Canine Tooth Eruption: Complete Guide
Key Takeaways
- Have you ever wondered about the complex process that brings your teeth into alignment, especially the prominent, pointed teeth known as canines? While often overshadowed by discussions of wisdom teeth or incisors, the canine tooth eruption process is a critical stage in your oral development, d
Canine Tooth Eruption: Complete Guide
Have you ever wondered about the complex process that brings your teeth into alignment, especially the prominent, pointed teeth known as canines? While often overshadowed by discussions of wisdom teeth or incisors, the canine tooth eruption process is a critical stage in your oral development, dictating not only your smile's appearance but also the health and functionality of your entire bite. A smooth eruption ensures proper chewing, clear speech, and a symmetrical facial structure. However, when issues arise, they can lead to significant dental problems, from crowding and misalignment to impaction and damage to adjacent teeth. Understanding this intricate journey, from the initial signs to potential complications and treatment options, is vital for maintaining optimal dental health for you and your family. This comprehensive guide will walk you through everything you need to know about canine tooth eruption, covering what to expect, common challenges, available solutions, and essential preventive care to ensure a healthy, beautiful smile.

Key Takeaways:
- Canine teeth, also known as cuspids, are crucial for biting, tearing food, and supporting facial structure.
- Baby (deciduous) canines typically erupt between 16-22 months for upper canines and 17-23 months for lower canines.
- Permanent canines usually erupt between 9-12 years for lower canines and 11-12 years for upper canines, making them the second-to-last teeth to emerge.
- Impaction, where a canine fails to erupt into its proper position, affects 1-3% of the population, with maxillary (upper) canines being most commonly affected.
- Treatment for impacted canines can range from orthodontic exposure and bonding (costs typically $1,500-$4,000, in addition to comprehensive orthodontic treatment) to extraction (costs $150-$600 per tooth) if repositioning is not feasible.
- Early orthodontic evaluation, often around age 7-8, is crucial for identifying potential eruption problems and planning timely intervention.
- Insurance coverage for orthodontic treatment and surgical interventions varies widely, with many plans covering 50% or more of costs after deductibles.

What It Is / Overview
Canine teeth, often called cuspids or eye teeth, are the pointy, robust teeth located at the corners of your mouth, between the incisors (front teeth) and premolars (back grinding teeth). You have four canine teeth in total: two in the upper jaw (maxillary canines) and two in the lower jaw (mandibular canines). They are considered cornerstones of the dental arch due to their critical role in the bite.
The eruption of a tooth refers to its emergence through the gums into the mouth. Canine tooth eruption is a two-stage process throughout a person's life:
- Primary (Deciduous) Canine Eruption: These are the "baby" canines. They are part of the primary dentition that begins to erupt in infancy.
- Permanent Canine Eruption: These are the "adult" canines. They replace the primary canines as a child grows, becoming a permanent fixture in the adult dentition.
Canine teeth are incredibly important for several reasons:
- Tearing Food: Their pointed shape is ideal for tearing tough foods.
- Guiding the Bite: They play a crucial role in guiding the jaw into a stable, healthy biting position, protecting the other teeth from excessive forces during chewing.
- Facial Support: They help support the lips and facial muscles, contributing to a balanced facial aesthetic.
- Dental Arch Stability: Canines are the longest teeth in terms of root length, providing strong anchorage and stability for the entire dental arch.
Understanding the typical timeline and process for both primary and permanent canine eruption is essential for parents and individuals to identify potential issues early on. The proper eruption of these teeth is a strong indicator of overall oral health and development.
Types / Variations in Canine Eruption
While the ideal eruption path is straightforward, several variations and potential problems can occur during canine tooth eruption, primarily impacting the permanent canines. These variations often lead to what is known as impaction. An impacted tooth is one that is unable to erupt into its normal functional position within the dental arch, either because it's blocked by another tooth, dense bone, or soft tissue, or because it's simply developing in the wrong position.
There are primarily two types of impacted permanent canines:
Buccal Impaction
This occurs when the impacted canine is positioned towards the cheek (buccal side) of the dental arch. It might be felt as a bulge on the outside of the gum tissue. Buccal impactions are generally less complex to treat than palatal impactions because they are more accessible for orthodontic intervention.
Palatal Impaction
This is more common and occurs when the impacted canine is positioned towards the roof of the mouth (palatal side). It can be harder to detect without dental imaging (X-rays) and may not show any external signs. Palatal impactions often require more involved surgical and orthodontic procedures due to their location and potential proximity to other vital structures.
Beyond impaction, other variations can include:
- Ectopic Eruption: The tooth begins to erupt in an abnormal position, often too far forward or backward.
- Transposition: A canine tooth erupts in the position typically occupied by another tooth, such as a premolar, and vice-versa. This is a rare but complex orthodontic issue.
- Delayed Eruption: The canine tooth takes significantly longer than the typical age range to emerge. This isn't necessarily an impaction but can be a precursor.
- Ankylosis: In very rare cases, a tooth's root can fuse directly to the bone, preventing any movement or eruption. This is more common in primary teeth but can affect permanent teeth.
Identifying these variations early is crucial, as the type of impaction or eruption anomaly directly influences the complexity and duration of treatment.
Causes / Why It Happens
The eruption of canine teeth, particularly the permanent ones, is a complex biological process that can be influenced by a myriad of factors. When things go awry, leading to delayed eruption or impaction, it's often due to one or a combination of these causes:
Genetic Predisposition
Genetics play a significant role in tooth size, jaw size, and the timing and path of eruption. If parents or close relatives had impacted canines or other dental anomalies, there's a higher likelihood that their children might experience similar issues. Some studies suggest a genetic link to specific syndromes that affect tooth development.
Insufficient Space in the Dental Arch
This is by far the most common reason for canine impaction. The permanent maxillary canines are typically the last anterior teeth (front teeth) to erupt. If there isn't enough space left between the lateral incisor and the first premolar, the canine tooth can become blocked and unable to descend properly. This lack of space can be due to:
- Small Jaw Size: The jaw simply isn't large enough to accommodate all the permanent teeth.
- Early Loss of Primary Teeth: If a baby canine is lost too early, adjacent teeth might drift into the space, blocking the path for the permanent canine.
- Late Loss of Primary Teeth: Conversely, if the baby canine is retained too long, it can prevent the permanent canine from erupting, forcing it into an abnormal path.
- Large Tooth Size: Relatively large permanent canine teeth can exacerbate space deficiencies.
Obstructions in the Eruption Path
Physical barriers can prevent a canine from erupting:
- Odontomas or Cysts: Benign tumors or fluid-filled sacs can develop in the bone and block the eruption path.
- Supernumerary Teeth: Extra teeth (also called supernumerary teeth) can be present in the bone and obstruct the normal eruption of the canine.
- Anomalous Root Formation: An abnormally shaped root of an adjacent tooth can interfere.
Abnormal Eruption Angle
Sometimes, the canine tooth germ (the developing tooth bud) starts in an incorrect position or angle within the bone. Instead of pointing downwards and outwards, it might be angled horizontally, too far towards the palate (roof of the mouth), or too far towards the cheek.
Systemic Factors and Syndromes
While less common, certain systemic conditions or syndromes can be associated with delayed or abnormal tooth eruption, including:
- Cleidocranial Dysplasia
- Down Syndrome
- Hypothyroidism
- Cleft lip and palate
Understanding these underlying causes helps dental professionals diagnose the specific issue and formulate the most effective treatment plan. Early detection through regular dental check-ups and X-rays is critical for mitigating the long-term impact of these issues.
Signs and Symptoms
The signs and symptoms of canine tooth eruption vary significantly depending on whether the eruption is normal or problematic. Recognizing these differences is crucial for timely intervention.
Normal Canine Tooth Eruption (Primary and Permanent)
For most children, the eruption of canine teeth, whether baby or permanent, is a relatively uneventful process, though it can still cause some discomfort.
What Does Baby Tooth Eruption Look Like? For primary canines, parents often observe:
- Gum Swelling and Redness: The gum tissue around where the tooth is emerging may appear slightly swollen, red, or tender.
- Irritability: Babies may be fussier than usual, especially leading up to the eruption.
- Increased Drooling: Excessive drooling is common as teeth push through the gums.
- Chewing on Objects: Babies often try to chew on toys, fingers, or anything they can get their hands on to relieve pressure.
- Mild Fever (Rare): While some parents report a slight increase in temperature, high fevers are generally not associated with teething and should be investigated by a pediatrician.
- Difficulty Sleeping: Discomfort can make it harder for infants to sleep through the night.
- Visible Bulge: Before the tooth fully emerges, you might see a whitish bulge under the gum line.
For permanent canines, children might experience similar but typically milder symptoms as their jaws are more developed:
- Mild Gum Soreness: A dull ache or tenderness in the gum area where the tooth is erupting.
- Pressure Sensation: A feeling of pressure as the tooth moves into position.
- Temporary Gaps: As the permanent canine makes its way, it might temporarily create gaps or shifts in adjacent teeth before settling into place.
Problematic Canine Tooth Eruption / Impaction
When a canine tooth fails to erupt properly, the signs can be more subtle but have greater long-term implications. Often, there are no pain symptoms until a complication arises, making early dental check-ups and X-rays essential.
What to Look For:
- Asymmetry in Eruption: If the canine on one side of the mouth has erupted, but the corresponding canine on the other side hasn't erupted within 6-12 months, it's a significant red flag.
- Non-Eruption by Age 13-14: If the permanent upper canine has not erupted by age 13-14, or the lower canine by 10-11, it's highly suggestive of an impaction.
- Visible Bulge in Abnormal Area: You might feel or see a bulge on the roof of the mouth (palatal impaction) or on the cheek side (buccal impaction) where the canine should not be.
- Delayed Loss of Baby Canine: The primary canine remains firmly in place long after its expected shedding time, indicating that the permanent tooth isn't pushing it out from beneath.
- Crowding of Adjacent Teeth: The lack of an erupting canine can cause other teeth to shift and become crowded, especially the incisors, as they drift into the space.
- Tilting or Flaring of Incisors: The developing permanent canine can put pressure on the roots of adjacent incisors, causing them to tilt, flare outwards, or even resorb (dissolve) their roots.
- Discolored Gums: Occasionally, the gum tissue over an impacted tooth might appear slightly discolored (blue or purple) due to the tooth being close to the surface.
- Pain (Less Common, but Possible): While impaction itself is often painless, pain can arise if the impacted tooth puts pressure on nerves, causes root resorption of an adjacent tooth, or becomes infected.
If any of these signs are observed, especially in children approaching the ages of permanent canine eruption, a prompt visit to a dentist or orthodontist is highly recommended. Early diagnosis significantly improves the success rate of interventions.
Treatment Options for Impaired Canine Eruption
When a canine tooth fails to erupt normally, especially if it's impacted, a range of treatment options are available. The choice of treatment depends on the specific type and severity of impaction, the patient's age, overall dental development, and the orthodontist's assessment.
1. Observation and Monitoring
- When: For very young children (ages 8-10) with mild impaction or delayed eruption, especially if space deficiencies are minimal.
- Process: Regular dental check-ups and X-rays to monitor the canine's position. Sometimes, simply removing an over-retained primary canine or creating minor space can allow the permanent canine to erupt spontaneously.
- Pros: Non-invasive, lowest cost if successful.
- Cons: Not always effective, may delay necessary treatment if the situation worsens.
- Cost: Included in regular dental visits ($50-$200 for exam and X-rays).
2. Space Creation
- When: When the primary issue is a lack of space for the canine to erupt.
- Process:
- Extraction of Primary Canine: If the baby canine is still present and blocking the path.
- Orthodontic Expansion: Using braces or expanders to widen the dental arch and create room.
- Distalization: Moving back teeth further back to create space in the front.
- Pros: Can prevent impaction or facilitate spontaneous eruption.
- Cons: May require additional orthodontic treatment.
- Cost: Extraction of primary tooth: $100-$300. Orthodontic expanders: $1,500-$3,500.
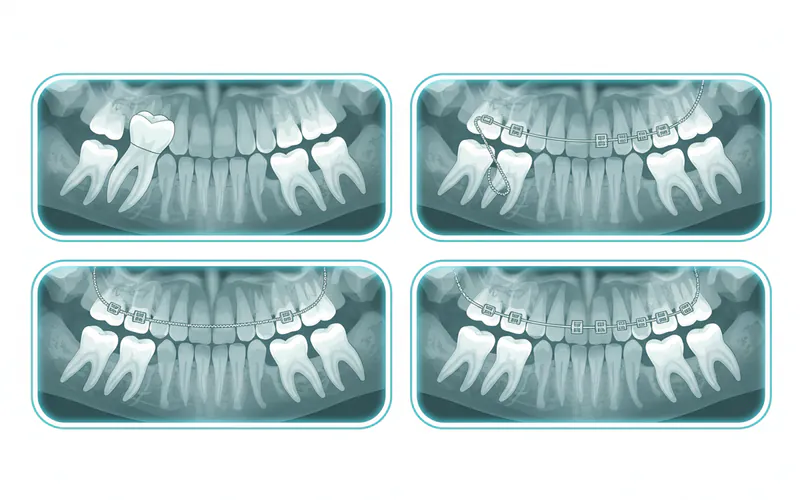
3. Surgical Exposure with Orthodontic Traction (Most Common)
- When: This is the primary treatment for most impacted canines that are good candidates for repositioning.
- Process:
- Surgical Exposure: An oral surgeon or periodontist surgically exposes the impacted canine.
- For palatal impactions, a small window of gum tissue is removed, and sometimes a tiny amount of bone, to reveal the crown. An orthodontic bracket with a small chain is then bonded directly to the exposed tooth. The gum tissue is then either sutured back around the bracket or left open.
- For buccal impactions, the tooth may be exposed, and the gum tissue trimmed to create a "window" for the tooth to erupt through (open eruption), or a bracket and chain are bonded, and the gum is closed over it (closed eruption).
- Orthodontic Traction: The attached chain is connected to the orthodontic archwire (braces). Over several months, the orthodontist applies gentle, continuous force to gradually pull the impacted canine into its correct position in the dental arch. This process is slow and controlled to avoid damaging the tooth or surrounding structures.
- Surgical Exposure: An oral surgeon or periodontist surgically exposes the impacted canine.
- Pros: Aims to save the natural tooth and achieve a functional, aesthetic outcome. High success rate when performed by experienced professionals.
- Cons: Invasive (surgical component), lengthy treatment time (often 6-12 months for traction alone, in addition to overall orthodontic treatment), discomfort post-surgery.
- Cost:
- Surgical exposure (by oral surgeon/periodontist): $800-$1,500 per tooth.
- Orthodontic bonding and traction (by orthodontist): $700-$2,500 per tooth (often included in overall comprehensive orthodontic treatment plans, which can range from $3,000-$8,000).
- Total additional cost for an impacted canine, separate from comprehensive orthodontics, could be $1,500-$4,000.
4. Autotransplantation
- When: A more complex option considered in rare cases where surgical exposure and traction are not feasible, usually if the impacted canine is severely displaced or if another tooth is missing in a suitable location.
- Process: The impacted canine is surgically extracted and immediately reimplanted into a prepared socket in its correct position in the dental arch.
- Pros: Uses the patient's natural tooth.
- Cons: Technically demanding, lower success rate than other options, requires a healthy tooth for transplantation, and specific root development stage.
- Cost: Highly variable, but generally expensive, ranging from $3,000-$6,000, plus potential root canal treatment for the transplanted tooth.
5. Extraction of the Impacted Canine
- When: This is typically a last resort, when the canine is severely malpositioned, fused to the bone (ankylosed), causing damage to adjacent teeth, or when other treatments have failed or are not practical.
- Process: The impacted canine is surgically removed by an oral surgeon.
- Pros: Resolves the immediate problem.
- Cons: Loss of a valuable natural tooth. Requires subsequent treatment to replace the missing tooth (dental implant, bridge, or leaving a gap, which can affect bite and aesthetics).
- Cost: Surgical extraction: $300-$600 per tooth. Subsequent tooth replacement (implant: $3,000-$6,000, bridge: $2,000-$5,000).
6. Extraction of the Deciduous Canine (Baby Tooth)
- When: Often done early to allow the permanent canine to erupt spontaneously, particularly if the permanent canine shows signs of erupting but is blocked by the primary tooth.
- Process: The primary (baby) canine is simply extracted.
- Pros: Simple, minimally invasive, potentially prevents impaction.
- Cons: Not always sufficient; needs careful monitoring for subsequent permanent canine eruption.
- Cost: $100-$300.
Comparison Table: Treatment Options for Impacted Canines
| Treatment Option | Description | Pros | Cons | Average US Cost Range (per tooth) * | Timeline |
|---|---|---|---|---|---|
| Observation | Monitor with X-rays. | Non-invasive, lowest cost. | Not always effective, potential for delayed treatment. | $50-$200 (for exams/X-rays) | Ongoing (months to years) |
| Space Creation (Orthodontics) | Use braces/expanders to make room. | Prevents impaction, avoids surgery. | Requires orthodontic treatment time. | $1,500-$3,500 (for expander) | 6-18 months |
| Surgical Exposure + Orthodontic Traction | Surgically expose tooth, bond bracket, pull with braces. | Saves natural tooth, excellent functional/aesthetic results. | Invasive, lengthy treatment, post-op discomfort. | $1,500-$4,000 (additional to full ortho) | Surgical: 1 hour. Traction: 6-12 months. Total ortho: 18-30 months. |
| Autotransplantation | Extract impacted canine, immediately replant into new socket. | Uses patient's natural tooth. | Complex, lower success rate, requires specific tooth conditions. | $3,000-$6,000 (plus possible root canal) | Surgical: 1-2 hours. Healing: 3-6 months. |
| Surgical Extraction | Remove the impacted canine. | Resolves immediate problem, less complex post-op than traction. | Loss of natural tooth, requires replacement (implant/bridge). | $300-$600 | Surgical: 30-60 min. Healing: 1-2 weeks. |

*Costs are estimates and can vary significantly based on geographic location, complexity, and specific provider.
Pro Tip: Early intervention is key. An orthodontic evaluation by age 7-8 can often predict potential impaction issues, allowing for simpler, less invasive treatments like space creation to guide the canine into proper position without surgery.
Step-by-Step Process for Surgical Exposure and Orthodontic Traction
This is the most common and detailed treatment for impacted canines. Here's what you can generally expect:
Step 1: Initial Consultation and Diagnosis
- Who: Orthodontist, General Dentist.
- What: Your orthodontist will perform a thorough clinical examination, reviewing your medical and dental history. Digital X-rays, including panoramic X-rays and potentially 3D cone-beam computed tomography (CBCT) scans, will be taken to precisely locate the impacted canine, assess its angulation, depth, and relationship to adjacent teeth and vital structures.
- Outcome: Confirmation of impaction, determination of its type (buccal or palatal), and initial treatment plan. This is also when your orthodontist may discuss types of teeth aligners or traditional braces that will be used for the traction and alignment phase.
Step 2: Pre-Surgical Orthodontic Preparation
- Who: Orthodontist.
- What: Before surgery, you will likely begin orthodontic treatment with braces or clear aligners. This phase is crucial for creating adequate space in the dental arch for the impacted canine to be pulled into. It may involve moving other teeth, expanding the arch, or removing crowded teeth if necessary.
- Duration: Typically 6-12 months.
Step 3: Surgical Exposure
- Who: Oral Surgeon or Periodontist.
- What: Once sufficient space is created, you will be referred to a specialist for the surgical procedure.
- Anesthesia: Local anesthesia will be administered to numb the area. Sedation options (e.g., nitrous oxide, oral sedation, or IV sedation) may also be offered for patient comfort.
- Incision: A small incision is made in the gum tissue over the anticipated location of the impacted tooth.
- Bone Removal (if necessary): If the tooth is covered by bone, a small amount of bone may be carefully removed to expose the crown.
- Attachment of Bracket: An orthodontic bracket with a small gold chain is carefully bonded to the exposed surface of the canine tooth.
- Closure/Open Eruption:
- Closed Eruption: For most palatal impactions, the gum tissue is gently repositioned and sutured back over the exposed tooth and bracket, leaving only the chain visible or tucked away. This protects the tooth during eruption.
- Open Eruption: For some buccal impactions, the gum tissue is trimmed to create a "window," leaving the tooth partially exposed to the oral cavity, which can allow for more rapid initial eruption.
- Duration: Approximately 45-90 minutes.
Step 4: Orthodontic Traction
- Who: Orthodontist.
- What: After the surgical site has healed (typically 1-2 weeks), you will return to your orthodontist.
- Activation: The orthodontist will attach the gold chain from the surgically exposed canine to the main archwire of your braces.
- Gentle Force: Very light, continuous forces are applied to gradually guide the impacted canine into its correct position. This usually involves adjustments to the chain or elastics during regular orthodontic appointments.
- Monitoring: Regular X-rays will be taken to monitor the tooth's movement and ensure it's progressing correctly.
- Duration: This phase can last anywhere from 6 to 18 months, depending on the severity of the impaction and the tooth's response.
Step 5: Final Orthodontic Alignment
- Who: Orthodontist.
- What: Once the canine tooth has been successfully brought into the dental arch, the remaining orthodontic treatment focuses on fine-tuning its position, aligning it with other teeth, and perfecting the overall bite. This might involve additional archwire adjustments, elastic wear, and specific bracket positioning.
- Duration: This is integrated into the broader orthodontic treatment, which often takes another 6-12 months after the canine is fully erupted.
Step 6: Retention
- Who: Orthodontist.
- What: After the braces are removed, retainers (removable or fixed) will be provided to maintain the new positions of your teeth, including the newly erupted canine, preventing them from shifting back.
- Duration: Lifelong retention is generally recommended.
Cost and Insurance
Understanding the financial aspect of canine tooth eruption issues is crucial for planning. Costs can vary widely depending on the complexity of the case, the chosen treatment, the region of the United States, and the specific dental professionals involved.
Average US Cost Ranges (Without Insurance)
- Initial Orthodontic Consultation & X-rays: $50 - $250
- Extraction of a Primary (Baby) Canine: $100 - $300
- Orthodontic Space Creation (e.g., Palatal Expander): $1,500 - $3,500 (often part of a larger orthodontic treatment)
- Surgical Exposure of Impacted Canine (Oral Surgeon/Periodontist fees):
- Simple (buccal): $800 - $1,200
- Complex (palatal, deep impaction): $1,200 - $1,500
- Orthodontic Bonding and Traction (Orthodontist fees, additional to comprehensive braces): $700 - $2,500
- Total for Surgical Exposure + Orthodontic Traction: $1,500 - $4,000 (on top of the cost of full orthodontic treatment)
- Comprehensive Orthodontic Treatment (Braces/Aligners):
- Traditional Metal Braces: $3,000 - $7,000
- Clear Aligners (e.g., Invisalign): $3,500 - $8,000
- Surgical Extraction of Impacted Canine (if not recoverable): $300 - $600
- Dental Implant (to replace extracted canine): $3,000 - $6,000 (per tooth, including abutment and crown)
- Dental Bridge (to replace extracted canine): $2,000 - $5,000 (for a 3-unit bridge)
Regional Cost Variations
Costs can be higher in major metropolitan areas and coastal states (e.g., New York, California) and generally lower in the Midwest and Southern states.
- Example for Surgical Exposure + Orthodontic Traction:
- Low Cost Region (e.g., Kansas, Alabama): $1,500 - $2,800
- Mid Cost Region (e.g., Ohio, Arizona): $2,000 - $3,500
- High Cost Region (e.g., New York, California): $2,500 - $4,000+
Insurance Coverage Details
Dental insurance coverage for canine tooth eruption issues can be complex and depends heavily on your specific plan.
- Orthodontic Coverage: Many dental insurance plans, especially employer-sponsored ones, offer coverage for orthodontics.
- Typically, there is a lifetime maximum benefit for orthodontics, ranging from $1,000 to $3,000.
- Plans may cover 50% of the cost up to this lifetime maximum, after a deductible is met.
- Some plans have age limitations for orthodontic coverage (e.g., only for dependents under 19).
- Surgical Coverage: The surgical exposure component is often considered a medical procedure, particularly if performed by an oral surgeon.
- It may be covered under your medical insurance plan or a specific dental surgery rider on your dental plan.
- Coverage for oral surgery can range from 50% to 80% after your medical deductible is met.
- Diagnostic Services: X-rays and consultations are usually covered at a higher percentage (e.g., 80-100%) by most dental plans.
- Exclusions: Purely cosmetic procedures are usually not covered. If the impacted canine is being extracted and not replaced, some plans might not cover the extraction if it's considered elective (though usually, removal of an impacted tooth is deemed medically necessary).
Pro Tip: Always contact your dental and medical insurance providers directly to understand your specific benefits, deductibles, co-pays, and lifetime maximums before beginning treatment. Obtain a pre-treatment estimate from your dental and oral surgery offices.
Payment Plans and Financing Options
Many dental and orthodontic practices offer payment plans to help manage costs:
- In-Office Payment Plans: Monthly installment plans directly through the practice, often interest-free for a certain period.
- Third-Party Financing: Companies like CareCredit or LendingClub provide healthcare financing with various interest rates and repayment terms.
- Flexible Spending Accounts (FSAs) / Health Savings Accounts (HSAs): You can use pre-tax dollars from these accounts to pay for eligible dental expenses, including orthodontic treatment and surgical procedures.
Recovery and Aftercare
Proper recovery and diligent aftercare are essential, especially following surgical exposure of an impacted canine, to ensure successful healing and minimize complications.
Immediately After Surgery (First 24-48 Hours)
- Pain Management: Expect some discomfort. Your oral surgeon will likely prescribe pain medication or recommend over-the-counter options like ibuprofen (Advil, Motrin) or acetaminophen (Tylenol). Take medication as directed.
- Swelling: Swelling is normal. Apply an ice pack to the outside of your cheek for 15-20 minutes on, 15-20 minutes off, for the first 24-48 hours.
- Bleeding: Minor oozing or bleeding from the surgical site is common. Bite gently on a gauze pad, changing it every 30-60 minutes if needed. Avoid vigorous rinsing or spitting.
- Diet: Stick to soft foods for the first few days (e.g., yogurt, smoothies, mashed potatoes, soups, scrambled eggs). Avoid hot liquids, hard, crunchy, or spicy foods that could irritate the surgical site.
- Oral Hygiene:
- Do NOT rinse your mouth vigorously for the first 24 hours.
- After 24 hours, you can gently rinse with warm salt water (1/2 teaspoon salt in 8 ounces warm water) 2-3 times a day, especially after meals.
- Brush your other teeth gently, avoiding the surgical area directly.
- Activity: Rest and avoid strenuous physical activity for at least 24-48 hours. Elevate your head with pillows when lying down to help reduce swelling.
First Week After Surgery
- Continued Soft Diet: Gradually reintroduce normal foods as comfort allows, but continue to be cautious around the surgical site.
- Oral Hygiene: Continue gentle salt water rinses. You may be prescribed an antimicrobial mouthwash (e.g., chlorhexidine) to use. Resume normal brushing and flossing for non-surgical areas. Be very careful around the bracket and chain if it's exposed.
- Check-up: You will likely have a follow-up appointment with your oral surgeon or periodontist within a week to ensure proper healing.
- Orthodontist Visit: Depending on the surgical approach, your orthodontist might want to see you within 1-2 weeks to begin activating the chain.
Long-Term Aftercare (During Orthodontic Traction)
- Orthodontic Adjustments: Attend all scheduled orthodontist appointments. These visits are critical for adjusting the forces on the chain to gradually move the canine.
- Oral Hygiene with Braces: Maintaining excellent oral hygiene is paramount with braces. Brush thoroughly after every meal, use floss threaders or interdental brushes, and consider a water flosser. Poor hygiene can lead to gum inflammation and cavities, especially around the erupting tooth.
- Diet with Braces: Avoid hard, sticky, or chewy foods that can damage braces or dislodge the chain.
- Monitoring for Issues: Be vigilant for any signs of infection (pus, increased pain, fever), excessive swelling, or if the chain breaks or detaches. Contact your orthodontist or surgeon immediately if you notice any problems.
Pro Tip: Follow all post-operative instructions meticulously. The success of the entire treatment hinges on good surgical healing and consistent orthodontic follow-up.
Prevention
While not all cases of abnormal canine eruption, especially those with a strong genetic component, can be entirely prevented, there are significant steps that can be taken to reduce the risk and ensure timely intervention. The key to prevention lies in early detection and proactive management.
1. Regular Dental Check-ups from an Early Age
- Beginning at age 1: The American Academy of Pediatric Dentistry (AAPD) recommends a child's first dental visit by age one. Regular check-ups throughout childhood allow dentists to monitor dental development.
- Monitoring Primary Dentition: Dentists can identify early signs of crowding or missing primary teeth that might indicate future space issues for permanent canines.
2. Early Orthodontic Evaluation
- Around Age 7-8: The American Association of Orthodontists (AAO) recommends a child's first orthodontic evaluation by age seven. At this age, a child typically has a mix of primary and permanent teeth, and the orthodontist can assess the developing bite and identify potential issues.
- Benefits of Early Evaluation:
- Space Analysis: Orthodontists can assess if there is enough space for the permanent canines to erupt.
- Detection of Impaction: X-rays at this age can often reveal the position and angle of developing permanent canines long before they are due to erupt.
- Interceptive Orthodontics (Phase 1): If potential issues are identified, early "interceptive" orthodontic treatment can be initiated. This might include:
- Extraction of Over-retained Primary Teeth: Removing a baby tooth that is not shedding on time.
- Space Maintainers: If a baby tooth is lost prematurely, a space maintainer can be used to hold the space open for the permanent canine.
- Palatal Expanders: To widen the upper jaw and create more room.
- Partial Braces: To move specific teeth to create space or guide eruption.
3. Monitoring for Over-retained Primary Canines
- Parents and dentists should pay close attention if a child's primary canine remains firmly in place significantly past its expected exfoliation (shedding) time (typically around 10-12 years old for upper canines, 9-11 for lower). This is often the first clinical sign of an underlying impaction.
4. Good Oral Hygiene
- While good hygiene doesn't prevent impaction directly, it ensures that if interceptive treatments or orthodontic appliances are needed, the oral environment is healthy, reducing the risk of complications like decay or gum disease during treatment.

5. Proper Nutrition
- A balanced diet supports overall growth and development, including healthy bone and tooth formation.
By taking these preventive steps, parents can significantly improve the chances that their child's permanent canine teeth will erupt smoothly and into their correct positions, potentially avoiding more complex and costly treatments later on.
Risks and Complications
While canine tooth eruption, especially when managed by dental professionals, generally has a high success rate, it's important to be aware of potential risks and complications, particularly concerning impacted canines and their treatment.
Risks of Untreated Impacted Canines
If an impacted canine is left untreated, it can lead to several serious issues:
- Root Resorption of Adjacent Teeth: The most concerning risk. The impacted canine can put pressure on the roots of neighboring teeth (especially the lateral incisors), causing them to dissolve or shorten. This can weaken these teeth and potentially lead to their loss.
- Damage to Adjacent Teeth: The crown of the impacted canine can erode the root surface of the adjacent tooth, making it vulnerable to decay or structural damage.
- Crowding and Malocclusion: The absence of the canine in its proper position can cause other teeth to shift and become crowded, leading to a misaligned bite (malocclusion) and aesthetic concerns.
- Cyst Formation: In some cases, a fluid-filled sac (dentigerous cyst) can form around the crown of the impacted tooth. These cysts can grow and damage surrounding bone and teeth.
- Infection: Although less common, an impacted tooth can become infected, leading to pain, swelling, and systemic issues.
- Referred Pain: Pressure from an impacted tooth can sometimes cause referred pain in the face, head, or jaw.
- Ankylosis: The impacted tooth may fuse to the surrounding bone, making it impossible to move orthodontically.
- Aesthetic Concerns: The missing canine creates a noticeable gap, and the baby canine may be retained, appearing smaller and yellower than the surrounding permanent teeth.
Risks and Complications of Treatment (Surgical Exposure & Orthodontic Traction)
While treatments are generally safe, potential complications can arise:
- Surgical Risks:
- Infection: As with any surgery, there's a risk of bacterial infection at the surgical site.
- Bleeding: Excessive bleeding during or after the procedure.
- Nerve Damage: Though rare, there's a slight risk of temporary or permanent damage to nearby nerves, leading to numbness or altered sensation.
- Damage to Adjacent Teeth/Roots: While careful planning minimizes this, there's a small risk of inadvertent damage to neighboring tooth roots during surgery.
- Insufficient Exposure: If the exposure isn't adequate, it can hinder successful orthodontic traction.
- Failure of Bonding: The bracket or chain might detach from the impacted tooth, requiring another minor surgical procedure to reattach it.
- Orthodontic Risks:
- Slow or No Movement: In some cases, the impacted canine may move very slowly or not at all, even with traction. This can be due to ankylosis, an unfavorable tooth position, or excessive force.
- Root Resorption of the Impacted Canine: The orthodontic forces applied to the impacted canine can sometimes lead to shortening of its own root, which can affect its long-term stability.
- Recurrence: If proper retention protocols are not followed, the newly aligned canine may shift back towards its original impacted position.
- Prolonged Treatment Time: The process of bringing an impacted canine into alignment can significantly extend the overall duration of orthodontic treatment.
- Aesthetic Concerns: While the goal is a beautiful smile, occasionally the gingival (gum) margin around the brought-down canine might be slightly uneven compared to its counterpart, requiring minor gum contouring later.
It is crucial to discuss all potential risks and benefits with your oral surgeon and orthodontist before proceeding with any treatment. They will help you understand the specific risks applicable to your unique situation.
Children / Pediatric Considerations
Canine tooth eruption in children is a critical phase of dental development, and parents play a vital role in monitoring this process. Understanding what does baby tooth eruption look like and the timeline for permanent teeth is essential.
Primary (Baby) Canine Eruption
- Timeline:
- Upper Baby Canines: Typically erupt between 16 to 22 months of age.
- Lower Baby Canines: Typically erupt between 17 to 23 months of age.
- Symptoms: As described in the "Signs and Symptoms" section, these include gum swelling, redness, irritability, increased drooling, and chewing on objects. These symptoms are generally mild and manageable.
- Parental Guidance:
- Comfort Measures: Offer chilled teething rings, gentle gum massage, or a clean, cool washcloth to chew on. Over-the-counter pain relievers (like infant acetaminophen) can be used as directed by a pediatrician.
- Oral Hygiene: Start brushing as soon as the first tooth emerges. Use a soft-bristled infant toothbrush and a tiny smear of fluoride toothpaste (rice-grain size) for children under three.
- Avoid Teething Gels with Benzocaine: The FDA advises against using gels containing benzocaine for children under two due to rare but serious side effects.
Permanent Canine Eruption
- Timeline:
- Lower Permanent Canines: Usually erupt between 9 to 12 years of age, typically before the upper canines.
- Upper Permanent Canines: Usually erupt between 11 to 12 years of age, making them the second-to-last teeth to erupt in the mouth (before wisdom teeth).
- Importance: Permanent canines are critical for the adult bite and facial aesthetics. Their proper eruption is a cornerstone of a healthy dentition.
- Pediatric Monitoring:
- Regular Dental Check-ups: Ensure your child has regular dental visits as recommended by the American Dental Association (ADA) and AAPD. This allows the dentist to monitor the shedding of primary teeth and the eruption of permanent ones.
- Early Orthodontic Evaluation (Age 7-8): This is the single most important preventive step for permanent canine issues. An orthodontist can use clinical exams and X-rays to:
- Assess Space: Determine if there is adequate space in the jaw for the canines to erupt.
- Identify Impaction Risks: Detect early signs of impaction, such as an abnormal eruption path or over-retained primary canines.
- Interceptive Treatment: Recommend early treatments (e.g., space maintainers, palatal expanders, timely extraction of baby teeth) to guide the permanent canines into their correct positions and potentially avoid impaction.
Pro Tip for Parents: If your child's primary canine tooth on one side falls out, but the corresponding canine on the other side does not within 6 months, or if a permanent canine has not appeared by age 13 (especially the upper ones), schedule an appointment with your dentist or orthodontist immediately. Early detection greatly simplifies treatment.
Frequently Asked Questions
What is the ideal age for canine tooth eruption?
The ideal age for primary (baby) upper canines to erupt is 16-22 months, and lower canines at 17-23 months. For permanent canines, the lower ones typically erupt between 9-12 years, and the upper ones between 11-12 years. Any significant delay beyond these ranges warrants a dental check-up.
Is canine tooth eruption painful?
Normal canine eruption can cause mild discomfort, soreness, or a dull ache as the tooth pushes through the gums. For babies, this might manifest as irritability or increased drooling. For permanent teeth, discomfort is usually less pronounced. Significant pain, swelling, or signs of infection are not normal and should be evaluated by a dentist.
What causes an impacted canine tooth?
Impacted canines are most commonly caused by a lack of space in the dental arch, which prevents the tooth from descending into its proper position. Other causes include genetic factors, an abnormal eruption path of the tooth bud, the presence of cysts or extra teeth (supernumerary teeth), or the prolonged retention of baby canine teeth.
Can an impacted canine erupt on its own without treatment?
While it's possible for some mildly delayed or partially impacted canines to eventually erupt, especially if space is created for them, severely impacted canines rarely erupt fully and correctly on their own. Without intervention, they are likely to remain impacted, potentially causing complications like damage to adjacent teeth.
What is the cost of treating an impacted canine?
The cost varies significantly based on the treatment. Surgical exposure and orthodontic traction typically range from $1,500 to $4,000 per tooth, in addition to the cost of comprehensive orthodontic treatment (which can be $3,000-$8,000). Extraction of an impacted canine costs $300-$600. These are estimates and can vary by region and complexity.
How long does it take to fix an impacted canine?
The process of surgically exposing an impacted canine and bringing it into alignment with braces usually takes 6-18 months of active orthodontic traction after the surgery. This is part of an overall orthodontic treatment plan that might last 18-30 months in total.
Can I get clear aligners (like Invisalign) if I have an impacted canine?
Yes, in many cases, clear aligners can be used to create space and manage the alignment once the impacted canine has been surgically exposed and brought into the arch using orthodontic traction. However, the initial phase of pulling the impacted tooth down often requires traditional braces and brackets. After the canine is mostly into position, some orthodontists transition to aligners for the finishing stages. Discuss the types of teeth aligners suitable for your specific situation with your orthodontist.
What are the alternatives to pulling down an impacted canine?
Alternatives include surgical extraction of the impacted canine (if it's not salvageable or if traction fails), followed by either leaving a gap, replacing the tooth with a dental implant, or creating a dental bridge. In very rare cases, autotransplantation (moving the tooth) might be considered.
Will my insurance cover the treatment for an impacted canine?
Most dental insurance plans offer some coverage for orthodontics (typically a lifetime maximum of $1,000-$3,000). The surgical component of exposing the tooth may be covered under your medical insurance plan or a dental surgery rider, often at 50-80% after deductibles. It's crucial to verify coverage with both your dental and medical insurance providers.
What happens if I don't treat an impacted canine?
Leaving an impacted canine untreated can lead to severe problems such as the roots of adjacent teeth dissolving, crowding and misalignment of other teeth, the formation of cysts, infection, and aesthetic issues. It can compromise the long-term health of your entire dental arch.
When to See a Dentist
Knowing when to seek professional dental attention for canine tooth eruption is crucial for preventing complications and ensuring optimal oral health.
Red Flags That Require Prompt Attention:
- Asymmetry in Eruption (Permanent Canines): If one permanent canine has erupted, but the corresponding canine on the opposite side of the mouth has not appeared within 6-12 months, schedule an appointment. This is a strong indicator of a potential impaction.
- Missing Permanent Canine by Age 13-14: If the permanent upper canine has not erupted by age 13-14, or the lower canine by 10-11, regardless of whether the primary canine is still present.
- Over-retained Primary Canine: If a child's baby canine is still firmly in place significantly past its expected shedding time (e.g., age 12 for an upper canine), and there's no sign of the permanent tooth.
- Visible Bulge in Abnormal Area: Feeling or seeing a hard lump or bulge on the roof of the mouth (palate) or high on the cheekbone where a canine tooth should not be.
- Crowding or Shifting of Other Teeth: If the incisors (front teeth) are starting to lean, flare, or develop significant gaps or crowding, it can be a sign that an impacted canine is putting pressure on them or that space is insufficient.
- Persistent Pain or Swelling: While mild discomfort is normal, significant, worsening pain, severe swelling, redness, or signs of infection (pus, fever) in the area of an unerupted canine warrant immediate attention.
- Damage to Adjacent Teeth: If an X-ray reveals that an impacted canine is damaging the roots of neighboring teeth.
Routine Care vs. Emergency:
- Routine Care: For general monitoring of canine eruption, particularly for children, regular dental check-ups (every 6 months) are sufficient. An initial orthodontic evaluation around age 7-8 is also routine preventive care.
- Scheduled Appointment: If you notice any of the "red flags" above, it generally warrants scheduling a non-emergency appointment with your general dentist or an orthodontist as soon as possible. While not always an "emergency," timely intervention is critical to prevent the situation from worsening.
- Emergency Appointment: If there is sudden, severe pain, signs of acute infection (fever, significant swelling spreading beyond the tooth area, difficulty swallowing), or uncontrolled bleeding, seek emergency dental care.
Early detection and intervention are paramount for the successful management of canine tooth eruption issues. Don't wait until complications arise; a simple X-ray can often reveal potential problems long before they become severe.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Tooth Eruption Order: Complete Guide
The journey of human teeth, from their initial emergence in infancy to the arrival of wisdom teeth in young adulthood, is a fascinating and crucial aspect of our overall health. Understanding the tooth eruption order is not just a matter of curiosity; it's a vital piece of knowledge that empower
February 23, 2026

Primary Tooth Eruption Sequence: Complete Guide
Did you know that by their third birthday, most children will have a full set of 20 primary teeth? The journey of these first teeth, from their initial appearance to their eventual replacement by permanent teeth, is a remarkable and often challenging milestone for both infants and parents. Understan
February 23, 2026

Permanent Tooth Eruption Sequence: Complete Guide
Welcome to SmilePedia.net, your trusted resource for comprehensive dental health information. The journey of your permanent teeth emerging into your mouth, known as the permanent tooth eruption sequence, is a fundamental aspect of oral development. Did you know that while primary (baby) teeth ty
February 23, 2026
Adult Tooth Eruption: Complete Guide
Have you ever wondered about the complex process that brings your permanent teeth into your mouth, or perhaps why some teeth never fully emerge? For many adults, the eruption of permanent teeth, particularly wisdom teeth, can be a source of significant discomfort, confusion, or even serious dental p
February 23, 2026