12 months): Wipe gums with a soft, damp cloth or gauze after feedings. Start brushing with a tiny smear of fluoride toothpaste (rice grain size) when the first tooth erupts.
- Toddlers (1-3 years): Use a soft-bristled toothbrush and a rice-grain-sized amount of fluoride toothpaste. Parents should brush their child's teeth twice daily.
- Preschoolers (3-6 years): Use a pea-sized amount of fluoride toothpaste. Parents should continue to supervise and assist with brushing, ensuring all surfaces are cleaned. Introduce flossing when teeth touch each other.
- School-Aged Children (6+ years): Children can start to brush and floss more independently, but continued supervision is recommended until around age 8-10, or until they demonstrate good technique. Emphasize thoroughness.
- Teenagers: Often a period of decreased oral hygiene and increased consumption of sugary drinks. Reinforce the importance of brushing, flossing, and regular dental visits, especially if they have braces.
Treatment for Children:
- Professional Cleanings: Just like adults, children need regular dental check-ups and cleanings, typically every six months, starting from their first birthday or when their first tooth erupts. Pediatric dentists are skilled at making these visits comfortable and educational for children.
- Education: Dental hygienists and dentists will educate children and parents on proper brushing and flossing techniques.
- Fluoride Treatments & Sealants: These preventive measures are particularly important in children to strengthen enamel and protect against decay, especially when calculus is present or a risk.
Pro Tip for Parents: Make oral hygiene a fun and consistent routine. Use colorful toothbrushes, flavored toothpaste, and brush alongside your child. Lead by example and reinforce positive habits to prevent the early onset of calculus and associated dental problems.
Cost Breakdown
A detailed breakdown of the costs associated with addressing calcium deposit teeth is crucial for patients in the US. These figures are average ranges and can vary by region, practitioner, and specific case complexity.
1. Routine Dental Cleaning (Prophylaxis - D1110)
- Description: For healthy mouths with minimal to moderate supragingival calculus.
- Average US Cost (without insurance):
- Low: $75
- Mid: $125
- High: $200
- With Insurance: Typically covered at 100% (0% out-of-pocket) by most PPO plans, usually twice a year. Some HMO/DMO plans may have a small co-pay (e.g., $10-$20).
2. Scaling and Root Planing (Deep Cleaning - D4341 for 4+ teeth per quadrant, D4342 for 1-3 teeth per quadrant)
- Description: For moderate to severe periodontitis with subgingival calculus, bone loss, and periodontal pockets. Billed per quadrant.
- Average US Cost (without insurance) PER QUADRANT:
- Low: $200
- Mid: $350
- High: $600+
- Average US Cost (without insurance) FOR FULL MOUTH (4 Quadrants):
- Low: $800
- Mid: $1,400
- High: $2,400+
- With Insurance: Generally covered at 50% - 80% after deductible. A full mouth deep cleaning could still mean $400 - $1,200+ out-of-pocket. May be subject to waiting periods or annual maximums.
3. Periodontal Maintenance (D4910)
- Description: Follow-up cleanings for patients who have undergone scaling and root planing, typically every 3-4 months. More extensive than a routine cleaning but less than deep cleaning.
- Average US Cost (without insurance):
- Low: $120
- Mid: $180
- High: $300
- With Insurance: Coverage varies widely. Some plans cover it as a routine cleaning (100%), others at a lower percentage (50-80%), or only allow 2 per year. It's crucial to check with your specific plan.
4. Adjunctive Therapies (Costs vary widely by specific product/service)
- Localized Antimicrobial Agent (e.g., Arestin - D4381):
- Average US Cost (without insurance): $50 - $100 per site (individual deep pocket).
- With Insurance: Often covered, but subject to specific criteria and limitations.
- Prescription Mouthrinses (e.g., Chlorhexidine):
- Average US Cost (without insurance): $20 - $50 per bottle.
- With Insurance: Rarely covered by dental insurance; sometimes covered by medical insurance if prescribed for a specific medical condition.
Payment Plans and Financing Options
- In-Office Payment Plans: Many dental offices offer flexible payment plans, allowing patients to pay in installments. These are usually interest-free for a short period.
- Third-Party Financing: Companies like CareCredit, LendingClub Patient Solutions, or Alphaeon Credit offer specialized healthcare financing. They provide credit lines for medical and dental expenses, often with interest-free promotional periods if paid in full within a certain timeframe.
- Dental Discount Plans: These are not insurance but offer a reduced fee for services at participating dentists. You pay an annual membership fee and then receive a discount (e.g., 10-50%) on various procedures.
- Dental Schools: Dental schools often offer treatments at a significantly reduced cost, as procedures are performed by students under the close supervision of experienced faculty.
Cost-Saving Tips
- Prioritize Prevention: The most cost-effective approach is preventing calculus formation through excellent daily oral hygiene and regular routine cleanings.
- Utilize Insurance Benefits: Understand your dental insurance plan thoroughly, including deductibles, annual maximums, and covered percentages for various procedures.
- Get a Pre-Treatment Estimate: For any non-routine procedure, ask your dentist to submit a pre-treatment estimate to your insurance company. This provides a clear understanding of your out-of-pocket costs before treatment begins.
- Shop Around: For significant procedures, you can get quotes from a few different dental offices, keeping in mind that the cheapest option isn't always the best in terms of quality of care.
- Ask About Cash Discounts: Some dental offices offer a discount for patients who pay in full at the time of service with cash.
By being proactive and informed, you can manage the costs associated with treating and preventing calcium deposit teeth effectively.
Frequently Asked Questions
What is the difference between plaque and calculus (tartar)?
Plaque is a soft, sticky, colorless film of bacteria that constantly forms on your teeth. If plaque is not removed daily through brushing and flossing, it can absorb minerals from your saliva and harden into calculus, also known as tartar. Calculus is a hard, calcified deposit that can only be removed by a dental professional.
Can I remove calcium deposits (tartar) myself at home?
No, you cannot safely or effectively remove calculus (tartar) at home. Once plaque has hardened into calculus, it adheres firmly to the tooth surface and requires specialized dental instruments to remove. Attempting to scrape it off yourself can damage your enamel, gums, or even lead to infection.
Is calculus painful?
Calculus itself is usually not painful, but the issues it causes can be. The bacteria in calculus irritate your gums, leading to inflammation (gingivitis), which can cause tenderness, swelling, and bleeding. If gingivitis progresses to periodontitis, it can cause gum recession, tooth sensitivity, and eventually painful tooth mobility.

How long does it take for calcium deposits to form?
Plaque begins to form on teeth immediately after cleaning. If not removed, it can start to harden into calculus within 24 to 72 hours. The speed of formation varies among individuals due to factors like saliva composition and oral hygiene habits.
What is the cost of removing calcium deposits?
The cost depends on the type and severity of the deposits. A routine cleaning (prophylaxis) to remove supragingival calculus typically costs $75-$200 without insurance. If deep deposits and gum disease are present, scaling and root planing (deep cleaning) can cost $200-$600 per quadrant, or $800-$2,400 for a full mouth, without insurance. Insurance often covers a significant portion.
Does dental insurance cover the removal of calcium deposits?
Yes, most dental insurance plans cover routine cleanings (prophylaxis) at 100% as a preventive measure, usually twice a year. For more extensive scaling and root planing, coverage typically ranges from 50% to 80% after your deductible, subject to annual maximums and potential waiting periods.
Can calcium deposits lead to tooth loss?
Yes, if left untreated, significant calculus buildup leads to periodontitis, a severe form of gum disease. This chronic infection destroys the bone and connective tissue supporting your teeth, causing them to loosen and eventually fall out or require extraction.
Are there any alternatives to professional cleaning for removing calculus?
No. While maintaining excellent oral hygiene (brushing, flossing, mouthwash) can prevent calculus formation, there are no effective or safe alternatives to professional dental scaling for removing existing calculus. Herbal remedies, specialized toothpastes, or home kits cannot remove hardened calculus.
Does acid erosion of teeth contribute to calcium deposits?
While acid erosion of teeth directly dissolves enamel and is distinct from calculus, it can indirectly contribute. Eroded enamel can become rougher, making it easier for plaque to adhere to the tooth surface. This increased plaque adherence can then accelerate the process of mineralization into calculus if oral hygiene is not meticulous.
What should I do if my gums bleed after a cleaning for calculus?
Some mild bleeding and soreness are normal for a day or two after a professional cleaning, especially after a deep cleaning. If bleeding persists or is excessive, contact your dental office. Continue gentle brushing and flossing, and rinse with warm salt water to aid healing.
When to See a Dentist
Recognizing when to seek professional dental care for calcium deposit teeth is crucial for maintaining your oral health and preventing more severe complications.
Schedule a Routine Appointment If You Notice:
- Visible Deposits: You can see yellowish, brownish, or dark deposits on your teeth, especially near the gum line, that don't come off with regular brushing.
- Rough Texture: You feel a rough or grainy texture on your teeth with your tongue, even after brushing.
- Persistent Bad Breath: You experience chronic bad breath that doesn't improve with brushing and flossing.
- Slightly Red or Swollen Gums: Your gums appear redder or a bit puffy, indicating early gingivitis.
- Minor Gum Bleeding: Your gums bleed occasionally when you brush or floss, but it's not severe or constant.
- It's Been More Than Six Months: Even without noticeable symptoms, the American Dental Association (ADA) recommends professional check-ups and cleanings every six months for most adults to remove plaque and calculus and catch problems early.
Seek Dental Attention Promptly (Within a Few Days) If You Experience:
- Consistent Gum Bleeding: Your gums bleed regularly and easily, even with gentle brushing or flossing, or spontaneously.
- Significant Gum Swelling or Tenderness: Your gums are noticeably swollen, bright red, or painful to the touch.
- Receding Gums: You notice your gums pulling away from your teeth, making your teeth appear longer.
- Increased Tooth Sensitivity: You experience new or worsening sensitivity to hot, cold, or sweet foods/drinks.
- New Gaps Between Teeth: You notice new spaces or shifting between your teeth.
Seek Emergency Dental Care Immediately (Within 24 Hours) If You Have:
- Severe, Unrelenting Pain: Intense toothache or gum pain that doesn't subside with over-the-counter pain relievers.
- Loose Teeth: One or more of your permanent teeth feel noticeably loose. This is a sign of advanced bone loss.
- Pus Around Teeth or Gums: You see pus oozing from between your teeth and gums, indicating a serious infection (abscess).
- Abscess Formation: Swelling on your gums, jaw, or face, potentially accompanied by fever.
- Difficulty Chewing or Swallowing: Pain or discomfort that interferes with eating.
Never ignore persistent signs of gum disease or calculus buildup. Early detection and treatment are paramount to preventing the progression of dental issues and safeguarding your overall health. Your dental professional is your best resource for personalized advice and care.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

What Are Calcium Deposits on Teeth
Are you one of the millions of Americans who notices a stubborn, yellowish buildup on your teeth despite regular brushing? You're likely experiencing what many refer to as "calcium deposits on teeth." This common dental concern, medically known as dental calculus or tartar, affects a vast ma
February 23, 2026

Calcium Good for Teeth: Complete Guide
More than 99% of your body's calcium resides in your bones and teeth, making it an undeniable cornerstone of skeletal and oral health. But did you know that an estimated 42% of American adults don't get enough calcium from their diet? This staggering statistic underscores a critical question
February 23, 2026

What Do Bulimia Teeth Look Like
"Bulimia teeth" refers to the specific and often severe damage that the self-induced vomiting characteristic of bulimia nervosa inflicts on a person's oral health. It's a critical issue, affecting approximately 1.5% of women and 0.5% of men in the US at some point in their lives, with many more
February 23, 2026

Erosion in Teeth: Complete Guide
Erosion in Teeth: Complete Guide
February 23, 2026