Knocked Out Tooth Emergency Near Me: Complete Guide

Key Takeaways
- A sudden blow to the face, a fall, or a sports injury can instantly change your smile, sometimes resulting in a tooth being completely knocked out. This harrowing experience, medically known as dental avulsion, is one of the most urgent dental emergencies you can face. Finding prompt and expert care
A sudden blow to the face, a fall, or a sports injury can instantly change your smile, sometimes resulting in a tooth being completely knocked out. This harrowing experience, medically known as dental avulsion, is one of the most urgent dental emergencies you can face. Finding prompt and expert care for a knocked out tooth emergency near me is not just about aesthetics; it's about preserving your natural tooth, preventing complications, and maintaining your overall oral health. In the United States, an estimated 5 million teeth are knocked out annually, highlighting how common yet critical this situation can be. Acting quickly and correctly within the first few minutes and hours can be the difference between successfully reimplanting the tooth and losing it permanently. This comprehensive guide will walk you through everything you need to know about managing a knocked out tooth, from immediate first aid to long-term treatment options, costs, and prevention strategies, ensuring you are prepared for this critical moment.
Key Takeaways:
- Time is Critical: For successful re-implantation, a knocked-out permanent tooth should be re-inserted into its socket or preserved in an appropriate medium within 30-60 minutes.
- Proper Handling: Always pick up the tooth by its crown, avoiding touching the root.
- Storage is Key: Best storage options (in order) are milk, saline solution, Save-A-Tooth kit, or inside the cheek (for adults only). Do NOT use tap water.
- Cost Range: Emergency dentist visit for replantation can range from $200 - $800. If the tooth is lost, replacement options like dental implants cost $3,000 - $6,000+ per tooth, and bridges $2,000 - $5,000.
- Children's Teeth: Knocked-out baby teeth are generally not re-implanted to avoid damaging developing permanent teeth. Seek immediate dental advice regardless.
- Follow-Up Care: Even if replanted, the tooth will require follow-up root canal treatment and long-term monitoring for complications like root resorption or infection.
- Prevention: Mouthguards are highly recommended for contact sports and activities with a risk of facial trauma.
What It Is / Overview
A "knocked out tooth," formally known as dental avulsion, occurs when a tooth is completely dislodged from its socket in the jawbone. This is distinct from a fractured tooth (where part of the tooth breaks off) or a luxated tooth (where the tooth is still in the socket but moved out of its normal position). In avulsion, the entire tooth, including its root, is separated from the surrounding tissues. This type of injury is a true dental emergency because the viability of the tooth for successful re-implantation is highly dependent on how quickly and appropriately it is handled after it leaves the socket.
When a tooth is avulsed, the tiny ligaments (periodontal ligament) that connect the tooth root to the jawbone are torn. The living cells on the surface of the tooth root, which are crucial for reattachment, begin to die if not kept moist and healthy. The faster these cells are preserved and the tooth is returned to its socket, the higher the chance of successful re-integration with the bone. Successful re-implantation can save your natural tooth, preserving its function, aesthetics, and preventing the need for more complex and costly replacement procedures down the line.
Types / Variations
While a knocked-out tooth primarily refers to complete avulsion, it's important to distinguish between different scenarios and degrees of injury:
1. Permanent (Adult) Tooth Avulsion
This is the most critical type for re-implantation. Adult teeth have fully formed roots, and the goal is always to save the natural tooth if possible. The success rate for replantation significantly decreases after 60 minutes out of the mouth, making immediate action paramount.
2. Primary (Baby) Tooth Avulsion
When a baby tooth is knocked out, the approach is generally different. Dentists typically advise against re-implanting primary teeth. The primary concern is to avoid potential damage to the developing permanent tooth bud located beneath the gum line. Re-implanting a primary tooth could lead to infection, fusion with the bone (ankylosis), or developmental issues for the permanent tooth. However, a dental visit is still crucial to ensure no fragments remain and to assess for other injuries.
3. Partial Avulsion (Luxation)
While not strictly a "knocked-out" tooth, luxation involves the tooth being displaced but still partially within the socket. It can be:
- Concussion: Tooth is sensitive but not displaced.
- Subluxation: Tooth is loosened but not displaced. Bleeding from the gum margin.
- Extrusive Luxation: Tooth is partially out of the socket.
- Lateral Luxation: Tooth is displaced sideways.
- Intrusive Luxation: Tooth is pushed into the socket.
These types of injuries also require immediate dental attention, as they can lead to pulp damage, root resorption, or eventual tooth loss if not properly treated.
Causes / Why It Happens
Dental avulsion usually results from sudden, forceful trauma to the mouth or face. Common causes include:
- Sports Injuries: High-impact contact sports like hockey, football, basketball, and soccer are frequent culprits. Accidents during recreational activities like skateboarding, cycling, or skiing also pose a significant risk.
- Falls: Tripping, slipping, or falling, especially in children, the elderly, or individuals with balance issues, can lead to direct impact on the mouth.
- Accidents: Automobile accidents, bicycle accidents, or workplace incidents can result in severe facial trauma, including knocked-out teeth.
- Fights/Assaults: Direct blows to the face during altercations are a common cause of dental avulsion.
- Other Trauma: Less common causes can include objects hitting the mouth (e.g., during play or work), or even severe impact from seemingly minor incidents depending on the angle and force.
Factors that might increase susceptibility to dental avulsion include:
- Protruding Upper Teeth (Overjet): Individuals with significantly protruding upper front teeth are more vulnerable to avulsion in case of a frontal impact.
- Lack of Protective Gear: Not wearing a mouthguard during sports dramatically increases the risk.
- Underlying Dental Conditions: While not a direct cause, severe gum disease can weaken the tooth's support structures, potentially making it easier for trauma to dislodge a tooth.
Signs and Symptoms
The signs and symptoms of a knocked-out tooth are usually obvious and immediate:
- Missing Tooth: The most apparent sign is an empty socket where a tooth used to be.
- Visible Tooth: The avulsed tooth will likely be found nearby, either on the ground or within the mouth.
- Bleeding: There will be active bleeding from the empty tooth socket and surrounding gum tissue. This can sometimes be quite profuse.
- Pain: Significant pain in the area of the missing tooth and potentially in the surrounding jaw and facial structures due to the trauma.
- Swelling: The gum tissue and possibly the lip or cheek around the injured area may begin to swell rapidly.
- Associated Injuries: Other injuries may be present, such as fractured bone (jaw, orbital, nasal), lacerations to the lips, tongue, or cheeks, or other dental trauma (e.g., fractured adjacent teeth).
- Difficulty Speaking or Eating: The missing tooth and associated pain will make it difficult to speak clearly or attempt to eat.
Recognizing Associated Issues: TMJ Swelling in Front of Ear
Sometimes, the trauma that causes a knocked-out tooth can also affect the temporomandibular joint (TMJ), which connects your jawbone to your skull. If you experience TMJ swelling in front of ear following a facial injury, it could indicate:
- Direct Trauma to the Joint: A blow near the ear or side of the face can directly injure the TMJ.
- Jaw Fracture: A fracture in the jawbone, even if not immediately obvious, can cause swelling and pain radiating to the ear area.
- Muscle Spasm: The muscles surrounding the TMJ can go into spasm due to trauma, leading to pain and swelling.
Any swelling in front of the ear after a facial injury should be evaluated by a dentist or oral surgeon, as it could signify a more complex injury requiring specific treatment in addition to managing the avulsed tooth.
Teeth Gum Swelling and What It Means
Teeth gum swelling can accompany a knocked-out tooth, but it can also be a symptom of various other dental emergencies or conditions. In the context of an avulsed tooth, gum swelling is primarily due to:
- Trauma: The immediate injury to the gum tissue around the socket causes inflammation and swelling.
- Bleeding: Blood accumulation beneath the tissue can contribute to swelling.
However, if gum swelling occurs without a recent avulsion, it could indicate:
- Abscess: An infection at the root of a tooth or in the gum tissue, often presenting as a localized, painful bump filled with pus.
- Gum Disease (Periodontitis): Chronic inflammation and infection of the gums, leading to swelling, redness, and bleeding.
- Impacted Wisdom Tooth: A wisdom tooth that cannot erupt properly can cause inflammation and swelling in the surrounding gum tissue.
- Food Impaction: Food lodged between teeth or under the gum line can irritate and inflame the gums.
- Cyst or Tumor: Although less common, persistent localized swelling could be a sign of a more serious underlying condition.
It is crucial to differentiate the cause of gum swelling. If it's related to trauma and a knocked-out tooth, emergency care is needed. If it's persistent and unexplained, a dental visit is also warranted to diagnose and treat the underlying issue.
Treatment Options
The primary goal for a knocked-out permanent tooth is re-implantation—placing the tooth back into its socket. If re-implantation isn't possible or successful, various replacement options exist.
A. Emergency Re-implantation (for Permanent Teeth)
This is the ideal treatment if performed promptly and correctly.
Pros:
- Preserves your natural tooth structure and appearance.
- Maintains the natural bite and chewing function.
- Avoids the need for prosthetic replacements immediately.
- Cost-effective compared to long-term replacement options.
Cons:
- Time-sensitive: Success rates drop dramatically after 30-60 minutes out of the mouth.
- Complications: Risk of root resorption (the body dissolving the root), ankylosis (tooth fusing to the bone), pulp necrosis (nerve death), and infection.
- Requires follow-up: Almost always requires root canal treatment and long-term monitoring.
- Not suitable for baby teeth.
B. Replacement Options (if Re-implantation Fails or isn't Possible)
If the tooth cannot be saved or replantation fails, you have several options for replacing the missing tooth:
1. Dental Implant
A dental implant is a titanium post surgically placed into the jawbone, acting as an artificial tooth root. After healing, a crown is attached to the implant.
Pros:
- Most natural-feeling and looking replacement.
- Preserves jawbone density, preventing bone loss.
- Does not affect adjacent teeth.
- High success rate and long-term durability (often lifelong).
Cons:
- Highest initial cost.
- Requires surgery and a healing period (several months).
- Not suitable for all patients (e.g., insufficient bone density, certain health conditions).
- Risk of surgical complications (infection, nerve damage).
2. Fixed Dental Bridge
A bridge consists of one or more artificial teeth (pontics) held in place by dental crowns cemented onto the natural teeth adjacent to the gap.
Pros:
- Provides a stable, fixed replacement.
- Less invasive than implants (no surgery).
- Faster treatment timeline than implants.
- Less expensive than implants, generally.
Cons:
- Requires preparation (shaping) of healthy adjacent teeth, which can weaken them.
- Does not prevent bone loss in the area of the missing tooth.
- Can be harder to clean, increasing the risk of decay in adjacent teeth.
- Typically lasts 5-15 years before needing replacement.
3. Removable Partial Denture (Flipper)
A removable partial denture is a prosthetic appliance that replaces one or more missing teeth, often held in place by clasps that attach to existing natural teeth.
Pros:
- Least expensive option.
- Non-invasive (no tooth preparation or surgery).
- Quickest to fabricate.
Cons:
- Removable, can feel less stable than fixed options.
- Can affect speech and eating.
- May irritate gums or surrounding teeth.
- Does not prevent bone loss.
- Least natural appearance and function.
- Can be temporary (e.g., while waiting for an implant to heal).
Step-by-Step Process: What to Do (And What to Expect)
Immediate action is critical for a knocked-out permanent tooth. Follow these steps precisely:
Immediate First Aid (What You Do)
- Stay Calm: Panic can lead to mistakes. Breathe and act quickly.
- Locate the Tooth: Find the tooth immediately.
- Handle with Care: Pick up the tooth by the crown (the chewing surface), never by the root. Touching the root can damage the delicate periodontal ligament cells necessary for reattachment.
- Clean the Tooth (Gently, if necessary):
- If dirty, gently rinse the tooth with milk or saline solution (like contact lens solution) for no more than 10 seconds.
- Do NOT scrub, scrape, or use soap/disinfectants. Do NOT dry the tooth.
- Do NOT wrap it in tissue or cloth.
- Re-insert the Tooth (If possible and you are an adult):
- This is the best option if done immediately and correctly.
- Gently try to push the tooth back into its socket. Make sure it's facing the correct way.
- Bite down gently on a gauze pad or clean cloth to hold it in place.
- Pro Tip: If you're unsure or uncomfortable, skip this step and proceed to proper storage. This step is generally not recommended for children due to the risk of aspiration or improper placement.
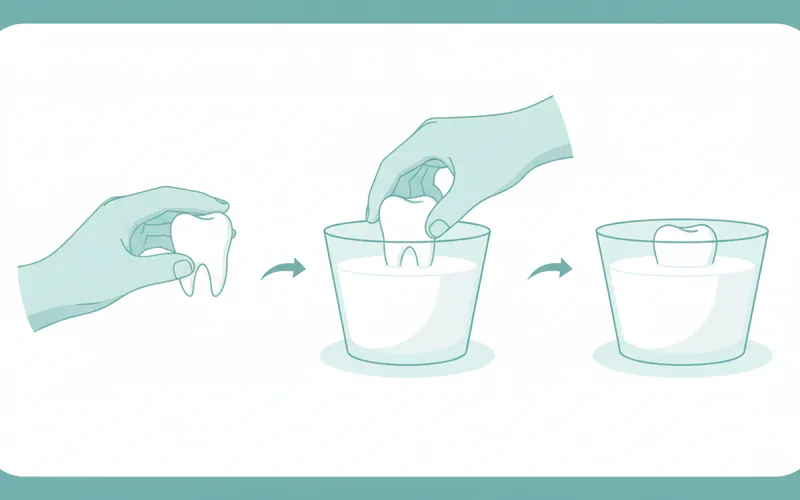
- Store the Tooth Correctly (If re-insertion isn't possible): The goal is to keep the root cells moist and viable.
- Best Options (in order of preference):
- A "Save-A-Tooth" kit: These commercial kits contain a special storage medium.
- Milk (cow's milk): Best readily available option, as it has a suitable pH and osmolality.
- Saline solution: Such as contact lens solution.
- Inside your mouth (between cheek and gum): Only for adults who can reliably prevent swallowing. This keeps the tooth moist in saliva. Do NOT do this for children due due to choking risk.
- Acceptable (short-term if others unavailable):
- Patient's own saliva: If you can collect it in a container.
- Absolutely NOT Recommended: Tap water. Its hypotonic nature causes root cells to swell and burst, killing them.
- Best Options (in order of preference):
- Seek Emergency Dental Care Immediately: Contact your dentist or an emergency dental clinic right away. Inform them you have a knocked-out tooth. Time is of the essence!
What to Expect at the Dentist
- Initial Assessment: The dentist will evaluate the tooth, its condition, and the socket. They'll also check for other injuries (fractures, lacerations). X-rays will be taken.
- Cleaning: The tooth and socket will be thoroughly rinsed.
- Re-implantation: If the tooth is viable, the dentist will carefully re-insert it into the socket.
- Stabilization (Splinting): The replanted tooth will be stabilized using a flexible splint, typically a thin wire and composite resin, bonded to adjacent healthy teeth. This splint usually stays in place for 1-2 weeks.
- Antibiotics & Tetanus Shot: The dentist may prescribe antibiotics to prevent infection. If the injury occurred outdoors or with contaminated objects, a tetanus booster might be recommended by your medical doctor.
- Root Canal Treatment: Almost all replanted permanent teeth will require root canal treatment, typically within 7-10 days after replantation, or once the splint is removed. This is because the pulp (nerve and blood vessels) inside the tooth is usually severed and dies, making it susceptible to infection.
- Follow-up Appointments: Regular follow-up appointments will be scheduled to monitor the tooth's healing, check for complications like root resorption or ankylosis, and ensure the splint is removed at the appropriate time.
Cost and Insurance
The cost of treating a knocked-out tooth in the US can vary significantly depending on whether the tooth is successfully replanted or if a replacement option is needed, and also on geographical location and the dentist's fees.
Cost of Emergency Re-implantation (Permanent Tooth)
- Emergency visit + Replantation: Generally ranges from $200 - $800. This often includes the emergency exam, cleaning, and re-insertion.
- Splinting: Usually included in the replantation cost, or an additional $100 - $300.
- Root Canal Treatment (subsequent): This is a separate procedure and typically costs $700 - $2,000+ per tooth, depending on the tooth's location (front teeth are generally less expensive than molars).
- Follow-up X-rays and Exams: $50 - $200 per visit.
Total for successful replantation with root canal: Approximately $1,000 - $3,000+.
Cost of Replacement Options (if Re-implantation Fails or isn't Possible)
These costs are for one tooth:
- Dental Implant:
- Implant Post (Surgery): $1,500 - $3,000
- Abutment: $300 - $600
- Crown: $1,000 - $2,500
- Total Per Tooth: $2,800 - $6,100+ (can be higher with bone grafting or complex cases).
- Fixed Dental Bridge:
- Per Unit: Typically priced per unit (two crowns on adjacent teeth + one pontic for the missing tooth = 3 units).
- Cost Per Unit: $700 - $1,700
- Total for a 3-unit Bridge: $2,100 - $5,100+
- Removable Partial Denture (Flipper):
- Cost: $300 - $800 (often used as a temporary placeholder).
Insurance Coverage Details
- Dental Insurance: Most dental insurance plans will cover a portion of emergency dental services.
- Emergency Exam & X-rays: Often covered at 80-100% after deductible.
- Replantation & Splinting: Typically considered a "major procedure" and may be covered at 50-80% after deductible.
- Root Canal: Also a "major procedure," covered at 50-80%.
- Dental Implants: Coverage varies widely. Some plans offer 0% coverage, others 50%. It's crucial to check your specific plan's benefits. Often, there are waiting periods or annual maximums that can limit coverage for implants.
- Bridges & Dentures: Usually covered at 50-80% as "major procedures."
- Medical Insurance: If the injury was part of a larger medical emergency (e.g., car accident, fall requiring ER visit), some aspects of initial diagnosis and stabilization (like X-rays or initial suturing of lacerations) might be covered by your medical insurance, but direct dental treatment usually falls under dental plans.
- Workers' Compensation: If the injury occurred at work, workers' compensation insurance should cover the full cost of treatment.
Pro Tip: Always contact your dental insurance provider before extensive treatment, even in an emergency, to understand your exact coverage, deductibles, and annual maximums. Your dentist's office can often help you with this.
Payment Plans and Financing Options
Many dental offices offer:
- In-house payment plans: Spreading the cost over several months.
- Third-party financing: Companies like CareCredit or LendingClub offer specialized healthcare credit cards with deferred interest options if paid within a certain timeframe.
- Discount dental plans: Not insurance, but offer reduced fees for a membership fee.
Recovery and Aftercare
Successful recovery after a replanted tooth depends heavily on diligent aftercare.
Immediately After Re-implantation:
- Pain Management: Over-the-counter pain relievers (ibuprofen, acetaminophen) or prescription medication for more severe pain.
- Diet: Stick to a soft diet for 1-2 weeks or as advised by your dentist. Avoid biting or chewing on the splinted tooth.
- Oral Hygiene: Brush gently around the splinted area using a soft-bristled toothbrush. Use an antimicrobial mouthwash (like chlorhexidine, prescribed by your dentist) to keep the area clean and reduce bacterial load.
- Avoid Habits: Refrain from biting fingernails, chewing on pens, or any habits that put stress on the splinted tooth.
- Avoid Strenuous Activity: Limit physical activity and contact sports while the splint is in place.
After Splint Removal & Root Canal:
- Continued Soft Diet: Gradual return to a normal diet as comfortable, but avoid very hard or sticky foods for a few more weeks.
- Regular Brushing and Flossing: Maintain excellent oral hygiene.
- Follow-up Appointments: Essential for long-term monitoring. The dentist will take X-rays to check for signs of root resorption, ankylosis, or infection. These complications can appear months or even years later.
- Mouthguard: If the injury was sports-related, invest in a custom-fitted mouthguard for future protection.
Potential Long-Term Issues:
- Root Resorption: The body's immune system can sometimes perceive the replanted tooth as foreign and begin to resorb (dissolve) the root. This can be external (from the outside) or internal (from within the pulp canal). It's the most common reason for long-term failure of replanted teeth.
- Ankylosis: The tooth fuses directly to the bone, losing its natural cushioning and becoming immobile. This can inhibit proper chewing and may lead to the tooth appearing "submerged" over time, especially in growing children.
- Discoloration: The tooth may darken over time due to pulp necrosis. Root canal treatment can help, and internal bleaching or a crown may be needed for cosmetic improvement.
- Infection: Although antibiotics are often prescribed, infection can still occur.
Prevention
Prevention is always better than cure, especially when it comes to preserving your natural teeth.

- Wear a Mouthguard for Sports: This is the single most effective way to prevent dental avulsion during athletic activities.
- Boil-and-bite mouthguards: Available over-the-counter, offer some protection.
- Custom-fitted mouthguards: Made by a dentist, offer the best fit, comfort, and protection, distributing impact force effectively. Highly recommended for contact sports (football, hockey, basketball, boxing), martial arts, and even recreational activities like skateboarding or mountain biking.
- Helmet Use: Wearing a helmet (e.g., for cycling, skiing, motorcycling) can protect against overall head and facial trauma, indirectly reducing the risk of dental injury.
- Safe Environment for Children:
- Child-proof your home.
- Supervise children, especially during play or on playgrounds.
- Use car seats and booster seats correctly.
- Avoid Chewing Hard Objects: Do not chew on ice, hard candies, or non-food items (e.g., pens, pencils) that could cause unexpected tooth fractures or avulsion if an underlying condition exists.
- Address Dental Issues: Promptly treat any dental problems like protruding teeth (overjet) with orthodontics, as they can increase the risk of injury.
Risks and Complications
Even with immediate and proper care, replanted teeth carry inherent risks and potential complications:
- Pulp Necrosis: The death of the nerve and blood vessels inside the tooth. This is almost universal in mature permanent teeth that have been avulsed, which is why root canal treatment is typically required.
- Root Resorption: As mentioned, this is the most common and serious long-term complication. The body's immune system mistakenly attacks and dissolves the tooth's root. There are different types:
- Surface Resorption: Mild, self-limiting, often doesn't require treatment.
- Inflammatory Resorption: Occurs when the necrotic pulp becomes infected, causing inflammation that triggers root dissolution. Prevented by timely root canal.
- Replacement Resorption (Ankylosis): The root surface is directly replaced by bone, leading to fusion. The tooth loses its natural flexibility and may appear shorter or "submerged" over time. This is more common with longer extra-oral dry times.
- Ankylosis: The tooth becomes rigidly fused to the bone, losing its natural mobility. This can be problematic, especially in growing children, as the tooth will not erupt further with the rest of the dentition, leading to an aesthetic and functional problem.
- Infection: Despite antibiotics, bacteria can still invade the root canal system or surrounding tissues.
- Discoloration: The tooth may darken due to pulp necrosis or hemorrhage within the dentin.
- Re-avulsion: The replanted tooth may be knocked out again if not adequately protected, especially during the healing phase.
- Failure of Replantation: In some cases, despite best efforts, the tooth simply does not reattach or develop severe complications, leading to its eventual loss.

Comparison of Storage Media for Avulsed Teeth
| Storage Medium | Description | Pros | Cons | Viability Preservation Time |
|---|---|---|---|---|
| Save-A-Tooth Kit | Commercial kit with Hank's Balanced Salt Solution (HBSS). | Optimal for preserving periodontal ligament cells. | Not widely available, may not be on hand immediately. | Up to 24 hours |
| Milk (Cow's) | Full-fat or skim milk. | Readily available, favorable pH, osmolality, and nutrients for cell viability. | Less ideal than HBSS for very long transport, but best readily available option. | 3-6 hours |
| Saline Solution | Sterile saline (e.g., contact lens solution, IV saline). | Isotonic, prevents cell bursting/shrinking. | Lacks nutrients, not as effective as HBSS or milk for extended periods. | 1-2 hours |
| Patient's Mouth | Held gently in cheek/gum pouch (for adults only). | Readily available, keeps tooth moist in saliva. | Risk of aspiration (choking) in children, not truly sterile. | Short-term (minutes) |
| Tap Water | Regular drinking water. | Readily available. | Highly detrimental. Hypotonic nature causes root cells to swell and burst, rapidly killing them. Leads to ankylosis/resorption. | <30 minutes |
Children / Pediatric Considerations
Handling a knocked-out tooth in a child differs significantly based on whether it's a primary (baby) tooth or a permanent (adult) tooth.
Knocked-Out Primary (Baby) Teeth:
- Do NOT Re-implant: The general rule is never to re-implant a knocked-out primary tooth. Doing so can cause serious damage to the developing permanent tooth bud underneath, leading to issues like enamel defects, root malformation, or even tooth impaction.
- Seek Dental Assessment: Even if re-implantation isn't recommended, it's crucial to see a pediatric dentist immediately. They will:
- Confirm it's a primary tooth.
- Check for any tooth fragments left in the socket or soft tissues.
- Assess for other injuries (jaw fractures, soft tissue lacerations).
- Discuss space maintenance if the child is very young, to prevent adjacent teeth from shifting and blocking the permanent tooth's eruption path.
- Monitor the eruption of the permanent tooth.
Knocked-Out Permanent Teeth in Children:
- Act Immediately, Same as Adults: If a permanent tooth is avulsed in a child, the same immediate first aid steps apply as for adults (handle by crown, proper storage, seek emergency care). The success rate for replantation is generally higher in younger permanent teeth because their roots are often not fully formed (open apex), allowing for better revascularization of the pulp.
- Different Root Canal Approach: If the root is immature, the dentist may attempt a procedure called apexification or revascularization to encourage the root to continue developing, rather than a full root canal immediately. This can potentially preserve the vitality of the pulp.
- High Risk of Complications: Children are also susceptible to complications like root resorption and ankylosis. Ankylosis is particularly problematic in growing children, as the fused tooth won't move with the rest of the jaw, potentially leading to an infra-occluded (submerged) tooth and cosmetic/functional issues requiring complex orthodontic or surgical intervention later.
Pro Tip: Always supervise children during play and ensure they wear custom-fitted mouthguards for any sports activities. Early education about dental safety is invaluable.
Cost Breakdown
To reiterate and summarize the average US costs for managing a knocked-out tooth, considering various scenarios:
Low-End Scenario (Successful Replantation with Insurance)
- Emergency Exam & Replantation: $200 (if highly covered by insurance)
- Splinting: $0-$100 (often included)
- Root Canal Treatment: $500 (for an anterior tooth, with good insurance coverage)
- Follow-up Visits (1-2): $50-$100
- TOTAL: $750 - $900 (after insurance contribution, not including deductible)
Mid-Range Scenario (Successful Replantation, Limited Insurance)
- Emergency Exam & Replantation: $400 - $800
- Splinting: $100 - $200
- Root Canal Treatment: $700 - $1,500
- Follow-up Visits (2-3): $100 - $300
- TOTAL: $1,300 - $2,800 (before insurance, or with moderate insurance coverage/high deductible)
High-End Scenario (Tooth Lost, Replaced by Dental Implant)
- Initial Emergency Visit (if tooth couldn't be saved): $200 - $500
- Dental Implant Placement (Post, Abutment, Crown): $2,800 - $6,100+
- Additional Procedures (Bone Grafting if needed): $500 - $2,500
- TOTAL: $3,500 - $9,100+ per tooth.
Without Insurance
If you don't have dental insurance, you would typically pay the full, unreduced fees for all procedures. A successful replantation and root canal could cost anywhere from $1,500 to $3,500. Replacing a tooth with an implant could easily exceed $3,000 to $6,000+ without any insurance contribution.
Payment Plans and Financing Options
- In-house payment plans: Many dental offices offer interest-free payment plans for larger treatments, allowing you to pay in installments over 3-12 months.
- Dental Credit Cards (e.g., CareCredit): These specialized credit lines for healthcare often offer promotional periods with 0% APR if the balance is paid within 6, 12, or 18 months. Be mindful of deferred interest if the balance isn't paid off.
- Personal Loans: Banks or credit unions may offer personal loans for larger dental expenses.
Cost-Saving Tips
- Act Fast: The best cost-saving tip is to act immediately to save the tooth. Replantation is far less expensive than any replacement option.
- Compare Costs: If choosing a replacement option, get quotes from several dentists, as prices can vary.
- Utilize Dental Schools: Dental schools often offer treatments at a reduced cost, performed by supervised students.
- Community Dental Clinics: Non-profit or government-funded clinics may offer services on a sliding scale based on income.
- Discount Dental Plans: These are not insurance but membership plans that offer a percentage off standard fees for an annual fee.
Frequently Asked Questions
What should I do immediately if my tooth gets knocked out?
Immediately find the tooth, pick it up by the crown (never the root), and if dirty, gently rinse it with milk or saline for no more than 10 seconds. Attempt to re-insert it into its socket if you are an adult and comfortable doing so. If not, store it in milk, saline, a Save-A-Tooth kit, or your cheek (for adults). Seek emergency dental care immediately, within 30-60 minutes if possible.
Can a knocked-out tooth always be saved?
No, successful replantation depends on several factors: how quickly the tooth is re-inserted, how it was handled and stored, the extent of damage to the tooth and surrounding tissues, and the patient's overall health. Primary (baby) teeth are generally not re-implanted. Even with perfect conditions, long-term complications like root resorption or ankylosis can occur.
Is it painful to have a tooth re-implanted?
The initial injury that caused the tooth to be knocked out is usually painful. During re-implantation, the dentist will numb the area with local anesthesia to minimize discomfort. You may experience some soreness and mild pain after the procedure, which can be managed with over-the-counter pain relievers or prescription medication.
How long does a replanted tooth last?
The longevity of a replanted tooth varies greatly. With optimal conditions and timely treatment, a replanted tooth can last for many years, even decades. However, complications such as root resorption or ankylosis can lead to eventual tooth loss, sometimes within months or a few years. Regular follow-up and monitoring are crucial.
What happens if I can't find my knocked-out tooth?
If you cannot find the tooth, or if it's a primary (baby) tooth, you still need to see a dentist immediately. The dentist will assess the empty socket for other injuries, check if any tooth fragments are present, and discuss replacement options if it was a permanent tooth. They will also check for any possible aspiration of the tooth if you coughed or inhaled after the injury.
What's the difference between a knocked-out tooth and a chipped or fractured tooth?
A knocked-out tooth (avulsion) means the entire tooth is completely out of its socket. A chipped tooth involves a small piece of enamel breaking off. A fractured tooth has a crack or break in the tooth structure, but it remains in the socket, though it may be loose or painful. All require dental attention, but avulsion is the most time-sensitive emergency.
Can I just use tap water to store the tooth?
No, absolutely not. Tap water is hypotonic, meaning it has a lower concentration of salts and minerals than the cells on the tooth's root. Placing the tooth in tap water will cause these delicate cells to swell and burst, severely reducing the chances of successful re-implantation and increasing the risk of complications. Always use milk, saline, or a Save-A-Tooth kit.
Will my dental insurance cover the cost of a knocked-out tooth?
Most dental insurance plans cover a portion of emergency dental services, including replantation and subsequent root canal treatment, typically at 50-80% after your deductible. Coverage for replacement options like dental implants or bridges varies significantly, with some plans covering little to nothing for implants. Always verify with your insurance provider.
What are alternatives if replantation isn't successful or possible?
If replantation isn't successful, the main alternatives are a dental implant, a fixed dental bridge, or a removable partial denture (flipper). Dental implants offer the most natural and long-lasting solution, while bridges are also fixed but require altering adjacent teeth. Removable partial dentures are the least expensive but also the least stable and natural.
How soon after replantation can I eat normally?
You should stick to a soft diet for at least 1-2 weeks after replantation, or as advised by your dentist. Avoid biting or chewing directly on the splinted tooth to allow proper healing and reattachment. Your dentist will guide you on gradually returning to a normal diet.
When to See a Dentist
Given the urgency of a knocked-out tooth, the answer is always immediately. This is a critical dental emergency requiring the fastest possible action.
You need to see a dentist (or emergency dental clinic) if:
- A permanent tooth has been completely knocked out (avulsed). Time is the most critical factor for successful re-implantation. Call ahead to inform them you're coming with an avulsed tooth.
- A primary (baby) tooth has been knocked out. While typically not re-implanted, a dentist needs to assess the socket for fragments, check for other injuries, and ensure the developing permanent tooth bud is safe.
- Any tooth is loose, displaced, or fractured after trauma. Even if not completely out, luxation or fractures are serious injuries that require prompt professional evaluation.
- You experience significant pain, bleeding, or swelling in the mouth or face after an injury. These are signs of trauma that need immediate attention.
- You notice swelling in front of your ear (TMJ swelling) after a facial injury. This could indicate a jaw or TMJ injury that needs to be diagnosed and treated.
- You have persistent, unexplained teeth gum swelling. While an avulsed tooth is an obvious cause, gum swelling can also signal infection (abscess), gum disease, or other issues requiring professional diagnosis.
Emergency vs. Scheduled Appointment Guidance:
- Knocked-out tooth (permanent): IMMEDIATE EMERGENCY. Go to the dentist or emergency dental clinic right now. Do not wait.
- Knocked-out tooth (baby): URGENT EMERGENCY. Call your pediatric dentist immediately to get guidance and an urgent appointment.
- Luxated (displaced) tooth: URGENT EMERGENCY. See a dentist as soon as possible, ideally within a few hours.
- Chipped/fractured tooth with pain or exposed nerve: URGENT EMERGENCY. See a dentist within 24 hours.
- TMJ swelling in front of ear or significant gum swelling without trauma: Schedule an appointment with your dentist promptly, typically within a day or two, but seek emergency care if accompanied by severe pain, fever, difficulty swallowing, or spreading infection.
Your prompt action can make all the difference in saving your tooth and preventing further complications.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

How to Relieve Gum Swelling
When your gums are swollen, it can be an alarming and uncomfortable experience, often signaling an underlying issue that requires attention. Statistics from the Centers for Disease Control and Prevention (CDC) reveal that **nearly half of adults aged 30 or older in the United States have some form o
February 23, 2026

Teeth Swelling: Complete Guide
When you experience teeth swelling, it's more than just a minor discomfort; it's a clear signal from your body that something is amiss within your oral cavity, often indicating an underlying infection or inflammation that requires prompt attention. A recent survey revealed that **over 25% of adu
February 23, 2026

Submandibular Salivary Gland Swelling: Complete Guide
When you notice a peculiar lump or uncomfortable fullness beneath your jaw, it can be an alarming experience. This sensation, often accompanied by pain and difficulty swallowing, could indicate submandibular salivary gland swelling. Affecting an estimated 1 in 10,000 adults annually, conditi
February 23, 2026

What Helps With Gum Swelling
Gum swelling, medically known as gingival swelling or gingivitis, is a common yet often underestimated dental issue affecting millions of Americans. Have you ever woken up with sore, puffy gums that bleed easily when you brush? You're not alone. Research indicates that nearly **half of all a
February 23, 2026