Diabetes and Teeth Problems: Complete Guide
Key Takeaways
- Diabetes is a chronic condition affecting millions of Americans, and while its systemic impacts on organs like the heart, kidneys, and eyes are well-documented, its profound effects on oral health are often underestimated. If you have diabetes, or are at risk, understanding the intricate link betwee
Diabetes is a chronic condition affecting millions of Americans, and while its systemic impacts on organs like the heart, kidneys, and eyes are well-documented, its profound effects on oral health are often underestimated. If you have diabetes, or are at risk, understanding the intricate link between diabetes and teeth problems is crucial for maintaining your overall well-being. Uncontrolled blood sugar levels can create a fertile ground for various dental issues, ranging from persistent gum disease and infections to chronic dry mouth and difficulty healing. Ignoring these oral symptoms can lead not only to discomfort and tooth loss but can also exacerbate your diabetes, creating a challenging cycle of worsening health. This comprehensive guide will explore the specific ways diabetes impacts your teeth and gums, delve into the causes, signs, and symptoms, and outline the most effective treatment, prevention, and management strategies to safeguard your oral health.
Key Takeaways:
- Bidirectional Relationship: Poorly controlled diabetes significantly increases the risk and severity of gum disease (periodontitis), while severe periodontitis can make blood sugar control more difficult.
- Increased Infection Risk: Diabetics are more susceptible to oral infections like candidiasis (thrush) and slower wound healing due to impaired immune function and reduced blood flow.
- Common Oral Issues: Be vigilant for signs of gingivitis, periodontitis, dry mouth (xerostomia), increased cavities, and diabetes and mouth ulcers.
- Aggressive Dental Care: Diabetics typically need more frequent dental check-ups (every 3-4 months) and professional cleanings, costing approximately $75-$200 per visit without insurance, for routine care. Deep cleaning (scaling and root planing) for periodontitis can range from $600 to $1,800 for the entire mouth.
- Gum Inflammation Management: Reducing inflammation of gums in diabetics primarily involves excellent blood sugar control, meticulous daily oral hygiene, and regular professional dental cleanings, potentially supplemented with antimicrobial rinses or localized antibiotics.
- Cost of Advanced Treatment: Treatments for severe periodontitis, such as gum surgery, can range from $500 to $4,000 per quadrant, with many dental insurance plans covering a portion (typically 50-80%) of major procedures after a deductible.
- Prevention is Key: Optimal blood glucose management, daily brushing and flossing, avoiding smoking, and communicating your diabetic status to your dentist are the most effective preventive measures.
What It Is: Diabetes and Its Oral Health Connection
Diabetes mellitus is a chronic metabolic disease characterized by high blood glucose (sugar) levels, resulting either from the body's inability to produce enough insulin (Type 1 diabetes), or from the body's inability to effectively use the insulin it produces (Type 2 diabetes). Gestational diabetes is a temporary form that can occur during pregnancy. Regardless of the type, sustained high blood sugar levels have a cascade of negative effects throughout the body, including the oral cavity.
The link between diabetes and oral health is a two-way street, often referred to as a bidirectional relationship. This means that diabetes can worsen oral health, and conversely, poor oral health, particularly severe gum disease, can make it harder to control blood sugar levels. This vicious cycle highlights why integrated management is essential. High glucose levels in the saliva, impaired immune response, compromised blood vessel function, and altered inflammatory responses all contribute to a heightened risk of various oral complications for individuals with diabetes.
Types of Oral Problems Associated with Diabetes
Individuals with diabetes are at a significantly increased risk for a range of specific oral health issues. These problems can impact comfort, function, and even lead to tooth loss if not properly managed.
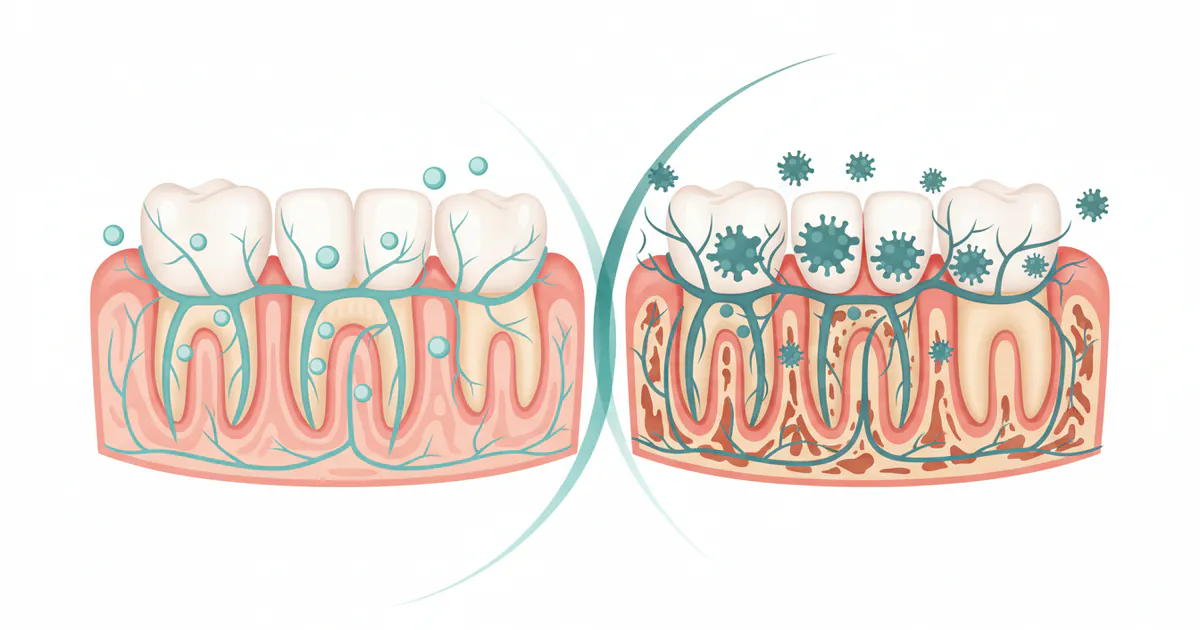
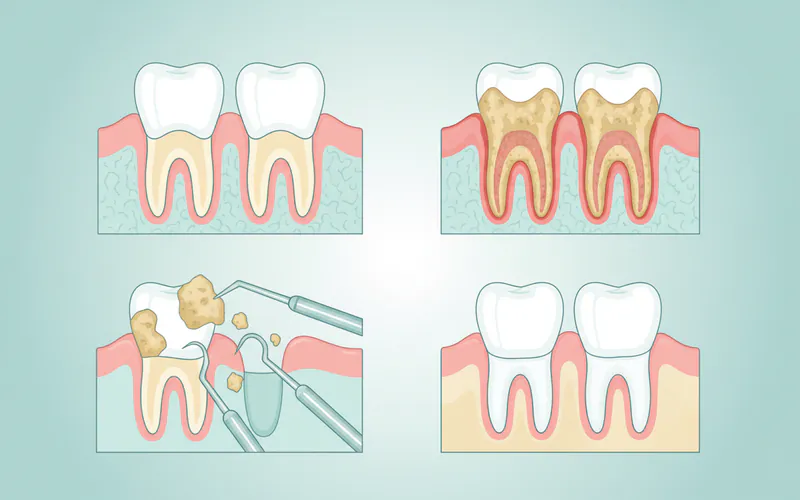
Periodontal Disease (Gum Disease)
This is by far the most common and serious oral complication of diabetes, affecting up to 90% of diabetic patients to some degree, and it's often more severe and progresses more rapidly than in non-diabetic individuals. Periodontal disease encompasses two main stages:
- Gingivitis: The mildest form, characterized by inflamed, red, swollen gums that bleed easily, especially during brushing or flossing. It's caused by plaque buildup along the gumline.
- Periodontitis: If gingivitis is left untreated, it can advance to periodontitis. Here, the inflammation spreads below the gumline, causing the gums to pull away from the teeth, forming pockets. Bacteria thrive in these pockets, leading to bone loss, tissue destruction, and eventually, tooth loosening and loss. Diabetics are particularly susceptible because high blood sugar impairs the body's ability to fight infection and heal, making them more vulnerable to the destructive effects of periodontal bacteria.
Dry Mouth (Xerostomia)
Many diabetics experience chronic dry mouth, a condition where the salivary glands do not produce enough saliva. This can be a side effect of certain diabetes medications, poor blood sugar control leading to fluid loss, or nerve damage. Saliva plays a crucial role in oral health by washing away food particles, neutralizing acids, and providing minerals that protect tooth enamel. Reduced saliva flow can lead to:
- Increased risk of tooth decay (cavities).
- Oral candidiasis (thrush).
- Difficulty chewing, swallowing, and speaking.
- Persistent bad breath (halitosis).
- Soreness and cracking at the corners of the mouth.
Oral Candidiasis (Thrush)
This is a fungal infection caused by an overgrowth of Candida albicans yeast, a common microorganism normally present in the mouth. High glucose levels in the saliva of diabetics provide an ideal environment for Candida to multiply. Symptoms include white, creamy patches on the tongue, inner cheeks, roof of the mouth, or throat, which may bleed slightly when scraped. It can also cause a burning sensation, difficulty eating, and altered taste. Diabetics, especially those who wear dentures or take antibiotics frequently, are at higher risk.
Tooth Decay (Cavities)
While often linked to dry mouth, diabetics can have an increased risk of cavities even with adequate saliva, due to higher sugar levels in their saliva. The bacteria in plaque feed on sugars, producing acids that erode tooth enamel. Impaired immune function can also make teeth more vulnerable to bacterial acid attacks.
Impaired Healing
Diabetics often experience slower and less efficient wound healing throughout the body, including the mouth. This is critical for dental procedures such as extractions, oral surgery, or even routine scaling, as the risk of post-operative infection and delayed recovery is higher. Poorly controlled diabetes can also compromise the success rates of dental implants.
Taste Disturbances and Burning Mouth Syndrome
Some individuals with diabetes report changes in their sense of taste (dysgeusia) or a persistent burning sensation in their mouth, tongue, lips, or throat, often without any visible lesions (Burning Mouth Syndrome). These can be related to nerve damage (neuropathy) associated with diabetes.
Oral Sores and Mouth Ulcers
Diabetics may experience diabetes and mouth ulcers more frequently, and these sores may take longer to heal. Compromised immunity and poor circulation can contribute to the formation and persistence of these lesions. They can be painful and interfere with eating and speaking.
Causes: Why Diabetes Wreaks Havoc on Oral Health
The primary driver behind diabetes-related oral health problems is hyperglycemia – persistently high blood sugar levels. This leads to a complex interplay of physiological changes that damage oral tissues:
- Advanced Glycation End Products (AGEs): High glucose reacts with proteins and fats to form AGEs. These harmful compounds accumulate in tissues, including those in the gums, and contribute to inflammation, oxidative stress, and impaired cellular function. AGEs can make tissues less elastic, disrupt collagen, and hinder the repair process.
- Impaired Immune Response: Diabetes can weaken the body's immune system, particularly the function of white blood cells (neutrophils) that are crucial for fighting bacterial and fungal infections. This reduced immune competence means diabetics are less able to fend off the bacteria that cause gum disease and other oral infections like thrush.
- Reduced Blood Flow (Microangiopathy): High blood sugar can damage small blood vessels (capillaries) throughout the body, including those supplying the gums and jawbone. This reduced blood flow diminishes the delivery of oxygen and nutrients to oral tissues and impairs the removal of waste products, further compromising tissue health and healing capacity.
- Exacerbated Inflammatory Response: Diabetics often have an exaggerated inflammatory response to bacterial challenges. When plaque bacteria trigger inflammation in the gums, the diabetic body's response can be overly aggressive and destructive, leading to more rapid breakdown of gum tissue and bone compared to non-diabetics. This contributes directly to the rapid progression of periodontitis.
- Altered Salivary Gland Function: As mentioned, diabetes can lead to decreased saliva production (xerostomia), which reduces the natural cleansing and protective mechanisms of the mouth.
- Genetic Predisposition and Lifestyle Factors: While diabetes is the underlying cause, certain genetic factors can make some individuals more susceptible to its oral complications. Lifestyle choices such as smoking significantly compound the risk, as smoking further impairs blood flow, immune function, and healing, making gum disease much worse and treatment less effective in diabetics. Poor oral hygiene also directly contributes to plaque buildup, initiating the inflammatory cycle.
Signs and Symptoms: What to Look For
Recognizing the early signs of diabetes-related oral problems is crucial for timely intervention. Be vigilant for any of these indicators:
- Bleeding Gums: Gums that bleed easily when brushing, flossing, or even spontaneously. This is often the first sign of gingivitis.
- Red, Swollen, or Tender Gums: Gums that appear inflamed and puffy instead of firm and pink.
- Persistent Bad Breath (Halitosis): Often a symptom of bacterial overgrowth and gum disease.
- Receding Gums: Gums that pull away from the teeth, making teeth look longer.
- Loose or Shifting Teeth: A late sign of advanced periodontitis and bone loss.
- Pus Between Teeth and Gums: Indicates an active infection.
- Changes in Bite: How your upper and lower teeth fit together.
- Persistent Dry Mouth: A constant feeling of dryness, thirst, or difficulty speaking/swallowing.
- Increased Tooth Sensitivity: Especially to hot or cold temperatures, due to exposed root surfaces from gum recession or new cavities.
- Sores, Ulcers, or White Patches in the Mouth: Could indicate thrush, diabetes and mouth ulcers, or other infections that are slow to heal.
- Frequent Cavities: Despite good oral hygiene.
- Unusual Taste: A metallic or generally altered taste sensation.
Pro Tip: Do not wait for pain to seek dental care. Many diabetes-related oral issues, especially gum disease, can progress significantly without causing severe pain until they are advanced. Regular self-examination and professional check-ups are vital.
Treatment Options for Diabetes-Related Oral Problems
Treating oral problems in diabetics requires a multi-pronged approach that includes meticulous dental care, effective blood sugar management, and often, collaboration between your dentist and your primary care physician or endocrinologist.
For Periodontal Disease (Gingivitis and Periodontitis)
The goal is to remove plaque and calculus (hardened plaque), control bacterial infection, and prevent further tissue and bone loss.
- Scaling and Root Planing (SRP) – Deep Cleaning:
- Description: This non-surgical procedure involves thoroughly cleaning below the gumline to remove plaque and calculus from the tooth roots, and then smoothing the root surfaces to deter future bacterial accumulation.
- Pros: Highly effective for early to moderate periodontitis, less invasive than surgery, can significantly reduce inflammation.
- Cons: May require local anesthesia, can cause temporary sensitivity or soreness, may need multiple appointments.
- Cost: Typically $600 - $1,800 for the entire mouth (four quadrants) without insurance.
- Antibiotics:
- Description: Oral antibiotics (e.g., doxycycline) or topical antibiotics (e.g., antibiotic gels placed directly into periodontal pockets) may be used to reduce bacterial load.
- Pros: Can effectively target specific bacteria, enhance the effects of SRP.
- Cons: Oral antibiotics can have side effects (GI upset, yeast infections), risk of antibiotic resistance with overuse.
- Laser Therapy:
- Description: Lasers can be used as an adjunct to SRP to remove inflamed tissue and kill bacteria with minimal discomfort and bleeding.
- Pros: Less invasive than traditional surgery, faster healing, reduced bleeding.
- Cons: Can be more expensive, not all dental offices offer it, effectiveness still debated for specific applications.
- Gum Surgery (Flap Surgery, Osseous Surgery):
- Description: For advanced periodontitis, the gums are lifted back to allow direct access to remove calculus and smooth bone irregularities.
- Pros: Allows for thorough cleaning and reshaping of bone, can halt disease progression in severe cases.
- Cons: More invasive, longer recovery time, potential for gum recession.
- Cost: Can range from $500 - $4,000 per quadrant.
- Bone Grafts and Soft Tissue Grafts:
- Description: Used to regenerate bone or gum tissue lost due to severe periodontitis.
- Pros: Can restore lost support and protect tooth roots.
- Cons: Invasive, longer healing, significant cost.
- Cost: Bone grafts $400 - $1,200 per site (excluding implant placement), soft tissue grafts $600 - $2,500 per site.
For Dry Mouth (Xerostomia)
- Saliva Substitutes: Over-the-counter sprays, gels, or rinses that mimic natural saliva.
- Xylitol Products: Chewing gum or lozenges containing xylitol can stimulate saliva flow and inhibit bacterial growth.
- Fluoride Treatments: Prescription-strength fluoride toothpaste or rinses to protect teeth from decay due to reduced saliva.
- Sialogogues: Prescription medications (e.g., pilocarpine) that stimulate saliva production, used in severe cases.
- Hydration: Sipping water frequently throughout the day.
For Oral Candidiasis (Thrush)
- Antifungal Medications: Topical (rinses, lozenges/troches like nystatin or clotrimazole) or systemic (oral tablets like fluconazole) antifungals. Duration typically 7-14 days.
- Denture Hygiene: If wearing dentures, remove them at night, clean them daily with an appropriate denture cleaner, and soak them in an antifungal solution as prescribed.
For Tooth Decay (Cavities)
- Fillings: To repair cavities. Materials include amalgam, composite resin, or porcelain.
- Cost: Amalgam $50-$200, Composite $90-$400 per filling.
- Crowns: For extensively decayed or damaged teeth.
- Cost: $800-$2,500 per crown.
- Root Canal Therapy: If decay reaches the pulp.
- Cost: $700-$2,000 for front teeth, $900-$2,500 for molars.
For Diabetes and Mouth Ulcers
- Over-the-Counter Pain Relief: Topical anesthetic gels or rinses (e.g., containing benzocaine) to numb the area.
- Prescription Rinses: Antimicrobial or corticosteroid rinses may be prescribed for persistent or severe ulcers to reduce pain and aid healing.
- Addressing Underlying Causes: Ensuring optimal blood sugar control is paramount for preventing and healing ulcers.
Pro Tip: Always inform your dentist about your diabetes diagnosis, current medications, and your most recent A1C level. This information is crucial for tailoring your dental treatment plan and managing potential complications.
Step-by-Step Process: Managing Periodontitis in a Diabetic Patient (Example: Scaling and Root Planing)
Here's what you can generally expect if you need a scaling and root planing (deep cleaning) procedure to address periodontitis, a common issue for diabetics:
- Initial Examination and Diagnosis: Your dentist or periodontist will thoroughly examine your gums, measure pocket depths around your teeth, and review X-rays to assess bone loss. They will discuss your diabetes status, A1C levels, and any medications. This allows them to determine if you're a good candidate and if any pre-treatment considerations (like adjusting insulin or antibiotics) are necessary.
- Local Anesthesia: To ensure comfort during the procedure, a local anesthetic will be administered to numb the specific areas of your mouth being treated. For diabetics, dentists may use epinephrine-free anesthetics if there are concerns about cardiovascular effects.
- Scaling: Using specialized instruments (manual scalers and/or ultrasonic devices), the dental hygienist or dentist will meticulously remove plaque and tartar (calculus) from above and below the gumline. This step targets the hardened bacterial deposits that contribute to gum inflammation.
- Root Planing: After scaling, the root surfaces of your teeth are smoothed. This removes any remaining bacterial toxins and rough spots, making it more difficult for plaque to reattach and allowing the gums to reattach more firmly to the clean, smooth tooth surface.
- Irrigation (Optional): Some dentists may irrigate the treated pockets with an antimicrobial solution (like chlorhexidine) to further reduce bacterial load.
- Antibiotic Placement (Optional): In certain cases, especially for persistent or deep pockets, a localized antibiotic medication (e.g., an antibiotic chip or gel) may be placed directly into the cleaned periodontal pockets to provide sustained antimicrobial action.
- Post-Procedure Instructions: You'll receive detailed instructions on post-treatment care, including managing any discomfort, dietary recommendations, and how to maintain oral hygiene during the healing period.
- Follow-Up Appointments: Several weeks after the SRP, you'll have a follow-up visit to assess gum healing and monitor pocket depths. Diabetics typically require more frequent maintenance appointments (periodontal recall) – often every 3 to 4 months – to prevent recurrence of the disease.
Cost and Insurance: Navigating Dental Care for Diabetics
The cost of dental care can be a significant concern, especially for diabetics who often require more frequent and sometimes more extensive treatments. Prices vary widely based on location (urban vs. rural), the specific dentist or specialist, and the complexity of the case.
Average US Price Ranges (Without Insurance)
- Routine Exam & Cleaning: $75 - $200 (for non-periodontal cleaning)
- Scaling and Root Planing (Deep Cleaning):
- Per quadrant: $150 - $450
- Full mouth (4 quadrants): $600 - $1,800
- Standard Filling (Composite): $90 - $400 per tooth
- Tooth Extraction (Simple): $75 - $300
- Tooth Extraction (Surgical/Impacted): $150 - $650+
- Crown (Porcelain/Ceramic): $800 - $2,500 per tooth
- Root Canal:
- Front tooth: $700 - $1,500
- Molar: $900 - $2,500
- Periodontal Maintenance (after SRP): $100 - $250 per visit (typically every 3-4 months)
- Antifungal Medication (Oral Thrush): Varies greatly by specific drug and dosage, from $20 for a generic rinse to $100+ for systemic pills without insurance.
- Gum Surgery (Per Quadrant): $500 - $4,000
Insurance Coverage Details
Dental insurance can significantly reduce out-of-pocket costs. Most plans categorize treatments:
- Preventive Care (Type 1): Exams, routine cleanings, X-rays. Often covered at 80-100%.
- Basic Procedures (Type 2): Fillings, simple extractions. Typically covered at 50-80%.
- Major Procedures (Type 3): Crowns, bridges, dentures, root canals, periodontal surgery. Usually covered at 20-50%.
Diabetic patients requiring more frequent periodontal maintenance (e.g., every 3 months instead of 6) might find their insurance doesn't cover the additional cleanings at 100% if they exceed typical annual limits. It's crucial to check your specific plan benefits for "periodontal maintenance" codes (D4910) and annual maximums, which often range from $1,000 to $2,500. Some plans offer specific enhanced benefits for individuals with chronic conditions like diabetes.
Pro Tip: Before any extensive treatment, ask your dental office for a detailed treatment plan including estimated costs and what your insurance is expected to cover. Pre-authorization from your insurance company can prevent unexpected bills.
Recovery and Aftercare
Recovery time and aftercare instructions vary depending on the specific procedure.
- After Scaling and Root Planing (SRP):
- Discomfort: Expect some soreness, sensitivity, and mild gum bleeding for a few days. Over-the-counter pain relievers (like ibuprofen or acetaminophen) can help. Avoid aspirin as it can thin blood.
- Diet: Stick to soft foods for 24-48 hours. Avoid very hot, cold, spicy, or crunchy foods.
- Oral Hygiene: Continue gentle brushing and flossing, but avoid the treated areas for the first day. Your dentist may recommend a prescription antimicrobial mouth rinse (e.g., chlorhexidine) for a week or two to aid healing and reduce bacteria.
- Blood Sugar Control: Maintain strict blood sugar control during recovery to facilitate healing and prevent infection.
- Follow-Up: Attend all scheduled follow-up appointments (typically 4-6 weeks after SRP) for evaluation.
- After Oral Surgery (e.g., gum surgery, extractions):
- Pain and Swelling: More significant than SRP. Ice packs, prescribed pain medication, and antibiotics (if prescribed) are common.
- Bleeding: Some oozing is normal; bite on gauze pads as instructed.
- Diet: Soft diet is essential, avoiding chewing on the surgical site.
- Oral Hygiene: Be extremely gentle around the surgical site. Your dentist will advise on specific rinsing instructions. Avoid vigorous rinsing or spitting.
- Blood Sugar: Paramount for optimal healing. Poorly controlled diabetes significantly increases the risk of dry socket, infection, and delayed healing after extractions.
- General Aftercare for Diabetics:
- Maintain Excellent Oral Hygiene: This is non-negotiable. Continue brushing twice daily and flossing once daily.
- Monitor Blood Glucose: Keep your blood sugar levels within your target range as recommended by your doctor. This directly impacts your mouth's ability to heal and fight infection.
- Stay Hydrated: Especially if you suffer from dry mouth.
- Avoid Tobacco: Smoking severely impairs healing and worsens gum disease in diabetics.
- Regular Dental Check-ups: Adhere to your dentist's recommended recall schedule, which for diabetics is often every 3-4 months for periodontal maintenance.
Prevention: Safeguarding Your Oral Health with Diabetes
Prevention is the cornerstone of managing diabetes-related oral health problems. By proactively addressing risk factors and maintaining diligent care, you can significantly reduce your chances of developing severe complications.
- Strict Blood Glucose Control: This is the most critical preventive measure. Keeping your A1C levels and daily blood sugar readings within your target range, as advised by your medical doctor, directly reduces inflammation, improves immune function, and promotes healthier oral tissues.
- Meticulous Daily Oral Hygiene:
- Brush Twice Daily: Use a soft-bristled toothbrush and fluoride toothpaste. Consider an electric toothbrush for more effective plaque removal. Brush for at least two minutes, covering all tooth surfaces and gently brushing your tongue.
- Floss Once Daily: Flossing removes plaque and food particles from between teeth and under the gumline where your toothbrush can't reach. This is crucial for preventing gum disease.
- Use an Antimicrobial Mouthwash: A therapeutic mouthwash (e.g., containing chlorhexidine, if prescribed, or an ADA-accepted antiseptic mouthwash) can help reduce bacteria and control gingivitis.
- Clean Dentures/Appliances: If you wear dentures, clean them daily and remove them at night. Follow your dentist's specific instructions.
- Regular Dental Check-ups and Professional Cleanings:
- Frequency: Diabetics should aim for dental check-ups every 3-4 months, rather than the standard six months, to monitor for early signs of problems and receive professional cleanings.
- Inform Your Dentist: Always remind your dental team about your diabetes diagnosis, medications, and recent A1C levels.
- Quit Smoking: Smoking dramatically increases the risk and severity of gum disease, particularly in diabetics. It impairs blood flow, suppresses the immune system, and hinders healing. Quitting is one of the most impactful steps you can take for both your oral and overall health.
- Healthy Diet: Limit sugary foods and drinks that feed cavity-causing bacteria. Choose a balanced diet rich in fruits, vegetables, and whole grains.
- Stay Hydrated: Drink plenty of water throughout the day, especially if you experience dry mouth.
- Self-Monitoring: Regularly examine your mouth for any changes – red, swollen, or bleeding gums; sores that won't heal; white patches; or persistent bad breath. Report any concerns to your dentist promptly.
How to Reduce Inflammation of Gums (Specific Strategies for Diabetics)
Reducing inflammation of gums is paramount for diabetics. Here's how:
- Optimal Blood Glucose Control: This is the foundational step. Well-controlled blood sugar minimizes the systemic inflammatory response and creates a healthier environment for gum tissue.
- Thorough Plaque Removal: Daily brushing and flossing (mechanical disruption of bacterial biofilms) are the most effective ways to remove the primary irritant causing inflammation.
- Regular Professional Cleanings: Dentists and hygienists remove hardened plaque (tartar) that cannot be removed by brushing and flossing alone, which is a constant source of inflammation.
- Antimicrobial Rinses: As an adjunct to mechanical cleaning, your dentist may recommend an antimicrobial mouthwash to reduce bacterial load.
- Localized Antibiotics: For specific deep pockets, a localized antibiotic placed by your dentist can target inflammation at its source.
- Anti-inflammatory Medications: In some cases, low-dose doxycycline may be prescribed for its anti-collagenase effects, helping to reduce the destructive inflammatory processes in the gums.
Risks and Complications
Failing to manage diabetes-related oral health issues can lead to several severe complications, both orally and systemically.
Oral Complications:
- Tooth Loss: Uncontrolled periodontitis is a leading cause of tooth loss in adults, and the risk is amplified in diabetics. Missing teeth can impair chewing, speaking, and self-esteem.
- Difficulty with Dental Prosthetics: Dentures and bridges may fit poorly due to changes in gum and bone structure.
- Dental Implant Failure: Diabetics, especially those with poorly controlled blood sugar, have a higher risk of implant failure due to impaired healing and increased susceptibility to infection (peri-implantitis).
- Chronic Oral Pain and Discomfort: From persistent gum inflammation, dry mouth, or unhealed sores.
- Increased Susceptibility to Other Oral Infections: Beyond candidiasis, other bacterial or viral infections may be more common and severe.
Systemic Complications (Bidirectional Impact):
- Worsening Blood Glucose Control: Chronic, severe gum disease (periodontitis) is considered a major chronic infection. The ongoing inflammation and bacterial burden in the mouth can increase insulin resistance, making it harder to control blood sugar levels, thereby exacerbating diabetes.
- Increased Risk of Other Diabetic Complications: The systemic inflammation from periodontal disease has been linked to an increased risk of other serious diabetic complications, including:
- Cardiovascular Disease: Heart attack and stroke.
- Kidney Disease: Diabetic nephropathy.
- Neuropathy: Nerve damage.
- Retinopathy: Eye disease leading to vision loss.
- Pregnancy Complications: For pregnant women with gestational diabetes, periodontal disease can increase the risk of preterm birth and low birth weight.
Comparison Tables
Table 1: Common Diabetes-Related Oral Issues & Management Approaches
| Oral Problem | Key Symptoms | Primary Management Strategies | Typical Treatment Costs (Uninsured) |
|---|---|---|---|
| Gingivitis | Red, swollen, bleeding gums | Daily brushing/flossing, regular professional cleanings | $75 - $200 (routine cleaning) |
| Periodontitis | Receding gums, loose teeth, bad breath, pus | Scaling & Root Planing (SRP), antibiotics, surgery, advanced blood sugar control | $600 - $1,800 (SRP), $500 - $4,000 (surgery) |
| Dry Mouth (Xerostomia) | Thirst, cracked lips, difficulty swallowing, increased cavities | Saliva substitutes, xylitol products, fluoride, frequent water intake | $10 - $30 (OTC products), prescription costs vary |
| Oral Candidiasis (Thrush) | White patches, burning sensation, altered taste | Antifungal medications (topical/systemic), denture hygiene | $20 - $100+ (medication) |
| Tooth Decay (Cavities) | Toothache, sensitivity, visible holes in teeth | Fillings, crowns, root canals | $90 - $400 (filling), $800 - $2,500 (crown) |
| Diabetes & Mouth Ulcers | Painful sores, slow healing | Topical pain relief, prescription rinses, blood sugar control | $10 - $50 (OTC), prescription costs vary |
Table 2: Periodontal Treatment Options for Diabetics: Cost, Recovery & Efficacy
| Treatment Option | Description | Average Cost (Uninsured) | Recovery Time | Efficacy for Diabetics (with good BS control) |
|---|---|---|---|---|
| Scaling & Root Planing (SRP) | Deep cleaning below gumline to remove plaque/tartar | $150 - $450 per quadrant | 1-3 days | High for mild-mod periodontitis, reduces inflammation significantly |
| Localized Antibiotics | Antimicrobial gel/chip placed in pockets | $40 - $100 per site | Minimal | Good as an adjunct to SRP for specific sites |
| Laser Periodontal Therapy | Laser used to remove inflamed tissue and bacteria | $500 - $2,000 per quadrant | 1-2 days | Promising, less invasive, potentially faster healing |
| Traditional Gum Surgery | Gums lifted for direct cleaning/bone reshaping | $500 - $4,000 per quadrant | 1-2 weeks | High for advanced periodontitis, halts disease progression |
| Bone/Tissue Grafting | Regenerating lost bone or gum tissue | $400 - $2,500 per site | Weeks-Months | Moderate to high, depends on defect and patient healing capacity |
Children / Pediatric Considerations
Children and adolescents with Type 1 diabetes are also at an increased risk for specific oral health problems. While periodontitis is more common in adults, early-onset forms can occur in diabetic youth.
- Increased Cavity Risk: Diabetic children often have higher sugar levels in their saliva, making them more susceptible to tooth decay.
- Gingivitis: Even young children with diabetes can exhibit signs of gingivitis (red, swollen gums) due to impaired immune response and higher blood sugar. It's crucial for parents to monitor their child's oral hygiene closely.
- Delayed Tooth Eruption: Some studies suggest that diabetic children may experience slightly delayed tooth eruption compared to their non-diabetic peers.
- Oral Candidiasis: As with adults, oral thrush can be more common in diabetic children, especially if blood sugar is poorly controlled or if they are taking antibiotics.
- Importance of Education: Parents of diabetic children need comprehensive education on the link between diabetes and oral health. They must be diligent in helping their children maintain excellent oral hygiene, monitor blood sugar, and adhere to regular dental check-ups.
- Dental Visits: Children with diabetes should see the dentist every six months, or even more frequently if recommended by their dentist, to monitor for early signs of decay or gum problems. Dentists might recommend fluoride varnishes or sealants to provide extra protection against cavities.
Frequently Asked Questions
Can diabetes cause tooth loss?
Yes, absolutely. Uncontrolled diabetes significantly increases the risk and severity of periodontal disease (gum disease), which is the leading cause of tooth loss in adults. The chronic inflammation and bone destruction associated with periodontitis can weaken the support structures of the teeth, eventually leading to their loosening and loss.
How often should a diabetic see the dentist?
Individuals with diabetes should generally see their dentist for check-ups and professional cleanings more frequently than the average person. While six months is standard, many dentists recommend diabetic patients come in every 3 to 4 months to monitor for early signs of gum disease, cavities, and other oral complications, and to maintain optimal oral health.
What's the best way to reduce inflammation of gums with diabetes?
The most effective way to reduce inflammation of gums for diabetics is a combination of meticulous daily oral hygiene (brushing twice, flossing once), regular professional dental cleanings, and, most importantly, strict control of blood glucose levels. Your dentist may also recommend antimicrobial mouthwashes or localized antibiotics for targeted inflammation.
Are mouth ulcers common with diabetes?
Yes, diabetes and mouth ulcers can be more common and problematic for individuals with diabetes. Compromised immune function, reduced blood flow, and slower healing can contribute to the formation of mouth sores and make them linger longer than in non-diabetic individuals. It's crucial to report persistent ulcers to your dentist.
Is dental work safe for diabetics?
Yes, dental work is generally safe for diabetics, but it requires careful planning and communication. Always inform your dentist about your diabetes, your medications, and your current blood sugar levels. Well-controlled diabetes poses fewer risks, but for those with poorly controlled blood sugar, dentists may need to take precautions, such as prescribing prophylactic antibiotics or postponing extensive procedures, to prevent infection and promote healing.
What specific oral hygiene products should diabetics use?
Diabetics should use a soft-bristled toothbrush (manual or electric) and fluoride toothpaste. If dry mouth is an issue, consider fluoride rinses, xylitol-containing products (gums, lozenges), and specialized dry mouth rinses or gels. Your dentist may also recommend a therapeutic antimicrobial mouthwash or a prescription-strength fluoride toothpaste for enhanced protection.
How does blood sugar control impact oral health?
Optimal blood sugar control is foundational to good oral health for diabetics. When blood sugar levels are consistently within a healthy range, the body's immune system functions better, inflammation is reduced, blood flow to oral tissues improves, and healing processes are more efficient. This directly lessens the risk and severity of gum disease, infections, and cavities.
What are the early signs of gum disease in diabetics?
Early signs of gum disease (gingivitis) in diabetics include red, swollen, or tender gums that bleed easily when brushing or flossing. As it progresses to periodontitis, you might notice persistent bad breath, receding gums, sensitivity, or a change in how your teeth fit together.
Is it true that diabetes can make dental implants fail?
Yes, poorly controlled diabetes can increase the risk of dental implant failure. High blood sugar impairs bone healing and increases susceptibility to infection around the implant (peri-implantitis). However, with good blood sugar control, proper pre-operative assessment, and meticulous post-operative care, dental implant success rates for diabetics can be comparable to those of non-diabetics.
What are the costs associated with treating diabetes-related oral issues?
The costs vary significantly depending on the issue and treatment needed. Routine cleanings are $75-$200. Deep cleanings (Scaling and Root Planing) can range from $600-$1,800. Fillings are $90-$400, and more advanced procedures like gum surgery can be $500-$4,000 per quadrant. Many dental insurance plans cover a portion of these costs, but it's essential to check your specific benefits and annual maximums.
When to See a Dentist
Given the heightened risks for individuals with diabetes, knowing when to seek professional dental care is crucial.
Schedule a routine dental check-up and cleaning immediately if you have diabetes and haven't seen a dentist in the last 6 months. Proactive monitoring is your best defense.
See your dentist promptly (within a few days) if you notice any of the following signs:
- Persistent Bleeding Gums: Gums that bleed consistently when you brush, floss, or even spontaneously, and don't improve with careful hygiene.
- Swollen, Red, or Tender Gums: Gums that are visibly inflamed and painful to the touch.
- Persistent Bad Breath: Halitosis that doesn't go away despite good oral hygiene, as this can be a sign of gum disease or infection.
- Receding Gums or Loose Teeth: These are indicators of advancing periodontal disease and require immediate evaluation to prevent tooth loss.
- Sores, Ulcers, or White Patches: Any oral lesions that don't heal within a week or two, or white, creamy patches that could indicate candidiasis.
- Persistent Dry Mouth: If your dry mouth is severe, affecting your ability to eat or speak, or leading to increased cavities.
- Pain or Sensitivity: New or worsening tooth pain or sensitivity, which could signal a cavity or gum recession.
Seek immediate emergency dental care if you experience:
- Severe, Unrelenting Toothache: Especially if accompanied by swelling in your face or jaw, as this could indicate an abscess or severe infection that needs urgent attention.
- Pus Draining from Your Gums or a Swollen Lump on Your Gums: These are clear signs of an active infection.
- Sudden Loosening of a Tooth: Indicating significant bone loss or trauma.
- Difficulty Swallowing or Breathing: If oral infection spreads, it can impact airways, requiring immediate medical and dental intervention.
Always remember that for diabetics, oral health isn't just about your mouth – it's an integral part of your overall diabetes management and systemic health. Regular dental care and effective blood sugar control go hand in hand in protecting your well-being.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Does Oil Pulling Help Gut Health
The intricate connection between our oral health and overall well-being is a topic of growing fascination and scientific inquiry. Often, when we think of health, we focus on specific organs or systems, overlooking the crucial role of the mouth as a gateway to the rest of the body. One ancient practi
February 23, 2026

Does Oil Pulling Help With Inflammation
It's a question many health-conscious individuals ask as they explore natural remedies: does oil pulling help with inflammation? In an era where holistic approaches to wellness are gaining traction, the ancient practice of oil pulling has resurfaced, promising benefits that extend beyond oral hy
February 23, 2026
Oil Pulling for Kidney Disease: Complete Guide
Chronic kidney disease (CKD) affects an estimated 37 million adults in the United States, often progressing silently until advanced stages. What many may not realize is the profound connection between the health of their mouth and the health of their kidneys. As a bridge between traditional wisd
February 23, 2026

Oil Pulling Oral Microbiome: Complete Guide
Have you ever considered the bustling universe thriving within your mouth? This intricate community, known as the oral microbiome, consists of billions of microorganisms – some beneficial, some harmful – all playing a critical role in your oral and overall systemic health. Maintaining a balanced
February 23, 2026