How Many Teeth Do Children Have

Key Takeaways
- Did you know that a child's smile goes through more dramatic transformations in their first 12 years than an adult's does in a lifetime? Understanding the journey of your child's dental development is fundamental to ensuring their lifelong oral health. For many parents, a common question arises: **h
How Many Teeth Do Children Have: A Comprehensive Guide to Your Child's Developing Smile
Did you know that a child's smile goes through more dramatic transformations in their first 12 years than an adult's does in a lifetime? Understanding the journey of your child's dental development is fundamental to ensuring their lifelong oral health. For many parents, a common question arises: how many teeth do children have at different stages, and what can they expect as their child's smile evolves? This comprehensive guide from SmilePedia.net will demystify the fascinating process of primary tooth eruption, shedding, and the emergence of permanent teeth, providing you with the knowledge to nurture a healthy smile from infancy through adolescence. We'll delve into timelines, potential challenges, preventive care, and essential tips for parents navigating this crucial developmental period.
Key Takeaways:
- Primary Dentition: Children typically develop 20 primary (baby) teeth, which usually fully erupt by age 2.5 to 3 years.
- Permanent Dentition: These primary teeth are gradually replaced by 32 permanent teeth (including wisdom teeth) throughout childhood and adolescence.
- First Eruption: The first primary teeth usually emerge between 6-10 months of age, often starting with the lower central incisors.
- Tooth Loss Timeline: Children generally begin to lose their primary teeth around age 6, with the process continuing until about age 12.
- Molar Milestones: The first permanent molars (often called "6-year molars") typically erupt behind the last baby teeth around age 6-7, playing a crucial role in shaping the adult bite.
- Early Dental Care is Key: The American Dental Association (ADA) recommends a child's first dental visit by their first birthday or when their first tooth appears, emphasizing prevention.
- Preventive Care Costs: Regular pediatric dental check-ups, including cleanings and fluoride treatments, typically range from $75-$200 per visit without insurance, but are often fully covered by dental plans.
The Journey of a Child's Smile: From Gums to Grin
The development of teeth is a complex and amazing biological process that begins long before a child is even born. While you can't see them, tooth buds for primary (deciduous) teeth start forming in the jaws during the second trimester of pregnancy. These tiny precursors wait patiently until it's their time to emerge, marking significant milestones in a child's growth and development.
What It Is / Overview: The Two Sets of Teeth
Humans are diphyodonts, meaning we develop two sets of teeth throughout our lives: primary (or deciduous, commonly known as "baby") teeth and permanent (or succedaneous, commonly known as "adult") teeth.
Primary Dentition: The first set of teeth a child develops consists of 20 primary teeth. These teeth are vital for a child's nutrition, speech development, and play a crucial role in maintaining space for the permanent teeth that will follow. While they are temporary, their health directly impacts the development and alignment of the permanent set. They typically start erupting around 6 months of age and are usually all present by the child's third birthday.
Permanent Dentition: As a child grows, their jaws enlarge, and the primary teeth begin to shed, making way for the permanent teeth. This process usually starts around age 6 and continues into early adolescence. A full set of permanent teeth, including wisdom teeth, comprises 32 teeth. The transition from primary to permanent dentition is a carefully orchestrated biological process, guided by genetics and influenced by oral health practices.
``
Types / Variations: Deciduous vs. Permanent Dentition
While both sets of teeth share the same fundamental purpose – chewing, speaking, and aesthetics – they have distinct differences in number, size, shape, color, and structure.
Primary Teeth (Deciduous Dentition)
Children have 20 primary teeth, divided into two arches (10 upper, 10 lower):
- Incisors (8): Four central incisors and four lateral incisors, located at the front of the mouth. These are for biting and cutting food.
- Canines (4): Also known as cuspids, these pointed teeth are next to the lateral incisors and are used for tearing food.
- Molars (8): Two first molars and two second molars on each side of the upper and lower jaws. These are the broad, flat teeth at the back of the mouth, designed for grinding food.
- Note: Children do not have premolars (bicuspids) in their primary dentition.
Characteristics of Primary Teeth:
- Whiter: Often appear whiter or more opaque than permanent teeth due to thinner enamel.
- Smaller: Generally smaller in overall size.
- Thinner Enamel: The enamel layer is thinner, making them more susceptible to rapid decay.
- Wider Pulp Chambers: The nerve and blood supply (pulp) area is proportionately larger.
- Flared Roots: The roots are often more flared to accommodate the developing permanent tooth bud beneath them.
Permanent Teeth (Succedaneous Dentition)
The full adult set comprises 32 permanent teeth (though many individuals have wisdom teeth removed, resulting in 28 functional teeth). These are also divided into two arches (16 upper, 16 lower):
- Incisors (8): Similar to primary incisors, for biting.
- Canines (4): For tearing food.
- Premolars (8): Also called bicuspids, these are unique to the permanent set and replace the primary molars. They have two cusps and are used for crushing food.
- Molars (12): These include first, second, and third molars (wisdom teeth). They are the largest teeth and are primarily for grinding.
Characteristics of Permanent Teeth:
- Darker: Appear slightly yellower or grayer due to thicker enamel that allows the underlying dentin to show through.
- Larger: Larger in size and stronger in structure.
- Thicker Enamel: More resistant to wear and decay, though still vulnerable.
- Smaller Pulp Chambers: Proportionately smaller.
- Non-Flared Roots: Roots are typically straight and longer, designed for a lifetime of service.
To highlight these differences, here's a comparison table:
| Feature | Primary (Deciduous) Teeth | Permanent (Succedaneous) Teeth |
|---|---|---|
| Total Count | 20 | 32 (including wisdom teeth) |
| Types Present | Incisors, Canines, Molars | Incisors, Canines, Premolars, Molars |
| Color | Whiter, more opaque | Slightly yellower, grayer |
| Size | Smaller overall | Larger, more robust |
| Enamel | Thinner, less mineralized | Thicker, more mineralized |
| Pulp Chambers | Proportionately larger | Proportionately smaller |
| Root Structure | Shorter, more flared, designed for resorption | Longer, stronger, generally non-flared |
| Lifespan | Temporary (sheds 6-12 years) | Lifelong (barring disease or trauma) |
| Purpose | Chewing, speech, space maintenance | Chewing, speech, aesthetics, jaw stability |
Causes / Why It Happens: The Natural Process of Tooth Development
The emergence and shedding of teeth are not random events but are driven by a complex interplay of genetic programming, jaw development, and hormonal signals.
- Genetic Predisposition: The timing and order of tooth eruption are largely genetically determined. This is why children often follow similar patterns to their parents or siblings regarding when their teeth come in or fall out.
- Jaw Growth and Development: As a child grows, their jawbones expand. This provides the necessary space for the larger permanent teeth to develop beneath the primary teeth and eventually emerge. The growth of the jaw is a critical "cause" for the sequential eruption of different tooth types.
- Physiological Root Resorption: For primary teeth to shed, their roots must undergo a process called root resorption. The developing permanent tooth below exerts pressure on the root of the primary tooth, signaling specialized cells (odontoclasts) to gradually dissolve the primary tooth's root structure. As the root shortens, the primary tooth becomes loose and eventually falls out.
- Hormonal and Nutritional Factors: While primarily genetic, general health, nutrition, and hormonal balance can subtly influence eruption timing. Severe malnutrition, certain chronic illnesses, or endocrine disorders can sometimes lead to delayed tooth eruption. Essential nutrients like calcium, phosphorus, and Vitamin D are crucial for strong tooth and bone development.
- Mechanical Stimuli: Chewing and biting play a role in stimulating jaw growth and can indirectly influence the eruption process by providing functional forces.
Signs and Symptoms: What to Look For
Understanding the signs associated with tooth eruption and shedding can help parents anticipate and manage their child's comfort.

Teething (Primary Teeth Eruption)
When primary teeth begin to push through the gums, it's known as teething. This can be an uncomfortable period for infants.
- Increased Drooling: Excessive saliva production is very common.
- Irritability and Fussiness: Children may be more restless, cry more, or have trouble sleeping.
- Swollen, Tender Gums: The gums around the erupting tooth may appear red, swollen, or bruised.
- Biting and Chewing: Infants often try to gnaw on anything they can get their hands on to relieve pressure.
- Disturbed Sleep Patterns: Discomfort can wake them up or make it difficult to fall asleep.
- Decreased Appetite: Some children may refuse food or bottles due to gum soreness.
- Mild Temperature Elevation: A slight increase in body temperature (below 100.4°F or 38°C) can be associated with teething, but a true fever is usually indicative of an illness unrelated to teething and should be investigated by a pediatrician.
- Rash around the Mouth: Constant drooling can sometimes lead to a mild rash.
Tooth Loss (Shedding Primary Teeth)
The signs of a primary tooth getting ready to fall out are usually less dramatic than teething, but still noticeable.
- Loose Tooth: This is the most obvious sign. The tooth will wiggle when touched.
- Gap Formation: As the tooth loosens and eventually falls out, a gap will appear.
- Minor Discomfort/Soreness: While generally not painful, some children may experience mild discomfort as the tooth becomes very loose.
- Minor Bleeding: Occasionally, there may be a tiny bit of blood when the tooth finally comes out, especially if pulled.
- Permanent Tooth Peeking Through: You might see the tip of the permanent tooth emerging from the gum directly beneath or slightly behind the loose primary tooth.
Treatment Options: Managing Discomfort and Dental Issues
While tooth eruption and shedding are natural processes that don't require "treatment" in the medical sense, managing associated discomfort and addressing any dental issues that arise during these periods is crucial.
For Teething Discomfort
- Gum Massage: Gently rub your child's gums with a clean finger or a soft, wet washcloth.
- Cold Objects: Offer a chilled (not frozen) teething ring, a cold washcloth, or a pacifier.
- Teething Biscuits/Crackers: For older infants who can handle solids, these can provide pressure relief, but ensure they don't contain excessive sugar.
- Over-the-Counter Pain Relievers: Acetaminophen (Tylenol) or ibuprofen (Motrin, Advil) can be used as directed by your pediatrician for temporary pain relief, especially for disturbed sleep. Always follow dosage instructions carefully.
- Teething Gels (Use with Caution): Some gels contain a topical anesthetic like benzocaine, but the ADA and FDA advise against their use in children under 2 years due to potential serious side effects, including methemoglobinemia. Opt for benzocaine-free alternatives if using gels.
For Primary Teeth Dental Issues (e.g., Cavities, Trauma)
It's a common misconception that primary teeth don't need treatment because they eventually fall out. This is incorrect; maintaining the health of primary teeth is vital.
- Fillings:
- Description: Used to treat cavities (caries). The decayed part of the tooth is removed, and the tooth is restored with a filling material.
- Pros: Stops decay, restores tooth function, prevents pain and infection.
- Cons: Requires cooperation from the child; if decay is deep, may lead to further procedures.
- Materials: Amalgam (silver), composite (tooth-colored resin), or glass ionomer (releases fluoride).
- Cost: $100-$300 per filling, depending on material and size.
- Stainless Steel Crowns (SSCs):
- Description: A pre-formed metal cap that covers the entire primary tooth, often used for large cavities, after pulpotomy, or for teeth with developmental defects.
- Pros: Durable, strong, relatively quick procedure, protects the tooth until it naturally falls out.
- Cons: Metal appearance (though tooth-colored alternatives exist, they are less durable), requires more tooth reduction than a filling.
- Cost: $200-$400 per crown.
- Pulpotomy/Pulpectomy (Baby Root Canal):
- Description: If decay reaches the pulp (nerve) of a primary tooth, a pulpotomy (removing part of the pulp) or pulpectomy (removing all the pulp) may be performed to save the tooth. An SSC is usually placed afterward.
- Pros: Saves the tooth from extraction, prevents infection spread, maintains space.
- Cons: More complex procedure, higher cost, not always successful if infection is severe.
- Cost: $300-$600 for a pulpotomy, $500-$900 for a pulpectomy.
- Extractions:
- Description: Removal of a primary tooth due to severe decay, infection, trauma, or if it's blocking the eruption of a permanent tooth.
- Pros: Eliminates pain/infection, resolves crowding.
- Cons: Creates a space that might need a space maintainer; can impact speech/chewing if many teeth are lost prematurely.
- Cost: $75-$250 per tooth.
- Space Maintainers:
- Description: If a primary tooth is lost prematurely, a custom-made appliance (fixed or removable) is used to hold the space open, preventing adjacent teeth from drifting and blocking the permanent tooth's eruption path.
- Pros: Prevents future orthodontic problems, ensures proper eruption of permanent teeth.
- Cons: Requires careful cleaning, potential for breakage, initial discomfort.
- Cost: $300-$700 per appliance.
``
Step-by-Step Process: From First Tooth to Full Adult Dentition
The eruption and shedding of teeth follow a fairly predictable sequence, though individual variations are common.
Primary Tooth Eruption Timeline
This timeline provides general age ranges. Girls often get their teeth slightly earlier than boys.
- Lower Central Incisors: 6-10 months
- Upper Central Incisors: 8-12 months
- Upper Lateral Incisors: 9-16 months
- Lower Lateral Incisors: 10-16 months
- Upper First Molars: 13-19 months (when do kids get molars? The first baby molars!)
- Lower First Molars: 14-18 months
- Upper Canines: 16-23 months
- Lower Canines: 17-23 months
- Lower Second Molars: 23-31 months
- Upper Second Molars: 25-33 months
By around 2.5 to 3 years of age, most children will have all 20 primary teeth.
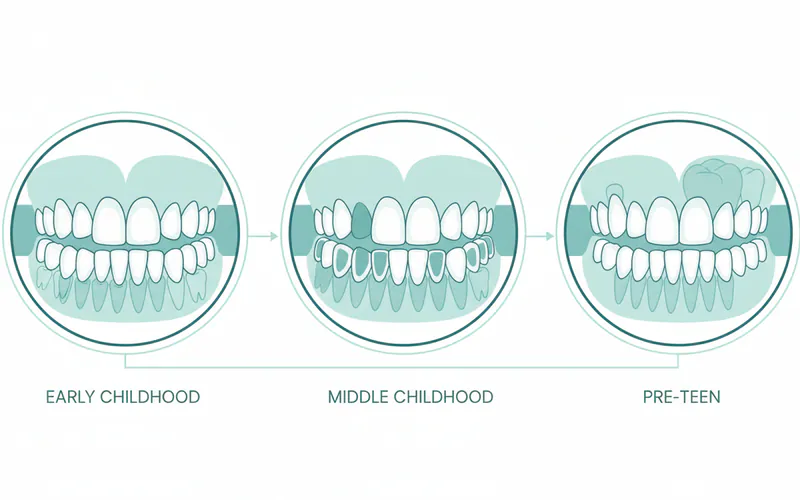
Primary Tooth Shedding & Permanent Tooth Eruption Timeline
This overlapping process marks the mixed dentition stage, where both primary and permanent teeth are present in the mouth. This is also where the question of "what age do kids lose teeth" and "when do kids get molars" (permanent ones) becomes particularly relevant.
- First Permanent Molars (The "6-Year Molars"): 6-7 years (These erupt behind the last primary molars and do not replace any baby teeth. This is often the first permanent molar a child gets.)
- Lower Central Incisors: 6-7 years (replaces primary lower central incisors)
- Upper Central Incisors: 7-8 years (replaces primary upper central incisors)
- Lower Lateral Incisors: 7-8 years (replaces primary lower lateral incisors)
- Upper Lateral Incisors: 8-9 years (replaces primary upper lateral incisors)
- Lower Canines: 9-12 years (replaces primary lower canines)
- First Premolars: 10-12 years (replaces primary first molars – children didn't have premolars before!)
- Upper Canines: 10-12 years (replaces primary upper canines)
- Second Premolars: 10-12 years (replaces primary second molars)
- Second Permanent Molars (The "12-Year Molars"): 11-13 years (These erupt behind the first permanent molars.)
- Third Permanent Molars (Wisdom Teeth): 17-25 years (These are the last to erupt, if at all.)
By the age of 12-13 years, most children will have lost all their primary teeth and have all their permanent teeth up to the second molars, totaling 28 teeth. The wisdom teeth typically emerge much later, if they have enough space.
Pro Tip: Keep a simple tooth chart at home to track your child's tooth eruption and shedding. It can be a fun way to monitor their development and identify any significant deviations that might warrant a dental check-up.
Here's a detailed timeline comparison:
| Tooth Type | Average Eruption Age (Primary) | Average Shedding Age (Primary) | Average Eruption Age (Permanent) |
|---|---|---|---|
| Central Incisors | 6-10 months | 6-8 years | 6-8 years |
| Lateral Incisors | 9-16 months | 7-9 years | 7-9 years |
| Canines | 16-23 months | 9-12 years | 9-12 years |
| First Molars/Premolars | 13-19 months | 10-12 years | 10-12 years (as Premolars) |
| Second Molars/Premolars | 23-33 months | 10-12 years | 10-12 years (as Premolars) |
| First Permanent Molars | N/A | N/A | 6-7 years (no primary predecessor) |
| Second Permanent Molars | N/A | N/A | 11-13 years |
| Third Permanent Molars | N/A | N/A | 17-25 years |
Cost and Insurance: Understanding Pediatric Dental Expenses in the US
Pediatric dental care is an investment in your child's overall health. Understanding the typical costs and how insurance plays a role can help you plan financially. Prices vary significantly based on location (urban vs. rural), the specific dental practice, and the child's individual needs.
Average US Costs for Common Pediatric Dental Procedures (Without Insurance)
- Initial Exam (new patient): $50-$150
- Routine Check-up & Cleaning (established patient): $75-$200
- Fluoride Treatment (per visit): $30-$70
- Dental Sealant (per tooth): $30-$60
- X-rays (full mouth or panoramic): $50-$150
- Composite (Tooth-Colored) Filling (per tooth): $100-$300
- Amalgam (Silver) Filling (per tooth): $75-$250
- Stainless Steel Crown (per tooth): $200-$400
- Primary Tooth Extraction: $75-$250
- Space Maintainer: $300-$700
Dental Insurance Coverage
Most dental insurance plans in the US follow a "100-80-50" coverage model, especially for children:
- Preventive Care (Exams, Cleanings, Fluoride, X-rays): Typically covered at 100%. This means little to no out-of-pocket cost for routine visits, which is why preventive care is highly encouraged.
- Basic Restorative Care (Fillings, Simple Extractions): Often covered at 80%. You would pay the remaining 20% co-insurance after meeting your deductible.
- Major Restorative Care (Crowns, Pulpotomies, Space Maintainers): Usually covered at 50%. You would pay the remaining 50% co-insurance.
Medicaid and CHIP (Children's Health Insurance Program): For low-income families, Medicaid and CHIP provide comprehensive dental benefits for children, often covering the full cost of preventive and restorative care. Eligibility varies by state, but these programs are critical for ensuring access to care.
Pro Tip: Maximize your insurance benefits by scheduling regular preventive check-ups. Catching issues early through routine cleanings and exams can prevent more expensive and invasive procedures down the line. Discuss your child's specific dental needs with your pediatric dentist to ensure you understand all recommended treatments and associated costs.
Recovery and Aftercare: Post-Procedure and Daily Oral Hygiene
Recovery after a pediatric dental procedure is generally quick, but proper aftercare is important. More importantly, consistent daily oral hygiene is crucial for preventing issues throughout childhood.
After Dental Procedures (e.g., Fillings, Extractions, Crowns)
- Numbness: If local anesthetic was used, remind your child not to bite or chew on their numb lips, tongue, or cheek. This typically wears off in 1-3 hours.
- Soft Diet: For the first 24 hours, offer soft, non-sticky foods. Avoid hard or chewy foods that could dislodge a filling or crown.
- Pain Management: Mild discomfort can be managed with over-the-counter pain relievers (acetaminophen or ibuprofen) as directed by your dentist.
- Bleeding (Extractions): Minor bleeding is normal. Apply gentle pressure with a clean gauze pad for 15-20 minutes. Avoid rinsing vigorously for 24 hours.
- Oral Hygiene: Continue gentle brushing and flossing, avoiding the immediate area of the procedure for the first day.
- Follow-up: Adhere to any specific aftercare instructions provided by your pediatric dentist.
Daily Oral Hygiene for Children
- Before First Tooth: Wipe your baby's gums with a soft, clean cloth after feedings to remove milk residue and promote good oral hygiene habits.
- First Tooth to Age 3: Start brushing with a soft-bristled, infant-sized toothbrush and a tiny smear (rice-grain size) of fluoride toothpaste. Parents should do the brushing.
- Ages 3-6: Use a pea-sized amount of fluoride toothpaste. Parents should continue to supervise and assist with brushing, ensuring all tooth surfaces are cleaned.
- Ages 6+: Most children can start brushing independently, but parents should continue to supervise until around age 8-10 to ensure thoroughness.
- Flossing: Begin flossing as soon as two teeth touch each other, usually around age 2-3. Use child-friendly flossers or a short piece of floss.
- Regular Dental Visits: Schedule routine check-ups and cleanings every six months, as recommended by the ADA.
Prevention: Protecting Your Child's Developing Smile
Preventive care is the cornerstone of pediatric dentistry. By establishing good habits early, you can significantly reduce the risk of cavities and other dental problems.
- Early Dental Visits: The American Dental Association (ADA) recommends a child's first dental visit by their first birthday or when their first tooth erupts, whichever comes first. This "dental home" approach allows for early detection of issues and parental education.
- Proper Brushing Technique: Teach and supervise your child's brushing. Brush for two minutes, twice a day, using a soft-bristled toothbrush and fluoride toothpaste appropriate for their age. Angle the brush at 45 degrees to the gum line.
- Daily Flossing: Floss daily once two teeth are touching. Flossing removes plaque and food particles that brushing alone cannot reach.
- Fluoride:
- Fluoridated Water: If your community water supply is fluoridated, it provides a safe and effective way to strengthen enamel.
- Fluoride Toothpaste: Use age-appropriate amounts.
- Professional Fluoride Applications: Your pediatric dentist can apply concentrated fluoride varnish during routine visits.
- Dental Sealants: These thin, protective coatings are applied to the chewing surfaces of back teeth (molars and premolars) where decay often begins. They act as a barrier, preventing food and bacteria from getting into the grooves and pits. Sealants are highly effective, especially when applied shortly after permanent molars erupt (around age 6-7 and 11-13).
- Healthy Diet: Limit sugary drinks and snacks. Frequent exposure to sugar feeds bacteria that produce acids, leading to cavities. Encourage a balanced diet rich in fruits, vegetables, and calcium-rich foods.
- Avoid Harmful Habits:
- Bottle Caries: Do not put your baby to bed with a bottle containing anything other than water. Sugary liquids bathing the teeth overnight can lead to severe decay.
- Thumb Sucking/Pacifier Use: While normal in infants, prolonged thumb sucking or pacifier use beyond age 3-4 can affect tooth alignment and jaw development, potentially requiring orthodontic intervention later.
- Mouthguards for Sports: If your child participates in contact sports, a custom-fitted mouthguard is essential to protect their teeth, gums, and jaws from injury.
Risks and Complications: What Can Go Wrong
While most children's dental development proceeds smoothly, various issues can arise. Awareness of these can help parents seek timely professional care.

Complications Related to Primary Teeth
- Early Childhood Caries (ECC): Commonly known as "baby bottle tooth decay," this is severe decay in infants and young children, often due to prolonged exposure to sugary liquids. It can lead to pain, infection, and premature tooth loss.
- Premature Tooth Loss: If a primary tooth is lost too early due to decay or trauma, adjacent teeth can drift into the empty space, blocking the eruption path for the permanent tooth beneath it. This often necessitates a space maintainer and can lead to orthodontic problems.
- Delayed Eruption: Primary teeth that don't erupt within the typical age range can be a sign of underlying issues, such as systemic conditions, nutritional deficiencies, or presence of extra teeth (supernumerary teeth) blocking the path.
- Teething Cysts/Eruption Hematomas: Occasionally, a bluish-black swelling (hematoma) or fluid-filled sac (cyst) may appear on the gum over an erupting tooth. These usually resolve on their own but should be monitored by a dentist.
- Dental Trauma: Falls and accidents are common in childhood. Trauma to primary teeth can damage the tooth itself or, more critically, injure the developing permanent tooth bud beneath it, leading to future enamel defects or eruption problems.
Complications Related to Permanent Teeth Eruption and Alignment
- Malocclusion (Bad Bite): This refers to any misalignment of teeth or incorrect relation between the upper and lower dental arches. Common types include crowded teeth, crooked teeth, overbite, underbite, and crossbite. These can be genetic or caused by habits like prolonged thumb sucking or premature primary tooth loss. Orthodontic treatment is often required.
- Impacted Teeth: A tooth is impacted when it's blocked from erupting into its proper position, often by another tooth, bone, or dense gum tissue. Wisdom teeth are most commonly impacted, but canines and premolars can also be affected.
- Congenitally Missing Teeth: Some children are born without the tooth buds for certain permanent teeth. The most common missing teeth are wisdom teeth, lateral incisors, and premolars.
- Supernumerary Teeth (Extra Teeth): The presence of extra teeth beyond the normal count. These can block the eruption of normal permanent teeth or cause crowding.
- Enamel Defects:
- Enamel Hypoplasia: Insufficient enamel formation, resulting in pits, grooves, or thin areas.
- Enamel Hypomineralization: Enamel that is formed but is soft and porous, making it highly susceptible to decay. These can be caused by genetic factors, severe illness or high fevers during enamel formation, or certain medications.
- Dental Fluorosis: While fluoride is beneficial, excessive fluoride intake during tooth development can lead to white or brown discoloration of the enamel.
- Delayed Eruption of Permanent Teeth: Similar to primary teeth, a permanent tooth may be delayed due to impaction, lack of space, or underlying medical conditions.
Children / Pediatric Considerations
Pediatric dentistry is a specialized field focused on the unique oral health needs of children from infancy through adolescence. Recognizing the distinct developmental stages and psychological aspects of children is paramount.
- The Dental Home Concept: The ADA advocates for establishing a "dental home" for your child by their first birthday or with the eruption of their first tooth. This means having a consistent relationship with a pediatric dentist who can provide comprehensive, continuous, and accessible oral health care.
- Age-Specific Guidance: Pediatric dentists are trained to provide age-appropriate guidance for parents and children, covering everything from proper brushing techniques for toddlers to discussing oral hygiene and dietary choices with teenagers.
- Managing Dental Anxiety: Children can be apprehensive about dental visits. Pediatric dentists and their staff are skilled in using child-friendly language, behavior management techniques (like "tell-show-do"), and creating a welcoming environment to alleviate fear and build trust.
- Importance of Primary Teeth: Beyond chewing and speech, primary teeth are crucial "space holders" for permanent teeth. Losing a baby tooth prematurely can lead to permanent teeth erupting incorrectly, necessitating future orthodontic treatment. Keeping primary teeth healthy is essential for the proper development of the permanent dentition and overall jaw structure.
- Growth and Development Monitoring: Pediatric dentists closely monitor your child's jaw growth, tooth eruption patterns, and bite development to identify potential orthodontic issues early. Early intervention can sometimes simplify or even prevent the need for extensive orthodontic treatment later.
- Sealants and Fluoride: These preventive measures are particularly vital for children. Sealants protect newly erupted permanent molars from cavities, and professional fluoride applications strengthen enamel, making it more resistant to decay.
Frequently Asked Questions
How many primary teeth do children have?
Children typically have 20 primary teeth, often referred to as baby teeth or deciduous teeth. These teeth usually fully erupt by the age of 2.5 to 3 years and are essential for chewing, speech development, and holding space for their permanent successors.
How many permanent teeth do children have?
A full set of permanent teeth, including wisdom teeth, consists of 32 teeth. However, many individuals have their wisdom teeth removed, so they may have 28 functional permanent teeth. These replace the primary teeth and also include additional molars and premolars.
At what age do kids lose teeth?
Children generally begin to lose their primary teeth around age 6, and this process continues until about age 12. The lower central incisors are often the first to go, followed by the upper central incisors, and then other teeth in sequence.
When do kids get molars?
Children get two sets of molars:
- Primary Molars: The first set of baby molars typically erupts between 13-19 months, and the second set between 23-33 months.
- Permanent Molars: The first permanent molars (often called "6-year molars") typically erupt around age 6-7, behind the last baby teeth. The second permanent molars ("12-year molars") erupt around age 11-13. Wisdom teeth (third molars) erupt much later, between ages 17-25, if they erupt at all.

Is it normal for baby teeth to fall out early?
While there's a typical range for tooth loss, some variation is normal. However, if a primary tooth falls out significantly earlier than expected (e.g., due to trauma or severe decay), it's important to see a dentist. Early loss can sometimes lead to space issues for the permanent tooth, requiring a space maintainer.
What causes delayed tooth eruption?
Delayed tooth eruption can be caused by various factors, including genetic predisposition, nutritional deficiencies, systemic illnesses, or local factors like overcrowding, an extra tooth (supernumerary tooth) blocking the path, or a dense gum tissue preventing eruption. A pediatric dentist can investigate the cause.
How can I make teething easier for my child?
To ease teething discomfort, you can gently massage your baby's gums with a clean finger, offer chilled (not frozen) teething rings or washcloths, and use over-the-counter pain relievers like acetaminophen or ibuprofen as directed by your pediatrician. Avoid benzocaine-containing gels for young children.
Why are baby teeth important if they fall out?
Baby teeth are incredibly important! They help children chew food properly for good nutrition, aid in clear speech development, and most critically, they act as natural space maintainers for the permanent teeth. Losing them too early can lead to alignment problems for the adult teeth.
How much does a pediatric dental visit cost without insurance?
A routine check-up and cleaning for a child typically costs between $75 and $200 without insurance in the US. More complex procedures like fillings or crowns will cost more. Many insurance plans, including Medicaid/CHIP, cover preventive pediatric care at 100%.
When should my child first see a dentist?
The American Dental Association (ADA) recommends that a child's first dental visit should be by their first birthday or when their first tooth appears, whichever comes first. This allows the dentist to establish a "dental home," monitor development, and educate parents on proper oral hygiene.
When to See a Dentist
Regular dental check-ups are essential for monitoring your child's dental development and maintaining oral health. However, there are specific instances when you should schedule an immediate or expedited visit:
- First Tooth or First Birthday: As per ADA guidelines, schedule the first visit when the first tooth erupts or by the child's first birthday to establish a "dental home."
- Signs of Pain or Discomfort: If your child complains of toothache, sensitivity, or has persistent pain in their mouth that doesn't resolve with home remedies.
- Swelling in Gums or Face: Swelling can indicate an infection, which requires prompt professional attention.
- Injury or Trauma: If your child sustains any injury to their mouth, teeth, or jaw, such as a chipped, cracked, knocked-out, or loosened tooth. Even if there's no visible damage, an internal injury might be present.
- Visible Cavities or Dark Spots: Any brown, black, or white spots on the teeth could indicate decay, which needs early intervention to prevent progression.
- Unusual Eruption Patterns: If teeth are significantly delayed in erupting or shedding compared to typical timelines, or if a permanent tooth is coming in behind a still-present baby tooth without the baby tooth loosening.
- Prolonged Teething Symptoms: While teething is normal, if symptoms are severe, include a high fever (above 100.4°F/38°C), or persist for an unusually long time, consult your pediatrician or dentist to rule out other issues.
- Concern about Oral Habits: If you're concerned about persistent thumb sucking, pacifier use, or tongue thrusting that could be affecting your child's bite or tooth alignment.
Early detection and intervention are key to preventing minor issues from becoming major problems and ensuring your child develops a healthy, confident smile for life.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

Kitten Teething Toys: Complete Guide
Few milestones in early life bring as much joy – and sometimes, as much discomfort – as teething. Just as a playful kitten explores its new world by mouthing and chewing on everything it can, human babies also embark on a similar developmental journey. In fact, over 80% of infants experience som
February 22, 2026

Teething Syndrome: Complete Guide
As a parent, few things are as universally anticipated and often dreaded as the arrival of your baby's first tooth. While a milestone to celebrate, the process of primary tooth eruption, commonly known as teething syndrome, can bring with it a host of challenging symptoms. In fact, studies sugge
February 22, 2026
When Do Kittens Lose Their Baby Teeth
When Do Kittens Lose Their Baby Teeth
February 22, 2026

When Do Puppies Start Teething
The journey of parenthood is filled with milestones, and for many new parents, one of the most anticipated—and sometimes dreaded—is teething. While the phrase "teething like a puppy" often comes to mind to describe an infant's discomfort, the process of when do puppies start teething is a distinct d
February 22, 2026