Tmj Nerve Damage Symptoms: Complete Guide
Key Takeaways
- Experiencing persistent facial pain, numbness, or tingling can be distressing, especially when the source is unclear. While many people are familiar with general jaw pain associated with temporomandibular joint (TMJ) disorders, the less commonly understood aspect of tmj nerve damage symptoms can
Tmj Nerve Damage Symptoms: Complete Guide
Experiencing persistent facial pain, numbness, or tingling can be distressing, especially when the source is unclear. While many people are familiar with general jaw pain associated with temporomandibular joint (TMJ) disorders, the less commonly understood aspect of tmj nerve damage symptoms can be far more debilitating. Affecting an estimated 10 to 15 million adults in the United States, temporomandibular disorders (TMDs) encompass a range of issues, and nerve involvement represents a particularly challenging facet. Understanding these specific symptoms is crucial for timely diagnosis and effective treatment, potentially preventing long-term complications and significantly improving quality of life.

This comprehensive guide from SmilePedia.net aims to shed light on the intricate connection between TMJ dysfunction and nerve damage. We will explore what the temporomandibular joint is, differentiate TMD from TMJ, delve into the various causes and specific signs of nerve damage, and provide an exhaustive overview of diagnostic methods, treatment options, associated costs, and preventative measures. By the end of this article, you will have a clear understanding of what to look for, when to seek professional help, and the pathways available for relief.
Key Takeaways:
- TMJ Nerve Damage Symptoms: Often include sharp, shooting pain; numbness, tingling, or burning sensations in the face, jaw, or mouth; and sometimes muscle weakness or altered facial sensation. These are distinct from general TMD pain.
- TMD vs. TMJ: TMJ refers to the temporomandibular joint itself, while TMD describes disorders affecting this joint and surrounding structures. Nerve damage is a potential complication of TMD.
- What Does TMJ Stand For?: TMJ stands for the Temporomandibular Joint, the hinge connecting your jawbone to your skull.
- Diagnosis is Key: Accurate diagnosis relies on a detailed clinical examination, advanced imaging like MRI, and potentially neurological tests (e.g., nerve conduction studies, EMG) to pinpoint nerve involvement.
- Treatment Approaches: Range from conservative methods (medication, physical therapy, oral splints, Botox injections) to minimally invasive procedures (arthrocentesis, arthroscopy) and, in severe cases, open-joint surgery.
- Cost Considerations: Treatment costs can vary significantly, from a few hundred dollars for conservative approaches to $10,000-$50,000+ for complex surgeries. Insurance coverage often depends on whether it's classified as medical or dental.
- Early Intervention: Prompt recognition of nerve damage symptoms and seeking professional help is vital to prevent chronic pain and irreversible nerve damage.
What It Is / Overview
To understand TMJ nerve damage, it's essential to first clarify what the TMJ is and how it relates to temporomandibular disorders (TMDs).
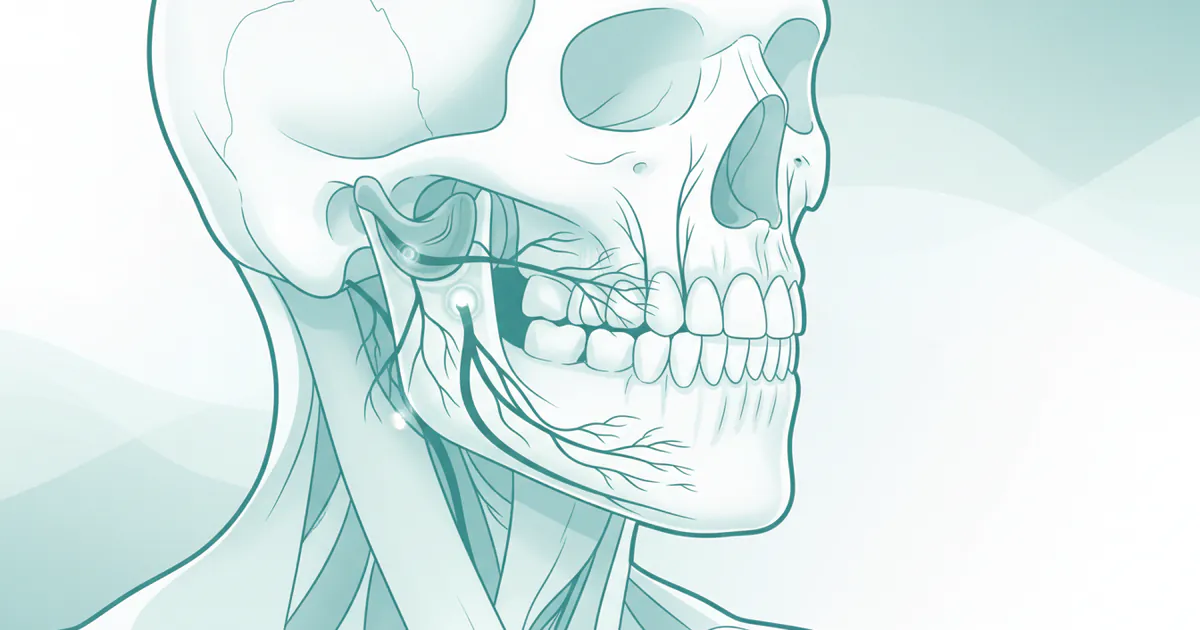
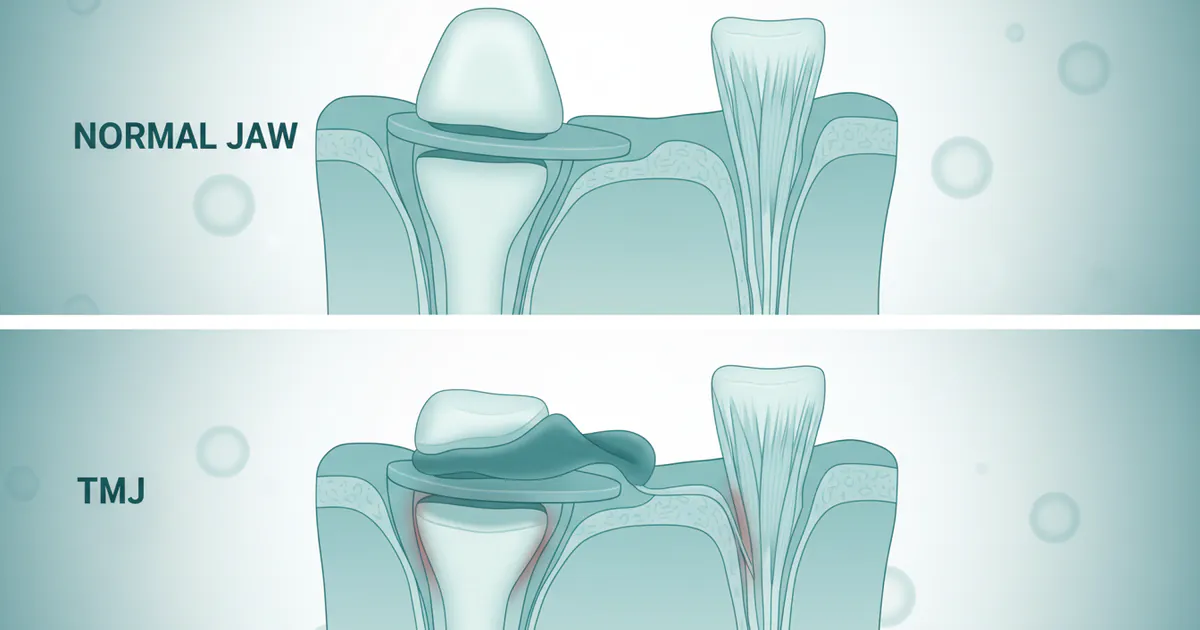
The TMJ, or Temporomandibular Joint, is the complex hinge joint that connects your mandible (jawbone) to your temporal bones of the skull, located just in front of your ears on both sides of your head. This joint is unique because it combines a hinge action with sliding motions, allowing you to open and close your mouth, move your jaw side-to-side, and forward and back, which are all crucial for speaking, chewing, and yawning. The TMJ is comprised of bone (condyle of the mandible and temporal bone), cartilage, and a small, shock-absorbing disc located between the bones. It's surrounded by a complex network of muscles, ligaments, and blood vessels.
What Does TMJ Stand For? As mentioned, TMJ stands for Temporomandibular Joint. Many people mistakenly use "TMJ" to refer to the disorder itself, but technically, the disorder is called TMD, or Temporomandibular Disorder.
TMD vs. TMJ:
- TMJ: Refers specifically to the joint itself.
- TMD: Refers to a collection of conditions that cause pain and dysfunction in the jaw joint and the muscles that control jaw movement. These disorders can arise from various issues affecting the joint, muscles, or associated structures.
Nerve damage related to the TMJ typically occurs when the delicate nerves in and around the joint are compressed, stretched, irritated, or directly injured. The primary nerve associated with this region is the trigeminal nerve (Cranial Nerve V), which has three main branches: ophthalmic, maxillary, and mandibular. The mandibular branch is particularly relevant to the TMJ as it supplies sensation to the lower jaw, teeth, and parts of the face, and controls the muscles of mastication (chewing). Other nerves, such as the facial nerve (Cranial Nerve VII), can also be affected, though less commonly in primary TMJ issues. When these nerves are compromised, it leads to the distinct tmj nerve damage symptoms that are the focus of this guide.
Types of Nerve Involvement in TMD
Nerve involvement in temporomandibular disorders can manifest in several ways, affecting different aspects of nerve function. Understanding these distinctions helps in accurate diagnosis and targeted treatment.
-
Sensory Neuropathy: This is the most common form of nerve damage associated with TMD, primarily affecting the sensory fibers of the trigeminal nerve. Symptoms include:
- Paresthesia: Abnormal sensations like tingling, "pins and needles," or prickling, often in the face, lips, or tongue.
- Numbness (Hypoesthesia/Anesthesia): Reduced or complete loss of sensation in affected areas.
- Dysesthesia: Unpleasant, abnormal sensations, such as burning, itching, or a crawling feeling, which can be spontaneous or evoked.
- Hyperesthesia: Increased sensitivity to stimuli that are normally not painful.
- Allodynia: Pain from stimuli that are not normally painful (e.g., light touch).
- Neuralgia-like Pain: Sharp, shooting, electric shock-like pain, often triggered by movement or touch, similar to trigeminal neuralgia.
-
Motor Neuropathy: Less common than sensory issues in direct TMJ nerve damage, but can occur if motor branches of the trigeminal nerve or the facial nerve are affected. This involves impairment of muscle function.
- Weakness or Paresis: Difficulty in moving the jaw or facial muscles.
- Muscle Atrophy: Wasting away of muscles due to lack of nerve supply.
- Facial Asymmetry: If the facial nerve (Cranial Nerve VII) is affected, leading to drooping or inability to move parts of the face. This is often more associated with direct trauma or surgery rather than primary TMJ dysfunction.
-
Autonomic Nerve Involvement: While rare, chronic inflammation or injury around the TMJ can sometimes impact autonomic nerve fibers, leading to symptoms like:
- Altered sweating patterns in the face.
- Changes in blood flow to facial tissues.
-
Referred Pain: While not direct nerve damage, it's crucial to mention that irritation of nerves around the TMJ can cause pain to be perceived in other areas, such as the ears, temples, neck, or even teeth, complicating diagnosis. This is due to the complex network of nerve pathways.
Causes / Why It Happens
TMJ nerve damage doesn't occur in isolation; it's typically a consequence of underlying issues within the temporomandibular joint or surrounding structures. Here are the primary causes and contributing factors:

-
Disc Displacement: The most common cause of TMD. The small, cartilaginous disc normally acts as a cushion between the bones of the joint. If this disc slips out of its proper position (often anteriorly), it can:
- Compress Nerves: The posterior attachment of the disc is highly innervated. Displacement can compress these delicate nerve endings, leading to pain and sensory changes.
- Bone-on-Bone Contact: In severe cases, disc degeneration can lead to the condyle of the jawbone grinding directly against the temporal bone, causing inflammation and direct irritation or damage to nearby nerves.
-
Trauma:
- Direct Impact: A blow to the jaw, face, or head (e.g., sports injury, fall, car accident) can directly injure nerves or cause severe joint displacement that impinges nerves.
- Whiplash: Neck injuries from sudden stops or impacts can affect the biomechanics of the jaw, leading to nerve irritation.
-
Chronic Muscle Spasm and Myofascial Pain:
- Sustained clenching or grinding of teeth (bruxism) or chronic stress can lead to persistent tension and spasms in the muscles of mastication (masseter, temporalis, pterygoids).
- These tight, painful muscles can put pressure on nearby nerves or create "trigger points" that refer pain along nerve pathways, mimicking nerve damage.
-
Arthritis:
- Osteoarthritis: Degenerative changes in the joint cartilage and bone can lead to inflammation, joint space narrowing, and the formation of bone spurs (osteophytes), all of which can irritate or compress adjacent nerves.
- Rheumatoid Arthritis and Psoriatic Arthritis: Systemic inflammatory conditions can affect the TMJ, causing destructive changes that indirectly lead to nerve involvement.
-
Iatrogenic Injury (Medical/Dental Procedures):
- TMJ Surgery: While often necessary, surgical procedures on the TMJ carry a risk of direct nerve damage (e.g., trigeminal, facial nerve branches) during incision, retraction, or manipulation of tissues.
- Dental Procedures: Prolonged mouth opening during extensive dental work, wisdom tooth extraction, or root canal therapy in the posterior mandible can, in rare cases, cause stretching or compression of nerves (e.g., lingual nerve, inferior alveolar nerve), leading to temporary or permanent neuropathy.
-
Infection and Inflammation:
- Severe infections in or around the TMJ can cause swelling and inflammation that compress nearby nerves.
- Chronic inflammation, even without infection, can also lead to nerve sensitization and pain.
-
Systemic Conditions:
- Though less common, certain neurological disorders, connective tissue diseases, or even tumors (very rare in the TMJ region) can present with nerve-related symptoms that might be initially misdiagnosed as TMD.
Signs and Symptoms
Identifying tmj nerve damage symptoms specifically requires careful attention, as they can sometimes overlap with general TMD discomfort or even mimic other conditions like dental pain or sinus issues. However, certain characteristics strongly suggest nerve involvement.
Key Symptoms Indicating Nerve Damage:
-
Persistent or Intermittent Facial Pain:
- Quality: Often described as sharp, shooting, electric shock-like, burning, stabbing, or tingling. This differs from the dull, aching pain common in muscle-related TMD.
- Location: Can be unilateral (one side) or bilateral, affecting the jaw, cheek, temple, ear, or around the eye. Pain can radiate into the neck or shoulder.
- Triggers: May be spontaneous or triggered by specific movements (chewing, talking, yawning), light touch, or temperature changes.
-
Altered Sensations (Paresthesia/Dysesthesia):
- Numbness: A complete loss of sensation, or a feeling of "deadness" in parts of the face, lips, tongue, or inside the mouth.
- Tingling or "Pins and Needles": A prickling sensation, often preceding or accompanying numbness.
- Burning: A persistent, uncomfortable sensation, as if the skin or tissue is hot.
- Hypersensitivity (Hyperesthesia/Allodynia): Unusually heightened sensitivity to touch, temperature, or pressure in the affected area, where even light contact can cause severe discomfort.
-
Motor Dysfunction:
- Muscle Weakness: Difficulty in chewing, biting, or moving the jaw. This might manifest as feeling like your jaw is "giving out" or simply lacking the power to chew certain foods.
- Difficulty with Jaw Movement: Limited jaw opening (trismus), deviation of the jaw when opening, or a feeling of the jaw "locking." While these can be general TMD symptoms, if accompanied by nerve damage, they can be more severe or resistant to typical treatments.
- Facial Asymmetry/Drooping: If the facial nerve (responsible for facial expressions) is involved, you might notice one side of your face drooping, difficulty smiling, or inability to close an eye fully. This is less common but a serious indicator.
-
Auditory Symptoms:
- Tinnitus: A persistent ringing, buzzing, or hissing sound in one or both ears.
- Muffled Hearing or Ear Fullness: A sensation of pressure or blockage in the ear, often without an actual ear infection.
- Vertigo or Dizziness: While less common, nerve irritation or inflammation near the TMJ can sometimes influence balance and lead to feelings of dizziness.
-
Headaches and Migraines:
- Frequent and severe headaches, often originating in the temple or behind the eye, can be a symptom. These might be distinct from tension headaches and often described as migraines.
-
Tooth Sensitivity or Pain:
- Referred pain from nerve irritation can sometimes manifest as tooth pain in apparently healthy teeth, leading to unnecessary dental procedures if the underlying TMJ issue is missed.
Pro Tip: Keep a detailed journal of your symptoms. Note the type of pain (sharp, dull, burning), its location, intensity (on a scale of 1-10), what triggers it, and what provides relief. This information is invaluable for your dentist or specialist to accurately diagnose nerve involvement.
Diagnosis of TMJ Nerve Damage
Accurately diagnosing tmj nerve damage symptoms requires a comprehensive approach, often involving a team of specialists.
-
Detailed Medical History and Physical Examination:
- Patient Interview: The dentist or oral surgeon will ask about your symptoms, their onset, triggers, duration, and any previous treatments. This is where your symptom journal becomes very useful.
- Palpation: The clinician will gently feel your jaw joints and the muscles around your jaw, head, and neck to identify areas of tenderness, spasm, or clicking/popping sounds.
- Range of Motion Assessment: Checking how wide you can open your mouth, and if there's any deviation or limitation in jaw movement.
- Neurological Exam: Specific tests to assess sensory function (touch, temperature, pinprick) and motor function (muscle strength, reflexes) in the face and jaw to pinpoint nerve involvement.
-
Imaging Studies:
- X-rays: Provide basic images of the bony structures of the joint, primarily useful for ruling out gross anatomical abnormalities or severe degenerative changes.
- Magnetic Resonance Imaging (MRI): This is often considered the gold standard for diagnosing disc displacement and evaluating the soft tissues of the TMJ, including the disc, ligaments, and potential inflammation or swelling that could be compressing nerves. It can also show fluid accumulation or changes in the joint space.
- Computed Tomography (CT) Scan / Cone Beam CT (CBCT): Provides detailed images of the bony structures, useful for identifying fractures, arthritis, or other bone pathologies that might be irritating nerves. CBCT offers high-resolution 3D images with lower radiation dose.
- Ultrasound: Can be used to assess muscle activity and joint inflammation, though less common for direct nerve damage diagnosis.
-
Specialized Neurological Tests:
- Nerve Conduction Studies (NCS): Measure how fast electrical signals travel through a nerve. Slowed conduction or blockages can indicate nerve damage.
- Electromyography (EMG): Assesses the electrical activity of muscles. Abnormalities can indicate nerve damage affecting muscle function. These tests are crucial for objectively confirming nerve damage and differentiating it from other sources of pain.
- Quantitative Sensory Testing (QST): Measures a patient's perception of different stimuli (e.g., heat, cold, vibration) to assess the function of small nerve fibers.
-
Diagnostic Nerve Blocks:
- In some cases, a local anesthetic can be injected near a suspected nerve or joint. If the pain is temporarily relieved, it strongly suggests that nerve or joint as the source of the symptoms.
``
Treatment Options
Treating tmj nerve damage symptoms is often multifaceted, aiming to alleviate pain, restore function, and address the underlying cause of nerve compression or irritation. The approach typically progresses from conservative, non-invasive methods to more invasive interventions if necessary.

1. Conservative Treatments (First-Line Approach)
- Medications:
- NSAIDs (Nonsteroidal Anti-inflammatory Drugs): Over-the-counter options like ibuprofen or naproxen reduce pain and inflammation.
- Muscle Relaxants: Prescribed for muscle spasms, which can contribute to nerve irritation. (e.g., cyclobenzaprine, tizanidine).
- Neuropathic Pain Medications: For chronic nerve pain (e.g., gabapentin, pregabalin, tricyclic antidepressants like amitriptyline, SNRIs like duloxetine). These modify nerve signals.
- Corticosteroids: Oral or injected directly into the joint to reduce severe inflammation.
- Oral Appliances (Splint Therapy):
- Custom-made clear acrylic mouthguards worn over the teeth, primarily at night.
- Pros: Reduces clenching/grinding forces, repositions the jaw, reduces stress on the TMJ, helps relax jaw muscles.
- Cons: Requires consistent use, can be uncomfortable initially, doesn't cure underlying issues if not combined with other therapies, average cost $300-$800.
- Physical Therapy (PT):
- Pros: Jaw exercises to improve range of motion, strengthen muscles, and reduce pain. Massage, stretching, heat/cold therapy, ultrasound, and TENS (Transcutaneous Electrical Nerve Stimulation) units can alleviate muscle tension and improve nerve health. Posture correction is also a key component.
- Cons: Requires patient compliance, can be slow to show results. Average cost $75-$200 per session (often 6-12 sessions).
- Botox (Botulinum Toxin) Injections:
- Pros: Injected into jaw muscles (masseter, temporalis) to relax them, reducing clenching/grinding forces and alleviating pressure on nerves. Can also directly reduce neuropathic pain by affecting neurotransmitters.
- Cons: Temporary (effects last 3-6 months), requires repeat injections, cost $500-$1500 per treatment, potential for temporary weakness in chewing muscles.
- Lifestyle Modifications & Self-Care:
- Soft diet, avoiding hard/chewy foods.
- Stress management techniques (meditation, yoga).
- Applying moist heat or ice packs.
- Avoiding extreme jaw movements (wide yawning, yelling).
- Good posture and ergonomic adjustments.
2. Minimally Invasive Procedures
- Arthrocentesis:
- Pros: Involves inserting small needles into the joint to lavage (wash out) inflammatory mediators and remove adhesions. Can improve disc mobility and reduce pain. Often done with local anesthesia.
- Cons: May require repeat procedures, not effective for severe structural damage. Average cost $1,500-$3,000.
- Arthroscopy:
- Pros: A minimally invasive surgical procedure where a small incision is made, and an arthroscope (a tiny camera) is inserted into the joint. The surgeon can visualize the joint, remove inflammatory tissue, smooth rough surfaces, or reposition the disc. Less recovery time than open surgery.
- Cons: Limited in scope for severe structural problems, requires general anesthesia. Average cost $5,000-$10,000.
3. Surgical Interventions (For Severe Cases)
- Open-Joint Surgery (Arthroplasty):
- Pros: Reserved for cases with severe structural damage, extensive disc displacement that doesn't respond to conservative treatment, or degenerative joint disease. Procedures include disc repair/repositioning, removal of bone spurs, or in severe cases, partial or total joint replacement.
- Cons: More invasive, longer recovery time, higher risks (infection, facial nerve damage, prolonged swelling), potential for scarring. Average cost $15,000-$50,000+.
- Nerve Decompression/Repair:
- In very rare instances, if a specific nerve is severely entrapped or damaged (e.g., post-surgical injury), a neurosurgeon or oral surgeon might perform microsurgical nerve decompression or repair.
- Pros: Direct addressing of severe nerve pathology.
- Cons: Highly specialized, high risk, not a primary TMJ treatment.
Pro Tip: Always seek a second opinion, especially for invasive procedures. Consult with an oral and maxillofacial surgeon or a TMJ specialist who has extensive experience in diagnosing and treating complex TMD and nerve involvement.
Step-by-Step Process: What to Expect During Treatment
Navigating treatment for tmj nerve damage symptoms can feel overwhelming, but understanding the typical process can help you prepare.
-
Initial Consultation and Comprehensive Evaluation (Weeks 1-2):
- Appointment 1: Detailed medical and dental history, symptom discussion, physical examination of the jaw, head, and neck. Your symptom journal will be crucial here.
- Appointment 2 (if needed): Referral for specialized imaging (MRI, CBCT) and/or neurological tests (NCS, EMG) to confirm nerve involvement and assess the extent of joint damage.
- Diagnosis: Based on clinical findings and test results, the specialist will provide a diagnosis and discuss initial treatment options.
-
Conservative Treatment Phase (Weeks 3-12+):
- Medication Management: Prescription of pain relievers, muscle relaxants, or neuropathic pain medications. Adjustments may be made based on effectiveness and side effects.
- Oral Appliance Fitting: If indicated, impressions will be taken for a custom oral splint. You'll receive instructions on its use and care.
- Physical Therapy Referral: Referral to a physical therapist specializing in craniomandibular disorders. Sessions will include exercises, massage, and other modalities.
- Lifestyle Counseling: Advice on diet, stress reduction, posture, and avoiding habits that exacerbate symptoms.
- Follow-up Appointments: Regular check-ups with your specialist to monitor progress, adjust medications, and evaluate the effectiveness of the splint and PT.
-
Intermediate Interventions (If Conservative Fails, Months 3-6+):
- If conservative treatments don't provide sufficient relief for your tmj nerve damage symptoms, the next step might be:
- Botox Injections: If muscle spasm is a significant contributor, Botox injections may be recommended. This is an office procedure.
- Joint Injections: Corticosteroid injections into the TMJ to reduce inflammation.
- Arthrocentesis: A minimally invasive procedure performed in an outpatient setting, often under local anesthesia or light sedation. Recovery is typically quick.
-
Surgical Consideration (If All Else Fails, Months 6+):
- If significant structural damage or persistent nerve impingement requires surgical correction, a discussion about arthroscopy or open-joint surgery will occur.
- Pre-surgical Planning: Detailed imaging, consultations with oral surgeons, and possibly other specialists.
- Surgery: Performed under general anesthesia. The length of the procedure and hospital stay depend on the complexity.
- Post-operative Care: Pain management, wound care, and early rehabilitation begin almost immediately.
-
Rehabilitation and Long-Term Management (Ongoing):
- Physical Therapy: Crucial post-surgery or after injections to regain jaw function, strength, and reduce scar tissue formation.
- Follow-up Care: Regular check-ups to monitor recovery, manage any residual symptoms, and prevent recurrence. This may include continued use of an oral appliance or ongoing self-care practices.
``
Cost and Insurance
Understanding the financial aspect of treating tmj nerve damage symptoms is crucial, as costs can vary significantly based on the severity of the condition, the type of treatment, and geographic location within the US.
Average US Price Ranges (Estimated)
| Service/Treatment | Low Range (USD) | Mid Range (USD) | High Range (USD) | Notes |
|---|---|---|---|---|
| Initial Consultation/Exam | $150 | $300 | $500 | Specialist consultation (oral surgeon, neurologist). |
| Basic Dental X-rays | $25 | $75 | $150 | Performed by general dentist. |
| MRI of TMJ (Unilateral/Bilateral) | $500 | $1,500 | $3,000 | Can be significantly higher without insurance negotiation. |
| CBCT Scan | $300 | $600 | $1,000 | |
| Nerve Conduction Study (NCS)/EMG | $500 | $2,000 | $5,000 | Depending on the number of nerves tested and complexity. |
| Oral Splint/Nightguard | $300 | $800 | $1,500 | Custom-made; varies by material and complexity. |
| Physical Therapy (per session) | $75 | $150 | $250 | Out-of-pocket, before insurance. Often requires multiple sessions (6-12+). |
| Botox Injections (per treatment) | $500 | $1,000 | $1,500 | Varies by units used and provider; typically needs repeat injections every 3-6 months. |
| Corticosteroid Joint Injection | $200 | $500 | $1,000 | Per joint, plus facility and doctor's fee. |
| Arthrocentesis (outpatient) | $1,500 | $3,000 | $5,000 | Includes facility, anesthesia, and surgeon fees. |
| TMJ Arthroscopy | $5,000 | $10,000 | $15,000 | Includes surgeon, anesthesia, facility fees; can be higher based on complexity. |
| Open-Joint TMJ Surgery | $15,000 | $30,000 | $50,000+ | Highly variable, includes surgeon, anesthesia, hospital stay, and potential hardware. Total joint replacement could exceed $75,000-$100,000. |
| Neuropathic Medications | $10 | $100 | $500+ | Monthly, depends on drug, dosage, and insurance coverage. |
Insurance Coverage Details
This is a critical area because TMD treatment often falls into a grey area between medical and dental insurance.
-
Medical Insurance: Most comprehensive medical insurance plans should cover the diagnosis and treatment of conditions affecting the TMJ, especially if they involve nerve damage, as these are considered medical conditions.
- What's usually covered: Consultations with specialists (oral surgeons, neurologists), diagnostic imaging (MRI, CT, NCS/EMG), physical therapy, prescription medications, Botox injections (if medically necessary and pre-approved), and surgical procedures (arthroscopy, open-joint surgery).
- What might not be covered fully: Oral splints/nightguards are sometimes considered "dental appliances" and may only be partially covered by medical insurance or require specific medical necessity documentation.
- Pre-authorization: Many medical treatments for TMD, particularly injections and surgeries, require extensive pre-authorization from your insurance company. This involves submitting detailed medical records, diagnostic test results, and a letter of medical necessity from your doctor.
- Deductibles and Co-pays: Expect to pay your plan's deductible and co-pays, even with good coverage.
-
Dental Insurance:
- Dental insurance typically covers preventative care, fillings, crowns, and oral surgery (like extractions), but rarely covers complex TMD treatments or nerve damage directly.
- What might be covered: Oral splints might be partially covered if coded as a "bite appliance" or "orthopedic appliance" under your dental plan, but often with significant limitations or a high patient co-pay.
- Limited Scope: Dental plans generally do not cover diagnostic tests like MRIs, neurological exams, physical therapy, or major TMJ surgeries.
Pro Tip: Always confirm coverage with both your medical and dental insurance providers before starting any major treatment. Get pre-authorization in writing whenever possible. Ask for CPT (Current Procedural Terminology) codes from your doctor's office to directly inquire with your insurer.
Recovery and Aftercare
Recovery from tmj nerve damage symptoms treatment varies widely depending on the chosen intervention, but consistent aftercare is vital for optimal outcomes and preventing recurrence.

Post-Treatment Care Instructions:
-
Medication Adherence:
- Continue all prescribed medications (pain relievers, anti-inflammatories, muscle relaxants, neuropathic drugs) as directed. Do not stop without consulting your doctor, especially for neuropathic medications which may require tapering.
-
Oral Appliance Use:
- If prescribed a splint or nightguard, wear it consistently as instructed (e.g., nightly, or throughout the day as advised). This protects the joint and teeth, and maintains proper jaw alignment. Clean it daily.
-
Physical Therapy and Home Exercises:
- Crucial for healing: Adhere strictly to your physical therapy regimen. This typically includes gentle jaw stretches, strengthening exercises, massage techniques, and posture correction exercises.
- Consistency is key: Regular, gentle exercises help improve blood flow, reduce stiffness, prevent muscle atrophy, and re-educate jaw muscles.
- Avoid overdoing it: Listen to your body and avoid movements that cause sharp pain.
-
Dietary Modifications:
- Soft Food Diet: Especially important after injections or surgery. Stick to soft, non-chewy foods (smoothies, yogurt, mashed potatoes, well-cooked pasta, soft fish, eggs) for several days to weeks.
- Gradual Reintroduction: Slowly reintroduce harder foods as directed by your healthcare provider, paying attention to any discomfort. Avoid chewing gum, nuts, hard candies, and tough meats.
-
Pain and Swelling Management:
- Ice/Heat: Apply ice packs (20 minutes on, 20 minutes off) for the first 24-48 hours post-procedure to reduce swelling. Then switch to moist heat to relax muscles.
- Elevation: Keep your head elevated, especially while sleeping, to minimize swelling.
-
Activity Restrictions:
- Limited Jaw Movement: Avoid wide yawning, yelling, or any strenuous jaw movements initially. Support your jaw when yawning.
- Rest: Ensure adequate rest to allow your body to heal. Avoid strenuous physical activity that could strain your jaw or neck, especially after surgery.
-
Surgical Site Care (if applicable):
- Wound Care: Follow specific instructions for cleaning surgical incisions and managing dressings. Watch for signs of infection (redness, pus, fever).
- Oral Hygiene: Maintain good oral hygiene, but be gentle around the surgical site. Use a soft-bristled toothbrush.
-
Regular Follow-up Appointments:
- Attend all scheduled follow-up visits with your oral surgeon, dentist, or specialist. These appointments are essential to monitor your healing, adjust treatment, and address any concerns.
-
Stress Management:
- Stress and anxiety can exacerbate TMD symptoms and bruxism. Continue practicing stress-reduction techniques (mindfulness, deep breathing, meditation).
-
Long-Term Monitoring:
- For chronic conditions or after significant procedures, long-term monitoring may be necessary to ensure continued relief and address any recurrence of tmj nerve damage symptoms. This might involve periodic check-ups or continued use of an oral appliance.
Recovery timelines:
- Conservative treatments: Symptom improvement can take weeks to months.
- Injections/Arthrocentesis: A few days to a few weeks for initial recovery, with full effects seen over several weeks.
- Arthroscopy: 1-2 weeks for initial recovery, with full recovery and rehabilitation taking 2-3 months.
- Open-joint surgery: 4-6 weeks for initial recovery, with full functional recovery and rehabilitation potentially taking 6 months to a year or longer.
Prevention
While not all cases of TMD and subsequent nerve damage are preventable, several strategies can significantly reduce your risk and mitigate the severity of tmj nerve damage symptoms.
-
Manage Stress:
- Stress is a major contributor to bruxism (teeth clenching and grinding), which puts immense pressure on the TMJ and surrounding nerves.
- Practice stress-reduction techniques: meditation, yoga, deep breathing exercises, regular physical activity, hobbies.
-
Address Bruxism and Clenching:
- If you grind or clench your teeth, especially at night, consider a custom-fitted nightguard (oral splint) prescribed by your dentist. This creates a barrier between your upper and lower teeth, protecting them and reducing stress on the TMJ.
- Be mindful of clenching during the day and consciously try to relax your jaw muscles.
-
Maintain Good Posture:
- Poor posture, especially "forward head posture" (head jutting forward), can strain the neck and jaw muscles, contributing to TMD.
- Practice good ergonomic habits at your workstation and while using electronic devices. Ensure your head is aligned over your shoulders.
-
Avoid Excessive Jaw Movements and Habits:
- Limit wide yawning. If you must yawn widely, try to support your chin with your hand.
- Avoid excessive gum chewing, nail biting, or chewing on non-food items (pens, ice).
- Cut food into smaller pieces to avoid large bites.
- Avoid consistently chewing on only one side of your mouth.
-
Protect Your Jaw from Trauma:
- Wear a mouthguard during contact sports to protect your jaw from impact injuries.
- Be cautious during activities that could lead to head or facial trauma.
-
Regular Dental Check-ups:
- Routine dental visits allow your dentist to identify early signs of bruxism, malocclusion (bad bite), or early TMD symptoms.
- Early intervention can prevent the progression of TMD to nerve involvement.
-
Address Malocclusion:
- If you have a significant bite problem that puts uneven stress on your TMJ, discuss orthodontic treatment or restorative dental work with your dentist to correct it.
-
Healthy Diet:
- Ensure a balanced diet to support overall joint and nerve health.
- Stay hydrated, as dehydration can contribute to muscle cramps and pain.
Risks and Complications
Left untreated, or even sometimes despite treatment, tmj nerve damage symptoms can lead to several risks and complications, impacting both physical and mental well-being.
-
Chronic Pain Syndrome:
- If nerve damage persists, the nervous system can become "sensitized," leading to chronic neuropathic pain that is difficult to manage and may not fully resolve even after the initial cause is addressed. This can be profoundly debilitating.
-
Permanent Nerve Damage:
- Prolonged compression, severe trauma, or irreversible changes to nerve tissue can result in permanent loss of sensation (anesthesia), persistent tingling (paresthesia), or chronic pain that may not respond to conventional treatments.
-
Functional Impairment:
- Limited Jaw Movement: Persistent pain, muscle weakness, or joint damage can severely restrict your ability to open your mouth, chew, and speak normally.
- Difficulty Eating: A soft diet may become a permanent necessity, leading to nutritional deficiencies and a reduced quality of life.
- Speech Impediments: If muscles controlling speech are affected, or due to restricted jaw movement.
-
Psychological Impact:
- Chronic pain and functional limitations significantly increase the risk of depression, anxiety, sleep disturbances, and social isolation. The constant discomfort and frustration can lead to a reduced quality of life.
-
Nutritional Deficiencies:
- If severe jaw pain or motor weakness prevents adequate chewing, patients may struggle to maintain a balanced diet, leading to weight loss or nutritional deficiencies.
-
Surgical Complications:
- While surgery is a last resort, it carries its own risks, including:
- Infection: At the surgical site.
- Further Nerve Damage: Accidental injury to the trigeminal or facial nerve during the procedure, potentially causing new or worsened sensory loss, pain, or facial weakness/paralysis.
- Scar Tissue Formation: Can lead to limited joint mobility.
- Bleeding: Excessive bleeding during or after surgery.
- Anesthesia Risks: All general anesthesia carries inherent risks.
- Failure of Surgery: The procedure may not fully alleviate symptoms, or they may recur.
- While surgery is a last resort, it carries its own risks, including:
-
Dental Problems:
- Untreated bruxism can lead to excessive tooth wear, fractures, and periodontal (gum) disease.
- Malocclusion may worsen over time.
Comparison Tables
To help differentiate between symptoms and understand treatment options, here are two comparison tables.

Comparison of General TMD Symptoms vs. TMJ Nerve Damage Symptoms
| Feature | General TMD Symptoms | TMJ Nerve Damage Symptoms |
|---|---|---|
| Type of Pain | Dull ache, throbbing, soreness, tightness. | Sharp, shooting, electric shock-like, burning, stabbing. |
| Location of Pain | Jaw joint, jaw muscles, temples, ear area, neck. | Jaw, face, lips, tongue, specific nerve pathways. |
| Associated Sensations | Tenderness, stiffness, clicking/popping, limited opening. | Numbness, tingling, "pins and needles," hypersensitivity, allodynia. |
| Triggers | Chewing, wide opening, stress, cold. | Light touch, wind, specific movements, temperature changes (often more severe). |
| Muscle Involvement | Muscle fatigue, spasm, weakness (general discomfort). | Muscle weakness (specific, e.g., difficulty chewing), facial asymmetry (if facial nerve affected). |
| Auditory Symptoms | Earache, fullness, occasional tinnitus. | Persistent tinnitus, muffled hearing, dizziness, vertigo (if nerve-related). |
| Duration of Pain | Often intermittent, worse with activity. | Can be constant, or episodic with severe, short bursts of pain. |
| Response to Basic Relief | Responds to NSAIDs, heat/cold, rest. | Often less responsive to standard pain relievers, may require neuropathic medications. |
| Key Differentiator | Mechanical joint/muscle issue, inflammation. | Direct irritation, compression, or injury to nerve fibers. |
``
Comparison of TMJ Nerve Damage Treatment Approaches
| Treatment Type | Description | Pros | Cons | Estimated Cost (USD) |
|---|---|---|---|---|
| Conservative | Medications, physical therapy, oral splints, stress management, lifestyle changes. | Non-invasive, low risk, often effective for mild-moderate cases. | Requires patient compliance, slow results, may not resolve severe cases. | $300 - $3,000 (per approach) |
| Injections | Botox, corticosteroids into joint/muscles. | Targeted relief, minimally invasive, quicker results than PT alone. | Temporary relief (3-6 months), requires repeat treatments, potential side effects. | $200 - $1,500 (per injection/session) |
| Minimally Invasive Surgery | Arthrocentesis (joint lavage), Arthroscopy (scope-guided repair). | Less invasive than open surgery, quicker recovery, can treat disc/inflammation. | Limited scope for severe damage, anesthesia risks, not always permanent fix. | $1,500 - $15,000 |
| Open-Joint Surgery | Disc repair/repositioning, joint replacement. | Addresses severe structural damage, can offer long-term solution. | Highly invasive, longer recovery, higher risks (incl. further nerve damage), scarring. | $15,000 - $50,000+ |
Children / Pediatric Considerations
While TMJ disorders are more commonly associated with adults, children and adolescents can also experience TMD and, in rare instances, nerve involvement. Pediatric considerations for tmj nerve damage symptoms are unique.
- Rarity: Severe nerve damage directly linked to TMJ dysfunction is less common in children compared to adults, primarily because their joints are still developing, and degenerative changes are rare.
- Causes:
- Trauma: Accidental falls, sports injuries, or direct blows to the jaw are significant causes of TMD in children, potentially leading to nerve irritation or damage.
- Bruxism: Habitual teeth grinding is common in children and can contribute to jaw pain and muscle tension.
- Orthodontic Treatment: While generally beneficial, complex orthodontic movements or prolonged mouth opening can sometimes exacerbate or trigger TMD symptoms.
- Developmental Anomalies: Rare congenital or developmental issues affecting the jaw or skull can sometimes predispose a child to TMD and nerve involvement.
- Symptoms: Children may not articulate their symptoms as clearly as adults. Parents should look for:
- Frequent complaints of earache or headache, especially without signs of infection.
- Difficulty chewing hard foods.
- Clicking or popping sounds from the jaw.
- Limited jaw opening.
- Unexplained facial pain, sensitivity, or numbness.
- Changes in eating habits.
- Persistent teeth grinding.
- Diagnosis: Diagnosis can be challenging and often involves a pediatric dentist, orthodontist, or oral and maxillofacial surgeon. Imaging like MRI is used cautiously to limit radiation exposure but may be necessary.
- Treatment:
- Conservative First: Treatment almost always begins with conservative, reversible therapies.
- Oral Appliances: Custom-made splints are often used to manage bruxism and reposition the jaw.
- Physical Therapy: Gentle exercises and stretches to improve jaw function.
- Soft Diet: Temporary dietary modifications.
- Medication: Pain relievers (NSAIDs) may be used, but neuropathic medications are typically reserved for severe, persistent cases under close supervision.
- Psychological Support: Counseling can help children manage stress and anxiety related to pain.
- Surgery: Invasive procedures are extremely rare and considered only as a last resort in cases of severe, debilitating structural issues unresponsive to all other treatments.
- Prognosis: Children generally have excellent healing potential. Early diagnosis and conservative management can often lead to good outcomes, preventing long-term complications.
Frequently Asked Questions
1. Can TMJ cause permanent nerve damage?
Yes, in severe or prolonged cases, particularly with persistent nerve compression, inflammation, or direct injury (e.g., during trauma or surgery), TMJ issues can lead to permanent nerve damage. This can manifest as chronic neuropathic pain, persistent numbness, or motor weakness that may not fully resolve. Early diagnosis and intervention are crucial to minimize this risk.
2. How is nerve damage from TMJ diagnosed?
Diagnosis involves a thorough clinical examination, detailed patient history, and often specialized imaging like MRI (to visualize soft tissues and disc displacement) or CBCT (for bony structures). Neurological tests such as Nerve Conduction Studies (NCS) and Electromyography (EMG) are often used to objectively confirm nerve damage, its type, and severity.
3. What are the most common tmj nerve damage symptoms?
The most common tmj nerve damage symptoms include sharp, shooting, or burning pain in the jaw, face, lips, or tongue; sensations of numbness, tingling ("pins and needles"), or prickling; and heightened sensitivity (hyperesthesia) to light touch or temperature in the affected area. Some individuals may also experience muscle weakness or facial asymmetry.
4. Is surgery always necessary for TMJ nerve damage?
No, surgery is rarely the first line of treatment and is reserved for severe cases of TMJ nerve damage where conservative and minimally invasive treatments have failed. Most patients find relief with non-surgical options like medication, physical therapy, oral splints, or targeted injections. A comprehensive evaluation will determine if surgery is appropriate.
5. How long does recovery take from TMJ nerve damage treatment?
Recovery time varies significantly depending on the severity of the nerve damage and the treatment chosen. Conservative treatments can take weeks to months for noticeable improvement. Minimally invasive procedures might involve a few weeks of initial recovery, while open-joint surgery can require several months to a year of rehabilitation.
6. Does insurance cover TMJ nerve damage treatment?
Coverage for TMJ nerve damage treatment often depends on whether your insurance company classifies it as a medical or dental issue. Typically, medical insurance covers diagnostic tests (MRI, NCS/EMG), physical therapy, medications, and surgical procedures if deemed medically necessary. Oral splints may have limited coverage or be classified under dental plans. Always verify with your specific insurance provider.
7. Can stress worsen TMJ nerve damage symptoms?
Yes, stress is a significant exacerbating factor for TMD and can worsen tmj nerve damage symptoms. Stress often leads to increased teeth clenching and grinding (bruxism) and muscle tension, which puts additional pressure on the TMJ and surrounding nerves, intensifying pain and discomfort. Stress management techniques are an integral part of treatment.
8. What is the difference between TMD and TMJ, and what does TMJ stand for?
TMJ stands for Temporomandibular Joint, the hinge connecting your jaw to your skull. TMD (Temporomandibular Disorder) refers to a range of conditions that cause pain and dysfunction in the TMJ and the muscles controlling jaw movement. So, TMJ is the joint, and TMD is the problem with the joint.
9. What specialists should I see for TMJ nerve damage?
For TMJ nerve damage, it's best to consult a multidisciplinary team. This may include an oral and maxillofacial surgeon, a neurologist, a pain management specialist, a physical therapist specializing in craniomandibular disorders, and a prosthodontist or general dentist with expertise in TMD.
10. Can TMJ nerve damage affect my vision or hearing?
While less common, severe TMJ nerve irritation or inflammation, particularly involving branches of the trigeminal nerve or referred pain pathways, can sometimes manifest as secondary symptoms affecting vision (e.g., blurred vision, eye pain) or hearing (e.g., persistent tinnitus, muffled hearing, vertigo). These are usually secondary to the primary jaw issue.
When to See a Dentist
Recognizing when to seek professional help for your jaw pain or related symptoms is crucial, especially when suspecting tmj nerve damage symptoms. Ignoring these signs can lead to chronic pain and more complex issues.
Seek Immediate Dental/Medical Attention (Emergency/Urgent Care) if you experience:
- Sudden onset of severe, excruciating facial pain: Especially if it's sharp, electric shock-like, or burning and appears without prior warning.
- New or worsening numbness or weakness in your face or jaw: This could indicate nerve compression or damage requiring prompt assessment.
- Difficulty closing your mouth completely or inability to move your jaw: If your jaw locks in an open or closed position and you cannot resolve it.
- Facial asymmetry or drooping: If one side of your face suddenly appears different or you cannot move facial muscles (e.g., smile, close an eye). This could indicate facial nerve involvement, potentially a serious condition.
- Signs of infection around your jaw: Redness, swelling, warmth, pus, accompanied by fever.
- Significant trauma to your jaw or head: If you've had a recent injury that could have damaged the TMJ or nerves.
Schedule a Prompt Appointment (Routine but Important) if you experience:
- Persistent jaw pain: Dull ache, tenderness, or stiffness that doesn't improve with self-care (soft diet, warm compresses) after a few days.
- Clicking, popping, or grinding sounds in your jaw: Especially if accompanied by pain or limited movement.
- Difficulty or pain when chewing, speaking, or yawning.
- Frequent headaches, earaches, or neck pain: Especially if they seem related to jaw movement or clenching.
- A feeling of your jaw "locking" or getting "stuck" occasionally.
- Chronic teeth grinding or clenching (bruxism): Your dentist can assess for tooth wear and recommend protective measures.
- Any concerns about tmj nerve damage symptoms such as persistent tingling, burning, or unusual sensations in your face or jaw, even if not immediately severe.
Your general dentist is often the first point of contact. They can evaluate your condition and, if necessary, refer you to a specialist such as an oral and maxillofacial surgeon, a prosthodontist, or a neurologist who specializes in TMJ disorders and facial pain. Early intervention provides the best opportunity for effective treatment and relief from tmj nerve damage symptoms.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Tmj Massage Near Me: Complete Guide
Temporomandibular joint disorder, commonly known as TMJD, affects millions of Americans, causing debilitating pain, discomfort, and significantly impacting quality of life. If you're experiencing jaw pain, clicking, or difficulty chewing, you're not alone. Up to 15% of American adults experience
February 23, 2026
Tmd Treatment: Complete Guide
Experiencing persistent jaw pain, clicking sounds when you chew, or debilitating headaches that seem to originate from your face? You're not alone. Temporomandibular joint (TMJ) disorders, often referred to collectively as TMD, affect an estimated 10 million Americans, with women disproportionat
February 23, 2026
Remi Night Guard: Complete Guide
Remi Night Guard: Complete Guide
February 23, 2026
Tmj vs Normal Jaw: Complete Comparison Guide
Experiencing persistent jaw pain, clicking sounds, or difficulty chewing can be frustrating and disruptive to daily life. While many people occasionally feel a stiff jaw, when these symptoms become chronic, they often signal an underlying issue with the temporomandibular joint (TMJ). Understanding t
February 23, 2026