How Long Is Hand Foot and Mouth Contagious

Key Takeaways
- When a child – or even an adult – develops painful sores in their mouth, a distinctive rash on their hands and feet, and a fever, the immediate concern often turns to Hand, Foot, and Mouth Disease (HFMD). A common viral illness, HFMD can sweep through households and daycares, leaving a trail of disc
When a child – or even an adult – develops painful sores in their mouth, a distinctive rash on their hands and feet, and a fever, the immediate concern often turns to Hand, Foot, and Mouth Disease (HFMD). A common viral illness, HFMD can sweep through households and daycares, leaving a trail of discomfort and parental anxiety. One of the most pressing questions for anyone dealing with an HFMD diagnosis is: how long is Hand, Foot, and Mouth contagious? Understanding the duration of contagiousness is crucial for preventing its spread, protecting vulnerable individuals, and knowing when it's safe to return to normal activities.
This comprehensive guide from SmilePedia.net will delve deep into the intricacies of Hand, Foot, and Mouth Disease. We'll explore its causes, symptoms, and the various factors influencing its contagiousness. You'll learn about effective strategies for managing symptoms, preventing transmission, and navigating the recovery process. From detailed treatment options to practical prevention tips and essential pediatric considerations, this article aims to be your definitive resource, equipping you with the knowledge to confidently address HFMD, understand its timeline, and maintain optimal oral and overall health.
Key Takeaways:
- HFMD is most contagious during the first week of illness, especially when fever is present and blisters are forming.
- The virus can shed in stool for several weeks to months after symptoms resolve, though transmission risk significantly decreases once symptoms are gone.
- Isolation period: Children should typically stay home from school/daycare until they are fever-free for 24 hours without medication and can swallow comfortably.
- Prevention is key: Rigorous handwashing (especially after diaper changes/toilet use) and disinfection of contaminated surfaces are paramount.
- Symptom management costs: Primarily involve over-the-counter pain relievers (e.g., ibuprofen, acetaminophen) costing $5-$20, and hydration solutions costing $10-$30. Doctor visits for diagnosis range from $100-$300 without insurance, often covered by insurance with a co-pay of $20-$75.
- Serious complications are rare, but dehydration from painful mouth sores is a primary concern, potentially requiring urgent care or hospital visits costing $1,000-$5,000+.
- While there's no specific cure, symptomatic relief can make the illness more tolerable, with most cases resolving within 7-10 days.
What It Is / Overview
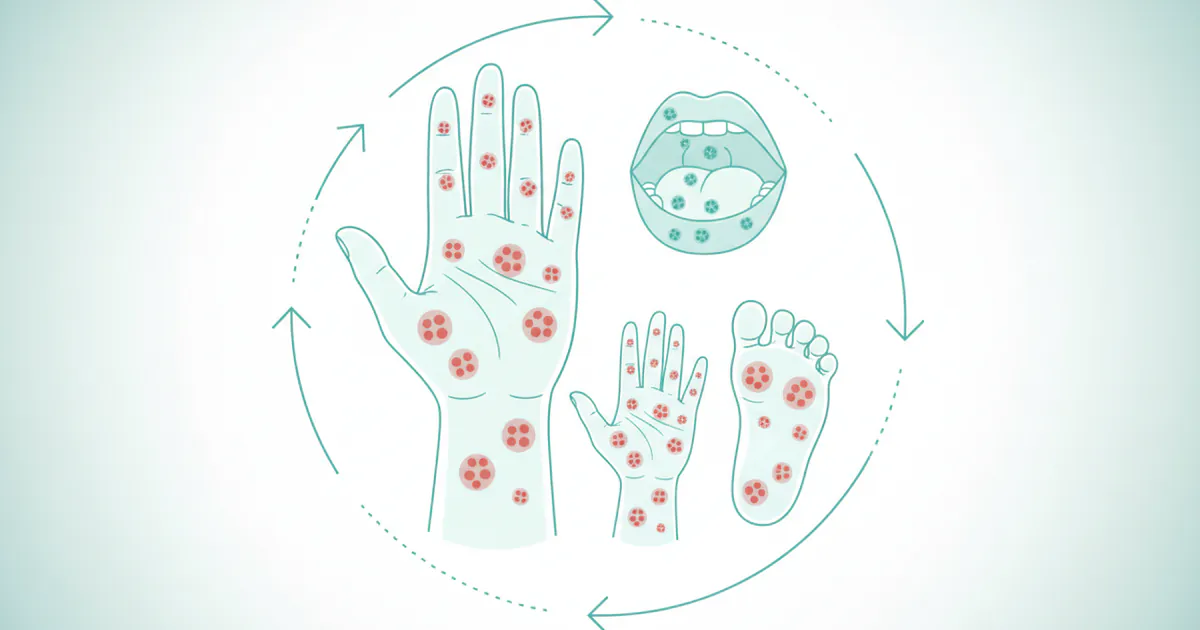
Hand, Foot, and Mouth Disease (HFMD) is a common, highly contagious viral infection that primarily affects infants and children younger than 5 years old, though older children and adults can also contract it. It is characterized by fever, painful sores in the mouth, and a rash with blisters on the hands, feet, and sometimes the buttocks and groin.

The condition is caused by viruses belonging to the Enterovirus genus, most commonly Coxsackievirus A16 (CVA16) and Enterovirus 71 (EV71). While generally a mild and self-limiting illness, its highly contagious nature and the discomfort it causes, particularly due to the oral lesions, make it a significant concern for parents and caregivers. HFMD is distinct from foot-and-mouth disease (also known as hoof-and-mouth disease), which affects livestock and is caused by a different virus, posing no threat to humans.
The oral manifestations of HFMD are often the most distressing. Small, red spots typically appear in the mouth, particularly on the tongue, gums, and inner cheeks, which quickly develop into painful blisters and then ulcers. These oral sores, known as herpangina, can make eating, drinking, and swallowing very difficult, leading to a significant risk of dehydration, especially in young children. The accompanying skin rash typically does not itch but can be tender. Understanding the full scope of HFMD, from its viral origins to its progression, is the first step in effective management and prevention.
Types / Variations
While the term "Hand, Foot, and Mouth Disease" generally refers to the classic presentation caused by Coxsackievirus A16, there are variations depending on the specific strain of enterovirus involved. The most common culprits include:
Coxsackievirus A16 (CVA16)
This is the most frequent cause of HFMD in the United States. Infections with CVA16 typically result in the classic symptoms: fever, sore throat, and the characteristic rash and mouth sores. The illness is usually mild and resolves within 7 to 10 days without serious complications.
Enterovirus 71 (EV71)
EV71 can also cause HFMD, and while it often presents similarly to CVA16 infections, it is sometimes associated with more severe complications, particularly neurological ones such as viral meningitis (inflammation of the membranes surrounding the brain and spinal cord), encephalitis (inflammation of the brain), or acute flaccid paralysis. EV71 outbreaks are more common in Southeast Asia, though cases can occur globally.
Coxsackievirus A6 (CVA6)
In recent years, Coxsackievirus A6 has emerged as another common cause of HFMD, particularly in the US and Europe. Infections with CVA6 can lead to a more severe or atypical form of HFMD. This "atypical HFMD" may feature:
- Wider rash distribution: The rash might appear on areas not typically affected, such as the trunk, arms, and legs, or even resemble chickenpox.
- More widespread or severe skin involvement: Larger blisters, sometimes with shedding of skin.
- Onychomadesis: This is the shedding of fingernails and toenails, a temporary but alarming complication that can occur several weeks after the initial infection. Nails typically regrow normally.
Other Enteroviruses
Less commonly, other enterovirus strains can cause HFMD or similar symptoms, though CVA16, EV71, and CVA6 are the predominant types associated with the classic illness. The general approach to managing symptoms and preventing spread remains similar regardless of the specific strain, as treatments are primarily supportive.
Understanding these variations is important for clinicians to consider potential complications, especially in the context of outbreaks or more severe presentations, though for the general public, the primary focus remains on symptom relief and infection control.
Causes / Why It Happens
Hand, Foot, and Mouth Disease is caused by enteroviruses, a group of viruses that typically reside in the intestinal tract. The most common viruses responsible for HFMD are Coxsackievirus A16 and Enterovirus 71, with Coxsackievirus A6 also becoming a prevalent cause of more atypical presentations.
How the Virus Spreads (Transmission)
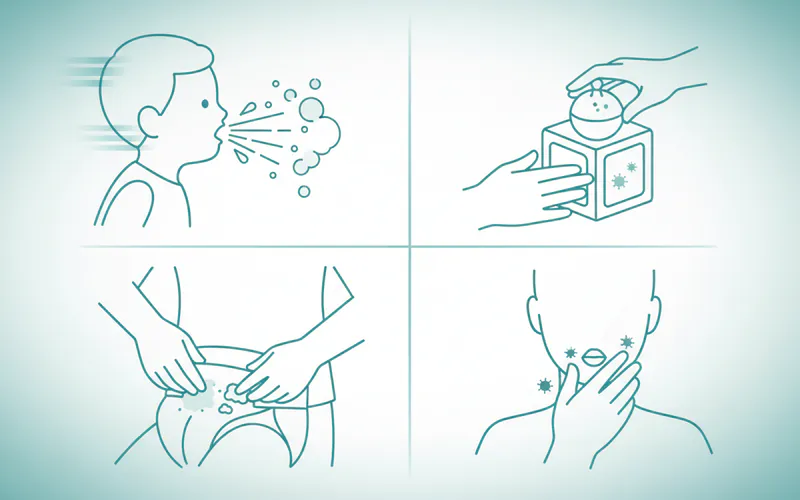
HFMD is highly contagious and spreads primarily through person-to-person contact via:
- Direct Contact:
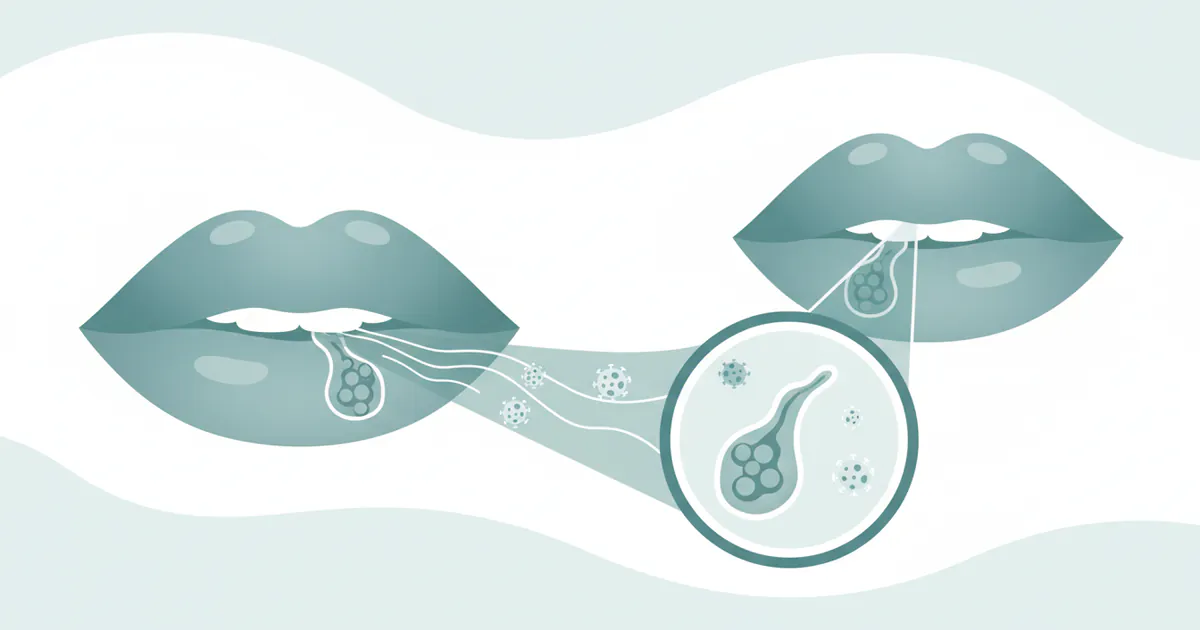
- Respiratory secretions: Droplets expelled when an infected person coughs, sneezes, or talks. These droplets can be inhaled by others or land on surfaces.
- Saliva: Direct contact with saliva from an infected person, such as sharing utensils or toys.
- Fluid from blisters: Direct contact with fluid from the characteristic blisters on the hands, feet, or mouth.
- Fecal-Oral Route: This is a major pathway for transmission, especially among young children in settings like daycares. The virus can be shed in the stool of an infected person for weeks, and even months, after symptoms have disappeared. If someone doesn't wash their hands thoroughly after using the toilet or changing a diaper, they can contaminate surfaces or food, leading to others ingesting the virus.
- Contaminated Objects: Touching contaminated surfaces or objects (toys, doorknobs) that have the virus on them and then touching one's mouth, nose, or eyes.
Risk Factors
Several factors increase the risk of contracting and spreading HFMD:
- Age: Infants and children under 5 years old are most susceptible because their immune systems are still developing and they are often in close contact with other children in group settings.
- Group Settings: Daycare centers, preschools, and schools are common sites for outbreaks due to the close proximity of children, shared toys, and sometimes less-than-ideal hygiene practices (e.g., incomplete handwashing).
- Immune Status: Individuals with compromised immune systems may be at a slightly higher risk for more severe disease, though HFMD is generally considered mild even in these cases.
- Seasonality: HFMD outbreaks tend to occur more frequently in the summer and fall in temperate climates, though cases can happen year-round.
Once exposed, the incubation period (the time from exposure to the onset of symptoms) typically ranges from 3 to 7 days. During this period, an infected person can already be shedding the virus and be contagious, even before symptoms appear. This pre-symptomatic shedding contributes significantly to the rapid spread of the virus within communities.
Signs and Symptoms
The presentation of Hand, Foot, and Mouth Disease typically follows a predictable pattern, though symptom severity can vary. Recognizing these signs early is crucial for timely management and preventing further spread.
Initial Symptoms (Prodromal Phase)
Symptoms usually begin abruptly with:
- Fever: Often the first sign, ranging from 100°F (38°C) to 102°F (39°C).
- Sore throat: This is a common early complaint, especially in older children and adults.
- Malaise: A general feeling of being unwell, tired, or fatigued.
- Loss of appetite: Due to the developing sore throat and later, mouth sores.
Characteristic Rash and Sores
Within one to two days after the fever starts, the more distinctive symptoms appear:
-
Mouth Sores (Herpangina):
- Small, red spots develop in the mouth, most commonly on the tongue, gums, inside of the cheeks, and the roof of the mouth.
- These spots quickly turn into painful blisters that rupture, forming shallow, yellow-gray ulcers with a red halo.
- These sores can be extremely painful, making it difficult and painful to eat, drink, or swallow (dysphagia). This pain is a significant concern for dehydration, particularly in infants and young children.
-
Skin Rash:
- A non-itchy rash typically appears on the palms of the hands and the soles of the feet. It can also appear on the buttocks, knees, elbows, and groin area, especially in atypical presentations.
- The rash starts as small, flat red spots, which then progress to small, fluid-filled blisters (vesicles). These blisters may be surrounded by a red margin.
- Unlike chickenpox, the rash of HFMD usually does not itch, but it can be tender or painful to the touch. The blisters are generally smaller and more oval-shaped than chickenpox lesions.
Other Possible Symptoms
- Irritability: Common in infants and young children due to discomfort and pain.
- Headache: More prevalent in older children and adults.
- Diarrhea: Less common but can occur.
Differential Diagnosis: Distinguishing HFMD from Other Conditions
Because HFMD involves oral sores and a rash, it can sometimes be confused with other conditions. Differentiating it is important for correct management:
- Oral Thrush (Candidiasis): This is a fungal infection that appears as creamy white lesions on the tongue, inner cheeks, gums, and tonsils. Unlike HFMD sores, oral thrush lesions can often be scraped off, revealing reddened tissue underneath, and are typically not as painful as HFMD ulcers. Oral thrush treatment involves antifungal medications, not the supportive care for HFMD.
- Canker Sores (Aphthous Ulcers): These are common, painful ulcers that appear inside the mouth. They are typically singular or in small clusters, have a white or yellow center with a red border, and are not usually accompanied by a rash on the hands or feet, or widespread fever. They are not contagious. Knowing how to get rid of a canker sore involves topical pain relievers and avoiding irritants, a different approach than HFMD management.
- Chickenpox (Varicella): Characterized by an itchy rash that turns into fluid-filled blisters all over the body, including the trunk and scalp, unlike the more localized rash of HFMD.
- Herpes Simplex Virus (Cold Sores/Herpes Gingivostomatitis): Initial oral herpes infections can cause widespread painful blisters and ulcers in the mouth, fever, and swollen lymph nodes, especially in young children. However, the skin rash typical of HFMD is absent.
| Symptom Feature | Hand, Foot, and Mouth Disease (HFMD) | Oral Thrush (Candidiasis) | Canker Sore (Aphthous Ulcer) |
|---|---|---|---|
| Cause | Viral (Coxsackievirus, Enterovirus) | Fungal (Candida albicans) | Unknown; stress, injury, diet, genetics |
| Contagious? | Highly contagious | No, but overgrowth can be. | No |
| Oral Lesions | Small, painful blisters turning into ulcers (tongue, cheeks, palate) | Creamy white patches (tongue, cheeks); can be scraped off | Single or few painful ulcers (white/yellow center, red border) |
| Location of Oral Lesions | Widespread in mouth, often in back of throat | Tongue, inner cheeks, gums | Inner cheeks, lips, tongue, soft palate |
| Skin Rash | Yes, on hands, feet, buttocks (non-itchy, blistery) | No | No |
| Fever | Common (initial symptom) | Rare, unless severe systemic infection | No |
| Pain Level (Oral) | High, interferes with eating/drinking | Mild to moderate, usually not interfering with eating/drinking | High, especially when eating acidic or spicy foods |
| Treatment Approach | Supportive care (pain relief, hydration) | Antifungal medications (e.g., Nystatin) | Symptomatic relief (topical anesthetics, oral rinses) |
Timely and accurate identification of HFMD symptoms allows for appropriate supportive care and crucial measures to limit its spread within communities.
How Long Is Hand Foot and Mouth Contagious?
This is the central question for parents and caregivers. Understanding the contagiousness timeline of Hand, Foot, and Mouth Disease is vital for infection control and making informed decisions about school, daycare, and social interactions.
HFMD is highly contagious, and the period of contagiousness can be surprisingly long. Here's a breakdown:
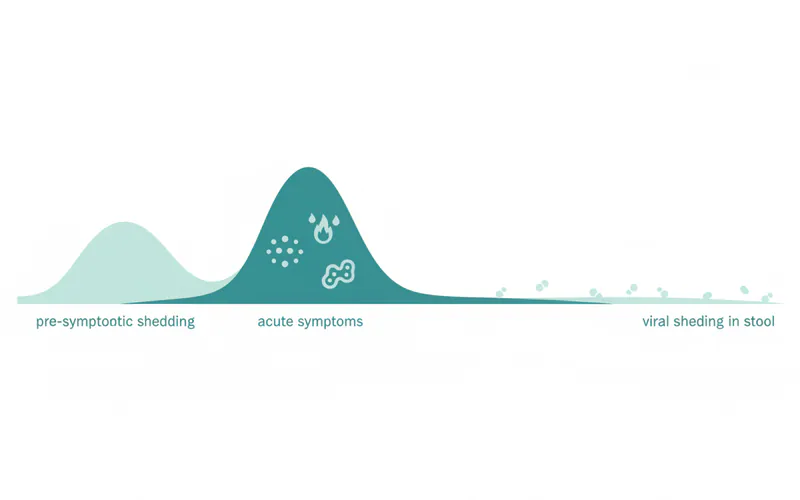
Peak Contagious Period: The First Week
- Most contagious: An individual with HFMD is most contagious during the first week of the illness, especially when they have a fever and when the blisters are first forming and are full of fluid.
- Pre-symptomatic shedding: The virus can be present in respiratory secretions (saliva, nasal mucus, phlegm) and stool before symptoms even appear. This means an infected person can spread the virus for a few days before they even know they are sick.
Post-Symptom Resolution: Continued Shedding
- Respiratory shedding: The virus can continue to shed in respiratory secretions for 1 to 3 weeks after symptoms have disappeared.
- Fecal shedding: This is where the contagiousness timeline extends significantly. The virus can continue to be shed in stool for several weeks, or even months, after all symptoms have resolved. While the risk of transmission from fecal shedding decreases over time and is generally lower than during the acute phase, it still represents a potential source of infection, especially in environments with poor hygiene.
Factors Influencing Contagiousness Duration:
- Virus Type: While general guidelines apply, some enterovirus strains might be shed for slightly different durations.
- Individual Immune Response: A person's immune system's efficiency in clearing the virus can influence how long they shed it.
- Hygiene Practices: Diligent handwashing is the single most important factor in limiting transmission, particularly from fecal shedding.
Practical Guidelines for Isolation and Return to Activities:
Based on the contagiousness profile, public health agencies and the American Academy of Pediatrics (AAP) generally recommend the following:
- Fever-Free: The individual should be fever-free for at least 24 hours without the use of fever-reducing medication.
- Mouth Sores Improved: The mouth sores should have sufficiently healed or improved so that the individual can eat and drink comfortably and saliva is not excessively drooling. Open, weeping blisters, especially in the mouth, pose a higher risk of viral transmission.
- Feeling Well: The child should feel well enough to participate in normal activities.
Pro Tip: Even after symptoms resolve and a child returns to school or daycare, it's crucial to continue emphasizing rigorous handwashing. This helps mitigate the risk from prolonged fecal shedding. Daycare centers often have strict policies regarding return, which should be followed closely.
While the virus can persist in the stool for an extended period, the highest risk of transmission is during the acute symptomatic phase. Once a person is symptom-free, the practical risk of casual transmission (e.g., through airborne droplets) is significantly reduced, though fecal-oral transmission remains a possibility without proper hand hygiene. This is why good hygiene practices become a lifelong habit, not just during illness.
Treatment Options
There is no specific antiviral treatment for Hand, Foot, and Mouth Disease. Since it's a viral infection, antibiotics are ineffective. Treatment is primarily supportive care, focused on alleviating symptoms and ensuring comfort while the body's immune system fights off the virus.
1. Pain Relief and Fever Reduction
- Over-the-Counter (OTC) Medications:
- Acetaminophen (Tylenol®): Effective for fever and pain.
- Ibuprofen (Advil®, Motrin®): Also effective for fever and pain, and has anti-inflammatory properties. Note: Do not give aspirin to children or teenagers with viral illnesses due to the risk of Reye's syndrome.
- Dosage: Always follow age- and weight-appropriate dosing instructions on the packaging or from your pediatrician.
- Topical Oral Anesthetics:
- Numbing gels or sprays: Products containing benzocaine (e.g., Orajel®) can temporarily relieve the pain of mouth sores. Caution: Benzocaine products are generally not recommended for children under 2 years old due to the risk of methemoglobinemia, a serious blood disorder. Consult a dentist or pediatrician for guidance.
- Magnesium hydroxide (Milk of Magnesia): Can be used as a soothing mouth rinse for older children and adults to coat and relieve irritated oral tissues. It's safe if swallowed.
2. Hydration and Nutrition
- Fluid Intake: This is the most critical aspect of care, especially for infants and young children, due to painful mouth sores making swallowing difficult.
- Offer small, frequent sips of cool liquids: water, diluted juices (e.g., apple juice), electrolyte solutions (Pedialyte®), or popsicles.
- Avoid acidic or spicy foods and drinks (e.g., orange juice, soda) as they can irritate mouth sores.
- Soft Foods:
- Offer bland, easy-to-swallow foods: yogurt, applesauce, pureed fruits, mashed potatoes, gelatin, soft cooked pasta, lukewarm soups.
- Avoid crunchy, salty, or spicy foods that can exacerbate oral pain.
3. Skin Rash Care
- The rash typically doesn't require specific treatment. Keep the areas clean and dry.
- If blisters rupture, gently clean the area with mild soap and water. Antiseptic creams or bandages are generally not needed unless there's concern for secondary bacterial infection (rare).
Pros and Cons of Treatment Options
| Treatment Type | Pros | Cons | Cost (OTC) |
|---|---|---|---|
| Oral Pain Relievers | Reduce fever and overall body pain; readily available. | Do not shorten duration of illness; may mask symptoms; potential side effects if overdosed (e.g., liver damage with acetaminophen, stomach upset with ibuprofen). | $5 - $20 (for a bottle of generic acetaminophen or ibuprofen) |
| Topical Numbing Gels | Direct relief for painful mouth sores. | Temporary relief; can taste unpleasant; benzocaine not recommended for children under 2; risk of methemoglobinemia with excessive use of benzocaine in infants. Can numb throat and affect swallowing reflex if overused. | $7 - $15 (for a tube of oral gel) |
| Hydration/Soft Foods | Prevents dehydration, maintains nutrition, aids recovery. | Can be challenging if child refuses to eat/drink due to pain; requires consistent effort from caregiver. | $10 - $30 (for electrolyte solutions, popsicles, yogurt over several days) |
| Oral Rinses (e.g. Milk of Magnesia) | Soothes mouth sores; safer than numbing gels for young children. | Taste can be unappealing for some; temporary relief; requires cooperation for rinsing. | $5 - $10 (for a bottle of generic magnesium hydroxide) |
Pro Tip: For very young children or those who are refusing liquids due to mouth pain, consider administering pain medication about 30 minutes before offering fluids or food. This can help alleviate the pain enough for them to swallow more comfortably.
When to Seek Medical Attention
While most cases of HFMD are mild and resolve on their own, it's important to know when to seek professional medical advice:
- Signs of dehydration: Decreased urination, dry mouth, no tears, lethargy.
- High fever or fever lasting more than 3 days.
- Severe mouth pain: Making it impossible to drink fluids.
- Neurological symptoms: Unusual drowsiness, confusion, headache with stiff neck, seizures, uncontrolled jerking movements (though rare, especially with CVA16).
- Persistent vomiting or diarrhea.
- Lack of improvement: Symptoms do not improve after 7-10 days.
- Immunocompromised individuals: Those with weakened immune systems should be monitored more closely.
Step-by-Step Process: What to Expect During HFMD
Understanding the typical progression of Hand, Foot, and Mouth Disease can help you anticipate symptoms and manage care effectively. While the exact timeline can vary, here’s a general step-by-step overview:

Step 1: Exposure and Incubation (Days 1-7)
- Exposure: The individual comes into contact with the virus through respiratory droplets, contaminated surfaces, or fecal-oral transmission.
- Incubation Period: For the next 3 to 7 days, the virus multiplies in the body, typically without any noticeable symptoms.
- Contagiousness: The infected person can begin shedding the virus and be contagious during this phase, even before symptoms appear.
Step 2: Prodromal Phase (Days 7-9 or 1-2 days before rash)
- Initial Symptoms: This phase typically lasts 1-2 days and marks the onset of initial, non-specific symptoms:
- Fever: Usually low-grade, but can be higher.
- Sore throat: Often a primary complaint, making swallowing uncomfortable.
- Malaise: A general feeling of being unwell and tired.
- Loss of appetite.
Step 3: Acute Symptomatic Phase (Days 9-14 or Days 1-5 of visible symptoms)
- Mouth Sores Erupt: Small, red spots appear in the mouth, usually on the tongue, gums, and inner cheeks. These quickly develop into painful blisters and then shallow ulcers (herpangina).
- Rash Develops: Within 1-2 days of mouth sores appearing, a characteristic rash emerges.
- Small, flat red spots, often evolving into small blisters, on the palms of the hands and soles of the feet.
- The rash can also appear on the buttocks, knees, elbows, or groin.
- This is typically the most uncomfortable phase due to the combined effects of fever, sore throat, and painful mouth sores.
- Peak Contagiousness: During this phase, the individual is highly contagious, especially when blisters are forming and fever is present.
- Management Focus: Aggressive pain management and diligent hydration are critical here to prevent dehydration.
Step 4: Resolution and Recovery (Days 14-21 or Days 5-10 of visible symptoms)
- Symptom Improvement: Over the next 5-7 days:
- Fever typically subsides.
- Mouth sores begin to heal, becoming less painful, allowing for easier eating and drinking.
- The skin rash starts to fade, and blisters may crust over or peel without scarring.
- Return to Activities: Once fever-free for 24 hours (without medication) and mouth sores have healed enough for comfortable swallowing, the individual can usually return to school or daycare.
- Continued Viral Shedding: Even after symptoms resolve, the virus continues to shed in respiratory secretions for 1-3 weeks and in stool for several weeks to months. Good hand hygiene remains crucial to prevent secondary spread.
Step 5: Post-Recovery (Weeks to Months Post-Infection)
- Onychomadesis (Rare but possible): In some cases, particularly with Coxsackievirus A6 infections, temporary nail shedding (fingernails and/or toenails) can occur 2-8 weeks after the illness. Nails typically regrow normally over several months. This is usually not painful.
The entire process, from initial symptoms to full resolution of the active illness, usually takes about 7 to 10 days. However, the prolonged fecal shedding period means vigilance in hygiene is necessary far beyond the visible illness.
Cost and Insurance
Managing a case of Hand, Foot, and Mouth Disease typically involves costs related to over-the-counter medications, potential doctor visits, and in rare severe cases, urgent care or hospitalizations.
1. Over-the-Counter (OTC) Medications
Most HFMD cases are managed at home with supportive care.
- Pain relievers/Fever reducers: Acetaminophen or ibuprofen.
- Cost: $5 - $20 for a bottle of generic medication, enough for several courses of illness.
- Oral numbing gels/rinses: Benzocaine gels (for older children/adults) or Milk of Magnesia.
- Cost: $7 - $15 for a tube or bottle.
- Hydration solutions: Electrolyte solutions (e.g., Pedialyte), popsicles.
- Cost: $10 - $30 for several days' supply.
- Total OTC Costs: For a typical mild case, expect to spend $20 - $65 on supplies.
2. Doctor Visits
Many cases of HFMD do not require a doctor's visit if symptoms are mild and dehydration is not a concern. However, if symptoms are severe, there are signs of dehydration, or you're unsure of the diagnosis, a doctor's visit is recommended.
- Without Insurance (Self-Pay):
- Primary Care Physician (PCP) visit: $100 - $300, depending on location and complexity.
- Urgent Care Center visit: $150 - $400, generally more expensive than a PCP due to convenience.
- Emergency Room (ER) visit: $500 - $3,000+, reserved for severe dehydration or neurological complications. This should be a last resort for non-life-threatening conditions due to the high cost.
- With Insurance:
- Most insurance plans cover doctor visits for HFMD as part of routine medical care.
- Co-pay: You will likely pay a co-pay ranging from $20 - $75 for a PCP or urgent care visit.
- Deductible: If your deductible has not been met, you may be responsible for the full cost of the visit until it is.
- ER visits: Often have higher co-pays (e.g., $100-$250) or coinsurance (e.g., 10-20% of the bill) even after the deductible.
3. Diagnostic Tests
HFMD is typically diagnosed clinically based on symptoms. Lab tests are rarely needed but might be considered in severe or atypical cases.
- Throat swab or stool sample: To confirm the specific enterovirus.
- Cost: $50 - $200+ if ordered, usually covered by insurance with a co-pay/coinsurance.
4. Hospitalization
In very rare cases, severe dehydration or neurological complications (e.g., encephalitis) might require hospitalization.
- Cost: Hospitalizations can range from $5,000 to $20,000+ depending on the length of stay and required interventions (e.g., IV fluids, specialized care). These costs are largely covered by insurance, but out-of-pocket maximums and deductibles will apply.
Cost-Saving Tips
- Home Management: For mild cases, focus on home care with OTC medications and diligent hydration to avoid unnecessary doctor visits.
- PCP First: If a visit is needed, always try to see your primary care physician first rather than going to urgent care or the ER for non-emergencies.
- Generic Medications: Opt for generic brands of acetaminophen and ibuprofen, which are just as effective as brand-name versions but significantly cheaper.
- Insurance Verification: Understand your insurance plan's coverage for urgent care vs. ER, co-pays, and deductibles before an illness strikes.
Recovery and Aftercare
Recovery from Hand, Foot, and Mouth Disease generally occurs within 7 to 10 days, with the body's immune system clearing the virus. While the active illness resolves relatively quickly, thoughtful aftercare can ease the transition back to normal life and prevent lingering issues.
1. Continued Hydration and Nutrition
- Sustained Fluid Intake: Even as mouth sores heal, continue to encourage plenty of fluids, especially if the individual has been hesitant to drink during the acute phase. Dehydration can lead to fatigue and prolonged recovery.
- Gradual Return to Normal Diet: Reintroduce a normal diet gradually. Start with soft, bland foods and slowly incorporate more varied textures and flavors. Avoid overly spicy, salty, or acidic foods for a few days even after mouth sores appear to be healed, as the mucous membranes can still be sensitive.
- Rest: Ensure adequate rest even after the fever subsides. The body expends a lot of energy fighting off a viral infection.
2. Oral Health Care
- Gentle Brushing: Continue regular oral hygiene with a soft-bristled toothbrush. Be gentle around any remaining sensitive areas or healing ulcers.
- Saline Rinses: Warm salt water rinses (1/2 teaspoon salt in 8 ounces of warm water) can continue to be soothing and help keep the mouth clean, promoting healing of any lingering oral sores. This is usually more appropriate for older children and adults who can rinse and spit effectively.
3. Skin Care
- Moisturize: If the skin on the hands and feet peeled or felt dry after the rash, a mild, unscented moisturizer can help soothe and aid skin regeneration.
- Nail Monitoring: If the infection was caused by Coxsackievirus A6, be aware that nail shedding (onychomadesis) can occur several weeks later. This is usually harmless, and nails typically regrow normally. No specific treatment is required, but monitoring is advisable.
4. Hygiene Practices
- Continued Handwashing: Emphasize stringent handwashing with soap and water for at least 20 seconds, especially after using the restroom and before eating. Remember, the virus can shed in stool for weeks to months. This is a critical habit for preventing future infections and the spread of other illnesses.
- Disinfection: Continue to routinely clean and disinfect frequently touched surfaces and shared toys, especially in common areas, for a period after recovery. Use a disinfectant that is effective against enteroviruses (e.g., diluted bleach solution, EPA-approved disinfectants).
5. Emotional Support
- For children, HFMD can be a distressing experience due to pain and discomfort. Provide comfort, reassurance, and distraction as they recover.
Pro Tip: Consider replacing toothbrushes after the acute phase of HFMD to minimize the risk of re-infection or spreading the virus to other household members, though this is a general recommendation for any oral infection.
By maintaining good hygiene and supportive care, you can ensure a smooth recovery and help prevent the spread of Hand, Foot, and Mouth Disease to others.
Prevention
Preventing Hand, Foot, and Mouth Disease primarily revolves around meticulous hygiene practices, as there is currently no vaccine available for general public use in the United States. Adhering to these strategies can significantly reduce the risk of contracting and spreading the virus.
1. Hand Hygiene: The Gold Standard
- Frequent and Thorough Handwashing: This is the most effective preventative measure.
- Wash hands with soap and water for at least 20 seconds, rubbing all surfaces.
- Crucially, wash hands:
- After using the toilet or changing diapers.
- Before preparing food and eating.
- After coughing, sneezing, or blowing your nose.
- After touching common surfaces in public.
- ADA Recommendation: The American Dental Association (ADA) and Centers for Disease Control and Prevention (CDC) consistently emphasize hand hygiene as foundational to preventing infectious disease transmission.
- Alcohol-Based Hand Sanitizers: If soap and water are not available, use an alcohol-based hand sanitizer with at least 60% alcohol. However, hand sanitizers are less effective than soap and water, especially if hands are visibly dirty or after contact with stool.
2. Disinfection of Contaminated Surfaces
- Regular Cleaning: Routinely clean and disinfect frequently touched surfaces, especially in homes with young children and in daycare settings.
- Examples: Toys, doorknobs, tables, countertops, faucets, shared electronic devices.
- Effective Disinfectants: Use a diluted bleach solution (e.g., 1 tablespoon of bleach in 4 cups of water) or EPA-approved disinfectants that are effective against enteroviruses. Follow product instructions carefully.
- Toy Cleaning: For shared toys in daycares, ensure they are cleaned and disinfected regularly, especially if a child with HFMD has played with them.
3. Avoid Close Contact
- Sick Individuals: Avoid close contact with people who have HFMD, particularly during the acute phase of their illness when they are most contagious.
- Sharing: Do not share eating utensils, cups, towels, or personal items with anyone, especially if they are symptomatic.
- Kissing and Hugging: Refrain from kissing or hugging individuals with active HFMD.
4. Isolation of Infected Individuals
- Stay Home: Keep children with HFMD home from school, daycare, or other group settings until their fever has resolved for 24 hours (without medication) and their mouth sores have healed enough for comfortable swallowing. While fecal shedding continues, isolating during the symptomatic phase significantly reduces the highest risk of transmission.
- Monitor Other Household Members: If one family member has HFMD, other household members, especially young children, should be monitored closely for symptoms and extra vigilance applied to hygiene.
5. Teach Children Good Hygiene
- Start teaching children proper handwashing techniques and the importance of not putting hands in their mouths from a young age. This foundational health education is crucial for preventing not just HFMD but a multitude of infections.
By implementing these comprehensive prevention strategies, families and communities can significantly reduce the incidence and spread of Hand, Foot, and Mouth Disease.
Risks and Complications
While Hand, Foot, and Mouth Disease is typically a mild and self-limiting illness, certain risks and complications can arise, especially in specific populations or due to the severity of symptoms. Awareness of these potential issues is important for timely intervention.
1. Dehydration
- Primary Concern: This is the most common and significant complication, particularly in infants and young children.
- Cause: The painful mouth sores (herpangina) can make swallowing extremely difficult and painful, leading to a refusal to eat or drink.
- Signs: Decreased urination (fewer wet diapers in infants), dry mouth, lack of tears, lethargy, sunken soft spot (fontanelle) in infants, and irritability.
- Intervention: If signs of dehydration are present, immediate medical attention is necessary. This may involve oral rehydration solutions or, in severe cases, intravenous (IV) fluids in an urgent care or hospital setting.

2. Secondary Bacterial Infections
- Rare: While uncommon, the open blisters and ulcers in the mouth or on the skin can potentially become infected by bacteria.
- Signs: Increasing pain, redness, swelling, pus formation, or a foul odor around the sores.
- Intervention: A doctor may prescribe antibiotics if a secondary bacterial infection is suspected, as antibiotics are ineffective against the viral HFMD itself.
3. Neurological Complications (More common with EV71)
- Very Rare: These are infrequent but serious complications, typically associated with Enterovirus 71 (EV71) outbreaks, which are more common in Southeast Asia but can occur globally.
- Types:
- Viral Meningitis (Aseptic Meningitis): Inflammation of the meninges (membranes surrounding the brain and spinal cord). Symptoms include severe headache, stiff neck, fever, and light sensitivity.
- Encephalitis: Inflammation of the brain, a more severe and potentially life-threatening condition. Symptoms can include altered mental status, seizures, weakness, or movement disorders.
- Acute Flaccid Paralysis: Sudden onset of weakness or paralysis in one or more limbs.
- Intervention: Any signs of neurological involvement warrant immediate emergency medical evaluation.
4. Onychomadesis (Nail Shedding)
- Temporary and Harmless: As mentioned, this is the shedding of fingernails and/or toenails, which can occur several weeks (2-8 weeks) after an HFMD infection, especially those caused by Coxsackievirus A6.
- No Treatment: The nails usually grow back normally over several months. It is not painful and typically causes no long-term damage.
5. Increased Risk for Pregnant Women
- While HFMD is generally mild for pregnant women, fever and illness during pregnancy can sometimes pose a risk to the fetus, especially close to delivery.
- Transmission to Newborn: If a pregnant woman contracts HFMD shortly before delivery, there's a small chance the virus could be passed to the newborn, who could develop a severe form of the disease.
- Recommendation: Pregnant women, especially those in their third trimester, should take extra precautions to avoid exposure, particularly if they work in childcare settings or have other young children at home. Consult an obstetrician if exposure or symptoms occur.
It's important to reiterate that the vast majority of HFMD cases resolve without any of these severe complications. Vigilant symptom monitoring and appropriate supportive care are usually sufficient for a full recovery.
Children / Pediatric Considerations
Hand, Foot, and Mouth Disease predominantly affects infants and young children, typically under the age of 5. This demographic has unique vulnerabilities and considerations that parents and caregivers need to understand.
Why Children are More Susceptible
- Developing Immune Systems: Young children's immune systems are still maturing, making them more susceptible to common viral infections like HFMD.
- Close Contact: Daycare centers, preschools, and playgroups are ideal environments for viral transmission due to children's close proximity, shared toys, and less developed hygiene habits.
- Fecal-Oral Transmission: Diaper changing and toddlers' tendency to put hands and objects into their mouths facilitate the fecal-oral spread of enteroviruses.
Specific Challenges in Pediatric HFMD
- Dehydration Risk: Infants and toddlers are particularly prone to dehydration because they cannot communicate their pain or thirst effectively, and their body reserves are smaller. The painful mouth sores can cause them to refuse bottles, breastfeeding, or sips of water.
- Parental Action: Parents must be vigilant for signs of dehydration (fewer wet diapers, dry mouth, no tears, lethargy). Offer small, frequent sips of cool liquids (breast milk, formula, water, electrolyte solutions like Pedialyte) using a spoon, dropper, or syringe if necessary. Avoid juice as it can irritate sores.
- Pain Management: Managing pain in young children can be challenging.
- Parental Action: Use age- and weight-appropriate doses of acetaminophen or ibuprofen. Time medication administration about 30 minutes before offering fluids or food to maximize comfort during eating/drinking. Topical oral gels (benzocaine-free for under 2s) can be considered with a pediatrician's guidance.
- Irritability and Sleep Disruption: Pain and discomfort can make children irritable and lead to disturbed sleep for both the child and parents.
- Parental Action: Create a comfortable, quiet environment. Offer comfort measures like cuddles, lukewarm baths (if the child tolerates it), and gentle distractions.
- School/Daycare Exclusion: Most childcare facilities have strict policies regarding HFMD to prevent outbreaks.
- Parental Action: Children usually need to stay home until they are fever-free for 24 hours (without medication) and their mouth sores have healed enough for comfortable swallowing and they are no longer excessively drooling. Always check with your specific daycare or school's policy.
Special Considerations for Infants
- Neonates (Newborns): While rare, HFMD in newborns can be more severe, especially if the mother was infected shortly before delivery. Neonates have immature immune systems, and the infection can be systemic. Close monitoring and immediate medical attention are crucial.
- Breastfeeding: Continue breastfeeding if possible, as breast milk provides critical antibodies and hydration. It is often well-tolerated even with mouth sores.
Pediatric Prevention Focus
- Handwashing Education: Teach and reinforce handwashing from a very young age. Make it a routine after toilet use, before eating, and after playing.
- Diaper Changing Hygiene: Meticulous handwashing after diaper changes is paramount for caregivers.
- Toy Disinfection: Regularly clean and disinfect shared toys, especially in group settings, using appropriate virucidal cleaners.
- Avoid Sharing: Teach children not to share cups, utensils, or toothbrushes.
Pro Tip: For children experiencing extreme pain with swallowing, offer bland, cold, smooth foods such as ice cream, yogurt, or smoothies. These can be less irritating and more appealing.
Frequently Asked Questions
What exactly causes Hand, Foot, and Mouth Disease?
Hand, Foot, and Mouth Disease (HFMD) is caused by various viruses belonging to the Enterovirus genus, most commonly Coxsackievirus A16 (CVA16), Enterovirus 71 (EV71), and Coxsackievirus A6 (CVA6). These viruses are highly contagious and spread through respiratory secretions, direct contact with blister fluid, and the fecal-oral route.
Is Hand, Foot, and Mouth Disease serious for adults?
While adults can get HFMD, it is generally milder than in children. However, some adults may experience more severe symptoms, including higher fevers, more widespread and painful rashes, and significant discomfort from oral sores. Adults can also experience the rarer complications seen in children, though this is uncommon.
How is Hand, Foot, and Mouth Disease different from oral thrush?
HFMD causes distinct, painful blisters and ulcers (herpangina) in the mouth, usually accompanied by a rash on the hands and feet and fever. Oral thrush, on the other hand, is a fungal infection characterized by creamy white patches that can be scraped off the tongue and inner cheeks, typically without fever or a body rash. Oral thrush treatment involves antifungal medications.
What should I do if my child refuses to drink due to mouth pain?
If your child refuses to drink, prioritize small, frequent sips of cool, non-acidic liquids like water, diluted clear juice, or electrolyte solutions. Offer popsicles, ice chips, or soft, cold foods like yogurt or applesauce. Administer age-appropriate pain relief (acetaminophen or ibuprofen) about 30 minutes before offering fluids to make swallowing more comfortable. Watch closely for signs of dehydration and seek medical attention if they appear.
Can I get Hand, Foot, and Mouth Disease more than once?
Yes, you can get HFMD multiple times. This is because there are several different strains of enteroviruses that can cause the disease. Immunity developed from one strain typically protects you only from that specific strain, leaving you susceptible to others.
Is there a vaccine for Hand, Foot, and Mouth Disease?
Currently, there is no widely available vaccine for Hand, Foot, and Mouth Disease in the United States. Research is ongoing, and some vaccines targeting specific enterovirus strains (like EV71) are used in certain countries, particularly in Asia, where severe outbreaks are more common.
How can I "get rid of a canker sore" versus HFMD mouth sores?
Canker sores are usually singular or small clusters of ulcers that are not contagious and not typically accompanied by fever or a body rash. How to get rid of a canker sore involves topical pain relievers, oral rinses, and avoiding irritants. HFMD mouth sores are part of a widespread viral infection, contagious, and come with a fever and rash. Treatment focuses on managing HFMD symptoms overall.
What are the average costs for managing HFMD?
For mild cases managed at home, expect to spend $20-$65 on over-the-counter pain relievers, oral soothing agents, and hydration solutions. A doctor's visit without insurance might cost $100-$300, or a co-pay of $20-$75 with insurance. Severe cases requiring urgent care or hospitalization can range from $1,000 to $20,000+, largely covered by insurance but subject to deductibles and co-insurance.
How can I prevent the spread of HFMD in my home?
The most effective methods are rigorous handwashing with soap and water for at least 20 seconds (especially after diaper changes/toilet use and before eating), regular cleaning and disinfecting of frequently touched surfaces and toys with a bleach solution or EPA-approved disinfectant, and avoiding close contact with sick individuals.
When is it safe for my child to return to school or daycare after HFMD?
Children should typically stay home until they are fever-free for at least 24 hours without fever-reducing medication, and their mouth sores have healed enough for them to eat and drink comfortably without excessive drooling. Always consult your specific school or daycare's policy, as guidelines can vary.
When to See a Dentist
While Hand, Foot, and Mouth Disease is primarily a medical condition managed by pediatricians or general practitioners, your dentist can play a supporting role, particularly concerning the oral manifestations and their impact on oral health. Here’s when consulting a dental professional might be beneficial or necessary:
Routine Dental Care vs. HFMD
- Postponing Appointments: If you or your child has active HFMD symptoms (fever, open mouth sores, rash), it is crucial to postpone any non-emergency dental appointments. This prevents the spread of the highly contagious virus within the dental office to staff and other patients. Call your dentist's office to reschedule and inform them of the reason.
- Dental Pain: If you are unsure whether oral pain is due to HFMD or another dental issue (like a cavity or abscess), your dentist can help differentiate the cause once you are no longer contagious.
When to Consult Your Dentist (Non-Emergency)
- Severe Oral Pain Interfering with Oral Hygiene: If mouth sores are so painful that they prevent you or your child from brushing teeth gently, your dentist can provide advice on alternative oral hygiene strategies to maintain some level of cleanliness without causing further discomfort.
- Lingering Oral Lesions or Concerns: If oral sores persist beyond the typical 7-10 day recovery period, or if you notice any unusual or concerning changes in the mouth (e.g., secondary infection, lesions not healing), your dentist can evaluate these. They can also help distinguish HFMD lesions from other conditions like oral thrush or severe canker sores.
- Advice on Topical Relief: While many topical remedies are available OTC, your dentist can recommend specific rinses or gels appropriate for your age and condition, especially if OTC options are not providing sufficient relief or are contraindicated (e.g., benzocaine in young children).
- Dental Anxiety after Illness: For young children who might develop dental anxiety due to the pain associated with HFMD mouth sores, your dentist can offer strategies to gently reintroduce positive oral health routines.
When to Seek Immediate Medical Attention (Not Necessarily Dental)
Remember, HFMD complications are medical emergencies, not dental emergencies. If you observe any of the following, contact your pediatrician, urgent care, or emergency room immediately:
- Signs of Dehydration: Decreased urination, dry mouth, no tears, lethargy.
- High fever or fever lasting more than 3 days.
- Severe mouth pain making it impossible to drink any fluids.
- Neurological symptoms: Unusual drowsiness, confusion, headache with stiff neck, seizures, or uncontrolled jerking movements.
- Difficulty breathing.
- Symptoms not improving after 7-10 days.
Your dental team is a valuable part of your overall health network. While they don't treat the viral infection itself, they can provide guidance and care related to oral comfort and health during and after an HFMD episode. Always prioritize your family dentist for routine oral health concerns, but remember that acute HFMD symptoms require medical, not dental, primary care.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Oral Candidiasis Symptoms: Complete Guide
Oral candidiasis, commonly known as oral thrush, is a fungal infection of the mouth caused by an overgrowth of Candida yeast, most often Candida albicans. While Candida is a normal inhabitant of the human mouth in small amounts, an imbalance can lead to uncomfortable and sometimes painful symptoms
February 23, 2026
Are Cold Sores Contagious
In the United States, an estimated 67% of the population under age 50 carries the herpes simplex virus type 1 (HSV-1), the primary cause of cold sores. This means millions of Americans are susceptible to these often painful and highly visible oral lesions. Beyond the discomfort and cosmetic conc
February 23, 2026
How Long Does Hand Foot and Mouth Last
Hand, Foot, and Mouth Disease (HFMD) is a common, often uncomfortable, viral illness that can affect anyone but is particularly prevalent among young children. If you or a loved one has ever experienced the tell-tale rash or painful mouth sores, you've likely wondered: **how long does Hand Foot and
February 23, 2026
Cold Sore vs Pimple on Lip: Complete Comparison Guide
When you notice an unexpected bump or lesion on your lip, your mind might immediately jump to questions of what it is, how long it will last, and most importantly, if it's contagious. The confusion between a cold sore vs pimple on lip is incredibly common, yet the distinction is crucial for prop
February 23, 2026