Hand Foot and Mouth Symptoms: Complete Guide

Key Takeaways
- Imagine your child wakes up with a fever, feels a little off, and then you spot painful sores appearing in their mouth, followed by a tell-tale rash on their hands and feet. This scenario, unfortunately common, is often the first encounter with Hand Foot and Mouth Disease (HFMD). Affecting millions
Hand Foot and Mouth Symptoms: Complete Guide
Imagine your child wakes up with a fever, feels a little off, and then you spot painful sores appearing in their mouth, followed by a tell-tale rash on their hands and feet. This scenario, unfortunately common, is often the first encounter with Hand Foot and Mouth Disease (HFMD). Affecting millions of children and sometimes adults across the United States each year, particularly in summer and fall, understanding hand foot and mouth symptoms is crucial for prompt recognition, effective management, and preventing its spread. While often mild, HFMD can be distressing due to the discomfort it causes, especially the painful oral lesions that can make eating and drinking a challenge. This comprehensive guide will equip you with everything you need to know about HFMD, from its causes and diverse symptoms to available treatments, prevention strategies, and how to differentiate it from other oral conditions like a cold sore in mouth or oral lichen planus. We'll delve into the nuances of its presentation in children and adults, discuss potential complications, and provide practical advice to help you navigate this common viral illness.

Key Takeaways:
- Cause: Hand Foot and Mouth Disease (HFMD) is primarily caused by coxsackieviruses, a type of enterovirus, highly contagious among young children.
- Symptoms: Key hand foot and mouth symptoms include fever, sore throat, painful mouth sores (often appearing as small red spots turning into blisters/ulcers), and a distinctive non-itchy rash on the palms, soles, and sometimes buttocks.
- Contagion: HFMD is highly contagious, spreading through close contact, respiratory droplets, blister fluid, and fecal-oral routes. Contagiousness is highest during the first week but can persist for weeks.
- Duration: Symptoms typically resolve within 7-10 days. Most cases are mild and self-limiting, requiring only supportive care.
- Treatment: There is no specific cure; treatment focuses on managing symptoms with over-the-counter pain relievers (e.g., acetaminophen, ibuprofen), oral numbing gels, and ensuring adequate hydration.
- Cost: A typical doctor's visit for HFMD costs between $100-$300 without insurance, or a $50-$200 co-pay with insurance. Over-the-counter relief medications generally cost $5-$25.
- Prevention: Frequent handwashing, disinfecting contaminated surfaces, and avoiding close contact with infected individuals are key to prevention.
What is Hand Foot and Mouth Disease?
Hand Foot and Mouth Disease (HFMD) is a common, contagious viral infection characterized by sores in the mouth and a rash on the hands and feet. It primarily affects infants and children under the age of five, though older children and adults can also contract it. HFMD is generally a mild illness that resolves on its own, but the associated discomfort, particularly from the mouth sores, can be significant.
The disease is named for the distinctive pattern of its rash and lesions. While the name might sound alarming, it is distinct from foot-and-mouth disease (also known as hoof-and-mouth disease), which affects livestock and is not transmitted to humans.
Types / Variations of HFMD
HFMD is primarily caused by viruses belonging to the Enterovirus genus. The most common culprits in the United States are:
- Coxsackievirus A16: This strain is responsible for the majority of HFMD cases and typically causes a milder form of the illness.
- Enterovirus 71 (EV-A71): While less common, EV-A71 can lead to more severe complications, including neurological issues like viral meningitis or encephalitis, especially in some Asian countries. Cases in the US are generally milder, but this strain warrants closer monitoring.
- Coxsackievirus A6: This strain is often associated with atypical presentations of HFMD, which may involve a wider distribution of the rash (e.g., on the trunk, limbs, face) and more pronounced blistering, sometimes affecting the nails weeks after recovery (onychomadesis or nail shedding).
A related condition, Herpangina, is also caused by enteroviruses (often Coxsackievirus A). It primarily presents with painful sores and blisters confined to the back of the mouth, throat, and tonsils, usually without the characteristic hand and foot rash. While technically distinct, it is part of the spectrum of illnesses caused by these viruses.
Causes and Transmission
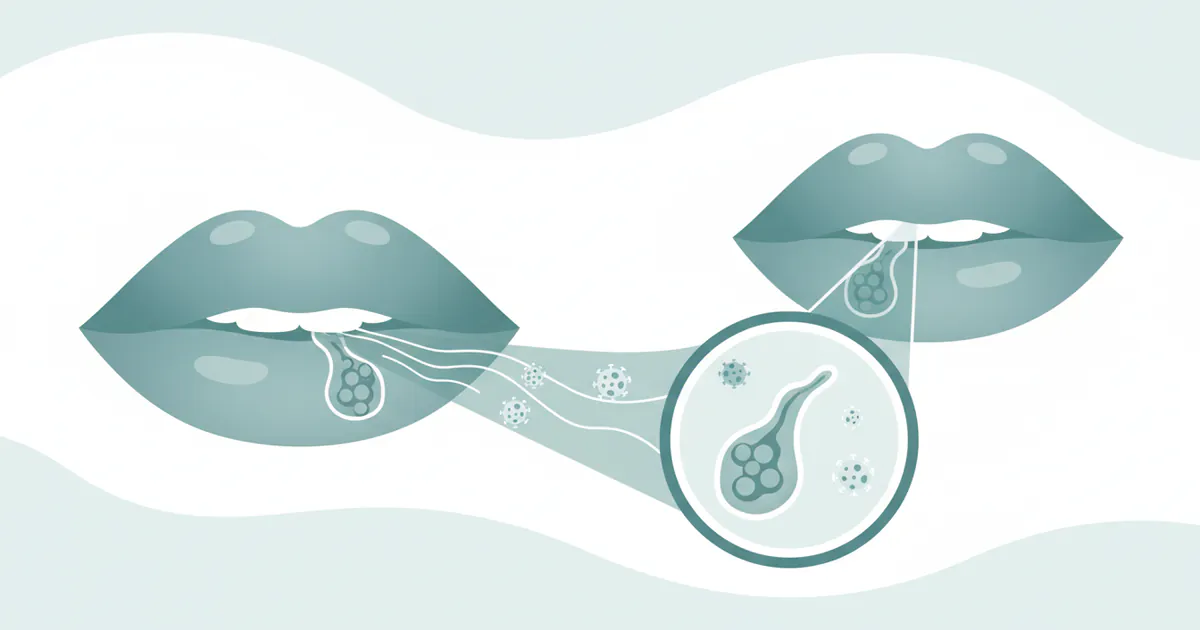
HFMD is highly contagious and spreads through direct contact with an infected person's:
- Nasal or throat secretions: This includes saliva, mucus, or sputum, especially when coughing or sneezing.
- Blister fluid: Contact with the fluid from the characteristic skin or oral blisters.
- Feces: The virus can be shed in stool for several weeks after symptoms resolve, making proper hand hygiene critical.
The fecal-oral route is particularly common in young children, who may not have fully developed toilet training or handwashing habits. Contaminated surfaces and objects (e.g., toys, doorknobs) also play a significant role in transmission, especially in crowded environments like daycares, preschools, and schools.
Contributing Factors:
- Age: Infants and children under five years old are most susceptible due to their developing immune systems and frequent close contact in group settings.
- Seasonality: Outbreaks are most common in the summer and early fall in temperate climates.
- Immunity: Once a person has been infected with a specific strain of enterovirus causing HFMD, they typically develop immunity to that strain. However, they can still get HFMD again from different strains of the virus.
Hand Foot and Mouth Symptoms: What to Look For
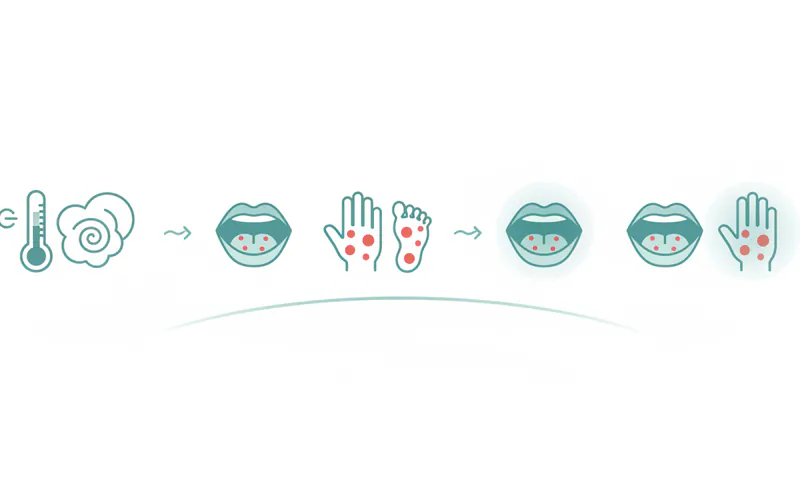
Recognizing hand foot and mouth symptoms early is key to managing the illness and preventing its spread. The incubation period (the time from exposure to symptom onset) is typically 3 to 7 days. Symptoms usually appear in stages:
Initial Symptoms (Prodromal Stage)
The illness often begins with general, non-specific symptoms that can mimic a common cold:
- Fever: Often low-grade (around 100°F-101°F / 38°C), but can sometimes be higher, especially in children.
- Sore Throat: Aching or scratchy throat, making swallowing uncomfortable.
- Malaise: A general feeling of being unwell, tired, or rundown.
- Loss of Appetite: Reduced desire to eat or drink due to discomfort or general illness.
- Irritability: Particularly noticeable in infants and young children.
These initial symptoms usually last for 1-2 days before the more distinctive signs appear.
Oral Symptoms (Enanthem)
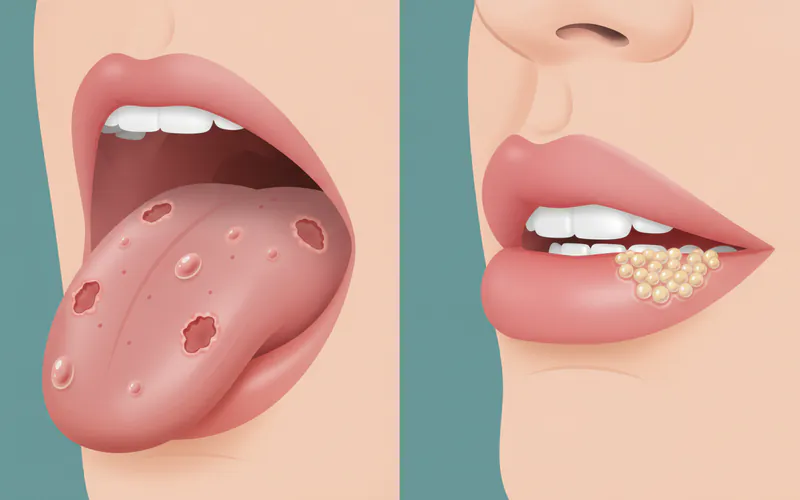
Within a day or two of the initial symptoms, painful sores develop in the mouth and throat. These are a hallmark of HFMD and can be the most distressing symptom, particularly for young children who may refuse to eat or drink.
- Appearance: The sores typically begin as small, red spots that quickly develop into tiny blisters (vesicles). These blisters then rupture, forming shallow, painful ulcers with a red base.
- Location: Common sites include the tongue, gums, inner cheeks (buccal mucosa), roof of the mouth (palate), and the back of the throat/tonsils.
- Pain: The oral sores are often intensely painful, leading to difficulty swallowing (dysphagia), drooling (especially in toddlers), and a general reluctance to eat or drink. This pain is the primary cause of dehydration in children with HFMD.
Pro Tip: For older children and adults, saltwater rinses (1/2 teaspoon salt in 8 ounces warm water) can help soothe mouth sores and promote healing.
It's important to differentiate these from other oral lesions:
- Cold Sore in Mouth: A cold sore in mouth (herpes labialis or oral herpes) is caused by the Herpes Simplex Virus (HSV-1). Unlike HFMD sores, cold sores typically appear as a cluster of small, fluid-filled blisters, usually on or around the lips, but can occasionally occur inside the mouth, particularly on the gums or hard palate. They tend to recur in the same location and are often preceded by a tingling or itching sensation. HFMD oral sores are more widespread throughout the mouth and throat, and are not recurrent in the same way.
- Oral Lichen Planus: Oral lichen planus is a chronic inflammatory condition, not an infection, that affects mucous membranes inside the mouth. It typically presents as white, lacy-patterned lesions (Wickham's striae), red inflamed patches, or open sores (erosive type). It's usually found on the inner cheeks, tongue, and gums, and can be painful. It is not contagious and has a completely different appearance and underlying cause than HFMD sores.
Skin Rash Symptoms (Exanthem)
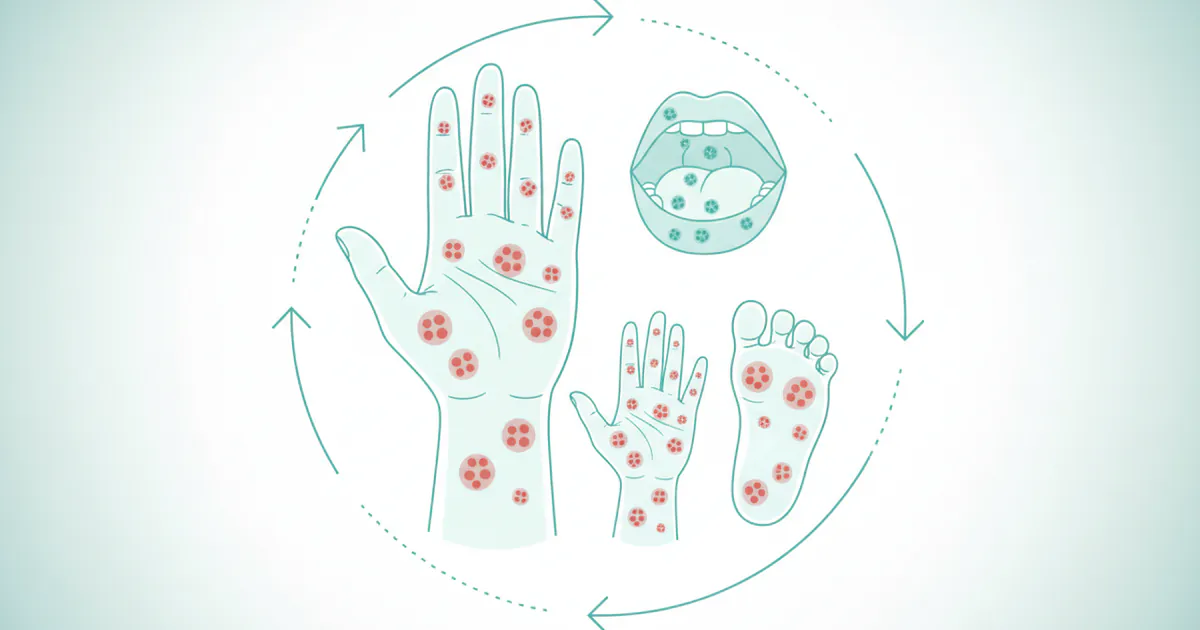
Concurrently with or shortly after the oral sores appear, a characteristic skin rash develops.
- Appearance: The rash starts as small, flat, red spots (macules) or slightly raised bumps (papules). Within a few hours, these can evolve into small, fluid-filled blisters (vesicles) that are typically grayish and oval-shaped.
- Location: The rash primarily affects the palms of the hands and the soles of the feet. It can also appear on the buttocks, knees, elbows, and sometimes on the torso or face (especially with atypical HFMD caused by Coxsackievirus A6).
- Itchiness: Unlike chickenpox, the HFMD rash is usually not itchy. However, some individuals, especially with Coxsackievirus A6 strains, may experience mild itching.
- Pain: The lesions on the hands and feet can sometimes be tender or painful, particularly if they are under pressure.
Less Common Symptoms
- Nail Changes (Onychomadesis): Several weeks (typically 1-2 months) after recovering from HFMD, some children may experience temporary shedding of fingernails or toenails. This is usually benign and painless, with new nails growing back naturally. It's more common with Coxsackievirus A6 infections.
- Dehydration: Due to painful mouth sores, children may refuse to drink, leading to dehydration. Signs include reduced urination, dry mouth, lack of tears, and lethargy. This is the most common serious complication.
- Neurological Complications: While rare in the US, severe neurological complications such as viral meningitis (inflammation of the membranes surrounding the brain and spinal cord) or encephalitis (inflammation of the brain) can occur, particularly with EV-A71 infections. Symptoms include severe headache, stiff neck, confusion, seizures, or weakness.
Symptom Timeline for HFMD
| Stage | Typical Duration | Key Characteristics |
|---|---|---|
| Incubation | 3-7 days | No symptoms; virus is replicating. |
| Prodromal | 1-2 days | Low-grade fever, sore throat, malaise, loss of appetite, irritability. |
| Active Illness | 7-10 days | Oral sores develop (red spots to painful ulcers); skin rash appears on hands, feet, sometimes buttocks/other areas. |
| Resolution | Within 10 days | Oral sores heal; skin rash fades, may leave temporary discoloration. Full recovery. |
| Post-Recovery | Weeks (occasional) | Nail shedding (onychomadesis) may occur 1-2 months after initial symptoms, typically harmless and temporary. |
Diagnosis of HFMD
Diagnosis of HFMD is typically clinical, meaning a healthcare provider identifies the condition based on the characteristic hand foot and mouth symptoms and a physical examination.
- Medical History: The doctor will ask about recent exposures, the onset of symptoms, and the progression of the illness.
- Physical Examination: The presence of fever, examination of the mouth for characteristic ulcers, and inspection of the hands, feet, and potentially buttocks for the rash are usually sufficient for diagnosis.
Lab tests (e.g., viral cultures or PCR tests from throat swabs or stool samples) are generally not necessary for routine cases. They may be performed in severe cases, for hospitalized patients, or during public health investigations of outbreaks, especially to identify specific viral strains if complications are suspected.
Treatment Options
There is no specific antiviral medication or cure for HFMD. Treatment is supportive, focusing on relieving symptoms and ensuring comfort while the body fights off the infection.
Supportive Care
- Pain Relief:
- Over-the-counter pain relievers: Acetaminophen (Tylenol) or ibuprofen (Advil, Motrin) can help reduce fever and alleviate pain from mouth sores and general body aches. Always follow dosage instructions based on age and weight.
- Topical oral anesthetics: Gels, sprays, or rinses containing ingredients like lidocaine or benzocaine (e.g., Orajel, liquid antacids like Maalox/Mylanta mixed with diphenhydramine) can temporarily numb painful mouth sores, making it easier to eat and drink. Consult a healthcare provider before using these, especially in young children.
- Hydration: Preventing dehydration is paramount, especially in children with painful mouth sores.
- Offer plenty of fluids: Water, diluted juices, oral rehydration solutions (Pedialyte).
- Cold liquids, popsicles, and ice chips can be soothing.
- Avoid acidic or spicy foods and drinks, which can irritate mouth sores.
- Rest: Ensure the patient gets plenty of rest to help their body recover.
Home Remedies & Comfort Measures
Beyond medical support, several home remedies can provide comfort:
- Soft, Bland Foods: Offer soft, easy-to-swallow foods like yogurt, applesauce, mashed potatoes, gelatin, and smoothies. Avoid crunchy, salty, spicy, or acidic foods.
- Cold Foods/Drinks: Ice cream, sherbet, and cold beverages can help soothe a sore mouth and throat.
- Saltwater Rinses: For older children and adults, rinsing the mouth several times a day with a warm saltwater solution (1/2 teaspoon of salt in 8 ounces of warm water) can help reduce inflammation and keep the mouth clean.
- Humidifier: A cool-mist humidifier in the bedroom can help soothe a sore throat and dry nasal passages.
Step-by-Step Recovery Process
The recovery from HFMD typically follows a predictable timeline:
- Initial Symptoms (Days 1-2): Fever, sore throat, and general malaise begin. These are often non-specific and might be mistaken for a common cold.
- Oral Sores Erupt (Days 2-3): Painful red spots appear in the mouth, quickly developing into blisters and then ulcers. This is often when eating and drinking become difficult.
- Rash Development (Days 2-4): The characteristic rash appears on the hands and feet, and sometimes other areas. It starts as red spots that may turn into small, grayish blisters.
- Symptom Peak (Days 3-5): Pain from mouth sores and discomfort from the rash are usually at their worst during this period. Fever may persist or fluctuate.
- Healing Phase (Days 5-10): Oral sores typically begin to heal and fade within a week. The skin rash gradually dries up and disappears. The total duration of active illness is usually 7 to 10 days.
- Post-Recovery (Weeks 1-8): In some cases, nail changes (loss or ridging) may occur weeks after full recovery, particularly following infection with Coxsackievirus A6. This is temporary and resolves as new nails grow.
Cost and Insurance
The cost associated with HFMD is generally manageable, as most cases require only supportive care. However, expenses can arise from doctor visits and over-the-counter medications.

- Doctor's Visit:
- With Insurance: A co-pay for a primary care physician (PCP) or pediatrician visit typically ranges from $20 to $75. An urgent care center visit might have a higher co-pay, often $50 to $150.
- Without Insurance: The cost for an office visit can range from $100 to $300 for a PCP or pediatrician, and $150 to $350 for an urgent care visit.
- Emergency Room: For severe complications (e.g., dehydration requiring IV fluids, suspected meningitis), an emergency room visit can be significantly more expensive, ranging from $500 to $3,000+, depending on the facility and services rendered, even with insurance.
- Over-the-Counter Medications:
- Acetaminophen or Ibuprofen: $5 to $15 per bottle.
- Oral numbing gels/sprays: $8 to $25 per tube/bottle.
- Oral rehydration solutions (e.g., Pedialyte): $5 to $15 per bottle.
Insurance Coverage: Most private health insurance plans, as well as Medicaid and CHIP (Children's Health Insurance Program), will cover necessary doctor visits and emergency care for HFMD-related complications. Over-the-counter medications are typically out-of-pocket expenses. Always check with your specific insurance provider for details on your coverage.
Cost Comparison Table: Common Oral Conditions
This table compares estimated typical costs for initial consultation and basic treatment for HFMD versus other oral conditions that might cause similar symptoms or concerns.
| Condition | Initial Consultation (No Insurance) | Initial Consultation (With Insurance Co-pay) | Basic Treatment Costs (OTC/Prescription) | Notes |
|---|---|---|---|---|
| Hand Foot and Mouth Disease | $100 - $300 (PCP/Urgent Care) | $20 - $150 (PCP/Urgent Care) | $5 - $25 (OTC pain relievers, oral gels) | Primarily supportive care. Severe complications requiring ER/hospitalization could cost $500-$3,000+. |
| Cold Sore in Mouth | $100 - $250 (PCP/Dentist) | $20 - $75 (PCP/Dentist) | $15 - $60 (OTC creams, prescription antivirals) | Often self-diagnosed and treated with OTCs. Prescription antivirals (e.g., acyclovir) have higher costs but can reduce duration. |
| Oral Lichen Planus | $150 - $400 (Dentist/Oral Pathologist) | $30 - $100 (Specialist co-pay) | $50 - $200+ (Prescription steroids, immunomodulators) | Requires specialist diagnosis (biopsy may be needed: $300-$800). Treatment is ongoing for chronic management. Costs vary widely based on medication and severity. |
Recovery and Aftercare
After the acute symptoms of HFMD subside, focus shifts to ensuring complete recovery and preventing further spread.
- Continued Hydration: Even as mouth sores heal, encourage continued fluid intake to ensure full rehydration.
- Monitor for Complications: Watch for any signs of lingering illness or rare complications, especially dehydration or neurological symptoms if severe.
- Return to Activities: Children can typically return to daycare or school once their fever has subsided for 24 hours (without fever-reducing medication) and they are feeling well enough to participate. Mouth sores and rashes are generally not a reason to exclude a child if they are otherwise well, though some institutions may have stricter policies. Check with your child's daycare or school.
- Hygiene: Reinforce diligent handwashing and hygiene practices, as the virus can still be shed in stool for several weeks.
Prevention
Preventing the spread of HFMD is crucial, especially in childcare settings and homes.
- Frequent Handwashing: This is the most effective preventive measure. Wash hands thoroughly with soap and water for at least 20 seconds, especially after using the toilet, changing diapers, before eating, and after coughing or sneezing.
- Disinfection of Surfaces: Regularly clean and disinfect frequently touched surfaces and shared items (e.g., toys, doorknobs, countertops) using a bleach solution (1 tablespoon bleach per quart of water) or a commercial disinfectant.
- Avoid Close Contact: Limit close contact (kissing, hugging, sharing eating utensils) with individuals who have HFMD.
- Teach Good Hygiene: Educate children on proper handwashing techniques and the importance of not touching their faces, especially their mouth and nose.
- Stay Home When Sick: Infected individuals, especially children, should stay home from school or daycare to prevent spreading the virus to others.
Pro Tip: Always use separate towels and drinking glasses for individuals who are sick to minimize viral transmission within the household.
Risks and Complications
While HFMD is usually a mild and self-limiting illness, some risks and complications can arise:
- Dehydration: This is the most common complication, particularly in infants and young children who refuse to drink due to painful mouth sores. Severe dehydration may require intravenous (IV) fluids in a hospital setting.
- Nail Changes (Onychomadesis): Temporary shedding of fingernails and toenails 1-2 months after the infection, more common with certain viral strains (e.g., Coxsackievirus A6). The nails regrow without intervention.
- Secondary Bacterial Infections: Open sores (especially if scratched) can become infected with bacteria, requiring antibiotic treatment.
- Neurological Complications: Although rare in the US, certain strains of enterovirus, particularly EV-A71, can lead to serious neurological complications:
- Viral Meningitis: Inflammation of the membranes surrounding the brain and spinal cord. Symptoms include severe headache, stiff neck, fever, and sensitivity to light.
- Encephalitis: Inflammation of the brain, a more severe and potentially life-threatening condition. Symptoms include confusion, seizures, weakness, or paralysis.
- Polio-like Paralysis: Extremely rare but observed with some enterovirus strains.
- Myocarditis: Very rarely, the virus can affect the heart muscle, leading to inflammation (myocarditis).
Comparison of Oral Lesions: HFMD, Cold Sores, and Oral Lichen Planus
Differentiating between various oral conditions is essential for accurate diagnosis and appropriate management. Here's a detailed comparison of Hand Foot and Mouth oral lesions, cold sores, and oral lichen planus.
| Feature | Hand Foot and Mouth Disease (HFMD) | Cold Sore (Herpes Labialis/Oral Herpes) | Oral Lichen Planus (OLP) |
|---|---|---|---|
| Cause | Enteroviruses (e.g., Coxsackievirus A16, EV-A71, A6) | Herpes Simplex Virus Type 1 (HSV-1) | Chronic inflammatory condition, autoimmune-like response (not infectious) |
| Appearance | Small, red spots that quickly become fluid-filled blisters (1-5mm) and then shallow, painful ulcers with a red base. | Clusters of small, clear, fluid-filled blisters (vesicles) that rupture, crust over, and heal. Sometimes larger ulcer. | White, lacy-patterned lesions (Wickham's striae), red inflamed patches, or painful open sores (erosive OLP). |
| Location | Widespread in mouth: Tongue, gums, inner cheeks, hard palate, soft palate, back of throat/tonsils. | Typically on or around the lips, but can appear on gums, hard palate, and sometimes inside the mouth (less common). | Inner cheeks (buccal mucosa) most common, also tongue, gums, roof of mouth. Usually bilateral. |
| Pain Level | Often intensely painful, especially for eating/drinking. | Painful, tingling, burning sensation usually precedes eruption. | Varies from asymptomatic (lacy type) to severely painful and burning (erosive type), especially with spicy/acidic foods. |
| Duration | 7-10 days for oral lesions to heal. | 7-14 days for healing, often recurs. | Chronic condition; lesions can persist for weeks, months, or years, often with periods of flare-up and remission. |
| Contagiousness | Highly contagious, especially in the first week. Spreads through saliva, stool, blister fluid. | Highly contagious, especially when blisters are present. Spreads through direct contact with lesions. | Not contagious. |
| Associated Symptoms | Fever, sore throat, malaise, rash on hands/feet/buttocks, loss of appetite. | Prodromal tingling/itching, sometimes fever or muscle aches with primary infection. | Can affect skin, scalp, nails, genitals (similar lesions), but oral is most common. No systemic viral symptoms. |
| Treatment | Supportive: Pain relief (OTC), hydration, soft foods. No antiviral. | Antivirals (oral or topical), pain relief. | Steroid medications (topical, systemic), immunomodulators. Requires long-term management, no cure. |
Children / Pediatric Considerations
HFMD disproportionately affects young children, making pediatric considerations central to understanding and managing the disease.
- Age Group: Most cases occur in children under the age of 5, with infants and toddlers being particularly vulnerable due to their underdeveloped immune systems.
- Transmission in Group Settings: Daycares, preschools, and kindergartens are common sites for HFMD outbreaks due to close contact, shared toys, and challenges in maintaining strict hygiene among young children.
- Hydration Challenges: The intense pain from mouth sores can make infants and toddlers refuse to drink, leading to rapid dehydration. Parents must diligently monitor for signs of dehydration (e.g., fewer wet diapers, dry mouth, sunken fontanelle in infants, lethargy).
- Communication Barriers: Young children cannot articulate their pain levels or specific symptoms, making it harder for parents to assess their discomfort. Increased irritability, crying, and refusal to eat/drink are key indicators.
- Comfort Measures: Offer cold foods and liquids (popsicles, ice cream, cold milk/formula), soft pureed foods. Acetaminophen or ibuprofen should be given according to age/weight guidelines to manage fever and pain.
- When to Seek Medical Care: While most HFMD cases are mild, parents should contact their pediatrician if:
- The child is not drinking fluids and shows signs of dehydration.
- Fever is high (over 102°F or 39°C) or lasts longer than 3 days.
- Symptoms worsen or don't improve after 7-10 days.
- The child is very young (under 6 months) or has a weakened immune system.
- Any signs of neurological complications appear (e.g., severe headache, stiff neck, extreme drowsiness, unusual irritability, confusion, seizures).
Cost Breakdown
A dedicated cost breakdown reinforces the financial aspects for readers.
- Typical Office Visit (Pediatrician/PCP):
- Without Insurance: $100 - $300
- With Insurance Co-pay: $20 - $75
- Urgent Care Visit:
- Without Insurance: $150 - $350
- With Insurance Co-pay: $50 - $150
- Emergency Room Visit (for severe complications like dehydration, meningitis):
- Without Insurance: $500 - $3,000+
- With Insurance Co-pay/Deductible: Varies widely, potentially $100 - $1,000+ out-of-pocket depending on plan and services.
- Over-the-Counter Medications & Supplies:
- Fever/Pain Reducers (Acetaminophen/Ibuprofen): $5 - $15
- Oral Numbing Gels/Sprays: $8 - $25
- Oral Rehydration Solutions: $5 - $15 per bottle
- Total OTC cost: $20 - $55 for a basic selection.
Payment Plans and Financing Options: For rare but severe complications requiring hospitalization, facilities often offer payment plans. Additionally, healthcare financing companies (e.g., CareCredit) can help cover larger medical bills, allowing patients to pay in installments.
Cost-Saving Tips:
- Preventative Hygiene: Diligent handwashing and disinfection are the best cost-savers, preventing the illness in the first place.
- Early Recognition & Home Care: For mild cases, early recognition of hand foot and mouth symptoms and prompt supportive care at home (OTC meds, hydration) can often prevent the need for a doctor's visit.
- Choose Appropriate Care: For non-emergency situations, opt for a pediatrician/PCP or urgent care clinic over an emergency room, which has significantly higher costs.
- Generic Medications: Choose generic brands for over-the-counter pain relievers, which are equally effective and less expensive.
Frequently Asked Questions
Is Hand Foot and Mouth contagious?
Yes, HFMD is highly contagious. It spreads through close personal contact, coughing and sneezing (respiratory droplets), contact with blister fluid, and contact with an infected person's feces. It is most contagious during the first week of illness but can be shed in stool for several weeks after symptoms resolve.
How long does Hand Foot and Mouth disease last?
Most cases of HFMD are mild and resolve on their own within 7 to 10 days from the onset of symptoms. The fever usually subsides within 2-3 days, and the mouth sores and rash typically heal within a week.
Can adults get Hand Foot and Mouth disease?
Yes, adults can definitely get HFMD, though it is more common in children. Adults often experience milder symptoms, but some can have more severe or prolonged illness, including intense pain from mouth sores. Previous exposure to a specific strain may provide immunity, but you can still get infected by a different strain.
What are the best home remedies for Hand Foot and Mouth mouth sores?
To relieve painful mouth sores, offer cold liquids like water, diluted juice, or popsicles. Soft, bland foods like yogurt, applesauce, and mashed potatoes are easier to eat. Avoid acidic, spicy, or salty foods. Over-the-counter pain relievers (acetaminophen/ibuprofen) and topical oral numbing gels can also provide relief. For older children and adults, warm saltwater rinses can be soothing.
When should I take my child to the doctor for Hand Foot and Mouth?
You should contact your pediatrician if your child is not drinking fluids and shows signs of dehydration (e.g., decreased urination, dry mouth), has a high fever (over 102°F/39°C) or fever lasting more than 3 days, seems unusually sleepy or irritable, or if symptoms worsen or don't improve after 10 days. Any signs of severe headache, stiff neck, or confusion warrant immediate medical attention.
Is there a vaccine for Hand Foot and Mouth?
Currently, there is no vaccine available in the United States to prevent HFMD. Vaccines are under development, especially for Enterovirus 71 (EV-A71), which causes more severe disease in some regions, but these are not yet widely available in the US.
Can HFMD cause long-term problems?
For the vast majority of people, HFMD is a mild illness with no long-term problems. Rare complications like temporary nail shedding are benign. Serious neurological complications (meningitis, encephalitis) are very rare, especially in the US, and usually resolve without lasting effects, though severe cases can have long-term impacts.
How is Hand Foot and Mouth different from cold sores?
HFMD is caused by enteroviruses and typically presents with widespread painful mouth sores (ulcers) and a rash on the hands and feet. A cold sore in mouth is caused by the Herpes Simplex Virus (HSV-1), usually appears as a localized cluster of blisters (vesicles) on or around the lips, and often recurs in the same spot. Cold sores typically don't cause a rash on the hands and feet.
What about Hand Foot and Mouth in pregnant women?
Pregnant women can contract HFMD, and generally, the illness is mild. There is no clear evidence that HFMD causes serious problems for the pregnant woman or her baby. However, if a pregnant woman contracts HFMD shortly before delivery, there's a small risk that the virus could be passed to the newborn. Always consult with your obstetrician if you develop symptoms during pregnancy.
When to See a Dentist
While Hand Foot and Mouth Disease is primarily a medical condition managed by a physician or pediatrician, a dentist might be involved in certain situations, especially concerning oral health.
- Persistent Oral Lesions: If mouth sores don't heal within the typical 7-10 day timeframe, or if they worsen, a dentist can help rule out secondary infections or other oral conditions.
- Atypical Oral Lesions: If the mouth sores look unusual or are accompanied by symptoms that don't fit the typical HFMD pattern (e.g., white lacy patterns indicative of oral lichen planus, or recurrent localized blisters suggesting a severe cold sore in mouth), a dental professional, particularly an oral pathologist, can provide a definitive diagnosis.
- Severe Oral Pain: If the pain from mouth sores is so severe that it prevents adequate hydration, a dentist can help assess the severity and potentially prescribe stronger topical pain relief options or recommend a referral to a physician if systemic support is needed.
- Dental Complications: While rare, if secondary bacterial infections develop in the mouth or if the oral lesions seem to affect dental structures (e.g., severe gum inflammation that persists), a dentist's evaluation is warranted.
- Differentiation from Other Oral Conditions: If you suspect a diagnosis other than HFMD, such as a severe outbreak of cold sores or the chronic issues of oral lichen planus, a dental examination is appropriate. Dentists are trained to distinguish between various oral pathologies and can provide targeted treatment or specialist referrals.
Red Flags for Immediate Medical Attention (Physician/ER, not Dentist):
- Signs of Dehydration: Decreased urination, sunken eyes, dry mouth, no tears, lethargy, or extreme fussiness (especially in children).
- High or Persistent Fever: Fever over 102°F (39°C) that doesn't respond to medication, or lasts more than 3 days.
- Neurological Symptoms: Severe headache, stiff neck, extreme drowsiness, confusion, unusual irritability, sensitivity to light, or seizures.
- Difficulty Breathing.
- Weakened Immune System: Individuals with compromised immune systems should see a doctor for any signs of infection.
For routine HFMD cases, managing symptoms at home with over-the-counter medications and ensuring hydration is usually sufficient. However, never hesitate to consult a healthcare professional if you have concerns about the severity of symptoms or the possibility of complications.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Oral Candidiasis Symptoms: Complete Guide
Oral candidiasis, commonly known as oral thrush, is a fungal infection of the mouth caused by an overgrowth of Candida yeast, most often Candida albicans. While Candida is a normal inhabitant of the human mouth in small amounts, an imbalance can lead to uncomfortable and sometimes painful symptoms
February 23, 2026
Are Cold Sores Contagious
In the United States, an estimated 67% of the population under age 50 carries the herpes simplex virus type 1 (HSV-1), the primary cause of cold sores. This means millions of Americans are susceptible to these often painful and highly visible oral lesions. Beyond the discomfort and cosmetic conc
February 23, 2026
How Long Does Hand Foot and Mouth Last
Hand, Foot, and Mouth Disease (HFMD) is a common, often uncomfortable, viral illness that can affect anyone but is particularly prevalent among young children. If you or a loved one has ever experienced the tell-tale rash or painful mouth sores, you've likely wondered: **how long does Hand Foot and
February 23, 2026
Cold Sore vs Pimple on Lip: Complete Comparison Guide
When you notice an unexpected bump or lesion on your lip, your mind might immediately jump to questions of what it is, how long it will last, and most importantly, if it's contagious. The confusion between a cold sore vs pimple on lip is incredibly common, yet the distinction is crucial for prop
February 23, 2026