Canine
4,515 words · 15 min read
Quick Definition
The pointed teeth located at the corners of the dental arches, designed for tearing food. Also called cuspids or eye teeth, there are four canines in a full adult dentition.
Canine: The Cornerstone Teeth of Your Smile
The term canine in dentistry refers to the pointed, cone-shaped teeth located at the corners of your dental arches. Designed with a single, strong cusp (point), these robust teeth are perfectly adapted for tearing and shredding food, playing a critical role in the initial stages of digestion. Known universally as cuspids due to their cusp-like shape, or colloquially as eye teeth because of their alignment with the eyes, canines are among the most stable and crucial teeth in the human mouth.

A full adult dentition typically includes four canines: one in each quadrant of the mouth – upper right, upper left, lower right, and lower left. These teeth are not just about function; they are vital for maintaining the structure and aesthetics of your smile. They serve as a transition between the flatter front incisors and the broader back molars, guiding your bite and supporting your facial structure. Issues with canines, such as improper eruption or impaction, can lead to significant dental health problems, affecting chewing efficiency, speech, and the alignment of other teeth. Canine impaction, where a permanent canine fails to erupt into its proper position, affects approximately 1-3% of the population, making it a common concern that often requires dental intervention. Understanding the canine's role and potential issues is fundamental to maintaining optimal oral health.
Key Takeaways:
- Canines are the pointed "cornerstone" teeth designed for tearing food.
- Also known as cuspids or eye teeth, there are four in a complete adult set.
- They are crucial for chewing, guiding the bite, and maintaining facial aesthetics.
- Canines are part of the anterior teeth group, bridging incisors and premolars.
- A common issue is canine impaction, where the tooth fails to erupt properly, affecting 1-3% of individuals.
- Early detection and treatment of canine problems are vital for long-term dental health.
Detailed Explanation of Canines
Canines are fascinating teeth, not just for their distinct shape and function, but also for their complex developmental journey and potential for issues. This section delves into every aspect of these essential teeth.
Types and Classifications
Canines are classified based on their location and developmental stage:
- Maxillary Canines (Upper Canines): Located in the upper jaw, these are often considered the most important canines clinically. They are typically longer and more prominent than their mandibular counterparts. Maxillary canines play a significant role in facial aesthetics and are the teeth most commonly affected by impaction.
- Mandibular Canines (Lower Canines): Situated in the lower jaw, these are generally narrower and less prone to impaction compared to maxillary canines. They still contribute significantly to the tearing function and maintain the integrity of the lower dental arch.
- Primary Canines (Deciduous Canines): Also known as "baby teeth," these erupt around 16-22 months of age. They serve the same functional role as permanent canines until they naturally exfoliate (fall out) to make way for their permanent successors.
- Permanent Canines: These begin to erupt around 11-12 years of age for upper canines and 9-10 years for lower canines, making them one of the last permanent teeth to emerge. Their late eruption timing can sometimes contribute to impaction issues if there isn't enough space in the dental arch.
Canines are also grouped as anterior teeth, which includes the incisors (central and lateral) and the canines themselves. These front teeth are primarily responsible for biting, tearing, and initial food processing, as well as influencing speech and facial appearance.
Causes and Risk Factors for Canine Issues
While canines are naturally strong, they are particularly susceptible to certain developmental problems, with impaction being the most prevalent. Canine impaction occurs when the tooth is prevented from erupting into its normal position within the dental arch. Several factors can contribute to this:
- Genetic Predisposition: Studies suggest a hereditary component, with a higher incidence of impaction in certain families. Some genetic syndromes can also increase the risk.
- Arch-Length Discrepancy (Crowding): The most common cause. If the jaw is too small to accommodate all permanent teeth, the canine, being one of the last to erupt, often loses its space and becomes impacted. This crowding can be exacerbated by premature loss of primary teeth or retained primary teeth.
- Retained Primary Canine: If the primary canine doesn't exfoliate (fall out) on time, it can block the path of the permanent canine, forcing it into an abnormal eruption trajectory or causing it to become stuck.
- Ankylosis of Primary Canine: In rare cases, the primary canine may fuse to the jawbone, preventing its natural exfoliation and obstructing the permanent canine.
- Presence of Supernumerary Teeth: Extra teeth (supernumerary teeth) in the area can physically block the eruption path of the permanent canine.
- Odontomas or Cysts: Benign tumors or fluid-filled sacs in the jawbone can obstruct eruption.
- Abnormal Eruption Path: The permanent canine might simply develop at an incorrect angle, causing it to collide with the roots of adjacent teeth or get trapped in the palate (roof of the mouth) or buccal plate (cheek side of the jaw).
- Trauma: Injury to the jaw or primary teeth during development can sometimes disrupt the permanent tooth bud.
Prevalence: Canine impaction is relatively common, affecting approximately 1% to 3% of the general population, with a slightly higher incidence in females and often occurring unilaterally (on one side). Palatal impaction (impaction towards the roof of the mouth) is far more common than buccal impaction (impaction towards the cheek).
Signs and Symptoms to Watch For
Recognizing the signs of potential canine problems, especially impaction, is crucial for timely intervention.
- Missing Permanent Canine: The most obvious sign is the absence of a permanent canine by the expected eruption age (around 11-12 years for upper canines). If the primary canine is still present and the permanent one hasn't appeared, it's a red flag.
- Prolonged Retention of Primary Canine: If a child's primary canine remains in place past the age of 13-14 years without the permanent canine emerging, it strongly suggests impaction.
- Visible Bulge on the Gum: Sometimes, an impacted canine might cause a palpable or visible bulge on the gum tissue (either on the palate or the cheek side) as it attempts to erupt.
- Asymmetry of Eruption: If the canine on one side has erupted, but its counterpart on the other side has not, it warrants investigation.
- Tilting or Crowding of Adjacent Teeth: An impacted canine can put pressure on neighboring teeth (like the lateral incisor), causing them to tip, splay, or become crowded.
- Pain or Discomfort: While many impacted canines are asymptomatic, some can cause localized pain, tenderness, or pressure.
- Root Resorption of Adjacent Teeth: In severe cases, an impacted canine can press against the roots of neighboring teeth, causing their roots to dissolve (resorb), which can lead to tooth loss if untreated.
Diagnosis Process — What Your Dentist Does
Diagnosing an impacted canine or other canine-related issues typically involves a combination of clinical examination and radiographic imaging:

-
Clinical Examination:
- Your dentist will physically examine your mouth, checking for the presence of primary canines beyond their expected exfoliation age.
- They will look for any missing permanent canines and note the symmetry of eruption.
- Palpation of the gum tissue will check for any bulges that might indicate the position of an impacted tooth.
- An assessment of overall dental crowding and alignment will also be performed.
-
Radiographic Imaging (X-rays):
- Panoramic X-ray (Panorex): This provides a broad overview of all teeth in both upper and lower jaws, including developing teeth, impactions, and overall bone structure. It's often the first diagnostic tool for detecting impacted canines.
- Periapical X-rays: These provide detailed views of individual teeth and their surrounding bone, helping to pinpoint the exact location and angulation of an impacted canine relative to adjacent teeth.
- Occlusal X-rays: Taken with the film positioned on the biting surface, these are particularly useful for determining whether an impacted canine is positioned buccally (towards the cheek) or palatally (towards the roof of the mouth).
- Cone Beam Computed Tomography (CBCT): This advanced 3D imaging technique is often considered the gold standard for diagnosing impacted canines. CBCT provides incredibly detailed 3D views, allowing the dentist or orthodontist to precisely determine the canine's exact location, angulation, proximity to adjacent roots, and the presence of any pathology (cysts, tumors). This information is crucial for planning the most effective treatment.
Early diagnosis, ideally between 8 and 10 years of age, is key. This allows for interceptive measures that can prevent full impaction or simplify future treatment.
Treatment Options with Pros, Cons, and Costs
Treatment for canine issues, particularly impaction, varies depending on the severity, position of the impacted tooth, and the patient's age.
| Treatment Option | Description | Pros | Cons | Estimated Cost Range (US, without insurance) |
|---|---|---|---|---|
| Observation | Monitoring in young patients with minimal impaction; often combined with extraction of primary canine. | Non-invasive, less costly initially. May allow spontaneous eruption if space is created. | Only suitable for mild cases or very early detection. Risk of continued impaction, damage to adjacent teeth, or requiring more complex treatment later. | $50 - $200 (initial X-rays & consult) |
| Extraction of Primary Canine | Removal of the baby tooth blocking the path of the permanent canine. | Simple procedure, can facilitate spontaneous eruption in 20-75% of cases if done early enough (ages 8-10). Less invasive than surgery. | Not always effective if impaction is severe or position is very unfavorable. May still require further orthodontic treatment. Risk of space loss if permanent tooth doesn't erupt in time. | $75 - $250 |
| Surgical Exposure & Orthodontic Traction | A minor surgical procedure to expose the crown of the impacted canine, followed by bonding an orthodontic bracket to the tooth. Orthodontic forces then gently pull (traction) the canine into its correct position. Often involves braces for overall alignment. | Most common and successful treatment for impacted canines, especially those in the palate. Preserves the natural tooth, maintains natural bite, and supports facial aesthetics. High success rate (often over 80%). | Invasive surgical step. Can be lengthy (months to years of orthodontic treatment). Requires patient compliance. Risk of root resorption, ankylosis (tooth fusing to bone), or nerve damage (rare). More expensive. | $1,500 - $3,500 (surgical exposure) + $3,000 - $8,000+ (orthodontics) |
| Autotransplantation | Surgical removal of the impacted canine and re-implantation into a surgically prepared socket in its correct position. | Preserves the natural tooth. Can be an option when traction is not feasible or has failed. | Highly technique-sensitive, requires a skilled surgeon. High risk of failure (ankylosis, root resorption) if not performed perfectly. Can only be done on specific teeth that have completed a certain amount of root formation. Not suitable for all impacted canines. | $2,500 - $6,000 (excluding post-op care) |
| Surgical Extraction of Impacted Canine | Removal of the impacted canine. This is typically considered if the tooth is severely impacted, ankylosed, causing damage to adjacent teeth, or if other treatments have failed or are not feasible. | Eliminates the problematic tooth, resolving pain or potential damage to adjacent teeth. May be simpler and quicker than orthodontic traction in some cases. | Loss of a natural tooth. Requires prosthetic replacement (implant or bridge) if the space needs to be filled for function and aesthetics. Alters the natural bite. Can be complex if the tooth is deep and close to vital structures. | $300 - $800 (simple extraction) to $800 - $1,800+ (complex surgical extraction) |
| Prosthetic Replacement | After extraction, replacing the missing canine with a dental implant, bridge, or removable partial denture. | Restores function and aesthetics. Implants offer a long-lasting, stable solution that doesn't affect adjacent teeth. Bridges are less invasive than implants but require altering adjacent teeth. | Implants are costly and require bone integration time. Bridges require reducing adjacent teeth. Removable dentures are less stable and less aesthetic. All options involve ongoing maintenance. | $3,000 - $6,000 (implant + crown) or $2,000 - $5,000 (bridge) |
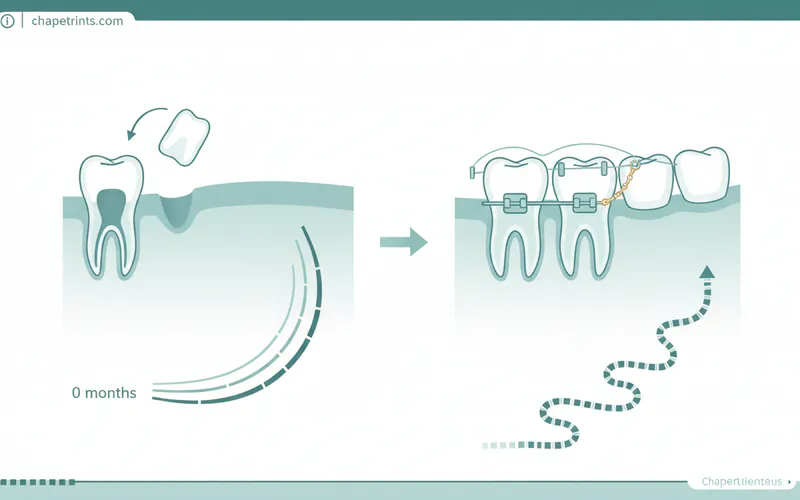
Step-by-Step: What to Expect During Treatment (Surgical Exposure & Orthodontic Traction)
This is the most common and detailed treatment approach for impacted canines:
-
Initial Consultation & Planning (Weeks 1-4):
- Diagnosis: Your orthodontist or oral surgeon will review your X-rays, including a CBCT scan, to pinpoint the exact location and angulation of the impacted canine.
- Treatment Plan: A detailed plan will be developed, outlining the surgical approach and the orthodontic mechanics needed to bring the tooth into alignment. This often involves placing full braces on other teeth first to create sufficient space for the canine.
-
Surgical Exposure (Day of Surgery):
- Anesthesia: Local anesthesia will be administered to numb the area. Sedation options (oral, IV) may also be offered for patient comfort.
- Gum Incision: The oral surgeon will make a small incision in the gum tissue to expose the crown of the impacted canine.
- Bone Removal (if necessary): In some cases, a small amount of overlying bone may need to be carefully removed to fully expose the tooth.
- Bracket Bonding: An orthodontic bracket with a small chain or ligature wire will be bonded to the exposed tooth surface.
- Repositioning Gum Flap: The gum tissue may be repositioned and sutured back in place to allow the chain to protrude through the gum, or it may be left open (open exposure technique) depending on the case.
- Recovery: You'll receive post-operative instructions for pain management, diet, and oral hygiene. Recovery from surgery typically takes a few days to a week.
-
Orthodontic Traction (Weeks 2-Months 18+):
- Connecting the Chain: Once the surgical site has healed (usually 1-2 weeks post-op), the orthodontist will connect the chain from the exposed canine to your existing braces or other orthodontic appliances.
- Gentle Forces: Very light, continuous forces will be applied to gradually pull the impacted canine into the dental arch. This process is slow and requires patience.
- Regular Adjustments: You will have regular orthodontic appointments (typically every 4-6 weeks) for adjustments to the traction force and monitoring of the tooth's movement.
- Eruption into Arch: Over several months, the canine will slowly emerge through the gum tissue and begin to align with the other teeth.
- Final Alignment: Once the canine is fully erupted and aligned, the orthodontic treatment will continue to ensure a proper bite and aesthetic finish for all teeth. The entire orthodontic phase, including initial space creation and final alignment, can last 18 months to 3 years.
Recovery Timeline and Aftercare
- Immediate Post-Surgery (First 24-48 hours):
- Pain: Mild to moderate pain is common; manage with prescribed pain medication and over-the-counter anti-inflammatories.
- Swelling: Expect some swelling, which can be minimized with ice packs applied intermittently for the first 24 hours.
- Bleeding: Slight oozing is normal; avoid vigorous rinsing.
- Diet: Stick to soft foods (yogurt, soup, mashed potatoes, smoothies).
- Oral Hygiene: Be gentle around the surgical site. Avoid brushing directly on the wound for the first few days. Your surgeon may recommend a medicated mouth rinse.
- First Week Post-Surgery:
- Swelling and pain should subside significantly.
- Continue with soft foods until comfortable.
- Avoid strenuous activity.
- Follow-up with your surgeon as scheduled (often within 7-10 days) to check healing and remove sutures if non-dissolvable ones were used.
- Orthodontic Traction Phase (Months to Years):
- Regular orthodontic adjustments will lead to some discomfort or soreness for a few days after each visit, which is manageable with OTC pain relievers.
- Maintain excellent oral hygiene around braces and the newly erupting canine.
- Avoid hard, sticky, or chewy foods that could damage braces or the exposed tooth.
- Commitment to follow-up appointments is essential for successful treatment.
Prevention Strategies
Preventing canine impaction, or at least detecting it early, is paramount.
- Regular Dental Check-ups: Routine visits to the dentist, starting in early childhood, are crucial. Your dentist can monitor the eruption sequence of all permanent teeth.
- Early Orthodontic Assessment: It's recommended that children have an orthodontic evaluation by age 7-8. An orthodontist can assess jaw growth, detect crowding, and identify potential impaction risks early on.
- Interceptive Orthodontics: If crowding or potential impaction is identified early, interceptive treatments can be performed:
- Extraction of Primary Canine: Timely removal of a primary canine that is over-retained or blocking the path can often allow the permanent canine to erupt spontaneously.
- Space Maintainers: If a primary tooth is lost prematurely, a space maintainer can prevent adjacent teeth from drifting and blocking the canine's eruption path.
- Palatal Expanders: If the upper jaw is too narrow, an expander can create more space, allowing canines to erupt properly.
- Monitoring Eruption: Parents should be aware of the typical eruption times for permanent teeth. If a canine hasn't appeared by 12-13 years of age, consult a dentist or orthodontist.
Cost Ranges in the US (with/without insurance)
The cost of canine treatment, particularly for impaction, can vary widely based on the complexity, location, and type of specialist.

- Initial Consultation & Diagnostic X-rays: $50 - $300 (often covered by insurance)
- CBCT Scan: $200 - $600 (may require specific insurance authorization)
- Extraction of Primary Canine: $75 - $250
- Surgical Exposure of Impacted Canine:
- Simple exposure (oral surgeon): $1,500 - $2,500
- Complex exposure with bone removal (oral surgeon): $2,500 - $3,500
- Orthodontic Treatment (Braces):
- Comprehensive treatment for impaction (including full braces, activation of canine): $3,000 - $8,000+
- The higher end of the range often applies to more complex cases or longer treatment times.
- Comprehensive treatment for impaction (including full braces, activation of canine): $3,000 - $8,000+
- Surgical Extraction of Impacted Canine:
- Simple extraction: $300 - $800
- Complex surgical extraction (deeply impacted): $800 - $1,800+
- Prosthetic Replacement (if canine is extracted):
- Dental Implant + Abutment + Crown: $3,000 - $6,000 per tooth
- Fixed Dental Bridge: $2,000 - $5,000 (for a 3-unit bridge replacing one tooth)
Insurance Coverage: Dental insurance typically covers a portion of these costs.
- Diagnostic procedures (X-rays, exams): Usually covered 80-100%.
- Extractions: Often covered 50-80%.
- Surgical exposure: May be covered under "oral surgery" with 50-80% coverage.
- Orthodontics: Many plans have a lifetime maximum for orthodontic treatment (e.g., $1,000 - $2,500), which may cover only a fraction of the total cost. Some plans do not cover orthodontics at all for adults.
- Implants/Bridges: Often covered 50%, subject to deductibles and annual maximums.
It is crucial to get a detailed breakdown of costs and verify insurance coverage with both your provider and the dental office before starting any treatment.
For Parents / Pediatric Considerations
Canine development is a critical area for parents to monitor. Permanent upper canines are among the last teeth to erupt, around 11-12 years of age, following the eruption of most other permanent teeth. This late eruption, coupled with their long roots and importance in the dental arch, makes them particularly vulnerable to impaction.
- Early Detection is Key: The best time to identify a potential problem with canine eruption is around 8 to 10 years of age.
- If your child's primary (baby) canine is still present past the age of 11-12, or if there's no sign of the permanent canine erupting, it's essential to consult a pediatric dentist or orthodontist.
- Look for asymmetry – if one upper permanent canine has erupted but the other hasn't by age 12, it warrants investigation.
- Role of the Pediatric Dentist: Your child's pediatric dentist plays a vital role in monitoring dental development through regular check-ups and panoramic X-rays (often taken around ages 7-9). They can identify early signs of crowding or an abnormal eruption path.
- Orthodontic Consultation: If any concerns arise, an early referral to an orthodontist is highly recommended. Interceptive orthodontics, such as timely primary canine extraction or space creation, can significantly reduce the complexity and cost of treatment later on. Waiting too long can lead to more difficult impactions, potential damage to adjacent teeth, and a longer, more involved treatment process.
- Long-Term Impact: Properly aligned canines are essential for a stable bite, efficient chewing, clear speech, and an attractive smile throughout adulthood. Addressing issues in childhood can prevent a lifetime of dental problems.
Frequently Asked Questions
How much does canine treatment cost?
The cost varies significantly depending on the issue and treatment chosen. For an impacted canine requiring surgical exposure and orthodontic traction, the total cost in the US can range from $4,500 to over $11,500 without insurance, encompassing oral surgery and comprehensive orthodontic treatment. Simple extraction of a primary canine might be $75-$250, while replacing an extracted canine with an implant could cost $3,000-$6,000. Insurance typically covers a portion, but often with limits on orthodontics.
Is canine impaction painful?
Many impacted canines are asymptomatic, meaning they don't cause pain. However, some individuals may experience localized pain, tenderness, or a feeling of pressure in the area where the tooth is trying to erupt. If the impacted canine is pressing against the roots of adjacent teeth, it can also cause pain or sensitivity in those teeth. Surgical treatment for impaction will involve some post-operative pain, which is manageable with medication.
How long does it take to treat an impacted canine?
The duration depends on the treatment method. If only a primary canine extraction is needed for spontaneous eruption, it might take a few months. However, for surgical exposure followed by orthodontic traction, the active treatment phase (pulling the tooth into position) can take 6 months to 2 years, sometimes longer. This is typically part of a broader orthodontic treatment plan that might last 18 months to 3 years in total for full bite correction.
Are there alternatives to surgery for impacted canines?
In some cases, particularly if detected early (around ages 8-10) and the impaction is mild, extraction of the primary canine alone might allow the permanent canine to erupt spontaneously. This is often the first, least invasive approach. However, for significantly impacted canines, especially those embedded in bone or far from their proper position, surgical exposure combined with orthodontic traction is generally the most effective and predictable method for saving the natural tooth. If traction fails or is not feasible, extraction of the impacted canine and subsequent prosthetic replacement (implant, bridge) is an alternative, but it means losing the natural tooth.
Does dental insurance cover impacted canine treatment?
Dental insurance coverage varies widely.
- Diagnosis (X-rays, CBCT): Often covered 80-100%.
- Extractions: Generally covered 50-80%.
- Surgical Exposure: May be covered under "oral surgery" benefits, typically 50-80%.
- Orthodontics: Many plans have a lifetime maximum for orthodontic treatment ($1,000-$2,500 is common), which may only cover a fraction of the total cost. Some adult orthodontic plans are limited or non-existent.
- Implants/Bridges: Covered under major restorative services, usually 50% after deductibles and within annual maximums. It is essential to consult with your insurance provider and the dental office's financial coordinator for an accurate estimate of your out-of-pocket expenses.
What is the difference between an incisor and a canine?
Incisors are the four front-most teeth in both the upper and lower jaws (central and lateral incisors). They have thin, flat edges designed primarily for biting and cutting food. They have a single root and are relatively delicate. Canines, on the other hand, are the pointed teeth located at the corners of the dental arches, next to the lateral incisors. They have a single, strong cusp (point) and are designed for tearing and shredding food. Canines have the longest and strongest roots of all single-rooted teeth, making them very stable in the jaw. Both are part of the anterior teeth.
What are anterior teeth?
Anterior teeth refers to the group of teeth located at the front of the mouth. This group includes the four incisors (central and lateral) and the two canines in both the upper and lower jaws, totaling 12 anterior teeth in a complete adult dentition. These teeth are primarily involved in biting, tearing, speech articulation, and contribute significantly to facial aesthetics. In contrast, the posterior teeth are the premolars and molars located further back, which are designed for crushing and grinding food.
Can canines cause problems if not treated?
Yes, untreated canine issues, especially impaction, can lead to several problems:
- Damage to adjacent teeth: The impacted canine can resorb (dissolve) the roots of neighboring teeth, potentially leading to their loss.
- Crowding and malocclusion: The impacted tooth can disrupt the alignment of other teeth, leading to a crooked smile and an improper bite.
- Cyst formation: In rare cases, a fluid-filled cyst can form around an impacted tooth, which can damage bone and adjacent teeth.
- Pain and infection: Although often asymptomatic, an impacted tooth can sometimes cause pain, or the gum around it can become inflamed or infected.
- Loss of function and aesthetics: A missing or improperly positioned canine can affect chewing efficiency, speech, and the overall appearance of your smile.
When to See a Dentist
It's always better to address potential dental issues proactively. Regarding your canines, seek professional dental advice if you notice any of the following:
- Age 10-11: If your child's upper permanent canines have not yet begun to erupt, or if their primary canines are still firmly in place.
- Age 12-13: If the permanent canine on one side has erupted, but its counterpart on the other side has not.
- Persistent Primary Canine: If a baby canine is still present past the age of 13-14 without any sign of the permanent tooth.
- Visible Bulge or Swelling: If you feel or see a bulge on the gum (either on the palate or cheek side) where a canine should be, it could indicate an impacted tooth.
- Crowding or Misalignment: If other teeth are becoming increasingly crowded or appear to be tilting due to lack of space for the canine.
- Pain or Discomfort: Any unexplained pain, pressure, or tenderness in the area where a canine should be erupting.
- Sensitivity in Adjacent Teeth: If teeth next to where a canine should be are becoming sensitive, it could indicate root resorption from an impacted tooth.
Routine dental check-ups, especially for children, are the most effective way to monitor canine development and identify potential problems early, allowing for simpler and less invasive intervention.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.