How Long Does Hand Foot and Mouth Last
Key Takeaways
- Hand, Foot, and Mouth Disease (HFMD) is a common, often uncomfortable, viral illness that can affect anyone but is particularly prevalent among young children. If you or a loved one has ever experienced the tell-tale rash or painful mouth sores, you've likely wondered: **how long does Hand Foot and
Hand, Foot, and Mouth Disease (HFMD) is a common, often uncomfortable, viral illness that can affect anyone but is particularly prevalent among young children. If you or a loved one has ever experienced the tell-tale rash or painful mouth sores, you've likely wondered: how long does Hand Foot and Mouth last? The answer isn't a simple fixed number, as its duration can vary based on individual factors, the specific virus strain, and the severity of symptoms. Understanding the typical timeline, symptoms, and care strategies is crucial for managing the illness effectively and minimizing discomfort. This comprehensive guide will delve into the intricacies of HFMD, exploring its causes, symptoms, treatment options, prevention strategies, and what you can expect during the course of the infection, helping you navigate this viral challenge with confidence and clarity.
Key Takeaways:
- Typical Duration: Hand, Foot, and Mouth Disease (HFMD) generally resolves within 7 to 10 days from the onset of symptoms, though some severe cases or specific viral strains might extend symptoms slightly.
- Initial Symptoms: Fever, sore throat, and malaise usually appear 3-7 days after exposure and last for 2-3 days before the characteristic rash develops.
- Rash and Sores: Painful mouth sores (herpangina) and rashes on hands and feet typically emerge 1-2 days after fever and resolve within 7-10 days.
- Contagious Period: Individuals are most contagious during the first week of illness but can shed the virus for several weeks (feces) or even months (saliva), even after symptoms disappear.
- No Specific Cure: Treatment is primarily supportive, focusing on managing pain, fever, and ensuring hydration. Over-the-counter medications like ibuprofen or acetaminophen, alongside oral rinses, are common.
- Cost of Care: A typical doctor's visit for HFMD ranges from $75 to $250 without insurance, plus costs for OTC medications (under $30). Severe cases requiring ER visits could range from $500 to $3,000+.
- Prevention: Frequent handwashing, disinfecting contaminated surfaces, and avoiding close contact with infected individuals are key to preventing the spread.
What Is Hand, Foot, and Mouth Disease (HFMD)?
Hand, Foot, and Mouth Disease (HFMD) is a common infectious disease caused by viruses, most commonly belonging to the Enterovirus genus. It's characterized by a distinct rash with small, blister-like lesions on the hands and feet, often accompanied by painful sores in the mouth and throat. While it can affect people of any age, infants and children under the age of five are most susceptible due to their developing immune systems and common close-contact environments like daycares and schools.
Despite its somewhat alarming name, HFMD is generally a mild illness that resolves on its own. However, the discomfort caused by the oral sores can be significant, leading to dehydration, especially in young children who refuse to eat or drink. It's a highly contagious condition, spreading easily through direct contact with an infected person's saliva, blister fluid, or stool. Understanding the nature of this virus is the first step in managing its impact on health and daily life.
Types of Viruses Causing HFMD
HFMD is primarily caused by several strains of enteroviruses. The most common culprits include:
Coxsackievirus A16
Historically, Coxsackievirus A16 has been the predominant cause of HFMD in the United States. Infections with this strain typically result in a milder form of the disease with a rapid recovery time, generally aligning with the typical 7-10 day duration.
Enterovirus 71 (EV-A71)
Enterovirus 71 (EV-A71) is another significant cause, often associated with more severe outbreaks, particularly in East and Southeast Asia. EV-A71 infections can sometimes lead to neurological complications such as encephalitis, meningitis, or acute flaccid paralysis, though this is rare in Western countries. The symptoms might be more pronounced, and recovery could potentially take slightly longer than with Coxsackievirus A16, sometimes extending beyond the 10-day mark in complicated cases.
Other Enteroviruses
Other enterovirus strains, such as Coxsackievirus A6 and Coxsackievirus A10, can also cause HFMD. Coxsackievirus A6, in particular, has been linked to cases with a more widespread rash, sometimes affecting areas beyond the hands, feet, and mouth, such as the arms, legs, and even the torso. These cases may also be accompanied by more pronounced skin peeling on the fingers and toes during recovery, known as desquamation, which can occur weeks after the initial symptoms subside. The duration of acute symptoms, however, still typically falls within the 7-10 day window.
The specific type of virus influencing the duration of Hand, Foot, and Mouth symptoms largely relates to the severity of the initial infection and the potential for complications. While most cases remain mild and self-limiting, understanding the different viral types helps medical professionals predict potential outcomes and advise on care.
Causes: Why Hand, Foot, and Mouth Disease Happens
HFMD is a highly contagious viral infection that spreads through person-to-person contact. The primary modes of transmission involve fluids and excretions from an infected individual.
Viral Transmission Routes
- Direct Contact with Nasal and Throat Secretions: This includes saliva, sputum, or mucus from the nose. Sneezing, coughing, or talking can release virus-laden droplets into the air, which can then be inhaled or land on surfaces.
- Direct Contact with Blister Fluid: The fluid within the characteristic blisters on the hands, feet, and mouth is highly contagious. If these blisters burst, the fluid can easily spread the virus.
- Direct Contact with Feces: The virus is present in the stool of an infected person, often for several weeks or even months after symptoms resolve. This is a significant route of transmission, particularly in childcare settings where diaper changes are frequent and hand hygiene may not be meticulously followed.
- Contaminated Objects and Surfaces: The virus can survive on inanimate objects like toys, doorknobs, and countertops for several days. Touching these contaminated surfaces and then touching one's eyes, nose, or mouth can lead to infection.
Risk Factors
While anyone can contract HFMD, certain factors increase the risk:
- Age: Infants and young children (under 5 years old) are most susceptible due to their developing immune systems and propensity for close physical contact in group settings.
- Childcare Settings: Daycares, preschools, and schools are common environments for HFMD outbreaks because children are in close quarters, share toys, and may not consistently practice good hand hygiene.
- Immunocompromised Individuals: People with weakened immune systems may be more vulnerable to infection and could potentially experience more severe symptoms or prolonged illness.
- Lack of Prior Exposure: Adults and older children who have not been exposed to the specific enterovirus strains causing HFMD lack immunity, making them susceptible. However, once infected with a particular strain, individuals typically develop immunity to that specific strain, reducing the likelihood of reinfection with the same virus but not against other strains.
Understanding these transmission routes and risk factors is crucial for implementing effective prevention strategies, particularly in high-risk environments.
Signs and Symptoms: What to Look For
The symptoms of Hand, Foot, and Mouth Disease typically progress in stages, offering clues about the infection's timeline. The incubation period, the time from exposure to the onset of symptoms, is usually 3 to 7 days.
Early Symptoms (Prodromal Stage)
The initial symptoms are often non-specific and can resemble a common cold or flu. These usually last for 1-2 days:
- Fever: Often the first sign, ranging from low-grade to moderate (typically 100°F to 102°F or 38°C to 39°C).
- Sore Throat: A prominent symptom, making swallowing difficult.
- Malaise: A general feeling of being unwell, tired, or achy.
- Irritability: Particularly noticeable in infants and young children.
- Loss of Appetite: Due to general unwellness and impending mouth sores.
Characteristic Rash and Sores
Following the initial prodromal stage, the hallmark symptoms of HFMD emerge, usually 1-2 days after the fever begins:
- Oral Sores (Herpangina):
- Small, red spots often appear at the back of the mouth, on the tongue, gums, and inside of the cheeks.
- These quickly develop into painful blisters that eventually ulcerate (open sores).
- The pain from these sores can be severe, making eating, drinking, and swallowing very difficult, leading to a risk of dehydration.
- Pro Tip: Look for refusal to eat or drink, excessive drooling (in children), or complaints of a sore throat.
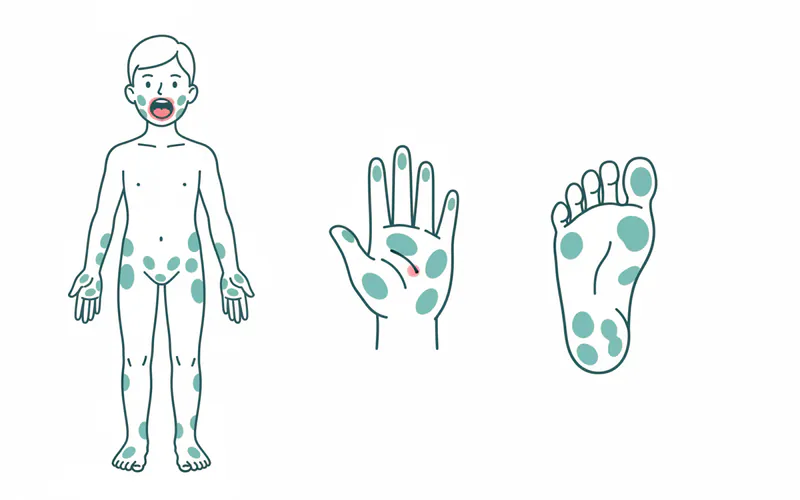
- Hand and Foot Rash:
- Flat, red spots (macules) or small, raised bumps (papules) appear on the palms of the hands and soles of the feet.
- These lesions may or may not blister. When they do, they are typically non-itchy but can be tender.
- The rash can sometimes extend to the buttocks, groin, knees, or elbows, especially with certain viral strains like Coxsackievirus A6.
- The rash usually fades within 7 to 10 days.
- Other Potential Symptoms:
- In some cases, children may experience diarrhea or vomiting.
- Nail changes: A rare but notable complication, especially with Coxsackievirus A6, involves temporary nail loss (onychomadesis) occurring weeks to months after the infection. New nails typically grow back without intervention.
The progression of symptoms, particularly the development and resolution of the oral sores and rash, is key to understanding how long Hand Foot and Mouth lasts. While the fever and initial malaise typically subside within a few days, the discomfort from the sores and rash often dictates the overall duration of the illness.
Treatment Options: Managing Discomfort
There is no specific antiviral treatment or cure for Hand, Foot, and Mouth Disease. Treatment is entirely supportive, focusing on relieving symptoms and ensuring comfort while the body's immune system fights off the virus. The primary goals are pain management, fever reduction, and prevention of dehydration.
Over-the-Counter Medications
- Pain Relievers and Fever Reducers:
- Acetaminophen (Tylenol): Effective for fever and pain.
- Ibuprofen (Advil, Motrin): Also effective for fever, pain, and inflammation.
- Pros: Readily available, generally safe, and effective for symptom relief.
- Cons: Must be dosed correctly, especially for children; ibuprofen should not be given to infants under 6 months. Aspirin should NEVER be given to children or teenagers with viral infections due to the risk of Reye's syndrome.
- Topical Oral Anesthetics:
- Over-the-counter oral gels or sprays containing ingredients like benzocaine can temporarily numb painful mouth sores.
- Pros: Provides localized relief, allowing for easier eating/drinking.
- Cons: Temporary effect, not suitable for very young children due to choking risk or potential for methemoglobinemia with excessive benzocaine use; use sparingly and under medical guidance.
Home Care Strategies
- Hydration is Key:
- Offer plenty of fluids to prevent dehydration, especially crucial for children with painful mouth sores who may refuse to drink.
- Cold liquids such as water, milk, or diluted fruit juices (avoid acidic juices like orange or grapefruit, which can irritate sores).
- Popsicles, ice chips, or gelatin can be soothing and provide hydration.
- Pros: Directly addresses the most serious complication of HFMD (dehydration).
- Cons: Can be challenging if pain is severe; consistency is vital.
- Soft Food Diet:
- Offer soft, bland foods that are easy to chew and swallow.
- Examples include yogurt, applesauce, mashed potatoes, well-cooked pasta, scrambled eggs, and cold pureed fruits.
- Avoid spicy, salty, acidic, or crunchy foods that can irritate mouth sores.
- Pros: Reduces pain during eating, maintains nutritional intake.
- Cons: May require creativity to ensure adequate nutrition; children might still refuse food.
- Oral Hygiene:
- Gentle oral care is important. Rinsing the mouth with warm salt water (for older children and adults) can help soothe sores and keep the mouth clean.
- Pro Tip: For young children, ensure pacifiers, bottles, and toys are cleaned frequently.
- Pros: Promotes healing and comfort.
- Cons: Can be painful initially; ensure solutions are not swallowed.
- Rest:
- Ample rest helps the body conserve energy to fight the viral infection.
- Pros: Supports immune function.
- Cons: Active children may resist rest, but encourage quiet activities.
- Soothing Skin Rash:
- While the rash is generally not itchy, some individuals might find mild relief from cool compresses or soothing lotions.
- Pros: Can alleviate minor discomfort.
- Cons: Not a primary concern for most HFMD rashes.
When Medical Intervention Might Be Needed
While most cases are mild and resolve with home care, a doctor should be consulted if:
- Symptoms worsen or do not improve after 10 days.
- Fever is very high or lasts longer than 3 days.
- Signs of dehydration appear (decreased urination, dry mouth, no tears).
- The child is very young (under 6 months) or immunocompromised.
- Signs of neurological complications develop (severe headache, stiff neck, seizures, disorientation).
Step-by-Step Process: What to Expect During HFMD
Understanding the typical progression of Hand, Foot, and Mouth Disease can help you anticipate symptoms and manage care effectively.
-
Exposure and Incubation (Days 0-7):
- The individual is exposed to the virus.
- No symptoms are present yet, but the virus is replicating internally.
- The typical incubation period is 3 to 7 days, but can range from 2 to 14 days.
-
Prodromal Stage (Days 7-9 or 1-2 days before rash):
- First symptoms appear: fever (often 100°F-102°F), sore throat, general malaise, loss of appetite, and irritability.
- These symptoms are non-specific and can be mistaken for a common cold.
- The individual is already contagious during this stage.
-
Oral Sores Emerge (Days 8-10 or Day 1-3 of rash):
- Small, red spots develop in the mouth, particularly on the tongue, gums, and inside cheeks.
- These rapidly turn into painful blisters, then open sores (ulcers). This stage is often the most uncomfortable due to pain with eating and drinking.
- The presence of these oral lesions is a key diagnostic feature.
-
Skin Rash Appears (Days 9-11 or Day 2-4 of rash):
- About 1-2 days after the fever starts and often coinciding with or shortly after the oral sores, the characteristic rash emerges.
- This typically appears as flat red spots or small, raised bumps on the palms of the hands and soles of the feet. It can also appear on the buttocks or other areas.
- These lesions may or may not blister but are generally non-itchy and can be tender.
-
Symptom Resolution (Days 11-17 or Day 4-10 of rash):
- Fever usually subsides within 2-3 days of its onset.
- Oral sores typically heal within 7-10 days from their appearance.
- The skin rash also fades and resolves within 7-10 days from its appearance.
- The most severe pain and discomfort usually peak in the first few days of the rash and then gradually diminish.
-
Full Recovery and Viral Shedding (Days 17+ or beyond 10 days post-onset):
- Most individuals are fully recovered within 7 to 10 days from the initial onset of symptoms.
- However, it's important to note that the virus can continue to be shed in stool for several weeks or even months after all visible symptoms have resolved, meaning individuals can still be contagious during this period, though less so than during acute illness. This prolonged shedding is why excellent hygiene practices remain important.
- In rare cases, nail shedding (onychomadesis) can occur weeks after recovery, with new nails growing back naturally.
This timeline illustrates that while the acute, most bothersome symptoms of HFMD typically last for about a week to ten days, the total duration from exposure to complete viral clearance can be much longer.

Cost and Insurance: Understanding the Financial Aspect of HFMD Care
While Hand, Foot, and Mouth Disease itself doesn't incur a direct "cost" for treatment beyond supportive care, managing the illness often involves expenses related to doctor visits, over-the-counter medications, and potentially lost work/school days. The costs can vary significantly based on your insurance coverage, location, and the severity of the illness.
Typical Costs Without Insurance (Out-of-Pocket)
- Primary Care Provider (PCP) Visit:
- Low: $75 (e.g., walk-in clinic, telehealth consultation in some areas)
- Mid: $150 - $250 (typical office visit)
- High: $300 - $400 (if extensive testing or procedures are mistakenly ordered, or for specialist consultation)
- Urgent Care Center Visit:
- Low: $100 - $200
- Mid: $250 - $350 (more common)
- High: $400 - $600 (if minor labs or procedures are done)
- Emergency Room (ER) Visit (for severe dehydration or complications):
- Low: $500 - $1,000 (for basic evaluation)
- Mid: $1,500 - $3,000 (if IV fluids, basic labs, or imaging are needed)
- High: $3,000 - $10,000+ (for extensive hospitalization, specialized care for neurological complications, though rare for HFMD).
- Over-the-Counter Medications:
- Pain relievers (acetaminophen/ibuprofen): $5 - $15 per bottle
- Oral numbing gels/sprays: $8 - $20 per tube/bottle
- Hydration solutions (pediatric electrolytes): $5 - $10 per box/bottle
- Total for OTCs: Typically $15 - $50.

Cost with Health Insurance
Most US health insurance plans, including PPOs, HMOs, and EPOs, cover medically necessary visits for infectious diseases like HFMD.
- Copayments: You will typically pay a copay for a doctor's visit, which can range from $15 - $50 for a PCP and $50 - $150 for urgent care. ER copays can be significantly higher, often $100 - $500.
- Deductibles: If you haven't met your annual deductible, you might be responsible for the full cost of the visit until the deductible is met. After that, your insurance will pay a percentage (e.g., 80%), and you'll pay the remaining coinsurance.
- Formularies: Most OTC medications are not covered by insurance, but if a doctor prescribes a stronger pain reliever or specific oral rinse, your prescription drug plan might cover a portion of it, subject to your copay or deductible.
- Out-of-Pocket Maximum: All costs you pay towards covered services (copays, deductibles, coinsurance) count towards your annual out-of-pocket maximum. Once this is met, your insurance typically covers 100% of further eligible medical expenses for the year.
Cost Comparison Table (US Averages)
| Service Type | Without Insurance (Avg. Range) | With Insurance (Avg. Copay/Cost) | Notes |
|---|---|---|---|
| PCP Office Visit | $150 - $250 | $20 - $50 | Initial diagnosis, mild cases |
| Urgent Care Visit | $250 - $350 | $50 - $150 | After-hours care, moderate symptoms |
| ER Visit | $1,500 - $3,000+ | $100 - $500+ (or deductible) | Severe dehydration, complications, high fever |
| OTC Medications | $15 - $50 | N/A (usually not covered) | Pain relievers, oral gels, hydration solutions |
| Prescription Meds (if any) | $20 - $100+ (full cost) | $10 - $30 (copay) | Stronger pain meds, specific mouth rinses |
Cost-Saving Tips
- Know Your Plan: Understand your insurance benefits, including copays, deductibles, and in-network providers, before you need care.
- Telehealth: Many insurance plans cover telehealth consultations for initial assessments, which can be less expensive than in-person visits and allow a doctor to determine if an in-person exam is necessary.
- Urgent Care vs. ER: For non-life-threatening conditions, choose an urgent care center over an emergency room to save significant costs.
- Generic Medications: Opt for generic versions of OTC medications, which are just as effective but much cheaper.
- Preventative Measures: Good hygiene (handwashing, disinfecting) is the most cost-effective way to prevent HFMD and avoid associated medical costs entirely.
Recovery and Aftercare
The recovery period for Hand, Foot, and Mouth Disease primarily involves continued symptom management until the body fully overcomes the viral infection. Even after acute symptoms subside, some aftercare considerations can ensure a smoother transition back to normalcy.
Post-Symptom Management
- Continued Hydration: Even if mouth sores are healing, continue to encourage fluid intake, especially for children who may still be recovering their appetite. Dehydration remains a risk until regular eating and drinking are fully established.
- Gradual Return to Normal Diet: Reintroduce regular foods gradually. Start with soft, bland foods and slowly incorporate more varied textures as comfort returns. Avoid irritating foods (spicy, acidic, crunchy) until all mouth sores are completely healed.
- Monitor for Secondary Infections: While rare, open mouth sores can sometimes become secondarily infected with bacteria. Monitor for signs of worsening pain, pus, or prolonged fever, which would warrant medical attention.
- Skin Care: If significant peeling (desquamation) occurs on the fingers or toes weeks after the rash, keep the skin moisturized with gentle lotions to prevent dryness and cracking. This is a natural part of the healing process after some HFMD strains.
- Rest and Recuperation: Ensure adequate rest. Although the acute phase might be over, the body has been fighting a viral infection, and rest supports full recovery.
When Can an Individual Return to School or Work?
Guidelines for returning to group settings like school, daycare, or work vary, but generally, the focus is on reducing the risk of transmission and ensuring the individual is well enough to participate.
ADA (American Dental Association) Guidelines and Public Health Recommendations often align on these points:
- Fever-Free for 24 Hours: The individual should be fever-free for at least 24 hours without the use of fever-reducing medication. This indicates the acute phase of the illness is subsiding.
- Mouth Sores Healed or No Longer Painful: The most contagious period for oral lesions is when they are open and weeping. While it's ideal for all sores to be completely healed, the practical guideline is that they are no longer painful enough to prevent eating and drinking, and significant drooling (a transmission risk) has stopped.
- Blisters Dried or Scabbed Over: The blisters on the hands and feet should be dried or scabbed over. Fluid-filled blisters are highly contagious.
- Feeling Well Enough: The individual should feel well enough to participate in normal activities. This means no significant malaise, fatigue, or irritability.
- Hand Hygiene: Emphasize stringent hand hygiene upon return. While viral shedding in stool can continue for weeks, careful handwashing after using the restroom or changing diapers is crucial to prevent further spread.
It's important to consult with your child's pediatrician or local public health guidelines, as specific recommendations may vary slightly. The general principle is to prevent further spread while ensuring the individual is genuinely on the path to full recovery.
Prevention: How to Avoid Hand, Foot, and Mouth Disease
Preventing HFMD revolves around meticulous hygiene practices and limiting exposure, especially in high-risk environments like childcare centers. Since there's no vaccine for HFMD (though research is ongoing for EV-A71), these measures are your primary defense.
1. Hand Hygiene
This is the single most effective way to prevent the spread of HFMD and many other infectious diseases.
- Frequent and Thorough Handwashing: Wash hands often with soap and water for at least 20 seconds, especially:
- After changing diapers or using the toilet.
- Before preparing food and eating.
- After coughing, sneezing, or blowing your nose.
- After touching potentially contaminated surfaces.
- Alcohol-Based Hand Sanitizer: If soap and water are not available, use an alcohol-based hand sanitizer with at least 60% alcohol. However, handwashing with soap and water is superior for inactivating enteroviruses, which are less susceptible to alcohol sanitizers than some other viruses.
2. Disinfection of Contaminated Surfaces
The HFMD virus can survive on surfaces for several days, making environmental cleaning critical.
- Regular Cleaning: Routinely clean and disinfect frequently touched surfaces, such as doorknobs, countertops, toys, and common areas.
- Disinfectants: Use a solution of 1 tablespoon of bleach to 4 cups of water (a dilute bleach solution) or a commercially available disinfectant that is effective against viruses. Read product labels for specific instructions and contact times.
- Childcare Settings: Daycare providers should be especially diligent about cleaning toys, changing tables, and shared play areas throughout the day.
3. Avoid Close Contact
Reduce the risk of transmission by minimizing direct contact with infected individuals.
- Avoid Kissing, Hugging, and Sharing Utensils: Do not share eating utensils, cups, towels, or personal items with someone who is infected.
- Maintain Distance: If possible, try to maintain some distance from individuals showing symptoms, particularly during the peak contagious period (first week of illness).
- Isolate Sick Individuals: Keep children with HFMD home from school or daycare until their fever has resolved and they are well enough to participate, and ideally, until blisters have dried up (as per school/daycare policy).
4. Respiratory Etiquette
Practice good respiratory hygiene to contain virus-laden droplets.
- Cover Coughs and Sneezes: Use a tissue to cover coughs and sneezes, then dispose of the tissue immediately. If a tissue isn't available, cough or sneeze into your elbow, not your hands.
- Avoid Touching Face: Try to avoid touching your eyes, nose, and mouth, as this is a common way for viruses to enter the body.
5. Diaper Hygiene
This is crucial in settings with young children.
- Careful Diaper Disposal: Dispose of soiled diapers properly and immediately.
- Dedicated Changing Areas: Use designated diaper-changing areas that can be easily cleaned and disinfected after each use.
- Immediate Handwashing: Always wash hands thoroughly after changing diapers, even if you wear gloves.
By adhering to these comprehensive prevention strategies, you can significantly reduce the likelihood of contracting and spreading Hand, Foot, and Mouth Disease, contributing to a healthier environment for yourself and your community.
Risks and Complications
While Hand, Foot, and Mouth Disease is generally a mild, self-limiting illness, it can sometimes lead to complications, particularly in specific populations or with certain viral strains. Understanding these risks is crucial for knowing when to seek additional medical attention.
Common Complications
- Dehydration: This is the most common complication, especially in young children. The painful mouth sores can make swallowing extremely difficult and painful, leading to a refusal to drink.
- Signs: Reduced urination, dry mouth, lethargy, sunken eyes, absence of tears when crying.
- Management: Constant encouragement of fluid intake, using soothing liquids, popsicles, or, in severe cases, intravenous (IV) fluids in a hospital setting.
- Fingernail and Toenail Loss (Onychomadesis): A notable, though uncommon, delayed complication, particularly associated with Coxsackievirus A6. Weeks to months after the acute infection, one or more nails may loosen and fall off.
- Risk: Primarily cosmetic; new nails typically grow back without intervention, though it can take several months.
- Management: No specific treatment is needed, but protecting the nail bed during regrowth is advisable.
Rare but Serious Complications (More common with EV-A71)
- Viral Meningitis (Aseptic Meningitis): An inflammation of the membranes (meninges) surrounding the brain and spinal cord. It's usually mild and resolves without long-term consequences.
- Signs: Severe headache, stiff neck, fever, sensitivity to light (photophobia), drowsiness.
- Management: Often supportive care in a hospital, though specific antiviral treatments are not typically used for viral meningitis.
- Encephalitis: A more severe and potentially life-threatening inflammation of the brain itself. This is extremely rare with HFMD, especially in Western countries, but is a recognized complication of EV-A71.
- Signs: Severe headache, high fever, confusion, seizures, behavioral changes, weakness, coordination problems.
- Management: Requires immediate hospitalization and intensive medical care.
- Myocarditis: Inflammation of the heart muscle, also extremely rare.
- Signs: Chest pain, shortness of breath, fatigue, abnormal heart rhythms.
- Management: Requires immediate medical attention and specialized cardiac care.
- Acute Flaccid Paralysis (AFP): A very rare polio-like syndrome characterized by sudden limb weakness, also mainly associated with EV-A71.
Who is at Higher Risk for Complications?
- Infants and Very Young Children: Their immune systems are less developed, and they are more prone to rapid dehydration.
- Immunocompromised Individuals: People with weakened immune systems due to underlying conditions or medications.
- Individuals Infected with EV-A71: This specific strain carries a higher risk of neurological complications.
While the thought of complications can be concerning, it's important to remember that the vast majority of HFMD cases are mild and resolve without incident. However, being aware of these potential risks and monitoring for unusual or worsening symptoms is a crucial part of managing the illness responsibly.
Children / Pediatric Considerations
Hand, Foot, and Mouth Disease disproportionately affects infants and young children, making pediatric considerations central to understanding and managing this illness. Due to their developing immune systems, close contact in group settings, and unique challenges in communicating discomfort, children face distinct aspects of HFMD.

Why Children Are More Susceptible
- Developing Immune Systems: Young children have not yet built up immunity to the various enterovirus strains, making them highly susceptible upon first exposure.
- Close Contact Environments: Daycare centers, preschools, and playgroups are breeding grounds for HFMD. Children frequently share toys, hug, and interact closely, facilitating rapid viral spread.
- Poor Hygiene Habits: Toddlers and preschoolers are still learning proper hand hygiene. They often put their hands in their mouths, touch their faces, and may not wash hands effectively after using the toilet or sneezing.
Unique Challenges in Children
- Communication of Pain: Infants and very young children cannot articulate the severity of their sore throat or mouth pain. Parents must rely on behavioral cues like increased irritability, crying, refusal to eat or drink, or excessive drooling.
- Dehydration Risk: This is the most significant concern. Painful mouth sores make swallowing difficult, and children may refuse liquids, leading to rapid dehydration.
- Signs to Watch For: Fewer wet diapers than usual, lack of tears when crying, dry mouth and tongue, lethargy, sunken soft spot (fontanelle) on an infant's head.
- Sleep Disruption: Discomfort from fever and sores can significantly disrupt sleep patterns, leading to further irritability and fatigue.
- Secondary Skin Issues: While rare, children with eczema or other skin conditions might experience a more widespread or irritated rash.
Guidance for Parents
- Hydration, Hydration, Hydration: Prioritize fluid intake. Offer small, frequent sips of water, milk, or diluted juice. Popsicles, gelatin, and cold pureed fruits can be very soothing. Avoid acidic beverages.
- Pain Management: Administer age-appropriate doses of acetaminophen or ibuprofen as directed by a pediatrician to manage fever and pain. Always consult a doctor for correct dosages based on weight.
- Soft Food Diet: Offer bland, soft foods that don't require much chewing. Examples: yogurt, applesauce, mashed potatoes, well-cooked noodles, scrambled eggs. Avoid anything spicy, salty, acidic, or crunchy.
- Oral Comfort: For older children, warm salt water rinses can help. For younger children, a cool, soft washcloth or gently applying a very small amount of a pediatric-approved oral numbing gel (under medical guidance) might offer temporary relief.
- Monitor Symptoms Closely: Watch for signs of dehydration or worsening symptoms (e.g., very high fever, stiff neck, extreme lethargy, prolonged irritability).
- Strict Hygiene: Emphasize handwashing for everyone in the household, especially after diaper changes, using the bathroom, and before preparing food. Disinfect toys and shared surfaces regularly.
- Isolation: Keep children home from daycare or school until they are fever-free for 24 hours (without medication), feel well enough to participate, and their blisters have largely dried. This prevents further spread within the community.
The average how long does Hand Foot and Mouth last question for children typically falls within the 7-10 day range. Parents should be prepared for a week of discomfort and vigilance in managing symptoms, especially hydration, to ensure their child recovers smoothly.
Frequently Asked Questions
Here are some common questions parents and caregivers ask about Hand, Foot, and Mouth Disease:
How long is a child contagious with Hand, Foot, and Mouth Disease?
A child is most contagious during the first week of illness when symptoms are active, but the virus can continue to shed in stool for several weeks or even months after symptoms resolve. Therefore, good hand hygiene remains crucial long after recovery.
Can adults get Hand, Foot, and Mouth Disease?
Yes, adults can definitely get HFMD, especially if they haven't been exposed to the specific viral strain before or have close contact with infected children. While often milder, adult cases can sometimes be more uncomfortable, with more pronounced symptoms or a more widespread rash.
Is Hand, Foot, and Mouth Disease related to Foot-and-Mouth Disease in animals?
No, despite the similar names, Hand, Foot, and Mouth Disease (HFMD) in humans is caused by human enteroviruses and is not related to Foot-and-Mouth Disease, which affects livestock like cows, sheep, and pigs. These are two completely different diseases caused by different viruses.
When should I worry about dehydration in my child?
You should worry about dehydration if your child has significantly decreased urination (fewer wet diapers or trips to the bathroom), very dry mouth, no tears when crying, unusual lethargy, or sunken eyes. These are clear signs to contact a doctor immediately.
What foods should I avoid giving my child with HFMD?
Avoid foods that are acidic (citrus fruits, tomatoes, certain juices), salty, spicy, crunchy, or hot in temperature, as these can irritate painful mouth sores. Stick to bland, soft, cool foods like yogurt, applesauce, mashed potatoes, and cold drinks.
Can a person get Hand, Foot, and Mouth Disease more than once?
Yes, a person can get HFMD multiple times because it is caused by different strains of enteroviruses. Infection with one strain provides immunity only to that specific strain, not to others.
Are there any long-term effects of Hand, Foot, and Mouth Disease?
For most individuals, there are no long-term effects. Rarely, some strains (like Coxsackievirus A6) can lead to temporary nail shedding weeks later, but the nails typically grow back without intervention. Very rare neurological complications exist, primarily with EV-A71, but are not typical.
Can I go to work if my child has Hand, Foot, and Mouth Disease?
You can generally go to work if your child has HFMD, provided you are not experiencing symptoms yourself. However, rigorous hand hygiene is essential to prevent yourself from contracting the virus and potentially spreading it to others at your workplace.
What are "tonsil stones" and are they related to HFMD?
Tonsil stones (tonsilloliths) are calcified accumulations of bacteria, food debris, and mucus that form in the crevices of the tonsils. They are not related to Hand, Foot, and Mouth Disease. While HFMD causes sore throats and sometimes white spots in the mouth, these are viral lesions, not tonsil stones.
What is the supportive therapy for tonsil stones?
Supportive therapy for tonsil stones typically involves good oral hygiene, gargling with salt water, and sometimes manually dislodging them with a cotton swab. Professional removal or, in recurrent severe cases, tonsillectomy, might be considered. This is a completely separate condition from HFMD.
When to See a Dentist
While Hand, Foot, and Mouth Disease is primarily a medical condition, the oral manifestations often cause significant discomfort and can warrant dental considerations or, more commonly, a referral from a dentist to a medical doctor.
Red Flags for Immediate Attention (Medical Doctor)
Most concerns related to HFMD's oral symptoms fall under general medical care, but a dentist might be the first to spot these issues or be asked for advice.
- Signs of Severe Dehydration: As noted, this is a major concern. If your child has very few wet diapers, a dry mouth, is lethargic, or isn't producing tears, seek immediate medical attention. A dentist might observe severe dry mouth (xerostomia) and swollen, painful gums during an oral exam, prompting a medical referral.
- High or Persistent Fever: A fever that remains very high (over 102°F/39°C) for more than 3 days, or returns after seemingly getting better, requires evaluation by a medical doctor.
- Worsening Oral Pain Preventing Eating/Drinking: If the mouth sores are so painful that the individual cannot consume adequate fluids or soft foods for an extended period, leading to concern for malnutrition or dehydration, a medical doctor should be consulted.
- Signs of Secondary Bacterial Infection: Although rare, open mouth sores could become secondarily infected. Look for increased redness, swelling, pus, or a foul odor from the mouth that isn't typical for HFMD.
- Neurological Symptoms: Any signs of severe headache, stiff neck, confusion, seizures, or unusual drowsiness warrant immediate emergency medical care.
When a Dentist Might Be Consulted or Provide Guidance
While a dentist typically doesn't treat HFMD, they can play a supportive role in oral health management and differential diagnosis:
- Oral Pain Management Advice: A dentist can offer specific recommendations for over-the-counter oral rinses or gels to help soothe mouth sores and improve comfort, especially for older children and adults. They can advise on non-irritating oral hygiene practices during the acute phase.
- Differentiating Oral Lesions: In some cases, oral lesions from HFMD might be mistaken for other conditions like herpes simplex stomatitis or aphthous ulcers. A dentist's expertise can help differentiate these, though a medical doctor typically confirms the HFMD diagnosis.
- Monitoring Oral Health: During recovery, a dentist can check for any residual oral issues or discuss long-term effects such as nail shedding if the patient has concerns.
- General Oral Hygiene During Illness: The ADA (American Dental Association) emphasizes the importance of maintaining oral hygiene even during illness. A dentist can provide guidance on gentle brushing techniques, recommending soft-bristled toothbrushes, and using non-irritating toothpaste during a flare-up of oral sores. They might also stress replacing toothbrushes after the illness resolves to prevent re-infection or spread.
For the primary diagnosis and management of Hand, Foot, and Mouth Disease, a medical doctor (pediatrician or family physician) is the appropriate healthcare provider. However, the dental team is an excellent resource for managing the specific oral discomfort and ensuring overall oral health during the course of the illness and recovery.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Oral Candidiasis Symptoms: Complete Guide
Oral candidiasis, commonly known as oral thrush, is a fungal infection of the mouth caused by an overgrowth of Candida yeast, most often Candida albicans. While Candida is a normal inhabitant of the human mouth in small amounts, an imbalance can lead to uncomfortable and sometimes painful symptoms
February 23, 2026
Are Cold Sores Contagious
In the United States, an estimated 67% of the population under age 50 carries the herpes simplex virus type 1 (HSV-1), the primary cause of cold sores. This means millions of Americans are susceptible to these often painful and highly visible oral lesions. Beyond the discomfort and cosmetic conc
February 23, 2026
Cold Sore vs Pimple on Lip: Complete Comparison Guide
When you notice an unexpected bump or lesion on your lip, your mind might immediately jump to questions of what it is, how long it will last, and most importantly, if it's contagious. The confusion between a cold sore vs pimple on lip is incredibly common, yet the distinction is crucial for prop
February 23, 2026

Hand Foot and Mouth Symptoms: Complete Guide
Imagine your child wakes up with a fever, feels a little off, and then you spot painful sores appearing in their mouth, followed by a tell-tale rash on their hands and feet. This scenario, unfortunately common, is often the first encounter with Hand Foot and Mouth Disease (HFMD). Affecting millions
February 23, 2026