Swelling on Floor of Mouth Under Tongue: Complete Guide
Key Takeaways
- Experiencing a swelling on the floor of your mouth under your tongue can be an alarming and uncomfortable symptom, disrupting everything from eating and speaking to your general sense of well-being. While many people might initially dismiss it as a minor irritation, this type of swelling can sig
Swelling on Floor of Mouth Under Tongue: Complete Guide
Experiencing a swelling on the floor of your mouth under your tongue can be an alarming and uncomfortable symptom, disrupting everything from eating and speaking to your general sense of well-being. While many people might initially dismiss it as a minor irritation, this type of swelling can signal a range of conditions, some benign and others requiring immediate medical attention. In fact, oral and maxillofacial infections account for a significant portion of dental emergencies, underscoring the importance of understanding this symptom. This comprehensive guide from SmilePedia.net aims to demystify swelling under the tongue, providing you with detailed insights into its causes, symptoms, diagnosis, and treatment options. We'll explore everything from common salivary gland issues to rare but serious conditions, empowering you to recognize warning signs and seek appropriate care to protect your oral and overall health.

Key Takeaways:
- Common Causes: Swelling under the tongue is most frequently caused by salivary gland issues (stones, infections) or cysts (e.g., ranula). Less common but serious causes include abscesses, allergic reactions, and tumors.
- Urgency: Seek immediate dental or medical attention if swelling is accompanied by difficulty breathing, swallowing, fever, or rapid progression, as these can indicate a severe infection or airway compromise.
- Diagnosis: Diagnosis typically involves a thorough clinical examination, often supplemented by imaging such as X-rays, CT scans, or ultrasound to pinpoint the exact cause and extent.
- Treatment Variability: Treatment ranges from conservative measures like antibiotics for infections and warm compresses for inflammation, to surgical interventions for stones, cysts, or tumors.
- Cost Range: Initial consultations and minor treatments (e.g., antibiotics, drainage) can cost $150-$500. More complex procedures like salivary stone removal or cyst excision can range from $1,500-$5,000 or more, depending on complexity and location (dental office vs. hospital).
- Recovery: Recovery timelines vary significantly based on the cause and treatment, from a few days for minor infections to several weeks for surgical interventions.
- Prevention: Maintaining excellent oral hygiene, staying hydrated, and regular dental check-ups can help prevent some causes of swelling under the tongue.
What It Is / Overview
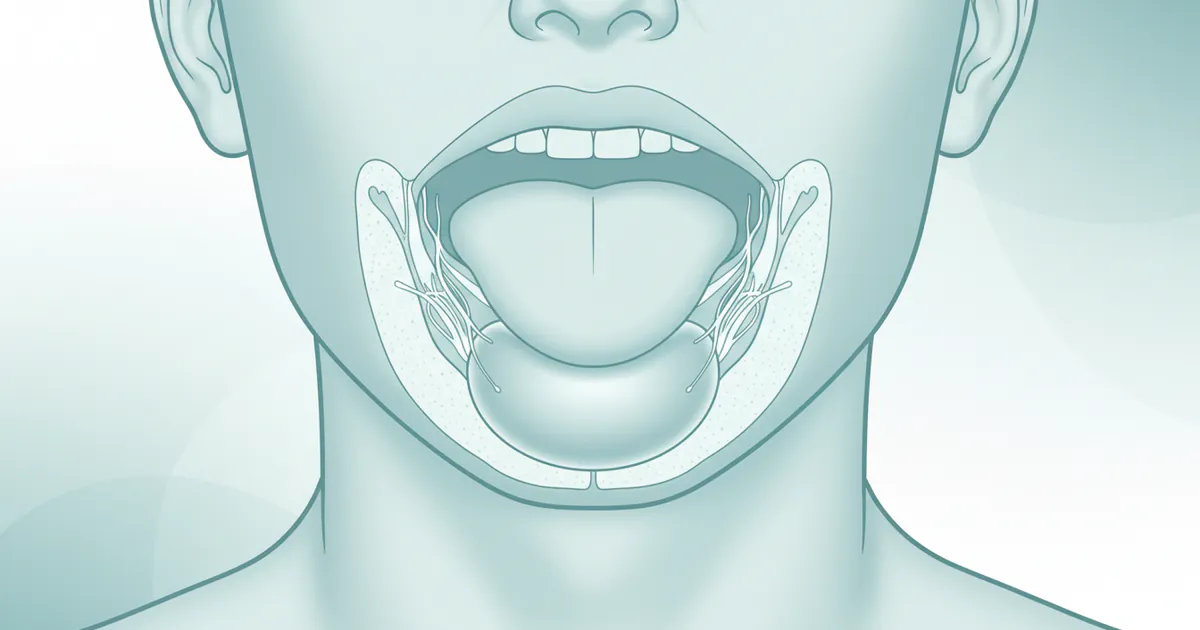
The floor of the mouth is the area directly beneath your tongue, extending from the inner surface of your lower jaw (mandible) to the base of your tongue. This region is vital, housing several structures including major blood vessels, nerves, muscles, and importantly, the sublingual and submandibular salivary glands and their ducts. When you experience a swelling on the floor of your mouth under your tongue, it signifies an abnormal enlargement or protrusion of tissue in this delicate area.
This swelling can vary greatly in appearance, texture, and accompanying symptoms. It might be soft and fluid-filled, firm and tender, red and inflamed, or even appear relatively normal in color. Its size can range from a small pea-like bump to a large mass that significantly impacts your oral function. The underlying cause determines these characteristics, making a precise diagnosis crucial for effective treatment. While the term "swelling" is broad, in this specific anatomical location, it often points to issues with the salivary glands or the development of a cyst or infection. It’s important to distinguish this localized swelling from more generalized conditions that might affect the entire mouth or other areas like TMJ swelling (which typically affects the jaw joint near the ear) or mouth swelling inside the cheek (which involves buccal mucosa or parotid gland issues). This article specifically focuses on the sublingual area, directly under the tongue.
Types / Variations of Swelling Under the Tongue
Swelling under the tongue isn't a single condition but rather a symptom of various underlying issues. Understanding the different "types" often refers to the specific medical diagnoses that manifest with this swelling. Here are the primary variations:
1. Salivary Gland Related Swelling
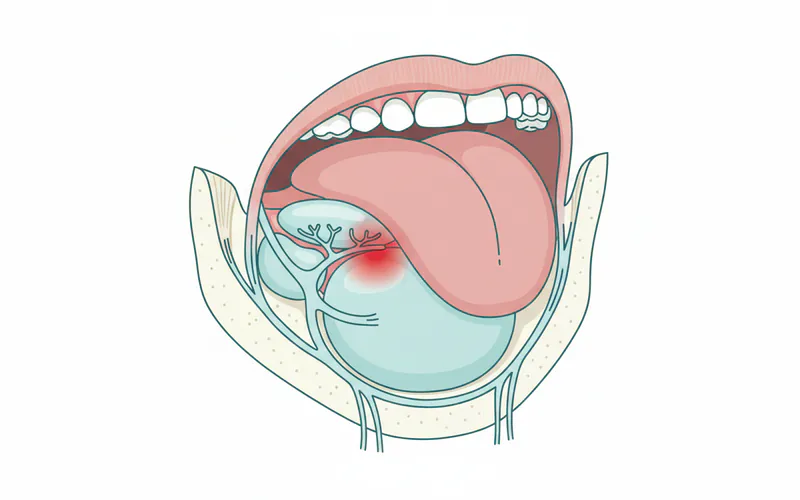
- Sialolithiasis (Salivary Stones): These are calcified deposits that form within the salivary glands or their ducts, obstructing the flow of saliva. The submandibular gland (Wharton's duct) is most commonly affected, and its duct empties precisely on the floor of the mouth under the tongue. When a stone blocks the duct, saliva backs up, causing a painful, often intermittent swelling that worsens with eating.
- Sialadenitis (Salivary Gland Infection): This is an infection of a salivary gland, often bacterial, which can occur secondary to a stone or due to dehydration, poor oral hygiene, or compromised immune function. It leads to painful, warm, red swelling, sometimes accompanied by pus drainage and fever. The sublingual and submandibular glands are susceptible.
- Mucocele/Ranula: A mucocele is a common, benign, fluid-filled lesion that results from the rupture of a minor salivary gland duct and subsequent leakage of mucin into the surrounding tissue. When this occurs on the floor of the mouth, specifically involving the sublingual gland, it's called a ranula. Ranulas are typically soft, bluish, translucent swellings. A "plunging ranula" is a larger, deeper variant that extends into the neck.
2. Infectious Swelling
- Dental Abscess/Odontogenic Infection: While typically originating from a tooth, a severe dental infection (e.g., from an infected lower molar) can spread to the floor of the mouth, creating an abscess or cellulitis in the sublingual space. This is a serious condition that can rapidly compromise the airway. Symptoms include severe pain, tenderness, firm swelling, fever, and difficulty opening the mouth (trismus).
- Cellulitis: A bacterial skin and soft tissue infection that can affect the floor of the mouth. It can be a progression from a dental abscess or other local trauma. It presents as diffuse, red, warm, tender swelling.
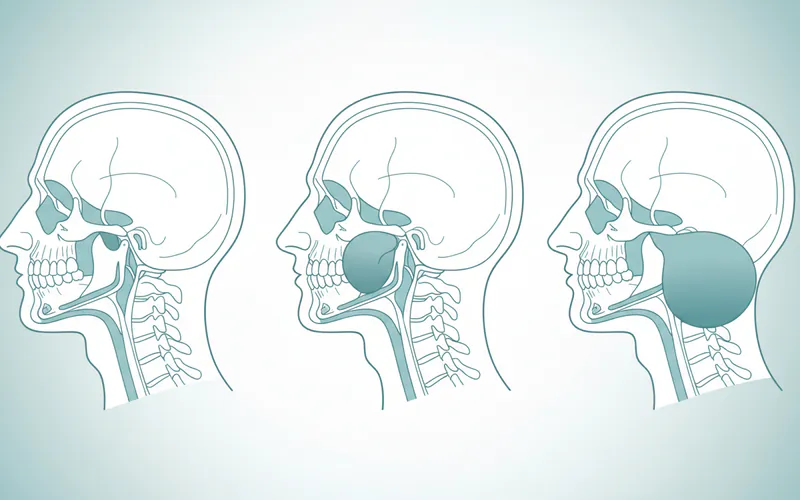
- Ludwig's Angina: This is a rapidly progressive, aggressive form of cellulitis that affects the submandibular, sublingual, and submental spaces bilaterally. It's often odontogenic in origin and can be life-threatening due to potential airway obstruction. The swelling can be firm, "woody," and rapidly spreads, pushing the tongue upwards and backwards.
3. Cystic Swelling
- Dermoid Cyst: A benign, congenital cyst that can develop on the floor of the mouth. It's usually slow-growing, painless, and rubbery or doughy to the touch. It contains various tissue components like hair follicles, sweat glands, and sebaceous glands.
- Epidermoid Cyst: Similar to a dermoid cyst but typically only contains keratinized epithelium. Also benign, slow-growing, and often asymptomatic until it grows large enough to cause mechanical obstruction or discomfort.
4. Allergic Reactions / Angioedema
- Angioedema: A severe allergic reaction or drug side effect (especially ACE inhibitors) that causes rapid, diffuse swelling of deeper tissues, including the tongue and floor of the mouth. This is a medical emergency due to the risk of airway obstruction. It typically appears suddenly and can be accompanied by difficulty breathing and hives.
5. Traumatic Swelling
- Hematoma: A collection of blood outside blood vessels, caused by injury or trauma to the floor of the mouth (e.g., from biting, dental procedures, or accidents). It can present as a soft, sometimes bluish swelling that may be painful.
- Post-Surgical Edema: Following oral surgery in the area, some swelling is expected as part of the healing process. This is usually transient and subsides over a few days.
6. Tumors (Benign and Malignant)
- Benign Tumors: These are non-cancerous growths, such as lipomas (fatty tumors), fibromas (fibrous tissue overgrowths), or salivary gland adenomas. They are usually slow-growing, painless, and mobile.
- Malignant Tumors (Oral Cancer): Squamous cell carcinoma is the most common type of oral cancer, which can develop on the floor of the mouth. It may initially appear as a persistent sore, a white or red patch (leukoplakia or erythroplakia), or a firm, fixed swelling. It often becomes painful as it progresses and may be associated with difficulty moving the tongue, speaking, or swallowing.
Causes / Why It Happens
The root causes for swelling under the tongue are diverse, stemming from infections, blockages, genetic predispositions, trauma, or abnormal cell growth. Here's a deeper dive into the common reasons:
- Salivary Gland Obstruction/Infection:
- Sialolithiasis (Salivary Stones): The most frequent cause, accounting for about 80-90% of all salivary gland obstructions. Stones form due to changes in saliva composition, dehydration, or inflammation. The submandibular gland duct (Wharton's duct) is especially prone due to its long, tortuous path and saliva's thicker, more alkaline nature. When saliva can't drain, it backs up, causing the gland to swell.
- Sialadenitis: Often a consequence of a salivary stone, but can also occur independently. Bacteria (like Staphylococcus aureus or Streptococcus viridans) enter the gland, especially when salivary flow is reduced. Factors like dehydration, chronic illness, and certain medications (antihistamines, diuretics) can contribute by decreasing saliva production.
- Cyst Formation:
- Ranula: Arises from trauma to a sublingual gland duct (minor trauma or rupture) or obstruction of the duct, leading to extravasation of mucus into the connective tissue or retention within the duct. They are pseudo-cysts as they lack a true epithelial lining in most cases of extravasation type.
- Dermoid/Epidermoid Cysts: These are developmental anomalies. Dermoid cysts contain ectodermal and mesodermal elements, while epidermoid cysts are simpler, lined by stratified squamous epithelium and containing keratin. They occur along embryonic fusion lines.
- Bacterial/Fungal Infections:
- Odontogenic Infections: Bacteria from a decayed tooth, gum disease, or a tooth extraction can spread into the deeper fascial spaces of the head and neck. The floor of the mouth is particularly vulnerable due to its proximity to the roots of the lower molars.
- Ludwig's Angina: A severe form of cellulitis, often initiated by an infected mandibular molar. It spreads rapidly, making it life-threatening.
- Allergic Reactions: Exposure to allergens (foods, medications, insect bites) can trigger an immune response causing angioedema. Certain medications, like ACE inhibitors, can also cause non-allergic angioedema.
- Trauma: Direct injury to the mouth floor, such as biting down hard, accidental punctures, or post-surgical irritation, can cause localized bleeding (hematoma) or inflammation.
- Neoplasms (Tumors):
- Benign: Can originate from fat cells (lipoma), fibrous tissue (fibroma), or salivary gland cells (pleomorphic adenoma, Warthin's tumor). Their growth mechanism is typically slow and localized.
- Malignant: Oral squamous cell carcinoma is strongly linked to tobacco and alcohol use, HPV infection, and chronic irritation. It involves uncontrolled growth of epithelial cells. Malignant salivary gland tumors are less common but can also manifest as swellings.
- Systemic Conditions (Less Common):
- Autoimmune diseases: Sjogren's syndrome can lead to chronic salivary gland inflammation and swelling, though usually more generalized dry mouth is the primary symptom.
- Nutritional deficiencies: Rarely, severe deficiencies might impact oral health, but are not direct causes of localized swelling under the tongue.
Signs and Symptoms
The presentation of swelling under the tongue can offer critical clues about its underlying cause. While swelling is the primary sign, associated symptoms help differentiate conditions.
- Visible or Palpable Swelling: The most obvious symptom. It can be localized to one side or extend across the floor of the mouth.
- Size: Varies from small (pea-sized) to large (obstructing tongue movement).
- Color: May be normal, red (inflammation/infection), bluish/translucent (ranula/hematoma), or white/grey (cancerous lesion or chronic irritation).
- Texture: Soft (fluid-filled, ranula, abscess), firm/hard (salivary stone, tumor, severe infection like Ludwig's Angina), or rubbery (dermoid cyst).
- Pain and Tenderness:
- Sialolithiasis: Often intermittent, sharp pain that intensifies during meals when saliva production increases.
- Infections (Sialadenitis, Abscess, Cellulitis): Constant, throbbing pain, worsening with touch or movement.
- Ranula, Dermoid/Epidermoid Cyst, Benign Tumors: Usually painless unless traumatized or very large.
- Malignant Tumors: Can be painless initially, but become painful as they grow or ulcerate.
- Difficulty with Oral Functions:
- Dysphagia (Difficulty Swallowing): Common with larger swellings, infections, or rapidly progressing conditions like Ludwig's Angina.
- Dysphonia (Difficulty Speaking): If the tongue's movement is restricted.
- Dyspnea (Difficulty Breathing): A critical emergency symptom, especially with Ludwig's Angina or severe allergic reactions, requiring immediate medical attention.
- Difficulty Chewing: Due to pain or mechanical obstruction.
- Restricted Tongue Movement: The tongue may feel "pushed up" or tethered.
- Systemic Symptoms (Indicating Infection/Inflammation):
- Fever and Chills: Strong indicators of a bacterial infection.
- Malaise: General feeling of unwellness.
- Lymphadenopathy: Swollen, tender lymph nodes in the neck.
- Other Localized Symptoms:
- Pus Drainage: May be observed from a salivary duct or an abscess if it ruptures. Often described as a foul taste in the mouth.
- Xerostomia (Dry Mouth): Can occur with salivary gland dysfunction or infection.
- Foul Breath (Halitosis): Associated with infections.
- Open Sore/Ulceration: Can indicate trauma, infection, or potentially malignancy.
- Numbness or Tingling: Could indicate nerve involvement, especially with aggressive tumors.
Pro Tip: Pay close attention to how quickly the swelling develops and if it's accompanied by systemic symptoms like fever or difficulty breathing. Rapidly progressing, painful swelling with systemic signs is often an emergency.
Treatment Options
Treatment for swelling under the tongue is highly dependent on the accurate diagnosis of the underlying cause. A dentist or oral and maxillofacial surgeon will typically lead the diagnosis and treatment plan.
1. Conservative Management
- Antibiotics:
- For: Bacterial infections like sialadenitis, dental abscesses, or cellulitis.
- Pros: Non-invasive, often effective for early-stage infections.
- Cons: Not effective for non-bacterial causes (cysts, stones, tumors), risk of antibiotic resistance, potential side effects (GI upset, allergic reactions).
- Typical Course: 7-14 days, often broad-spectrum initially (e.g., Amoxicillin-Clavulanate, Clindamycin).
- Pain Relievers and Anti-inflammatories:
- For: Symptomatic relief from pain and inflammation.
- Pros: Readily available over-the-counter (NSAIDs like ibuprofen) or prescription strength.
- Cons: Address symptoms, not the underlying cause; long-term use can have side effects.
- Warm Compresses & Massage:
- For: Sialolithiasis, sialadenitis, to encourage salivary flow and stone expulsion.
- Pros: Non-invasive, provides comfort.
- Cons: Not a primary treatment for most conditions, may not dislodge larger stones.
- Sialogogues (Salivary Stimulants):
- For: Sialolithiasis. Foods like sour candy or lemon drops can increase saliva production to help flush out stones.
- Pros: Natural, easy to use.
- Cons: Only effective for small stones or prevention; can cause discomfort if ducts are severely blocked.
- Corticosteroids/Antihistamines:
- For: Allergic reactions (angioedema).
- Pros: Rapidly reduce swelling, potentially life-saving for airway compromise.
- Cons: Systemic side effects with prolonged use, specific to allergic/inflammatory causes.
2. Surgical Interventions
- Abscess Drainage (Incision and Drainage - I&D):
- For: Localized abscesses.
- Pros: Immediate relief of pressure and pain, removal of infectious material, allows antibiotics to be more effective.
- Cons: Invasive, requires local anesthesia (or general for larger/deeper abscesses), risk of infection recurrence if source not addressed.
- Process: A small incision is made into the most prominent part of the swelling to release pus, sometimes a drain is placed.
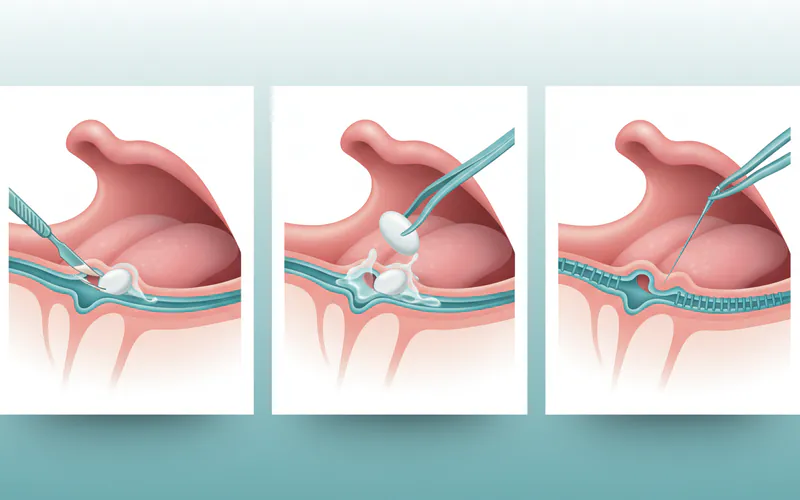
- Sialolithotomy (Salivary Stone Removal):
- For: Salivary stones, especially those palpable near the duct opening.
- Pros: Resolves obstruction, preserves the gland.
- Cons: Invasive, risk of duct damage, recurrence possible.
- Techniques:
- Transoral approach: Incision over the duct for accessible stones.
- Sialendoscopy: Minimally invasive, uses a tiny endoscope to visualize and retrieve stones from within the duct.
- Open surgery: For larger, deeper stones within the gland itself, which may require removal of the entire submandibular gland (sialadenectomy).
- Marsupialization/Excision (for Ranulas and Cysts):
- For: Ranulas, dermoid cysts, epidermoid cysts.
- Marsupialization: For ranulas, the roof of the cyst is removed, and the edges are sutured to the oral mucosa, creating a pouch that drains into the mouth.
- Pros: Less invasive than full excision, preserves gland.
- Cons: Higher recurrence rate than excision.
- Excision: Complete surgical removal of the cyst. For ranulas, this often involves removal of the entire sublingual gland to prevent recurrence.
- Pros: Lower recurrence rate.
- Cons: More invasive, potential for damage to surrounding structures.
- Biopsy and Tumor Excision:
- For: Suspected benign or malignant tumors.
- Pros: Definitive diagnosis, complete removal of the growth.
- Cons: Invasive, may require complex reconstructive surgery for malignant tumors, potential for functional deficits.
3. Adjunctive Therapies
- Radiation Therapy/Chemotherapy: For malignant tumors, often used in conjunction with surgery or as primary treatment for advanced cases.
- Lifestyle Modifications: Hydration, good oral hygiene, avoidance of irritants (tobacco, alcohol).
Step-by-Step Process: What to Expect During Treatment
The journey from initial symptom to full recovery involves several stages. Here's a general overview of what you can expect:
1. Initial Consultation and Diagnosis (Usually a Dental Office or ER)
- Patient History: Your dentist will ask about the onset of swelling, associated pain, any recent injuries, medications, and medical history.
- Clinical Examination: A thorough visual inspection and palpation (touching) of the floor of the mouth, tongue, and neck. The dentist will assess the size, texture, color, and tenderness of the swelling.
- Imaging (if necessary):
- X-rays (Occlusal or Panoramic): Good for detecting radiopaque salivary stones.
- Ultrasound: Excellent for differentiating fluid-filled cysts (ranulas), abscesses, and solid lesions, and can visualize salivary glands and ducts.
- CT Scan: Provides detailed cross-sectional images, crucial for evaluating deeper infections (like Ludwig's Angina), complex cysts, or tumors, and assessing bone involvement.
- MRI: Offers superior soft tissue contrast, useful for distinguishing between different types of soft tissue masses and determining tumor extent.
- Biopsy (if tumor suspected): A small tissue sample is taken and sent for pathological analysis to confirm the presence of cancer or other abnormal cells.
- Referral: Depending on the diagnosis, you may be referred to an oral and maxillofacial surgeon, ENT specialist, or general surgeon.
2. Treatment Implementation (Varies Greatly)
- For Infections (e.g., Sialadenitis, Small Abscess):
- Prescription: Antibiotics are prescribed immediately.
- Supportive Care: Instructions for warm compresses, pain medication, and increased hydration.
- Follow-up: A follow-up appointment within a few days to ensure the infection is resolving.
- For Salivary Stones (Sialolithiasis):
- Localized Anesthesia: If the stone is superficial, the area is numbed.
- Incision: A small incision is made along the salivary duct.
- Stone Removal: The stone is carefully extracted.
- Suturing: The incision may be closed with dissolvable sutures or left open to drain.
- Post-op Instructions: Care for the surgical site, pain management, and potentially sialogogues.
- For Ranula/Cysts (Marsupialization or Excision):
- Anesthesia: Local anesthesia with sedation or general anesthesia, especially for larger lesions or complete gland removal.
- Surgical Access: The surgeon accesses the cyst/ranula.
- Procedure:
- Marsupialization: The top of the ranula is removed, and the remaining edges are sutured to the oral mucosa.
- Excision: The entire cyst or ranula (and often the associated sublingual gland) is carefully dissected and removed.
- Closure: The surgical site is closed with sutures.
- Post-op Instructions: Detailed care instructions, dietary modifications, pain control.
- For Larger Abscesses/Ludwig's Angina:
- Hospital Admission: Often required due to the severity and risk of airway compromise.
- Airway Management: May include intubation or tracheostomy if breathing is severely compromised.
- Aggressive Drainage: Surgical incision and drainage of pus from the sublingual and submandibular spaces, often under general anesthesia. Multiple incisions may be needed.
- Intravenous Antibiotics: High-dose IV antibiotics are administered.
- Monitoring: Continuous monitoring of vital signs and airway patency.
3. Recovery and Aftercare
- Pain Management: Prescription or over-the-counter pain relievers will be recommended.
- Diet: Soft diet initially, gradually transitioning to normal food. Avoid spicy, acidic, or hard foods that might irritate the surgical site.
- Oral Hygiene: Gentle rinsing with salt water or prescribed medicated mouthwash to keep the area clean, avoiding direct brushing of the surgical site initially.
- Activity Restrictions: Avoid strenuous activity for a few days to weeks, depending on the invasiveness of the procedure.
- Follow-up Appointments: Essential to monitor healing, remove sutures (if non-dissolvable), and ensure there are no complications or recurrence.
- Specific Instructions: For conditions like Ludwig's Angina, recovery can be prolonged, requiring continued medical care and potentially physical therapy if jaw movement is restricted.
Cost and Insurance
The cost of treating swelling under the tongue in the US can vary significantly based on the diagnosis, the complexity of the treatment, the type of provider (general dentist, oral surgeon, hospital), geographic location, and whether you have dental and/or medical insurance.

Average US Price Ranges:
| Procedure / Service | Average Low (No Insurance) | Average Mid (No Insurance) | Average High (No Insurance) |
|---|---|---|---|
| Initial Consultation/Exam | $80 | $150 | $300 |
| X-rays (per film/series) | $25 | $75 | $150 |
| Ultrasound | $200 | $400 | $800 |
| CT Scan (Oral/Maxillofacial) | $400 | $800 | $2,000 |
| Antibiotic Prescription | $10 | $50 | $200+ (depending on drug) |
| Incision & Drainage (Abscess) | $300 | $700 | $1,500 |
| Sialolithotomy (Transoral) | $1,500 | $3,000 | $4,500 |
| Sialendoscopy | $2,500 | $5,000 | $8,000+ |
| Marsupialization (Ranula) | $1,000 | $2,500 | $4,000 |
| Excision (Ranula/Cyst w/ gland) | $3,000 | $6,000 | $10,000+ |
| Biopsy (Incisional/Excisional) | $300 | $800 | $1,500 |
| Hospital Stay (per day) | $1,000 | $3,000 | $10,000+ (ICU) |
Note: These are general estimates. Costs can be higher in metropolitan areas or for highly specialized surgeons. Hospital fees (anesthesia, facility charges) are often separate and can significantly increase the total cost, especially for procedures performed under general anesthesia.
Insurance Coverage Details:
- Dental Insurance: Typically covers a portion of diagnostic procedures (exams, X-rays), antibiotics, and sometimes minor surgical procedures (e.g., simple extractions if related, small abscess drainage). Major surgical procedures, especially those involving salivary glands or deep infections, may have limited coverage or be denied as "medical" rather than "dental."
- Medical Insurance: This is often the primary coverage for more complex issues like deep space infections (Ludwig's Angina), major salivary gland surgery, CT/MRI scans, hospital stays, and tumor excisions. It’s crucial to verify your plan’s coverage for oral and maxillofacial surgery, specialist visits, and hospitalizations.
- Coordination of Benefits: If both dental and medical insurance apply, they may coordinate benefits, meaning one plan pays first and the other covers a portion of the remaining balance. This can reduce your out-of-pocket expenses.
- Out-of-Pocket Expenses: Be prepared for deductibles, co-pays, and co-insurance. For significant procedures, reaching your out-of-pocket maximum is possible.
Pro Tip: Always contact your dental and medical insurance providers before treatment (if it's not an emergency) to understand your benefits, coverage limits, and any pre-authorization requirements. Ask for a detailed cost estimate from your provider.
Payment Plans and Financing Options:
- In-Office Payment Plans: Many dental and oral surgery offices offer installment plans.
- Third-Party Financing: Companies like CareCredit or Alphaeon Credit offer specialized healthcare credit cards with deferred interest options if paid within a certain period.
- Personal Loans: Banks or credit unions may offer personal loans for healthcare expenses.
- Negotiation: In some cases, if paying entirely out-of-pocket, you might be able to negotiate a discount with the provider.
Recovery and Aftercare
Successful recovery hinges on diligent aftercare, which varies depending on the treatment received.
General Post-Treatment Guidelines:
- Pain Management:
- Take prescribed pain medication as directed.
- Over-the-counter NSAIDs (ibuprofen, naproxen) or acetaminophen can manage mild to moderate pain.
- Swelling and Bruising:
- Apply cold compresses to the outside of the face/neck for the first 24-48 hours to minimize swelling.
- After 48 hours, switch to warm compresses to encourage blood flow and healing.
- Elevate your head while sleeping to reduce swelling.
- Diet:
- Start with clear liquids and soft foods (yogurt, mashed potatoes, soups) for the first few days.
- Gradually introduce semi-soft and then solid foods as comfort allows.
- Avoid hot, spicy, acidic, crunchy, or chewy foods that might irritate the surgical site or displace sutures.
- Oral Hygiene:
- Gently rinse your mouth with warm salt water (1/2 teaspoon salt in 8 ounces warm water) several times a day, especially after meals. This helps keep the area clean and promotes healing.
- Avoid vigorous rinsing or spitting for the first 24 hours to prevent dislodging blood clots.
- Continue brushing other teeth normally, but avoid the surgical site until your dentist advises.
- Activity Restrictions:
- Rest is crucial. Avoid strenuous physical activity for at least 3-7 days, or as advised by your surgeon, to prevent bleeding and swelling.
- Do not smoke or use tobacco products, as they significantly impair healing and increase complication risks. Avoid alcohol.
- Follow-up Appointments:
- Attend all scheduled follow-up appointments to allow your dentist or surgeon to monitor your healing progress, remove sutures, and address any concerns.
Specific Aftercare for Salivary Gland Issues:
- For Sialolithiasis: Continue to hydrate well and use sialogogues (sugar-free sour candies) to stimulate saliva flow, which can help prevent future stone formation.
- For Ranulas: If marsupialized, follow strict oral hygiene to prevent the new "pouch" from closing prematurely. If excised, monitor for recurrence, though less common.
Warning Signs Requiring Immediate Attention:
- Increased swelling or pain after the first 2-3 days.
- High fever or chills.
- Difficulty breathing or swallowing worsening.
- Excessive bleeding.
- Pus or foul-smelling discharge from the surgical site.
- Numbness or tingling that doesn't resolve.
Prevention
While not all causes of swelling under the tongue are preventable, you can significantly reduce your risk for many common conditions.
- Maintain Excellent Oral Hygiene:
- Brush your teeth twice a day for two minutes with fluoride toothpaste.
- Floss daily.
- Regularly use an antiseptic mouthwash to reduce bacterial load.
- This prevents dental infections that can spread to the floor of the mouth.
- Stay Hydrated:
- Drink plenty of water throughout the day. Dehydration reduces saliva production, increasing the risk of salivary stone formation and gland infections.
- Regular Dental Check-ups and Cleanings:
- Visit your dentist every six months for comprehensive exams and professional cleanings. Early detection of dental problems, salivary gland issues, or suspicious lesions is key.
- Avoid Tobacco and Limit Alcohol:
- Smoking and excessive alcohol consumption are major risk factors for oral cancer and can compromise overall oral health. The ADA strongly recommends avoiding these substances.
- Manage Underlying Medical Conditions:
- If you have conditions like Sjogren's syndrome or take medications that cause dry mouth, discuss management strategies with your doctor.
- Healthy Diet:
- Eat a balanced diet rich in fruits and vegetables. Limit sugary and acidic foods that can contribute to dental decay and inflammation.
- Address Dry Mouth (Xerostomia):
- If you suffer from chronic dry mouth, discuss solutions with your dentist or doctor, such as artificial saliva products, humidifiers, or medications that stimulate saliva production.
- Be Aware of Medication Side Effects:
- If starting new medications, especially ACE inhibitors, be aware of angioedema as a potential side effect and report any swelling promptly.
Risks and Complications
Even with appropriate treatment, there are potential risks and complications associated with swelling under the tongue and its management.
- Airway Obstruction: This is the most life-threatening complication, especially with severe infections like Ludwig's Angina or rapidly progressing angioedema. Swelling can push the tongue back, blocking the airway.
- Spread of Infection: Untreated or inadequately treated infections can spread to deeper fascial spaces, the blood (sepsis), or even the brain.
- Nerve Damage: Surgical procedures in the floor of the mouth carry a risk of temporary or permanent damage to nerves, particularly the lingual nerve (affecting sensation and taste on the tongue) or the hypoglossal nerve (affecting tongue movement).
- Bleeding: Post-operative bleeding can occur, sometimes requiring further intervention.
- Scarring: Surgical incisions can result in scar tissue, which may affect aesthetics or, rarely, restrict tongue movement.
- Recurrence:
- Ranulas have a recurrence rate of 5-20% after marsupialization if the gland isn't also removed.
- Salivary stones can recur if the predisposing factors (e.g., dehydration) are not addressed.
- Cysts or tumors may recur if not completely excised.
- Salivary Fistula: After salivary gland surgery, an abnormal tract (fistula) may form, leading to persistent leakage of saliva into the mouth or onto the skin.
- Dry Mouth: Removal of a salivary gland (e.g., sublingual or submandibular) can lead to a localized reduction in saliva, potentially causing dry mouth symptoms.
- Difficulty with Oral Functions: Persistent pain, swelling, or nerve damage can lead to long-term difficulties with speaking, swallowing, or chewing.
- Anesthesia Risks: As with any surgical procedure, there are risks associated with local or general anesthesia, including allergic reactions, respiratory problems, or cardiovascular events.
Children / Pediatric Considerations
Swelling on the floor of the mouth under the tongue in children warrants careful attention, as their smaller airways make them more vulnerable to obstruction.
- Ranulas: These are the most common cause of non-inflammatory swelling under the tongue in children, particularly in newborns and young children. They typically appear as soft, bluish, translucent lesions. While usually benign, they can grow large enough to interfere with feeding, swallowing, or breathing, especially if they are plunging ranulas extending into the neck. Treatment is usually surgical (marsupialization or excision with the sublingual gland).
- Dermoid and Epidermoid Cysts: These are also common congenital lesions in children, though less frequent than ranulas. They are typically firm, rubbery, and painless, and may grow slowly. Treatment is surgical excision.
- Sialadenitis (Salivary Gland Infection): While less common than in adults, children can develop salivary gland infections, often linked to dehydration, viral infections (e.g., mumps, though less common now due to vaccination), or rarely, salivary stones. Symptoms include fever, pain, and localized swelling. Treatment involves antibiotics and supportive care.
- Trauma: Children are prone to oral injuries from falls, sports, or foreign objects, which can cause hematomas or inflammation leading to swelling.
- Dental Infections: Severe dental infections in primary or permanent teeth can spread and cause sublingual swelling in children, similar to adults, but can progress more rapidly due to immature immune systems.
- Ludwig's Angina: Although rare in children, it is extremely dangerous. Any rapidly progressing, firm swelling with fever and difficulty breathing or swallowing in a child needs immediate emergency medical evaluation.
Pro Tip for Parents: If your child develops swelling under the tongue, observe for changes in feeding, breathing, or overall behavior. Any fever, increased pain, or difficulty breathing requires urgent medical attention. Early diagnosis and intervention are critical in children.
Cost Breakdown
Understanding the cost breakdown for treating swelling under the tongue is crucial for financial planning. Here's a more detailed look, emphasizing scenarios with and without insurance.
| Service/Procedure | Average Cost (Without Insurance) | Average Cost (With Insurance - Patient Out-of-Pocket) | Notes |
|---|---|---|---|
| Initial Exam/Consultation | $80 - $300 | $20 - $75 (co-pay) | Often covered 80-100% by dental plans after deductible. |
| X-rays (occlusal/panoramic) | $25 - $150 | $10 - $40 | Basic X-rays usually covered by dental insurance. |
| CT/MRI Scan | $400 - $2,000+ | $100 - $500+ (co-pay/co-insurance after deductible) | Primarily covered by medical insurance. Often subject to deductible. |
| Antibiotics (Prescription) | $10 - $200+ | $0 - $50 (co-pay) | Covered by medical prescription plans. Price varies by generic/brand. |
| Minor I&D (Abscess) | $300 - $1,500 | $50 - $400 | May be covered by dental or medical insurance. |
| Sialolithotomy (Transoral) | $1,500 - $4,500 | $300 - $1,500 | Often covered by medical insurance for functional issues. |
| Sialendoscopy | $2,500 - $8,000+ | $500 - $2,500+ | Specialized procedure, typically medical insurance. |
| Ranula Marsupialization | $1,000 - $4,000 | $200 - $1,000 | Often covered by medical insurance. |
| Ranula/Cyst Excision (w/ gland) | $3,000 - $10,000+ | $500 - $3,000+ | Significant surgery, generally medical insurance. |
| Biopsy | $300 - $1,500 | $50 - $400 | Can be covered by dental or medical. |
| Hospital Stay (per night) | $1,000 - $10,000+ | $500 - $3,000+ | Strictly medical insurance, subject to high deductibles/co-insurance. |
| Anesthesia Fees (separate) | $300 - $2,000+ (per hour) | $100 - $800+ | Depends on type (local, IV sedation, general) and duration. |
Cost-Saving Tips:
- Understand Your Insurance: Before any non-emergency procedure, call your dental and medical insurance providers. Ask about deductibles, co-pays, co-insurance percentages, and out-of-pocket maximums. Confirm if the specific procedure and provider are in-network.
- Get Multiple Quotes: For elective or non-emergency procedures, inquire about costs from different oral surgeons or specialists in your area.
- Generic Prescriptions: Always ask your doctor if a generic version of a prescribed medication is available, as it's significantly cheaper.
- Payment Plans: Many offices offer interest-free payment plans for several months. Don't hesitate to ask.
- Health Savings Account (HSA) or Flexible Spending Account (FSA): If you have an HSA or FSA, use these tax-advantaged accounts to pay for qualified medical expenses.
- Negotiate Cash Prices: If you are uninsured or paying entirely out-of-pocket, ask if the provider offers a discount for cash payments made upfront.
Frequently Asked Questions
### 1. Is swelling under the tongue always a medical emergency?
Not always, but it can be. While some causes like a small ranula may be benign, others like a rapidly spreading infection (Ludwig's Angina) or severe allergic reaction (angioedema) are life-threatening emergencies due to potential airway obstruction. Always seek prompt evaluation if swelling is painful, rapidly growing, or accompanied by difficulty breathing or swallowing, fever, or chills.
### 2. What's the difference between a ranula and a salivary stone?
A ranula is a type of mucocele, a fluid-filled cyst that results from mucus leakage from a damaged salivary gland, typically the sublingual gland. It appears as a soft, bluish, translucent swelling. A salivary stone (sialolith) is a calcified deposit that blocks a salivary duct, often from the submandibular gland, leading to a build-up of saliva and painful, firm swelling, especially during meals.
### 3. Can I treat swelling under my tongue at home?
Minor swelling due to minor trauma or very early-stage sialadenitis might respond to warm compresses, increased hydration, and good oral hygiene. However, most causes require professional diagnosis and treatment. Attempting to drain an abscess yourself or ignoring a salivary stone can lead to severe complications. Always consult a dental professional.
### 4. How long does it take for swelling under the tongue to go away?
The duration varies greatly. Swelling from a minor infection treated with antibiotics might resolve within a few days to a week. Surgical removal of a salivary stone or cyst may involve several days to weeks of recovery. Untreated or chronic conditions can persist indefinitely or worsen over time.
### 5. What kind of doctor treats swelling under the tongue?
You should initially consult your general dentist. Depending on the diagnosis, they may refer you to an oral and maxillofacial surgeon (OMFS), an otolaryngologist (ENT specialist), or, in emergency situations, the emergency room for urgent medical care.
### 6. Will insurance cover the cost of treatment?
Coverage depends on your specific dental and medical insurance plans and the underlying cause. Minor procedures might be covered by dental insurance, while more complex surgeries, imaging (CT/MRI), and hospital stays are typically covered by medical insurance. It's crucial to verify coverage with both providers.
### 7. Can stress cause swelling under the tongue?
While stress itself doesn't directly cause swelling under the tongue, it can exacerbate certain conditions or impact your immune system, potentially making you more susceptible to infections or flare-ups of existing oral health issues. Chronic stress can also lead to habits like clenching or grinding, though this typically affects other areas.
### 8. Is oral cancer a common cause of this type of swelling?
While less common than salivary gland issues or cysts, oral cancer, specifically squamous cell carcinoma, can manifest as a persistent, often painless, firm swelling or ulcer on the floor of the mouth. This is why any persistent swelling that doesn't resolve within a couple of weeks warrants a professional examination.
### 9. What happens if I ignore the swelling?
Ignoring swelling under the tongue can lead to serious complications. Infections can spread, potentially causing life-threatening airway obstruction (like Ludwig's Angina) or sepsis. Salivary stones can lead to chronic pain and recurrent infections. Cysts can grow larger, impacting speech and eating. Undiagnosed cancer can spread, making treatment more difficult and reducing prognosis.
### 10. Can dry mouth contribute to swelling under the tongue?
Yes, chronic dry mouth (xerostomia) significantly reduces salivary flow, which is a major risk factor for the formation of salivary stones and subsequent salivary gland infections (sialadenitis). These conditions are common causes of swelling under the tongue.
When to See a Dentist
Recognizing when to seek professional help is paramount for your health and safety.
See a Dentist/Doctor Immediately (Emergency Situations - Go to ER or call 911):
- Difficulty Breathing: Any sensation of shortness of breath, gasping, or noisy breathing.
- Difficulty Swallowing: Inability to swallow your own saliva, choking, or severe pain with swallowing.
- Rapidly Worsening Swelling: If the swelling is increasing quickly in size, especially over hours.
- High Fever and Chills: Especially when accompanied by severe pain or general malaise.
- Protruding Tongue: If the swelling pushes your tongue up or back, making it feel "too big" for your mouth.
- Inability to Open Your Mouth Fully (Trismus): May indicate a severe infection spreading to jaw muscles.
- Severe, Throbbing Pain: Especially if it's constant and not relieved by over-the-counter pain medication.
- Signs of Allergic Reaction: Swelling appearing suddenly after exposure to an allergen or new medication, especially if accompanied by hives or widespread itching.
Schedule an Appointment with Your Dentist Promptly (Within a Few Days):
- Persistent Swelling: Any swelling that lasts for more than a few days and doesn't improve.
- Intermittent Pain/Swelling During Meals: A classic sign of a salivary stone.
- Visible Lump or Sore: If you notice a growth, lump, or an ulcer that doesn't heal within 1-2 weeks.
- Pain or Tenderness: Even if mild, if it persists.
- Difficulty Speaking or Eating: If the swelling is mechanically interfering with these functions, even without severe pain.
- Foul Taste or Odor: May indicate an infection or pus drainage.
Routine Care/When to Mention at Your Next Check-up:
- Very small, painless, slow-growing lumps that have been present for a long time without changes (though still worth mentioning for documentation).
- Minor, transient swelling related to known benign conditions, but still requires a professional opinion to confirm the diagnosis.
Remember: When in doubt, it's always safer to consult a dental professional. Early diagnosis and intervention can prevent minor issues from becoming major, life-threatening emergencies. Your oral health is intricately linked to your overall health.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

How to Relieve Gum Swelling
When your gums are swollen, it can be an alarming and uncomfortable experience, often signaling an underlying issue that requires attention. Statistics from the Centers for Disease Control and Prevention (CDC) reveal that **nearly half of adults aged 30 or older in the United States have some form o
February 23, 2026

Teeth Swelling: Complete Guide
When you experience teeth swelling, it's more than just a minor discomfort; it's a clear signal from your body that something is amiss within your oral cavity, often indicating an underlying infection or inflammation that requires prompt attention. A recent survey revealed that **over 25% of adu
February 23, 2026

Submandibular Salivary Gland Swelling: Complete Guide
When you notice a peculiar lump or uncomfortable fullness beneath your jaw, it can be an alarming experience. This sensation, often accompanied by pain and difficulty swallowing, could indicate submandibular salivary gland swelling. Affecting an estimated 1 in 10,000 adults annually, conditi
February 23, 2026

What Helps With Gum Swelling
Gum swelling, medically known as gingival swelling or gingivitis, is a common yet often underestimated dental issue affecting millions of Americans. Have you ever woken up with sore, puffy gums that bleed easily when you brush? You're not alone. Research indicates that nearly **half of all a
February 23, 2026