Is All Snoring Sleep Apnea

Key Takeaways
- Many individuals, perhaps even you or a loved one, have been told they snore loudly. It's often dismissed as a harmless, albeit annoying, nocturnal habit. However, what if that nightly rumble is more than just noise? What if it's a critical indicator of an underlying health condition that significan
Is All Snoring Sleep Apnea? Unraveling the Link Between Noise and a Serious Sleep Disorder
Many individuals, perhaps even you or a loved one, have been told they snore loudly. It's often dismissed as a harmless, albeit annoying, nocturnal habit. However, what if that nightly rumble is more than just noise? What if it's a critical indicator of an underlying health condition that significantly impacts your well-being? The question, is all snoring sleep apnea, is a common and vital one that warrants a deep dive into the mechanisms of sleep, breathing, and potential health risks. Roughly 45% of adults snore occasionally, and 25% are habitual snorers. While not all snoring signifies sleep apnea, a significant portion of habitual snorers do suffer from this potentially severe sleep disorder. Understanding the difference is crucial, as misdiagnosing or ignoring sleep apnea can lead to a cascade of serious health complications, from cardiovascular disease to chronic fatigue and impaired cognitive function.
This comprehensive guide from SmilePedia.net will demystify the relationship between snoring and sleep apnea. We'll explore the various types of snoring, delve into the intricacies of sleep apnea, examine their causes, and discuss the latest diagnostic and treatment options available. From lifestyle modifications to advanced dental and medical interventions like CPAP therapy and oral appliances, we aim to provide you with the knowledge needed to distinguish between benign snoring and a condition that demands professional attention, ensuring you and your loved ones can breathe easier and sleep sounder.
Key Takeaways:
- Not all snoring is sleep apnea: While snoring is a primary symptom of obstructive sleep apnea (OSA), many people snore without having OSA. The key difference is obstructed breathing and oxygen drops.
- Symptoms beyond noise are red flags: If snoring is accompanied by daytime sleepiness, gasping, choking, morning headaches, or pauses in breathing, seek medical evaluation.
- Diagnosis requires a sleep study: A polysomnography (in-lab or home sleep test) is the definitive method to diagnose sleep apnea and determine its severity, typically costing $300-$5,000 depending on type and location.
- CPAP is the gold standard for OSA: Continuous Positive Airway Pressure (CPAP) therapy effectively keeps airways open. Expect to spend $800-$3,000 for a machine, with ongoing mask/accessory costs. Many insurance plans cover a significant portion as durable medical equipment (DME).
- Oral Appliance Therapy (OAT) is a dentist's role: Custom-fit dental devices can effectively treat mild to moderate OSA and primary snoring, often costing $1,800-$4,000, with some insurance coverage.
- Addressing dry mouth CPAP and mouth tape for CPAP: Common CPAP side effects like dry mouth can be managed with humidifiers. Mouth tape can help train nasal breathing but should be used cautiously and under guidance.
- Untreated sleep apnea carries significant risks: It increases the risk of high blood pressure, heart attack, stroke, diabetes, and accidents. Early diagnosis and treatment are vital.
What It Is: Snoring vs. Sleep Apnea
To understand if is all snoring sleep apnea, we first need to clearly define both conditions. While they are often intertwined, they are distinct in their nature and implications.
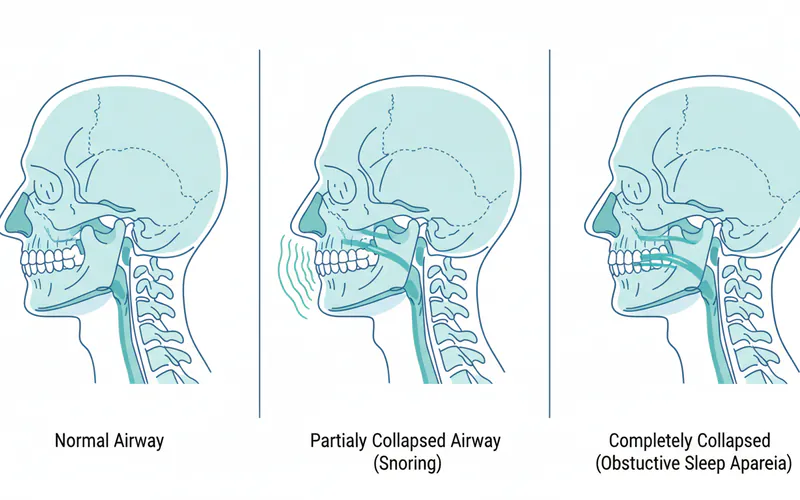
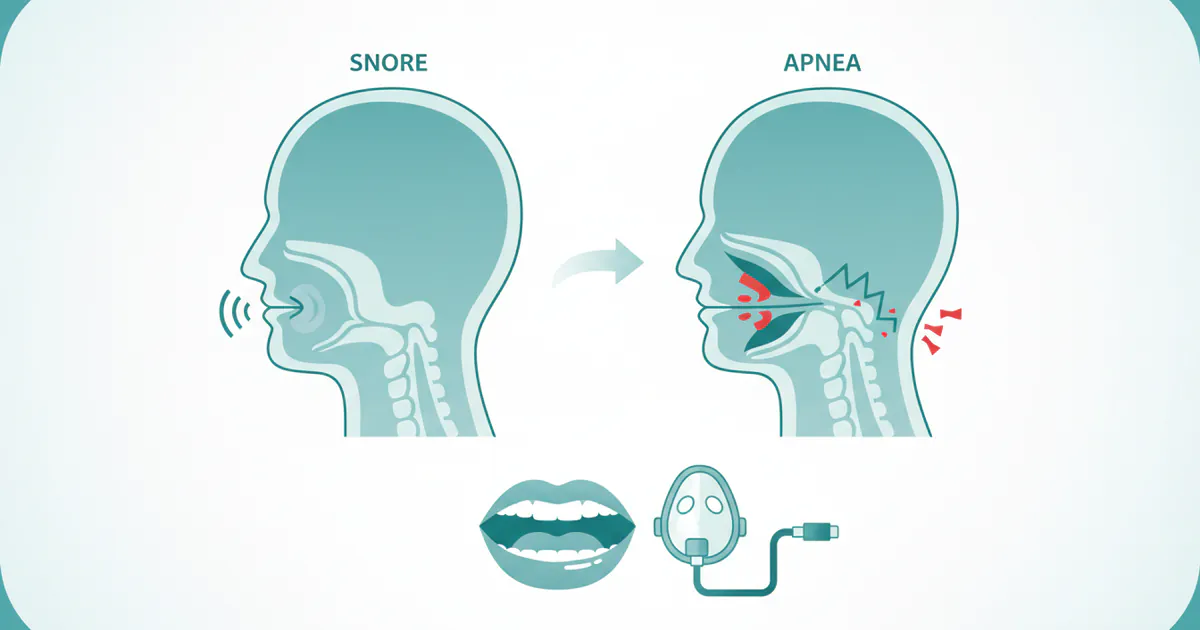
Snoring is the hoarse or harsh sound that occurs when air flows past relaxed tissues in your throat, causing the tissues to vibrate as you breathe. It's a common phenomenon, estimated to affect nearly half of all adults at some point in their lives. The sound is produced when the upper airway (nose, mouth, and throat) partially collapses during sleep, causing turbulence in the airflow.
Sleep Apnea, particularly Obstructive Sleep Apnea (OSA), is a much more serious medical condition. It is characterized by recurrent episodes of complete or partial collapse of the upper airway during sleep, leading to pauses in breathing (apneas) or shallow breathing (hypopneas). These events can last from a few seconds to over a minute and can occur hundreds of times a night. Each episode causes a drop in blood oxygen levels and typically ends with a brief awakening (often unnoticed by the sleeper) as the brain signals the body to resume breathing. Snoring is a prominent symptom of OSA, but the key differentiator is the repeated cessation of airflow and subsequent drops in oxygen saturation.
Types and Variations
Understanding the different types of snoring and sleep apnea is crucial for accurate diagnosis and effective treatment.
Types of Snoring
While snoring itself isn't classified into distinct medical types, its characteristics can offer clues about its cause and severity:
- Primary Snoring (Simple Snoring): This is snoring that is not associated with sleep apnea, frequent awakenings, or significant daytime sleepiness. It's often positional (worse on the back) and can be influenced by lifestyle factors. While not directly harmful, severe primary snoring can still disrupt a bed partner's sleep and sometimes indicates a predisposition to developing OSA later.
- Snoring with Upper Airway Resistance Syndrome (UARS): This is a milder form of sleep-disordered breathing where the airway narrows, requiring more effort to breathe, but without the full apneas or significant oxygen drops seen in OSA. It can still cause sleep fragmentation and lead to symptoms like daytime fatigue.
- Snoring associated with OSA: This is loud, disruptive snoring often punctuated by gasps, snorts, or observed breathing pauses. It's the most common and concerning type of snoring.
Types of Sleep Apnea
There are three main types of sleep apnea:
- Obstructive Sleep Apnea (OSA): This is the most common type, accounting for about 85-90% of all cases. It occurs when the muscles in the back of your throat relax too much, causing the soft tissue to collapse and block the airway. Despite efforts to breathe, air cannot reach the lungs.
- Central Sleep Apnea (CSA): This less common type occurs when your brain fails to send proper signals to the muscles that control breathing. There's no physical obstruction, but the brain simply "forgets" to tell the body to breathe for brief periods.
- Mixed (or Complex) Sleep Apnea: This is a combination of both OSA and CSA. It often begins as OSA and then develops central characteristics, especially during CPAP therapy.
Causes: Why It Happens
Both snoring and sleep apnea share many underlying causes, primarily related to the anatomy and muscle tone of the upper airway.
Causes of Snoring (and Contributing Factors to OSA)
- Relaxed Throat Muscles: During deep sleep, the muscles in your palate, tongue, and throat relax. If they relax too much, they can sag and narrow the airway.
- Obstructed Nasal Passages: A stuffy nose from allergies, a cold, or anatomical issues like a deviated septum or nasal polyps can force you to breathe through your mouth, increasing the likelihood of snoring.
- Bulky Throat Tissue: Enlarged tonsils or adenoids (especially in children), a long soft palate, or a large uvula can narrow the airway.
- Excess Weight: Fat tissue around the neck and throat can put pressure on the airway, making it more prone to collapse. This is a significant risk factor for OSA.
- Alcohol and Sedatives: These substances relax throat muscles, increasing the chance of snoring and worsening sleep apnea.
- Sleep Position: Sleeping on your back allows gravity to pull your tongue and soft palate backward, narrowing the airway.
- Age: As people age, throat muscles tend to lose tone, making them more susceptible to collapse.
- Jaw Structure: A smaller lower jaw or a recessed chin can contribute to a narrower airway.
Specific Causes of Obstructive Sleep Apnea (OSA)
In addition to the factors above, which often exacerbate OSA:
- Anatomical Abnormalities: Beyond typical bulky tissues, certain craniofacial structures can significantly predispose individuals to OSA. This includes retrognathia (receded lower jaw), micrognathia (abnormally small lower jaw), or a large tongue (macroglossia).
- Neuromuscular Conditions: Diseases that affect nerve and muscle function can reduce muscle tone in the throat.
- Endocrine Disorders: Conditions like hypothyroidism or acromegaly can lead to tissue enlargement in the airway.
Specific Causes of Central Sleep Apnea (CSA)
- Heart Failure: CSA is often associated with congestive heart failure.
- Stroke or Brain Tumor: Conditions affecting the brainstem can disrupt the brain's control over breathing.
- Opioid Use: Long-term use of opioid medications can interfere with respiratory control.
- High Altitude: Some people develop CSA temporarily at high altitudes due to changes in oxygen levels.
Signs and Symptoms
Distinguishing between primary snoring and sleep apnea often comes down to recognizing accompanying symptoms beyond just the noise.
Signs and Symptoms of Snoring (Primary Snoring)
- Loud, disruptive breathing sounds during sleep.
- No significant daytime fatigue or other health complaints directly attributed to snoring (though bed partners may experience sleep disruption).
- Often occurs only when sleeping on the back.
Signs and Symptoms of Sleep Apnea (OSA and CSA)
These symptoms indicate a higher likelihood that snoring is a symptom of sleep apnea and warrant medical evaluation:
- Loud and chronic snoring (a hallmark of OSA).
- Observed episodes of breathing cessation during sleep (reported by a bed partner).
- Gasping, choking, or snorting sounds during sleep as breathing restarts.
- Excessive daytime sleepiness (hypersomnia), even after a full night's sleep. This is a crucial indicator.
- Morning headaches.
- Dry mouth or sore throat upon waking.
- Irritability, mood changes, or depression.
- Difficulty concentrating or memory problems.
- Frequent nighttime urination (nocturia).
- High blood pressure (hypertension), which may be resistant to medication.
- Decreased libido.
Pro Tip: If a bed partner reports you stop breathing or you wake up gasping, these are strong indicators of sleep apnea and require immediate medical consultation.
Diagnosis of Sleep Apnea
If you or your bed partner suspect sleep apnea, the first step is to consult your primary care physician or a sleep specialist. A definitive diagnosis typically involves a sleep study.

- Initial Consultation: Your doctor will take a detailed medical history, discuss your symptoms, and may ask about your lifestyle and medications. They might use questionnaires (e.g., Epworth Sleepiness Scale) to assess daytime sleepiness. They may also inspect your mouth and throat for anatomical issues. Dentists specializing in sleep medicine can also initiate this process, especially if oral appliance therapy is a potential solution.
- Sleep Study (Polysomnography): This is the gold standard for diagnosing sleep apnea.
- In-Lab Polysomnography (PSG): Performed overnight in a sleep lab, this comprehensive test monitors various physiological parameters, including brain waves (EEG), eye movements (EOG), muscle activity (EMG), heart rate (ECG), blood oxygen levels (oximetry), breathing effort, airflow, and body position. A technician monitors you throughout the night.
- Home Sleep Apnea Test (HSAT): A simpler, portable version of a sleep study that you conduct at home. It typically monitors breathing effort, airflow, oxygen saturation, and heart rate. HSATs are generally used for patients with a high probability of moderate to severe OSA and no significant comorbidities. They are more convenient and less expensive but provide less comprehensive data than in-lab PSGs.
The results of the sleep study will determine an Apnea-Hypopnea Index (AHI), which measures the average number of apneas and hypopneas per hour of sleep.
- Normal: AHI < 5 events/hour
- Mild Sleep Apnea: AHI 5-15 events/hour
- Moderate Sleep Apnea: AHI 15-30 events/hour
- Severe Sleep Apnea: AHI > 30 events/hour
This AHI score, along with your symptoms, guides treatment decisions.
Treatment Options
Treatment for snoring and sleep apnea varies widely, from simple lifestyle adjustments to complex surgeries. The choice of treatment depends on the severity of the condition, the underlying causes, and individual patient preferences.
Treatment for Primary Snoring (without Apnea)
- Lifestyle Changes:
- Weight Loss: Even a modest reduction in weight can significantly decrease snoring by reducing tissue around the throat.
- Avoid Alcohol and Sedatives: Especially before bed, as they relax throat muscles.
- Change Sleep Position: Sleeping on your side rather than your back can prevent the tongue and soft palate from collapsing. Positional therapy devices (e.g., special pillows, bumper belts) can help.
- Treat Nasal Congestion: Use nasal sprays, antihistamines, or decongestants if allergies or colds are the cause.
- Nasal Devices:
- Nasal Strips: Adhesive strips placed across the bridge of the nose to widen nasal passages.
- Nasal Dilators: Devices inserted into the nostrils to keep them open.
- Oral Appliances (OTC): While some over-the-counter mouthpieces exist, they are not custom-fit and generally not recommended by dental professionals due to potential jaw issues and lack of efficacy for more severe cases.
Treatment for Sleep Apnea (and severe snoring)
The American Academy of Sleep Medicine (AASM) and American Dental Association (ADA) provide guidelines for the various treatment modalities.
1. Continuous Positive Airway Pressure (CPAP) Therapy
What it is: CPAP is the most common and generally most effective treatment for moderate to severe OSA. A machine delivers a continuous stream of air through a hose to a mask worn over your nose, mouth, or both, creating enough air pressure to keep your airway open during sleep. Pros: Highly effective, non-invasive, improves sleep quality and reduces health risks. Cons: Can be noisy, uncomfortable for some, mask fit issues, potential dry mouth CPAP, claustrophobia. Side effects & Solutions:
- Dry mouth CPAP: This is a very common complaint. The continuous airflow can dry out the mucous membranes. Solutions include using a heated humidifier integrated into the CPAP machine, ensuring a good mask seal to prevent air leaks, using a full-face mask instead of a nasal mask, or trying nasal saline sprays.
- Mask discomfort: Various mask types (nasal pillows, nasal masks, full-face masks) are available. Finding the right fit is crucial.
- Claustrophobia: Gradually increasing wear time, practicing relaxation techniques, and trying different mask styles can help.
- Aerophagia (swallowing air): Can cause bloating or gas. Adjusting CPAP pressure or using an auto-CPAP may help.
- Mouth tape for CPAP: Some individuals find taping their mouth shut helps prevent mouth breathing and improve nasal breathing while using a nasal or nasal pillow mask. This can reduce dry mouth CPAP and ensure the CPAP pressure is effectively delivered through the nose. Pro Tip: Consult your sleep doctor before using mouth tape, especially if you have nasal congestion or feel claustrophobic. Ensure it's a breathable, medical-grade tape.
2. Oral Appliance Therapy (OAT)
What it is: Custom-made dental devices, similar to a mouthguard, worn during sleep. These devices work by repositioning the lower jaw and/or tongue forward, opening the airway. OAT is often recommended for mild to moderate OSA or for patients with severe OSA who cannot tolerate CPAP. Sleep dentists are specially trained to fit and manage these appliances. Types:
- Mandibular Advancement Devices (MADs): These are the most common type, designed to move the lower jaw forward, pulling the tongue and soft palate away from the back of the throat.
- Tongue Retaining Devices (TRDs): These devices hold the tongue in a forward position using a suction bulb, preventing it from falling back and obstructing the airway. Pros: Non-invasive, portable, relatively comfortable, silent, good alternative for CPAP intolerance. Cons: Not as effective as CPAP for severe OSA, may cause jaw discomfort, teeth movement, or excessive salivation, requires regular dental follow-ups. Step-by-Step Process for OAT:
- Consultation: Initial assessment with a sleep dentist after a sleep apnea diagnosis.
- Impressions: Dentist takes impressions of your teeth and precise measurements of your jaw.
- Appliance Fabrication: A custom oral appliance is fabricated in a dental lab.
- Fitting and Adjustment: You'll return for a fitting, and the dentist will instruct you on how to gradually adjust the device.
- Follow-up Sleep Study: After a few weeks of use, another sleep study (often an HSAT) is recommended to confirm the appliance's effectiveness.
- Ongoing Care: Regular check-ups with your sleep dentist to ensure comfort, efficacy, and address any changes in your bite or jaw.
3. Surgical Interventions
Surgery is generally considered when other treatments fail or if there's a significant anatomical obstruction. Types:
- Uvulopalatopharyngoplasty (UPPP): Removes excess tissue from the back of the throat, soft palate, and uvula.
- Genioglossus Advancement (GA): Tightens the tendon connecting the tongue to the lower jaw, preventing the tongue from falling back.
- Maxillomandibular Advancement (MMA): A more aggressive surgery that moves the upper and lower jaws forward, significantly enlarging the airway.
- Tonsillectomy/Adenoidectomy: Especially effective in children with enlarged tonsils and adenoids.
- Nasal Surgery: To correct a deviated septum or remove polyps, improving nasal airflow.
- Hypoglossal Nerve Stimulation (e.g., Inspire®): An implanted device that monitors breathing and stimulates the hypoglossal nerve to move the tongue forward during sleep.
Pros: Can be curative for selected patients, especially MMA. Cons: Invasive, risks of surgery (pain, bleeding, infection, voice changes, difficulty swallowing), variable success rates, long recovery.
4. Lifestyle Modifications (for OSA)
While also treatments for primary snoring, these are crucial adjuncts for sleep apnea therapy:
- Weight Management: Significant weight loss can reduce or even eliminate OSA in some individuals.
- Positional Therapy: Devices that prevent sleeping on the back.
- Avoid Alcohol and Sedatives: Critical for OSA patients.
- Smoking Cessation: Smoking can worsen airway inflammation and swelling.
Cost and Insurance
The cost of diagnosing and treating snoring and sleep apnea can vary significantly based on the type of test, chosen treatment, geographical location, and insurance coverage.
Diagnostic Costs (US Averages)
| Service | Description | Average Cost (Without Insurance) | Insurance Coverage |
|---|---|---|---|
| Initial Consultation | Sleep specialist or dentist | $150 - $400 | Often covered |
| Home Sleep Apnea Test | Portable device for at-home monitoring | $300 - $1,000 | Often covered |
| In-Lab Polysomnography | Overnight study at a sleep center | $1,500 - $5,000 | Usually covered |
Treatment Costs (US Averages)
| Treatment Option | Description | Average Cost (Without Insurance) | Insurance Coverage |
|---|---|---|---|
| CPAP Machine | Basic to advanced models, often includes mask & tubing | $800 - $3,000 | Usually covered (DME) |
| CPAP Supplies | Masks, tubing, filters (annual replacement) | $200 - $500 per year | Often covered |
| Oral Appliance Therapy (OAT) | Custom-fit MAD or TRD from a sleep dentist | $1,800 - $4,000 | Medical (some dental) |
| UPPP Surgery | Surgical removal of throat tissue | $4,000 - $10,000 | Usually covered |
| MMA Surgery | Maxillomandibular Advancement | $30,000 - $100,000+ | Often covered |
| Hypoglossal Nerve Stim. | Implantable device (e.g., Inspire) | $25,000 - $50,000+ (device + surgery) | Increasingly covered |
| Weight Loss Programs | Varies widely, may or may not be covered | $100 - $10,000+ (program dependent) | Varies |
Insurance Coverage Details:
- Medical Insurance: Most diagnostic tests (sleep studies) and treatments like CPAP machines and surgical procedures are typically covered under medical insurance as Durable Medical Equipment (DME) or surgical benefits. You will likely be responsible for deductibles, co-pays, and co-insurance.
- Dental Insurance: While some dental plans may offer limited coverage for oral appliances, OAT is often billed through medical insurance because it's treating a medical condition (sleep apnea). Your sleep dentist's office can help you navigate this.
- Pre-authorization: Always verify coverage and pre-authorization requirements with your insurance provider before undergoing any tests or treatments.
Recovery and Aftercare
Recovery and aftercare depend entirely on the chosen treatment method.
- CPAP Therapy: Requires an adjustment period. It's crucial to use the device every night for the prescribed duration. Regular cleaning of masks, tubing, and humidifiers is essential to prevent infections and maintain efficacy. Follow-up appointments with your sleep doctor are vital for pressure adjustments and addressing any side effects like dry mouth CPAP or mask issues.
- Oral Appliance Therapy: Initial adaptation may involve minor jaw discomfort, excessive salivation, or a feeling of an altered bite in the morning, which usually resolves quickly. Regular follow-up with your sleep dentist (typically every 6-12 months) is needed to monitor device fit, efficacy, and check for any dental changes. The device itself requires daily cleaning.
- Surgical Interventions: Recovery time can range from a few days for minor nasal procedures to several weeks for more invasive throat or jaw surgeries. Pain management, dietary restrictions (soft foods), and activity limitations are common. Post-operative sleep studies may be required to assess the success of the surgery.
Prevention
While not all cases of snoring or sleep apnea are preventable, especially those linked to anatomical factors or genetics, many can be mitigated or prevented through lifestyle choices:
- Maintain a Healthy Weight: Losing even a small amount of weight can significantly reduce fatty tissue in the throat.
- Avoid Alcohol and Sedatives: Especially in the hours leading up to bedtime.
- Quit Smoking: Smoking irritates the airways, leading to inflammation and swelling.
- Sleep on Your Side: Avoid sleeping on your back.
- Manage Allergies: Keep nasal passages clear.
- Address Nasal Obstructions: Consult an ENT if you suspect a deviated septum or other structural issues.
- Regular Exercise: Improves overall muscle tone, including throat muscles.
- Good Sleep Hygiene: Establish a regular sleep schedule, ensure a comfortable sleep environment.
Risks and Complications of Untreated Sleep Apnea
Ignoring the symptoms of sleep apnea can have severe and long-lasting consequences for your health, emphasizing why it's crucial to understand that is all snoring sleep apnea warrants serious consideration.

- Cardiovascular Problems: Untreated sleep apnea significantly increases the risk of high blood pressure (hypertension), heart attack, stroke, irregular heartbeats (arrhythmias), and heart failure. Each breathing cessation puts stress on your heart.
- Type 2 Diabetes: There is a strong link between sleep apnea and insulin resistance, increasing the risk of developing or worsening type 2 diabetes.
- Daytime Fatigue and Accidents: The chronic sleep deprivation leads to excessive daytime sleepiness, increasing the risk of workplace accidents and drowsy driving accidents.
- Metabolic Syndrome: A cluster of conditions including high blood pressure, high blood sugar, excess body fat around the waist, and abnormal cholesterol levels, which together increase your risk of heart disease, stroke, and diabetes.
- Liver Problems: People with sleep apnea are more likely to have abnormal liver function test results and fatty liver disease.
- Complications with Medications and Surgery: Sleep apnea can worsen breathing problems when certain medications are used and can lead to complications during surgery due to airway management challenges.
- Mental Health Issues: Depression, anxiety, and irritability are commonly associated with chronic sleep disruption.
- Decreased Quality of Life: Chronic fatigue, poor concentration, and mood disturbances can severely impact personal relationships, work performance, and overall enjoyment of life.
Comparison Table: Snoring vs. Obstructive Sleep Apnea
| Feature | Primary Snoring (without Apnea) | Obstructive Sleep Apnea (OSA) |
|---|---|---|
| Definition | Sound of turbulent airflow through partially obstructed airway | Repeated episodes of complete/partial airway collapse with breathing pauses and oxygen drops |
| Breathing | Continuous, albeit noisy, airflow | Interrupted breathing, apneas (pauses >10s), hypopneas (shallow breaths) |
| Oxygen Levels | Generally stable | Repeated drops in blood oxygen saturation |
| Awakenings | Minimal or none, not usually associated with awakenings | Frequent, brief (often unnoticed) awakenings to resume breathing |
| Daytime Symptoms | Typically none, or mild fatigue if sleep is disturbed by noise | Excessive daytime sleepiness, morning headaches, impaired concentration, mood changes |
| Health Risks | Primarily social nuisance, potential for sleep disruption in bed partner | Significantly increased risk of hypertension, heart attack, stroke, diabetes, accidents, depression |
| Treatment Focus | Lifestyle changes, nasal dilators, positional therapy, some OTC devices | CPAP, Oral Appliance Therapy (OAT), surgery, lifestyle modifications |
Children / Pediatric Considerations
Snoring and sleep apnea are not exclusive to adults; they can also affect children, often with unique causes and symptoms. Addressing these issues early in childhood is crucial for development and long-term health.
Causes in Children
- Enlarged Tonsils and Adenoids: This is the most common cause of OSA in children. These lymphoid tissues are larger in childhood and can block the airway.
- Obesity: Increasing prevalence of childhood obesity is a growing risk factor.
- Craniofacial Abnormalities: Conditions like Down syndrome, Pierre Robin sequence, or Treacher Collins syndrome can predispose children to OSA due to structural differences.
- Neuromuscular Conditions: Conditions affecting muscle tone.
- Allergies: Chronic nasal congestion can lead to mouth breathing and airway obstruction.
Signs and Symptoms in Children
Unlike adults, children with sleep apnea may not always exhibit excessive daytime sleepiness. Instead, they might show:
- Behavioral Problems: Hyperactivity, aggression, difficulty concentrating (often misdiagnosed as ADHD).
- Poor School Performance: Due to fragmented sleep.
- Irritability and Mood Swings.
- Loud Snoring: Often accompanied by gasps, snorts, or pauses in breathing.
- Restless Sleep: Tossing and turning, unusual sleep positions (e.g., hyperextending the neck).
- Mouth Breathing: Especially at night, or persistent nasal congestion.
- Bedwetting (Enuresis): May develop or worsen.
- Slow Growth or Failure to Thrive: Due to the metabolic stress of poor sleep.
- Morning Headaches.
- Sweating excessively during sleep.
Diagnosis and Treatment in Children
- Diagnosis: A pediatric sleep specialist should evaluate any child suspected of having sleep apnea. An overnight sleep study (polysomnography) is typically recommended.
- Treatment:
- Adenotonsillectomy: Surgical removal of tonsils and adenoids is the first-line treatment for most children with OSA caused by enlarged tissues and is often highly effective.
- Weight Management: For obese children.
- Allergy Management: To reduce nasal congestion.
- Orthodontic Treatment: Rapid Maxillary Expansion (RME) or other orthodontic interventions can widen the palate and nasal passages in some cases.
- CPAP: Used for children who do not respond to surgery or have complex causes of OSA.
- Oral Appliances: Custom oral appliances can be used for some older children and adolescents.
Pro Tip: If your child snores loudly, struggles in school, or shows behavioral issues, discuss these concerns with your pediatrician. Early intervention can prevent long-term developmental and health problems.
Cost Breakdown
Understanding the financial aspect of sleep apnea diagnosis and treatment is crucial for informed decision-making. Here's a more detailed look at average US costs.
Diagnostic Costs:
- Initial Consultation with Sleep Specialist/Dentist: $150 - $400. Most insurance plans cover this.
- Home Sleep Apnea Test (HSAT): $300 - $1,000. Often fully covered by insurance, with a co-pay.
- In-Lab Polysomnography (PSG): $1,500 - $5,000. Higher end for major metropolitan areas or complex cases. Typically requires pre-authorization and will be subject to deductibles and co-insurance.
- Without Insurance: You'd pay the full amount.
- With Insurance: After meeting your deductible (e.g., $500-$2,000), you might pay 10-30% of the remaining cost.
Treatment Costs:
- CPAP Machine:
- Basic Model: $800 - $1,500
- Auto-CPAP/BiPAP: $1,500 - $3,000
- Without Insurance: Full cash price.
- With Insurance: Often covered as Durable Medical Equipment (DME). You may rent-to-own or buy, with co-pays and deductibles. Expect to pay 10-30% of the total or a fixed co-pay.
- CPAP Supplies (Annual):
- Mask (replacement every 3-6 months): $100 - $300 each
- Tubing (replacement every 3-6 months): $20 - $50 each
- Filters (monthly replacement): $5 - $20 per pack
- With Insurance: Often covered, but subject to co-pays.
- Oral Appliance Therapy (OAT): $1,800 - $4,000.
- Without Insurance: Full cash price. Payment plans often available directly from the dental office.
- With Insurance: Coverage varies greatly. Some medical insurance plans cover OAT for OSA; fewer dental plans do. It often requires a medical pre-authorization and can be subject to significant out-of-pocket costs (e.g., 20-50% co-insurance after deductible).
- Surgical Interventions: Costs can range from $4,000 to over $100,000 for complex procedures like MMA. These are generally covered by medical insurance for medically necessary cases, but often involve high deductibles and out-of-pocket maximums.
Payment Plans and Financing Options: Many providers (sleep clinics, dental offices) offer:
- Payment Plans: In-house financing options that allow you to pay over several months.
- Healthcare Credit Cards: Services like CareCredit offer special financing options.
- Flexible Spending Accounts (FSAs) and Health Savings Accounts (HSAs): These tax-advantaged accounts can be used to pay for qualified medical expenses, including sleep apnea diagnosis and treatment.
Cost-Saving Tips:
- Compare Providers: Costs for sleep studies and treatments can vary between facilities and regions.
- In-Network vs. Out-of-Network: Always use in-network providers to maximize insurance benefits.
- Generic CPAP Supplies: Some non-brand-name CPAP supplies are available and can be more affordable.
- Home Sleep Apnea Test: Opt for an HSAT if appropriate, as it's significantly cheaper than an in-lab study.
- Discuss Options: Talk openly with your doctor and dentist about the most cost-effective treatment options for your specific condition and budget.
Frequently Asked Questions
1. Is it always necessary to get a sleep study if I snore?
While not all snoring is sleep apnea, if your snoring is loud, consistent, or accompanied by symptoms like daytime fatigue, gasping, or observed breathing pauses, a sleep study is highly recommended. It's the only way to definitively diagnose sleep apnea and rule out serious health risks.
2. Can I treat my snoring without seeing a doctor?
For mild, primary snoring without other symptoms of sleep apnea, lifestyle changes like weight loss, avoiding alcohol before bed, and sleeping on your side can often help. However, if these don't work or if you suspect sleep apnea, professional medical evaluation is essential.
3. How much does a sleep apnea diagnosis cost?
The cost for a sleep apnea diagnosis ranges from approximately $300-$1,000 for a Home Sleep Apnea Test (HSAT) to $1,500-$5,000 for an in-lab Polysomnography (PSG) without insurance. With insurance, you typically pay a co-pay or a percentage after your deductible is met.
4. Is CPAP painful or difficult to get used to?
CPAP therapy is not painful, but many people experience an adjustment period. Some find the mask uncomfortable, claustrophobic, or deal with issues like dry mouth CPAP. With patience, proper mask fitting, and adjustments to settings like ramp time and humidity, most people successfully adapt.
5. What causes dry mouth CPAP and how can I prevent it?
Dry mouth CPAP is often caused by the continuous airflow drying out your mouth, especially if you mouth-breathe or have mask leaks. Using a heated humidifier with your CPAP machine, ensuring a good mask seal, or exploring a full-face mask can significantly alleviate this symptom.
6. Can mouth tape for CPAP really help?
Some individuals find mouth tape for CPAP helpful, particularly if they tend to mouth-breathe while using a nasal or nasal pillow mask. It can promote nasal breathing, potentially reducing dry mouth CPAP and ensuring better pressure delivery. However, it should only be used after consulting your sleep doctor, especially if you have nasal congestion or claustrophobia.
7. Are oral appliances as effective as CPAP?
Oral appliances are highly effective for primary snoring and mild to moderate obstructive sleep apnea. For severe OSA, CPAP generally remains the gold standard due to its higher efficacy. However, for patients who cannot tolerate CPAP, an oral appliance is an excellent alternative and can significantly improve symptoms.
8. How long does it take to see results from sleep apnea treatment?
Many people experience immediate relief from symptoms like loud snoring and observed breathing pauses on the first night of CPAP or oral appliance use. Daytime sleepiness and improved cognitive function typically improve within a few days to a few weeks of consistent use.
9. What are the long-term side effects of oral appliance therapy?
Long-term side effects can include temporary changes in bite alignment, jaw joint discomfort (TMJ issues), or minor tooth movement. Regular follow-ups with your sleep dentist are crucial to monitor and manage these potential issues, ensuring the appliance remains comfortable and effective.
10. Does insurance cover sleep apnea treatment?
Most medical insurance plans cover the diagnosis and treatment of sleep apnea, including sleep studies, CPAP machines, and often oral appliances (as a medical device). Surgical interventions are also typically covered if medically necessary. Always verify specific coverage details, deductibles, and co-pays with your insurance provider.
When to See a Dentist or Doctor
Understanding when to seek professional help is critical. While some snoring is harmless, certain signs warrant immediate medical or dental attention.
See your primary care physician or a sleep specialist if:
- You snore loudly and frequently (most nights), especially if your bed partner reports breathing pauses, gasping, or choking.
- You experience excessive daytime sleepiness, despite getting enough sleep.
- You wake up with morning headaches, a dry mouth, or a sore throat.
- You have high blood pressure, diabetes, or a history of heart attack or stroke, and also snore.
- Your child snores loudly and exhibits behavioral problems, poor school performance, or restless sleep.
See a sleep dentist if:
- You have been diagnosed with mild to moderate sleep apnea and are looking for an alternative to CPAP.
- You have severe sleep apnea but cannot tolerate CPAP therapy.
- You have significant primary snoring that is disrupting your or your partner's sleep, and lifestyle changes haven't helped.
- You are concerned about the dental implications of using a CPAP machine or are interested in custom oral appliance therapy.
- Pro Tip: Look for a dentist who is a member of the American Academy of Dental Sleep Medicine (AADSM), as they have specialized training in this field, adhering to ADA-recognized guidelines for oral appliance therapy.
Don't dismiss snoring as merely a noisy annoyance. By recognizing the potential link between is all snoring sleep apnea and its profound health implications, you can take proactive steps to protect your well-being. A conversation with a healthcare professional is the first and most important step toward quieter nights and healthier days.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Difference Between Snoring and Sleep Apnea: Complete Guide
More than 80 million Americans regularly snore, and while often dismissed as a mere nuisance, loud and persistent snoring can be a critical indicator of a much more serious underlying health condition: sleep apnea. The difference between snoring and sleep apnea is profound, impacting not just yo
February 23, 2026
Mouth Taping for Snoring: Complete Guide
Snoring. It's the nocturnal soundtrack for millions of Americans, often a source of frustration for bed partners and a potential indicator of underlying health issues for the snorer themselves. Roughly 45% of adults snore occasionally, and 25% are habitual snorers, impacting sleep quality, relat
February 23, 2026
Cpap Dry Mouth Even With Humidifier: Complete Guide
Experiencing dry mouth while using a CPAP machine, even with a humidifier, is a common and incredibly frustrating issue for millions of Americans. It can disrupt sleep, diminish the effectiveness of your sleep apnea treatment, and significantly impact your oral health. Imagine waking up every mornin
February 23, 2026
Sleep Apnea Mouth Tape: Complete Guide
You've likely heard the sound – the unmistakable rumble of snoring, echoing through the night. For many, snoring is more than just an annoyance; it's a potential warning sign of a serious underlying condition: sleep apnea. Affecting an estimated 30 million adults in the United States, sleep apne
February 23, 2026