Tooth Eruption Timeline: Complete Guide

Key Takeaways
- Did you know that the journey of your teeth begins long before you ever see them? Deep within your jawbones, a complex and marvelously orchestrated process unfolds, culminating in the emergence of your primary (baby) and then your permanent teeth. Understanding the tooth eruption timeline is not
Tooth Eruption Timeline: Complete Guide
Did you know that the journey of your teeth begins long before you ever see them? Deep within your jawbones, a complex and marvelously orchestrated process unfolds, culminating in the emergence of your primary (baby) and then your permanent teeth. Understanding the tooth eruption timeline is not just fascinating; it's crucial for monitoring your child's dental development, addressing potential issues early, and ensuring lifelong oral health. From the first tiny white cap peeking through your baby's gums to the wisdom teeth that often arrive in early adulthood, each stage of tooth eruption is a landmark in dental maturation.

For parents, anticipating the stages of tooth eruption in babies can bring both excitement and a desire for information on managing teething discomfort. For older children and adults, knowing the permanent tooth eruption chart helps identify when new teeth should appear and when to seek professional advice for delays or complications. This comprehensive guide from SmilePedia.net will demystify the entire process, providing you with detailed insights into what to expect at every age, how to manage common issues, and when to consult your dental professional. We'll cover everything from the earliest signs of teething to the complexities of wisdom tooth eruption, offering practical advice and medically accurate information to empower you in your oral health journey.
Key Takeaways:
- First Baby Tooth: Typically erupts between 6-10 months of age, usually a lower central incisor.
- Full Primary Dentition: All 20 baby teeth usually emerge by 2.5 to 3 years of age.
- First Permanent Molar: Often the very first permanent tooth to erupt, around 6 years old, appearing behind the last baby molar.
- Full Permanent Dentition (excluding wisdom teeth): Most permanent teeth are in place by 12-14 years of age.
- Wisdom Teeth (Third Molars): Erupt much later, typically between 17-25 years, but are often impacted and may require removal.
- Early Dental Visit: The American Dental Association (ADA) recommends a child's first dental visit by their first birthday to monitor eruption and overall oral health.
- Cost of Wisdom Tooth Extraction: Can range from $75 to $1,500+ per tooth depending on impaction and complexity, often partially covered by insurance.
What Is Tooth Eruption? An Overview
Tooth eruption is the complex biological process by which teeth emerge from their developmental position within the jawbone, penetrate the gum tissue, and become visible in the mouth. This isn't just a simple popping-through; it involves a series of coordinated cellular and molecular events that precisely guide each tooth into its functional position in the dental arch.
The process of tooth eruption is broadly divided into three phases:
- Pre-eruptive Phase: This phase occurs before the tooth begins to move towards the oral cavity. It involves the formation and growth of the tooth bud (the precursor to the tooth) and the development of the crown (the visible part of the tooth). During this phase, the tooth germ undergoes significant morphological changes and begins to form root structures.
- Eruptive Phase: This is the active phase where the tooth moves from its bony crypt within the jaw towards the oral cavity. It involves coordinated bone remodeling (resorption of bone above the tooth and deposition of bone below it), root elongation, and penetration of the overlying soft tissues (gums).
- Post-eruptive Phase: Once the tooth has reached its functional position in the mouth and comes into occlusion (contact) with the opposing teeth, the post-eruptive phase begins. During this stage, the tooth continues to undergo subtle adjustments to maintain its position as the jaw grows and other teeth erupt. Root development also typically completes during this phase.
Understanding these phases helps explain why dental X-rays can show developing teeth long before they are visible in the mouth, and why the process isn't always smooth. The force that drives eruption is still an area of active research, but it's understood to involve a combination of factors including root development, bone remodeling, and forces from the surrounding tissues.
The Journey of Primary Teeth: Stages of Tooth Eruption in Babies
The eruption of primary, or "baby," teeth is a significant milestone for infants and their parents. These 20 teeth, also known as deciduous or milk teeth, typically begin to appear around 6 months of age and are usually all in place by the age of 2.5 to 3 years. While there can be variations, the general sequence of eruption is quite predictable.
Understanding the Sequence:
- Lower Central Incisors (Front Bottom Teeth): These are usually the very first teeth to make an appearance, often between 6 and 10 months of age. You might notice a slight swelling or redness on the gum line before these tiny, sharp teeth peek through.
- Upper Central Incisors (Front Top Teeth): Following the lower centrals, the upper central incisors typically erupt between 8 and 12 months. These are also flat and shovel-shaped.
- Upper Lateral Incisors (Next to Front Top Teeth): These usually emerge on either side of the upper central incisors between 9 and 13 months.
- Lower Lateral Incisors (Next to Front Bottom Teeth): Corresponding to their upper counterparts, the lower lateral incisors appear between 10 and 16 months. At this point, your baby will have their full set of eight incisors.
- First Molars (Back Teeth): These are the first grinding teeth and are larger than incisors. The upper first molars usually erupt between 13 and 19 months, followed closely by the lower first molars between 14 and 18 months. These can sometimes cause more discomfort due to their larger size.
- Canines (Eye Teeth or Cuspids): These pointy teeth help tear food. The upper canines typically erupt between 16 and 22 months, with the lower canines appearing between 17 and 23 months. Their emergence can sometimes be associated with increased discomfort.
- Second Molars (Farthest Back Teeth): These are the final primary teeth to erupt and are the largest. The lower second molars usually emerge between 23 and 31 months, followed by the upper second molars between 25 and 33 months. Once these have erupted, your child will have their full set of 20 primary teeth.
Pro Tip: Remember that these timelines are averages. It's completely normal for a baby's first tooth to appear as early as 4 months or as late as 14 months. Genetics often play a role, so if you or your partner were late or early teethers, your child might follow a similar pattern. If there are no teeth by 18 months, it's advisable to consult with a pediatric dentist.
Understanding Permanent Tooth Eruption: The Adult Dentition Chart
The transition from primary to permanent teeth is a critical period in a child's dental development, shaping their bite and oral health for life. This process typically begins around age 6 and continues into early adulthood, often concluding with the eruption of wisdom teeth. There are 32 permanent teeth, including the third molars (wisdom teeth).
The Shedding Process (Exfoliation): Before a permanent tooth can erupt, its primary predecessor must loosen and fall out. This process, called exfoliation, is driven by the developing permanent tooth underneath. As the permanent tooth grows, it puts pressure on the roots of the baby tooth, causing them to resorb (dissolve). This gradual root resorption leads to the loosening of the primary tooth, which eventually falls out, making way for the permanent tooth.
The Permanent Tooth Eruption Chart:
- First Molars (6-Year Molars): These are often the first permanent teeth to erupt, typically between 6 and 7 years of age. Crucially, they erupt behind the last primary molar, meaning no baby tooth needs to be lost for them to appear. They are fundamental to establishing the adult bite.
- Central Incisors (Front Top & Bottom Teeth): The lower central incisors usually replace their primary counterparts between 6 and 8 years, followed by the upper central incisors between 7 and 8 years.
- Lateral Incisors (Next to Front Top & Bottom Teeth): The upper lateral incisors erupt between 8 and 9 years, with the lower lateral incisors appearing slightly later, between 7 and 8 years.
- Canines (Cuspids): These pointy teeth replace the primary canines. The lower canines typically erupt between 9 and 10 years, while the upper canines emerge later, between 10 and 12 years. The upper canines are sometimes prone to impaction if there isn't enough space.
- First Premolars (Bicuspids): These replace the first primary molars. The upper first premolars usually erupt between 10 and 11 years, and the lower first premolars between 10 and 12 years.
- Second Premolars (Bicuspids): Replacing the second primary molars, the lower second premolars erupt between 11 and 12 years, and the upper second premolars between 10 and 12 years.
- Second Molars (12-Year Molars): These erupt behind the first permanent molars, typically between 11 and 13 years. Like the first molars, they do not replace any primary teeth.
- Third Molars (Wisdom Teeth): These are the last teeth to erupt, usually between 17 and 25 years of age. However, not everyone develops wisdom teeth, and they are frequently impacted (unable to fully erupt) due to lack of space.
Table 1: Comprehensive Tooth Eruption Timeline Chart (Primary and Permanent)
| Tooth Type | Primary (Baby) Teeth Eruption Age (Average Range) | Permanent Teeth Eruption Age (Average Range) | Notes |
|---|---|---|---|
| Central Incisors | Lower: 6-10 months Upper: 8-12 months |
Lower: 6-8 years Upper: 7-8 years |
First baby teeth to appear, first permanent front teeth to replace them. |
| Lateral Incisors | Lower: 10-16 months Upper: 9-13 months |
Lower: 7-8 years Upper: 8-9 years |
Flank the central incisors. |
| Canines (Cuspids) | Upper: 16-22 months Lower: 17-23 months |
Lower: 9-10 years Upper: 10-12 years |
Pointy teeth, critical for tearing food. Upper canines prone to impaction. |
| First Premolars | (No Primary Predecessor) | Upper: 10-11 years Lower: 10-12 years |
Replace primary first molars. |
| Second Premolars | (No Primary Predecessor) | Upper: 10-12 years Lower: 11-12 years |
Replace primary second molars. |
| First Molars | Lower: 14-18 months Upper: 13-19 months |
Lower: 6-7 years Upper: 6-7 years |
First permanent teeth to erupt, erupt behind primary molars. Key for bite. |
| Second Molars | Lower: 23-31 months Upper: 25-33 months |
Lower: 11-13 years Upper: 11-13 years |
Final primary teeth to erupt. Second set of permanent molars. |
| Third Molars | (No Primary Predecessor) | Upper/Lower: 17-25 years | Wisdom teeth, often impacted or absent. |
Factors Influencing Tooth Eruption
While the tooth eruption timeline provides a general guide, several factors can influence the exact timing and sequence of eruption. Understanding these can help explain variations and alert you to potential underlying issues.
Genetics
Genetics play a significant role in determining the timing of tooth eruption. It's common for children to follow a similar eruption pattern to their parents or close relatives. If you or your partner experienced early or late teething, your child might too. This genetic predisposition can also influence tooth size, shape, and even the presence or absence of certain teeth (like wisdom teeth).
Nutrition and Overall Health
Adequate nutrition is vital for healthy tooth development and eruption. Deficiencies in key vitamins and minerals, particularly Vitamin D and calcium, can slow down the process of bone and tooth formation, potentially leading to delayed eruption.
Systemic health conditions can also impact eruption. Conditions such as:
- Hypothyroidism: An underactive thyroid can slow down metabolic processes, including tooth development and eruption.
- Hypopituitarism: This condition affects growth hormones, which can delay tooth eruption.
- Chronic Illnesses: Severe or prolonged illnesses during infancy and childhood can impact growth and development, including dentition.
- Low Birth Weight or Premature Birth: Babies born prematurely or with very low birth weights may experience slightly delayed tooth eruption compared to full-term infants.
Local Factors in the Mouth
Problems within the mouth itself can also affect eruption:
- Crowding: If there isn't enough space in the jaw, teeth may struggle to erupt properly or become impacted.
- Early Loss of Primary Teeth: If a baby tooth is lost prematurely due to decay or injury, the permanent tooth underneath might erupt earlier than expected, or adjacent teeth might shift, blocking the path of the erupting tooth.
- Retained Primary Teeth: Sometimes, a primary tooth doesn't fall out when it should, preventing the permanent tooth from erupting or causing it to erupt in an abnormal position.
- Dental Cysts or Tumors: Rarely, a cyst or tumor can obstruct the eruption path of a tooth.
- Ankylosis: This is a rare condition where the root of a tooth fuses directly to the jawbone, preventing it from erupting or continuing to erupt into proper occlusion.
Gender and Ethnicity
Studies suggest that girls tend to erupt teeth slightly earlier than boys, though this difference is usually minor. There can also be subtle variations in eruption patterns among different ethnic groups.
Pro Tip: While some variations are normal, persistent delays or unusual eruption patterns should always be discussed with your dentist. They can determine if an underlying issue requires intervention.
Signs and Symptoms of Tooth Eruption (Teething and Beyond)
The process of tooth eruption, especially for primary teeth, can be uncomfortable for babies. For older children and adults, the eruption of permanent teeth is usually less symptomatic but can still present some signs.
For Babies (Teething)
Teething symptoms are widely recognized and can begin weeks or even months before a tooth actually breaks through the gum. It's important to differentiate typical teething discomfort from signs of illness.
Common Teething Signs:
- Drooling: Excessive drooling is one of the most common signs, starting around 3-4 months. It can lead to a rash around the mouth or on the chin.
- Gum Irritation: The gums around the erupting tooth may appear red, swollen, or tender. You might even see a slight bump or, in some cases, a bluish bulge (an eruption hematoma).
- Irritability and Fussiness: Babies may become more irritable, restless, or cry more than usual due to discomfort.
- Difficulty Sleeping: Pain and discomfort can interrupt sleep patterns.
- Chewing and Biting: Babies will often try to chew on anything they can get their hands on – toys, fingers, clothing – to relieve pressure on their gums.
- Mild Temperature Rise: Some babies might experience a very slight increase in body temperature (usually below 101°F or 38.3°C). However, high fever (above 101°F / 38.3°C) is NOT a typical symptom of teething and warrants a call to the pediatrician.
- Rubbing Ears or Cheeks: This can be a referred pain from the gums.
- Reduced Appetite: Some babies may temporarily refuse solid foods due to gum soreness.
What Teething Doesn't Cause: It's a common misconception that teething causes high fevers, diarrhea, vomiting, or severe rashes. While mild symptoms are possible, these more severe issues are usually indicative of an illness and should be addressed by a healthcare provider. The ADA and American Academy of Pediatrics (AAP) both emphasize this distinction.
For Children and Adults (Permanent Teeth)
The eruption of permanent teeth is generally less disruptive than teething. However, you might still notice some signs:
- Gum Tenderness or Swelling: The gum tissue over an erupting permanent tooth might feel sore, tender, or appear slightly swollen.
- Slight Pressure or Aching: A mild sensation of pressure or a dull ache in the jaw or gum area is common as a tooth pushes through.
- Loosening of Primary Teeth: For children, the most obvious sign is the loosening of a primary tooth as its permanent successor prepares to erupt.
- Eruption Cysts/Hematomas: Occasionally, a bluish or purplish fluid-filled sac (an eruption cyst or hematoma) can form over an erupting tooth, especially molars. These are usually harmless and resolve on their own as the tooth emerges.
- Pain from Impacted Teeth: If a permanent tooth, particularly a wisdom tooth, is impacted, it can cause significant pain, swelling, jaw stiffness, and even infection if bacteria get trapped under the gum flap (pericoronitis).
Pro Tip: For children losing baby teeth, encourage them to gently wiggle the tooth to help it along. This can make the process quicker and less uncomfortable.
Common Issues and Complications During Tooth Eruption
While tooth eruption is a natural physiological process, it can sometimes be accompanied by a range of issues and complications. Early identification and management are key to preventing more serious problems.
Delayed Eruption (Primary or Permanent)
A tooth is considered to have delayed eruption if it hasn't appeared by a certain age threshold.
- For primary teeth: If no teeth have erupted by 12-14 months, or if there's a significant delay in the general sequence.
- For permanent teeth: If a tooth has not erupted within 12 months of the expected age or if the same tooth on the opposite side of the mouth has erupted, but the other hasn't.
Causes of Delayed Eruption:
- Genetic Factors: Familial history of delayed eruption.
- Systemic Conditions: Hypothyroidism, hypopituitarism, certain syndromes (e.g., Down syndrome), chronic illness, nutritional deficiencies.
- Local Factors:
- Thick Gums: Excessively fibrous gum tissue can physically block eruption.
- Obstruction: Cysts, tumors, or supernumerary (extra) teeth blocking the path.
- Ankylosis: The tooth root fuses to the bone, preventing further movement.
- Lack of Space: Insufficient jaw space, especially for permanent teeth.
- Impacted Teeth: The tooth is stuck within the bone or soft tissue.
Early Eruption (Natal and Neonatal Teeth)
While less common, some babies are born with teeth (natal teeth) or develop them within the first 30 days of life (neonatal teeth). These are usually lower central incisors.
- Concerns: Natal/neonatal teeth can be loose, posing a choking hazard, or they may irritate the baby's tongue or the mother's breast during feeding.
- Management: A dentist will assess their stability and decide if extraction is necessary.
Impacted Teeth
An impacted tooth is one that is unable to fully erupt into its correct position due to a physical obstruction (like bone, gum tissue, or another tooth) or lack of space in the jaw.
- Most Common: Wisdom teeth (third molars) are the most frequently impacted teeth.
- Others: Upper canines are also commonly impacted.
- Symptoms: Pain, swelling, redness in the gum, difficulty opening the mouth, bad breath, chronic infection (pericoronitis).
- Risks: Can damage adjacent teeth, cause cysts or tumors, lead to infection, or contribute to crowding.
Ectopic Eruption
This occurs when a tooth erupts in an abnormal position, often due to inadequate space or an improper eruption path.
- Most Common: Maxillary first permanent molars (erupting into the side of the primary second molar), permanent canines.
- Consequences: Can lead to premature loss of primary teeth, damage to adjacent permanent teeth, or significant malocclusion.
Crowding and Malocclusion
Insufficient space in the jaw for the full complement of permanent teeth can lead to crowding, where teeth overlap or erupt out of alignment. This can also contribute to malocclusion (improper bite).
Eruption Cysts and Hematomas
Sometimes, a soft, fluid-filled swelling develops over an erupting tooth. If it contains blood, it's called an eruption hematoma and appears bluish or purplish.
- Nature: These are generally benign and typically rupture on their own as the tooth emerges.
- Intervention: Rarely, a minor incision might be needed if they are very large or painful.
Pericoronitis
This is an inflammation of the gum tissue (operculum) surrounding a partially erupted tooth, most commonly seen with wisdom teeth.
- Cause: Food particles and bacteria get trapped under the gum flap, leading to infection.
- Symptoms: Severe pain, swelling, pus discharge, bad taste, difficulty biting down, fever.
- Treatment: Antibiotics, irrigation, removal of the operculum, or extraction of the tooth.
Pro Tip: Regular dental check-ups, especially for children, are crucial for identifying these issues early. Your dentist can use X-rays to monitor tooth development and eruption patterns.
Managing Tooth Eruption Related Problems
Addressing issues related to tooth eruption depends heavily on the specific problem and the age of the individual. Management ranges from simple home remedies for teething to complex surgical procedures for impacted teeth.
For Teething Pain (Babies)
While teeth must erupt, the discomfort doesn't have to be overwhelming.
- Home Remedies:
- Gum Massage: Gently rub your baby's gums with a clean finger.
- Chilled Teething Toys/Rings: Provide a firm, chilled (not frozen) teething toy or a clean, cold washcloth for your baby to chew on.
- Cold Foods: For babies on solids, offer chilled purees or soft fruits.
- Over-the-Counter (OTC) Pain Relief:
- Acetaminophen (Tylenol): Follow age and weight-appropriate dosing instructions.
- Ibuprofen (Advil, Motrin): Can be used for babies 6 months and older. Follow dosing instructions.
- What to AVOID:
- Topical Anesthetics with Benzocaine: The FDA warns against using products containing benzocaine (like Orajel) for children under 2 years old due to the risk of methemoglobinemia, a serious blood disorder.
- Homeopathic Teething Tablets: The FDA has issued warnings about inconsistencies in ingredients and potential health risks.
- Teething Necklaces/Bracelets: These pose choking and strangulation hazards.
For Delayed Eruption
- Monitoring and X-rays: Your dentist will closely monitor the situation. X-rays can reveal if the tooth is present, its position, and if any obstruction exists.
- Extraction of Retained Primary Teeth: If a baby tooth is preventing a permanent tooth from erupting, its extraction may be necessary. This allows the permanent tooth to move into its proper place.
- Surgical Exposure: For an otherwise healthy permanent tooth that is impacted by gum tissue or a thin layer of bone, a minor surgical procedure can expose the crown, sometimes followed by orthodontic brackets to guide it into position.
For Impacted Teeth
Management depends on the tooth type, degree of impaction, and symptoms.
- Monitoring: Asymptomatic wisdom teeth that are not causing problems may be monitored with regular X-rays.
- Surgical Extraction: This is the most common "treatment" for impacted wisdom teeth, especially if they are causing pain, infection, or damage to adjacent teeth. This procedure can range from a simple extraction (if partially visible) to a more complex surgical removal involving bone and tissue.
- Orthodontic Intervention: For impacted canines, surgical exposure combined with orthodontics (braces) can often guide the tooth into its correct position.
For Ectopic Eruption or Crowding
- Orthodontic Treatment: Braces or clear aligners are often used to create space, move teeth into their correct positions, and correct malocclusion.
- Space Maintainers/Expanders: For children, appliances can be used to hold space for permanent teeth or widen the dental arch.
- Serial Extractions: In severe cases of crowding, the planned extraction of certain primary teeth (and sometimes permanent premolars) might be done in a specific sequence to facilitate the proper eruption of other permanent teeth and reduce the need for more extensive orthodontic work later.
For Eruption Cysts/Hematomas
These typically resolve on their own as the tooth breaks through. If they are large, painful, or interfere with eating, a dentist might perform a small incision to drain the fluid, which is usually a quick and simple procedure.
For Pericoronitis
- Initial Management: Thorough cleaning and irrigation of the area to remove trapped food and bacteria.
- Antibiotics: Prescribed if there's significant infection and swelling.
- Removal of Operculum: A minor surgical procedure to remove the gum flap.
- Extraction: Often, the impacted wisdom tooth causing recurrent pericoronitis will need to be extracted.
Pro Tip: Never ignore persistent pain or swelling during any stage of tooth eruption. Early dental intervention can prevent minor issues from becoming major problems.
The Step-by-Step Physiological Process of Tooth Eruption
While the timelines give us the "when," understanding the "how" of tooth eruption reveals the remarkable precision of the human body. This intricate process involves a symphony of cellular activities and tissue changes.
-
Crown Formation (Pre-eruptive Phase):
- The tooth development begins deep within the jawbone, with the formation of the tooth germ.
- The enamel and dentin (the hard tissues of the crown) are laid down by specialized cells, forming the visible part of the tooth.
- At this stage, the tooth is encased in a protective sac called the dental follicle.
-
Root Development Begins (Eruptive Phase Initiation):
- Once the crown is largely formed, the root begins to develop from the base of the crown.
- This root elongation is crucial; it pushes the tooth towards the surface. As the root grows longer, it creates a force.
-
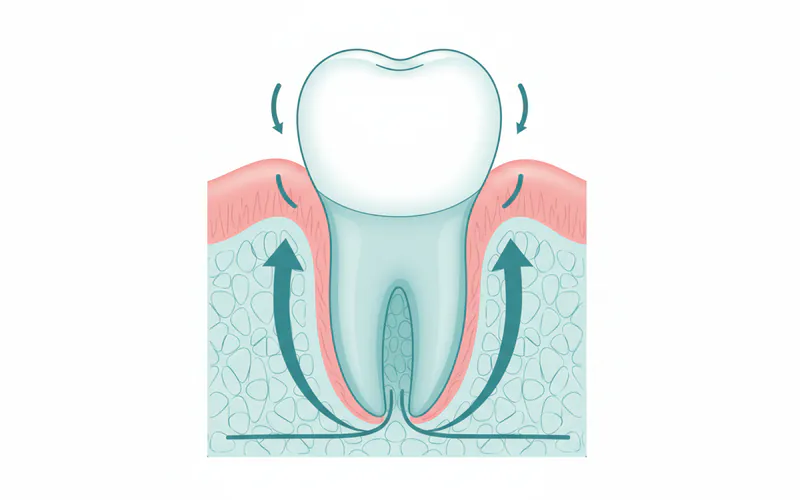
Bone Resorption and Deposition:
- Simultaneously, the body orchestrates precise bone remodeling.
- Osteoclasts (bone-resorbing cells) break down the bone directly above the developing tooth, creating a pathway.
- Below the tooth, osteoblasts (bone-forming cells) deposit new bone, effectively pushing the tooth upwards.
- The dental follicle plays a key role in signaling these bone remodeling events.
-
Movement Through Bone and Soft Tissue:
- The tooth steadily migrates through the created bony tunnel.
- As it approaches the surface, the overlying connective tissue and gum layers become compressed and eventually break down.
-
Penetration of Oral Mucosa:
- The cusp (point) or incisal edge (cutting edge) of the tooth finally pierces the gum tissue, becoming visible in the mouth. This is the moment a tooth is "erupted."
- The surrounding gum tissue then attaches to the neck of the tooth, forming a protective seal (the gingival attachment).
-
Root Completion and Positional Adjustments (Post-eruptive Phase):
- Even after the tooth has emerged and reached its opposing tooth, its root continues to develop, often taking several more months or even years to fully form and close at the apex.
- Throughout life, teeth make minor positional adjustments to maintain proper occlusion as the jaw grows and other teeth wear down.
This remarkable biological ballet ensures that teeth not only arrive at the right time but also in the correct orientation and position to perform their vital functions of chewing, speaking, and contributing to facial aesthetics. Any disruption to this delicate process can lead to the eruption complications discussed earlier.
Cost of Managing Eruption-Related Issues
The cost of managing tooth eruption-related issues can vary significantly based on the complexity of the problem, the type of intervention needed, the dental professional's fees, and your geographic location within the US. Insurance coverage also plays a crucial role.
Average US Costs (Out-of-Pocket, Without Insurance)
-
Routine Pediatric Dental Check-up (including X-rays for eruption monitoring):
- Low: $100 - $150
- Mid: $200 - $300
- High: $350+ (Includes exam, cleaning, fluoride, and potentially bite-wing X-rays to monitor developing teeth.)
-
Extraction of a Retained Primary Tooth:
- Simple (local anesthetic): $75 - $250 per tooth
- Complex (surgical, e.g., removal of bone): $200 - $400 per tooth
-
Surgical Exposure of an Impacted Tooth (e.g., canine):
- Average: $300 - $800 per tooth (Often followed by orthodontic bonding, which is an additional cost.)
-
Wisdom Tooth Extraction: This is one of the most common eruption-related procedures.
- Simple Eruption (fully erupted, non-surgical): $75 - $250 per tooth
- Soft Tissue Impaction (covered by gum): $250 - $450 per tooth
- Bony Impaction (partially or fully covered by bone): $350 - $750 per tooth
- Complex/Deeply Bony Impaction: $600 - $1,500+ per tooth (Sedation/anesthesia costs are additional, ranging from $200 - $800+ for IV sedation, or $50 - $150 for nitrous oxide.)
-
Orthodontic Treatment (for crowding, ectopic eruption, guiding impacted teeth):
- Phase 1 (early intervention for children): $2,000 - $5,000
- Comprehensive (full braces/aligners): $3,000 - $8,000 (traditional braces); $4,000 - $9,000+ (clear aligners like Invisalign).
Insurance Coverage Details
-
Dental Insurance: Most standard dental insurance plans will cover a percentage of routine check-ups, X-rays, and basic extractions (like retained primary teeth) after a deductible is met.
- Diagnostic/Preventive (Exams, X-rays, cleanings): Often covered at 80-100%.
- Basic Procedures (Simple Extractions): Typically covered at 50-80%.
- Major Procedures (Surgical extractions, surgical exposure): Often covered at 30-50%, subject to annual maximums (which can range from $1,000 - $2,000 per year).
- Orthodontics: Many plans have separate orthodontic coverage with a lifetime maximum (e.g., $1,000 - $3,000), or they may not cover it at all.
-
Medical Insurance: In some cases, if wisdom tooth extraction is particularly complex and requires hospital-level anesthesia or oral surgery, your medical insurance might cover a portion of the surgical facility fees or the anesthesiologist's fees, even if the dental surgeon's fee falls under dental insurance. Always check with both your dental and medical insurance providers.
Payment Plans and Financing Options
- In-Office Payment Plans: Many dental offices offer interest-free payment plans for larger procedures, allowing you to pay in installments over several months.
- Third-Party Financing: Services like CareCredit are widely used. They offer deferred interest or low-interest financing options for healthcare expenses, allowing you to pay over a longer period.
- Dental Schools/Community Clinics: These can often provide services at a significantly reduced cost, as procedures are performed by students under the supervision of experienced faculty. Quality of care is typically high, but appointment availability and treatment duration may be longer.
Table 2: Comparative Costs of Common Eruption-Related Interventions (US Average, without insurance)
| Procedure | Average Cost Range (USD) | Common Insurance Coverage | Notes |
|---|---|---|---|
| Pediatric Dental Check-up | $100 - $350 | 80-100% | Includes exam, cleaning, X-rays. Essential for monitoring eruption. |
| Simple Primary Tooth Extraction | $75 - $250 | 50-80% | Removal of a loose baby tooth blocking a permanent one. |
| Surgical Exposure (Impacted) | $300 - $800 | 30-50% (Major) | Exposing a tooth to allow eruption or orthodontically guide it. |
| Wisdom Tooth Extraction (Simple) | $75 - $250 per tooth | 50-80% (Basic) | For fully erupted, easily removable wisdom teeth. |
| Wisdom Tooth Extraction (Bony) | $350 - $750 per tooth | 30-50% (Major) | For impacted wisdom teeth requiring surgical removal of bone. |
| IV Sedation (Oral Surgery) | $200 - $800+ | Often separate or limited | Additional cost for comfort during surgical extractions. |
| Comprehensive Orthodontics | $3,000 - $8,000+ | Separate lifetime max | For correcting crowding, malocclusion, or guiding impacted teeth. |
Recovery and Aftercare for Eruption-Related Procedures
Proper recovery and aftercare are essential after any dental intervention related to tooth eruption to ensure optimal healing and prevent complications.
For Teething Discomfort (No Procedure)
- Continue with home remedies (chilled toys, gum massage).
- Administer age-appropriate OTC pain relievers if needed.
- Keep the area around the mouth dry to prevent drool rash.
- Maintain gentle oral hygiene, even with erupting teeth. Use a soft cloth or baby toothbrush.
Post-Extraction (e.g., Retained Primary Tooth, Wisdom Tooth)
Whether it's a simple removal of a baby tooth or a complex wisdom tooth extraction, specific aftercare instructions are critical.
- Bleeding Control: Bite firmly on the gauze pad provided for 30-60 minutes to promote clot formation. Change gauze as needed.
- Pain Management: Take prescribed pain medication or OTC pain relievers (ibuprofen, acetaminophen) as directed before the anesthetic wears off.
- Swelling Reduction: Apply an ice pack to the outside of your face for 15-20 minutes at a time, every hour for the first 24-48 hours.
- Diet: Stick to soft foods and liquids for the first few days (e.g., yogurt, mashed potatoes, soup). Avoid hot, spicy, crunchy, or chewy foods.
- Oral Hygiene:
- First 24 Hours: Avoid rinsing, spitting, or using a straw, as these actions can dislodge the blood clot and lead to a painful "dry socket."
- After 24 Hours: Gently rinse with warm salt water (1/2 teaspoon salt in 8 ounces of warm water) several times a day, especially after meals. Brush other teeth carefully, avoiding the extraction site.
- Activity: Rest and avoid strenuous activity for at least 24-48 hours to prevent increased bleeding and swelling.
- Smoking/Alcohol: Absolutely avoid smoking and alcohol for at least 72 hours, as they significantly impair healing and increase the risk of complications.
- Follow-up: Attend any scheduled follow-up appointments to ensure proper healing.
Post-Orthodontic Procedures (e.g., After Surgical Exposure and Bonding)
- Oral Hygiene: Meticulous brushing and flossing are crucial with orthodontic appliances. Your orthodontist will provide specific tools and techniques.
- Dietary Restrictions: Avoid sticky, hard, or chewy foods that can damage braces or wires.
- Pain/Discomfort: Expect some initial soreness. OTC pain relievers can help. Orthodontic wax can cover any irritating brackets or wires.
- Regular Adjustments: Keep all scheduled orthodontic appointments for adjustments and monitoring.
General Aftercare Tips
- Hydration: Drink plenty of fluids to stay hydrated.
- Monitor for Complications: Watch for signs of infection (fever, excessive swelling, pus), persistent severe pain not relieved by medication, or excessive bleeding.
- Follow Dentist's Instructions: Always adhere strictly to the specific post-operative instructions provided by your dental professional.
Prevention of Eruption Complications
While tooth eruption is a natural process, there are several steps you can take to prevent or minimize potential complications, particularly for children.
- Early and Regular Dental Check-ups: The American Dental Association (ADA) recommends a child's first dental visit by their first birthday or within six months of the first tooth erupting. Regular check-ups thereafter (every six months) allow the dentist to monitor the eruption timeline, assess jaw development, and identify potential issues like crowding or impaction early on.
- Pro Tip: Early visits also help children become comfortable with the dental environment, promoting a lifetime of good oral health habits.
- Good Oral Hygiene from Infancy: Even before teeth erupt, gently wipe your baby's gums with a clean, damp cloth after feedings. Once the first tooth appears, brush twice daily with a soft-bristled, age-appropriate toothbrush and a tiny smear of fluoride toothpaste (rice-grain size for under 3, pea-size for 3-6 years). This prevents early childhood caries (cavities), which can lead to premature loss of primary teeth and subsequent eruption problems for permanent teeth.
- Proper Nutrition: A balanced diet rich in calcium, phosphorus, and Vitamin D supports healthy bone and tooth development. Limit sugary drinks and snacks, which contribute to tooth decay.
- Avoid Premature Loss of Primary Teeth: Primary teeth act as natural space maintainers for permanent teeth. Losing them too early due to decay or injury can cause adjacent teeth to drift into the empty space, blocking the eruption path of the underlying permanent tooth.
- If a baby tooth is lost prematurely, your dentist may recommend a space maintainer to hold the space until the permanent tooth is ready to erupt.
- Monitor for Signs of Trouble: Be observant of your child's dental development. If you notice persistent pain, significant delays in eruption (e.g., no teeth by 14-18 months, or a permanent tooth not erupting a year after its counterpart on the other side), unusual swelling, or teeth coming in at odd angles, contact your dentist.
- Early Orthodontic Consultation: For children with signs of crowding or malocclusion, an orthodontic evaluation around age 7-8 can help determine if early intervention (Phase I orthodontics) might prevent more complex issues later, such as impacted teeth or severe crowding.
- Protective Measures for Trauma: Protect your child's teeth from injury during sports by using a properly fitted mouthguard, as trauma can affect developing teeth.
By proactively managing oral health and staying informed about the tooth eruption timeline, you can significantly contribute to a smoother process and a healthier smile for yourself and your family.
Children / Pediatric Considerations
The eruption of teeth is a cornerstone of pediatric dental health. For parents, understanding the nuances of tooth eruption in children is vital for their child's overall well-being.
First Dental Visit: By Age One!
The American Academy of Pediatric Dentistry (AAPD) and the ADA strongly recommend that a child's first dental visit occur no later than their first birthday or within six months of the first tooth erupting. This initial visit is not just about checking for teeth; it's about:
- Establishing a "Dental Home": A continuous relationship between the patient and the dental professional.
- Parental Education: Providing guidance on proper oral hygiene, diet, fluoride use, and what to expect with tooth eruption.
- Risk Assessment: Identifying any early signs of decay or developmental issues.
- Monitoring Eruption: The dentist can assess the sequence and timing of erupting teeth and identify any potential delays or abnormalities.
Importance of Primary Teeth
Primary teeth are far more than just "placeholders." They are crucial for:
- Eating and Nutrition: Proper chewing of food for digestion.
- Speech Development: Helping form sounds and words correctly.
- Space Maintenance: Holding the necessary space for the permanent teeth to erupt into their correct positions. Premature loss of a primary tooth can lead to crowding and orthodontic problems.
- Jaw Development: Stimulating proper growth of the jawbones.
- Self-Esteem: Contributing to a child's smile and confidence.
Managing Teething Comfort
As discussed, teething is a normal part of tooth eruption for babies. Parents should focus on comfort measures:
- Gentle Gum Massage: Use a clean finger.
- Chilled Teething Rings: Ensure they are not frozen solid, which can hurt gums.
- Age-Appropriate Pain Relievers: Acetaminophen or ibuprofen, if necessary, strictly following dosage instructions.
- Avoid Harmful Products: Steer clear of benzocaine products and homeopathic teething remedies due to safety concerns.
"Lift the Lip" Check
Pediatric dentists often teach parents the "Lift the Lip" technique. By gently lifting your child's upper lip, you can regularly inspect their gums and the surfaces of their teeth. This helps detect early signs of decay, gum inflammation, or eruption cysts that might otherwise go unnoticed.
Fluoride and Erupting Teeth
Fluoride is essential for strengthening tooth enamel and preventing decay, especially for newly erupted teeth that are more susceptible to cavities.
- Fluoride Toothpaste: A rice-grain smear for children under 3, a pea-size amount for ages 3-6.
- Fluoridated Water: If your community water is fluoridated, ensure your child drinks it.
- Topical Fluoride: Your dentist may recommend professional fluoride applications during check-ups.
Addressing Parental Concerns
It's natural for parents to have questions or concerns about their child's tooth eruption. Common questions include:
- "My baby's teeth are coming in late/early, is that normal?"
- "Why is this tooth coming in crooked?"
- "What do I do about the fever during teething?"
- "My child lost a tooth too early, what now?"
These are all valid concerns that your pediatric dentist is best equipped to answer with accurate, individualized advice based on your child's specific development. Early intervention can often prevent more significant problems down the line.
Cost Breakdown for Eruption-Related Interventions
Beyond the specific procedure costs, it's helpful to understand the overall financial landscape of managing eruption issues, including how to plan and potentially save money.
Average US Costs (Low, Mid, High)
To reiterate and expand on the previous cost section:
- Initial Consultations/Exams:
- Pediatric Dental Exam (infant/child): $100 - $350. This is the starting point for monitoring eruption.
- Orthodontic Consultation: $50 - $250 (many orthodontists offer free initial consultations).
- Diagnostic Imaging:
- Bitewing X-rays: $25 - $75 (typically taken annually for children).
- Panoramic X-ray: $100 - $200 (a full-mouth X-ray, often taken around age 6-8 and again in the teens to assess permanent tooth development, impaction, and wisdom teeth).
- 3D Cone Beam CT (CBCT): $300 - $600+ (for complex impactions or detailed orthodontic planning).
- Basic Extractions (Primary Teeth):
- Non-surgical: $75 - $250 per tooth.
- Surgical Extractions (Permanent Teeth, e.g., wisdom teeth):
- Simple (fully erupted): $75 - $250 per tooth.
- Impacted (soft tissue): $250 - $450 per tooth.
- Impacted (bony): $350 - $750 per tooth.
- Complex (deep bony, nerve proximity): $600 - $1,500+ per tooth.
- Anesthesia/Sedation:
- Nitrous Oxide (laughing gas): $50 - $150 per visit.
- Oral Sedation (pills): $100 - $300 per visit.
- IV Sedation: $200 - $800+ per hour.
- General Anesthesia (hospital setting): $1,000 - $3,000+ (hospital fees are significant).
- Adjunctive Procedures:
- Space Maintainer (for premature primary tooth loss): $200 - $500.
- Orthodontic Appliances (braces, aligners): $3,000 - $9,000+.
With vs. Without Insurance
The presence of dental insurance can significantly reduce your out-of-pocket costs, but it's vital to understand your plan's specifics.
- Preventive Care: Most plans cover 80-100% of exams, cleanings, and routine X-rays. This means early detection of eruption issues is often low-cost.
- Basic Procedures: Fillings, simple extractions, etc., typically covered at 50-80%.
- Major Procedures: Surgical extractions, crowns, bridges, surgical exposure, typically covered at 30-50%. These are often subject to a deductible (e.g., $50-$100 per year) and an annual maximum (e.g., $1,000-$2,000). Once you hit the maximum, you pay 100%.
- Orthodontics: Often has a separate lifetime maximum (e.g., $1,000-$3,000) or is not covered at all. Some plans only cover orthodontics for children under 18.
- Medical Insurance Crossover: For complex oral surgeries, especially those performed by an oral surgeon in a hospital or surgical center, your medical insurance might cover the facility and anesthesia fees, even if the dentist's professional fee falls under dental. This can save thousands.
Payment Plans and Financing Options
- In-Office Plans: Many dental practices offer flexible payment plans, often interest-free for shorter terms, to help spread the cost of treatment.
- Third-Party Medical Financing: Companies like CareCredit and Alphaeon Credit offer specialized credit lines for healthcare expenses. They often have promotional periods with deferred interest if the balance is paid within a certain timeframe (e.g., 6, 12, 18, 24 months). Be mindful of interest rates if the balance isn't paid off.
- Health Savings Accounts (HSAs) and Flexible Spending Accounts (FSAs): If you have access to these employer-sponsored accounts, they allow you to use pre-tax dollars for qualified medical and dental expenses, effectively saving you money.
Cost-Saving Tips
- Preventive Care is Key: Regular check-ups and good oral hygiene prevent costly problems. It's much cheaper to monitor eruption than to treat an impacted tooth that has caused complications.
- Shop Around: For major procedures like wisdom tooth extraction or orthodontics, get multiple quotes from different providers.
- Dental Schools: Consider major university dental schools for significant savings on a wide range of procedures. Treatment is supervised by experienced faculty.
- Community Dental Clinics: Many communities have non-profit clinics that offer reduced-cost dental care based on income.
- Negotiate: Don't be afraid to ask your dentist about cash discounts for upfront payment, especially if you don't have insurance.
Frequently Asked Questions
Q1: Is it normal for my baby to have a fever during teething?
A: While a very mild elevation in temperature (below 100.4°F or 38°C) can sometimes accompany teething due to gum inflammation, a true fever (above 101°F or 38.3°C) is generally not a normal symptom of teething. If your baby has a high fever, diarrhea, vomiting, or a severe rash, it's more likely a sign of an illness, and you should contact your pediatrician.
Q2: What is the typical age for the first baby tooth to erupt?
A: The first baby tooth, usually a lower central incisor, typically erupts between 6 and 10 months of age. However, there's a wide normal range, with some babies getting their first tooth as early as 4 months and others not until 12-14 months.
Q3: My child lost a baby tooth early due to an injury. Is that a problem?
A: Yes, losing a baby tooth prematurely can be a problem. Primary teeth act as "space maintainers" for the permanent teeth underneath. If a baby tooth is lost too early, adjacent teeth can drift into the empty space, potentially blocking the permanent tooth from erupting or causing it to come in crooked. Your dentist may recommend a space maintainer.
Q4: When do wisdom teeth usually come in?
A: Wisdom teeth (third molars) are the last teeth to erupt, typically between the ages of 17 and 25 years. However, their eruption can be highly variable, and many people never have them erupt fully due to lack of space, leading to impaction.
Q5: Is delayed eruption a sign of a serious problem?
A: Delayed eruption can sometimes be an isolated, benign genetic trait. However, it can also be a symptom of underlying systemic conditions (like hypothyroidism) or local issues (like impaction, thick gums, or extra teeth blocking the path). If your child has no teeth by 14-18 months, or if a permanent tooth hasn't erupted a year after its counterpart on the opposite side, consult your dentist for evaluation and potentially X-rays.
Q6: How can I tell if a tooth, particularly a wisdom tooth, is impacted?
A: An impacted tooth is one that can't fully erupt. Symptoms of an impacted wisdom tooth can include persistent pain at the back of the jaw, swelling or tenderness in the gum, difficulty opening your mouth, an unpleasant taste, or signs of infection (pericoronitis). Often, an impacted tooth causes no symptoms initially and is only detected through dental X-rays during a routine check-up.
Q7: Are there any home remedies for teething pain I should avoid?
A: Yes, it's important to avoid certain products. The FDA advises against using topical anesthetics containing benzocaine (like Orajel) for children under 2 years old due to the risk of a serious blood disorder. Also, avoid homeopathic teething tablets, as they can have inconsistent ingredients, and teething necklaces/bracelets, which pose choking and strangulation hazards. Stick to chilled teething toys and gentle gum massage.
Q8: What is the average cost of wisdom tooth removal?
A: The cost of wisdom tooth removal varies significantly based on the complexity of the impaction and whether it requires general anesthesia. A simple, fully erupted wisdom tooth removal can cost $75-$250 per tooth, while a deeply bony impacted wisdom tooth might cost $350-$750 or more per tooth. Sedation adds to the cost. With insurance, your out-of-pocket expense will be lower, but coverage varies.
Q9: How long does the tooth eruption process take for one tooth?
A: The actual movement of a tooth from its bony crypt through the gum can take several weeks or even months once it begins. The entire developmental process, from the initial tooth bud to full root completion after eruption, takes several years for each tooth. For example, a baby tooth starts forming around 6 weeks in utero but doesn't fully erupt until 6-10 months after birth.
Q10: Can adult teeth erupt before all baby teeth are lost?
A: Yes, this is quite common, especially with the eruption of the first permanent molars around age 6. These molars erupt behind the last baby teeth, so no primary tooth needs to be lost for them to appear. Sometimes, permanent incisors can also start to erupt behind the primary incisors before the baby teeth have fully fallen out, creating a "shark teeth" appearance, which often self-corrects.
When to See a Dentist
Knowing when to seek professional dental advice regarding tooth eruption is crucial for preventing minor issues from escalating. Here are clear warning signs and guidelines:
Red Flags That Need Immediate Attention:
- No Teeth by 14-18 Months: While there's a wide range for first tooth eruption, if your baby has no teeth by 14-18 months, it's advisable to have them evaluated by a pediatric dentist to rule out underlying causes like delayed development or absence of tooth buds.
- Significant Pain or Swelling: If your child or you experience severe, persistent pain, significant facial swelling, or tenderness around an erupting tooth, especially if accompanied by a high fever (above 101°F / 38.3°C), it could indicate an infection or a more serious problem than typical eruption discomfort. This warrants an emergency dental appointment.
- Pus or Discharge: Any sign of pus or foul-smelling discharge around an erupting tooth (often seen with partially erupted wisdom teeth) is a clear indication of infection (like pericoronitis) and requires immediate dental intervention.
- Difficulty Opening Mouth or Swallowing: These symptoms, especially when associated with an erupting wisdom tooth, suggest a severe infection or swelling that needs urgent medical attention.
- Early Loss of a Primary Tooth Due to Trauma or Decay: If your child loses a baby tooth significantly earlier than expected due to an accident or severe decay, see a dentist. They can assess the space and determine if a space maintainer is needed to prevent future crowding.
- Unusual Lumps or Discoloration on Gums: While an eruption hematoma (bluish bulge) is usually benign, any firm, persistent, or rapidly growing lump or unusual discoloration on the gums should be evaluated by a dentist to rule out other conditions.
Routine Care vs. Emergency Guidance:
- Routine Care:
- First Dental Visit: Schedule your baby's first dental visit by their first birthday to establish a dental home and monitor eruption.
- Regular Check-ups: Maintain biannual dental check-ups for children and adults to monitor tooth development, identify potential eruption issues early, and ensure overall oral health.
- Mild Teething Symptoms: Manage with home remedies and age-appropriate OTC pain relievers as described in the "Managing Tooth Eruption Related Problems" section.
- Scheduled Appointment for Concerns (Non-Emergency):
- Significant Delay in Permanent Tooth Eruption: If a permanent tooth has not erupted within 6-12 months after its counterpart on the opposite side of the mouth, or well beyond its expected eruption age.
- Crowding or Misalignment: If you notice teeth coming in severely crooked, overlapping, or if there's significant crowding, an orthodontic consultation is advisable, often around age 7-8 for children.
- Persistent Irritation: If a partially erupted wisdom tooth repeatedly causes mild discomfort or irritation but without severe infection symptoms.
- Retained Primary Teeth: If a baby tooth is still present when its permanent successor is clearly visible or overdue.
Always err on the side of caution. If you are ever unsure whether a symptom is normal or requires attention, contact your dentist. They are your best resource for guiding you through every stage of the tooth eruption timeline.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Tooth Eruption Order: Complete Guide
The journey of human teeth, from their initial emergence in infancy to the arrival of wisdom teeth in young adulthood, is a fascinating and crucial aspect of our overall health. Understanding the tooth eruption order is not just a matter of curiosity; it's a vital piece of knowledge that empower
February 23, 2026

Primary Tooth Eruption Sequence: Complete Guide
Did you know that by their third birthday, most children will have a full set of 20 primary teeth? The journey of these first teeth, from their initial appearance to their eventual replacement by permanent teeth, is a remarkable and often challenging milestone for both infants and parents. Understan
February 23, 2026
Canine Tooth Eruption: Complete Guide
Have you ever wondered about the complex process that brings your teeth into alignment, especially the prominent, pointed teeth known as canines? While often overshadowed by discussions of wisdom teeth or incisors, the canine tooth eruption process is a critical stage in your oral development, d
February 23, 2026

Permanent Tooth Eruption Sequence: Complete Guide
Welcome to SmilePedia.net, your trusted resource for comprehensive dental health information. The journey of your permanent teeth emerging into your mouth, known as the permanent tooth eruption sequence, is a fundamental aspect of oral development. Did you know that while primary (baby) teeth ty
February 23, 2026