Tooth Anatomy Labeled: Complete Guide

Key Takeaways
- Understanding the intricate architecture of your teeth is more than just academic curiosity—it's foundational to maintaining a lifetime of optimal oral health. Every component, from the outermost protective layer to the innermost vital tissues, plays a crucial role in enabling you to chew, speak, an
Understanding the intricate architecture of your teeth is more than just academic curiosity—it's foundational to maintaining a lifetime of optimal oral health. Every component, from the outermost protective layer to the innermost vital tissues, plays a crucial role in enabling you to chew, speak, and smile with confidence. In fact, over 90% of adults aged 20-64 have had at least one dental cavity, often stemming from issues related to compromised tooth structure. This comprehensive guide will take you on a detailed journey through tooth anatomy labeled, explaining each part, its function, and how it contributes to your overall well-being. We'll explore everything from the visible crown to the hidden roots, delve into the unique aspects of pediatric dental development, discuss common issues, and equip you with the knowledge to protect your pearly whites. Get ready to uncover the fascinating world hidden beneath your smile.
Key Takeaways:
- Comprehensive Anatomy: Teeth consist of three main parts—the crown, neck, and root—each with distinct layers: enamel, dentin, cementum, and pulp.
- Pulp Vitality: The tooth pulp chamber is the living core containing nerves and blood vessels, responsible for tooth sensation and nourishment. Damage here often requires a root canal.
- Childhood Development: Primary teeth follow a predictable eruption schedule, typically starting around 6 months, and are crucial for jaw development and speech; a pediatric tooth eruption chart helps track this.
- Prevention is Key: Regular brushing, flossing, fluoride, and dental check-ups are paramount to prevent decay, gum disease, and trauma that compromise tooth structure.
- Treatment Costs: Restorative procedures like fillings range from $100-$400, crowns from $800-$3,000, and root canals from $700-$2,000, varying significantly by location and complexity.
- Insurance Coverage: Most dental insurance plans cover 80-100% of preventive care, 50-80% of basic procedures, and 0-50% of major procedures after deductibles and waiting periods.
- When to Act: Persistent pain, severe sensitivity, swelling, or visible damage to any part of the tooth structure warrants immediate dental attention to prevent further complications and potential tooth loss.
What It Is / Overview: The Marvel of Tooth Anatomy
A tooth is a complex, living organ, far more intricate than it appears. It's perfectly designed for its primary functions: tearing, chewing, and grinding food, aiding in speech, and maintaining the structure of the face. Understanding its anatomy provides insight into how these functions are performed and, crucially, how dental problems can arise when any part is compromised.

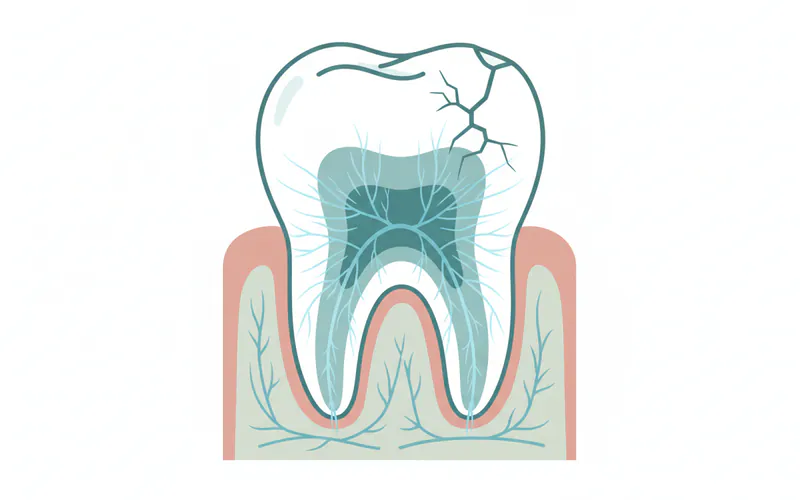
At a high level, every tooth has two main anatomical sections: the crown and the root. The crown is the visible part that protrudes above the gum line, while the root is embedded within the jawbone, anchoring the tooth firmly in place. The junction where the crown meets the root is called the neck or cervix.
Internally, teeth are composed of several distinct layers, each with specific properties and functions:
- Enamel: The outermost, hardest layer of the crown.
- Dentin: The layer beneath the enamel and cementum, making up the bulk of the tooth.
- Cementum: The bone-like layer covering the root surface.
- Pulp: The innermost core, containing nerves, blood vessels, and connective tissue.
Surrounding the tooth are supporting structures collectively known as the periodontium, which includes the gums (gingiva), alveolar bone, and periodontal ligaments. These structures ensure the tooth remains stable and healthy within the oral cavity.
![A detailed sagittal cross-section of a human molar tooth, clearly labeling the crown, root, neck, enamel, dentin, cementum, pulp chamber(/dental-anatomy/types-of-teeth-shapes-complete-guide), root canal, apical foramen, gingiva, alveolar bone, and periodontal ligament.]
{kind=link}
External Tooth Anatomy
The external appearance of a tooth varies significantly depending on its type and location in the mouth. However, the fundamental components remain consistent.
The Crown
The crown is the portion of the tooth visible above the gum line. It's the functional part responsible for chewing and biting. Its shape is adapted to its specific role:
- Incisors: Sharp, chisel-shaped crowns for cutting food.
- Canines: Pointed, cone-shaped crowns for tearing food.
- Premolars (Bicuspids): Broad crowns with two cusps for crushing and grinding.
- Molars: The largest crowns, with multiple cusps (typically 4-5) for extensive grinding.
The outer surface of the crown is covered by enamel, the hardest substance in the human body. Enamel is primarily composed of hydroxyapatite crystals, making it incredibly durable and resistant to wear and tear. Its primary function is to protect the softer underlying dentin and pulp from bacteria, temperature changes, and physical forces during mastication. However, enamel is non-living tissue and cannot regenerate if damaged by acid erosion or decay.
The Root
The root is the hidden part of the tooth, embedded within the alveolar bone of the jaw. Its primary function is to anchor the tooth securely in the jaw and transmit chewing forces to the bone. The number of roots varies by tooth type:
- Incisors and Canines: Typically one single root.
- Premolars: Usually one or two roots.
- Molars: Two or three roots (mandibular molars usually have two, maxillary molars usually have three).
The root surface is covered by cementum, a specialized calcified tissue that is softer than enamel and dentin. Cementum serves as the attachment site for the periodontal ligament, a fibrous connective tissue that connects the tooth root to the alveolar bone. This ligament acts as a shock absorber, distributing chewing forces and allowing slight tooth movement, which is essential for healthy function.
Internal Tooth Anatomy
Delving inside the tooth reveals its living tissues and intricate structures.
Enamel (Revisited)
As discussed, enamel is the outermost protective layer of the crown. Its extreme hardness is crucial for resisting the daily stresses of chewing. Despite its strength, enamel can be demineralized by acids produced by bacteria (leading to cavities) or by acidic foods and drinks (leading to erosion). Once enamel is lost, it's gone for good, though fluoride can help remineralize weakened areas.
Dentin
Beneath the enamel and cementum lies dentin, a yellowish tissue that forms the bulk of the tooth structure. Dentin is softer than enamel but harder than bone. Unlike enamel, dentin is a living tissue, containing microscopic tubules (dentinal tubules) that extend from the pulp to the outer surface of the dentin. These tubules contain fluid and extensions of pulp cells, making dentin sensitive to temperature changes, pressure, and tactile stimuli if the overlying enamel or cementum is breached. Dentin can regenerate to some extent, forming "secondary dentin" throughout life and "tertiary dentin" in response to irritation or injury.
The Tooth Pulp Chamber and Root Canals
Deep within the dentin lies the tooth pulp chamber, the innermost and most vital part of the tooth. This central cavity houses the dental pulp, a soft, gelatinous tissue rich in blood vessels, nerves, and connective tissue. The pulp chamber is located in the crown, and it extends into the root(s) as narrow channels called root canals. Each root typically contains one or more root canals.
The pulp has several critical functions:
- Sensory: The nerves within the pulp detect pain, temperature changes (hot and cold), and pressure.
- Nutritive: Blood vessels supply nutrients to the dentin.
- Formative: Specialized cells (odontoblasts) within the pulp produce new dentin.
- Defensive: The pulp can initiate inflammatory and immune responses.
At the very tip of each root, the root canal opens into the surrounding bone through a small opening called the apical foramen. This opening allows blood vessels and nerves to enter and exit the pulp, connecting the tooth to the body's circulatory and nervous systems. When the pulp becomes infected or inflamed (e.g., due to deep decay or trauma), it can cause severe pain and may necessitate a root canal treatment to save the tooth.
Cementum (Revisited)
Cementum covers the root surface, acting as the bridge between the tooth and the bone. It's less mineralized than enamel or dentin and is susceptible to abrasion and erosion if exposed, for instance, due to gum recession. The primary function of cementum is to provide a firm anchorage for the periodontal ligament fibers, ensuring the tooth's stability.
Supporting Structures: The Periodontium
The periodontium is the specialized apparatus that supports the teeth in the jaws and includes:
- Gingiva (Gums): The soft tissue that surrounds the teeth and covers the alveolar bone. Healthy gums are pink, firm, and hug the teeth tightly, protecting the underlying structures.
- Alveolar Bone: The part of the jawbone that holds the tooth roots in place. It constantly remodels in response to forces exerted on the teeth.
- Periodontal Ligament (PDL): A fibrous connective tissue that connects the cementum of the tooth root to the alveolar bone. The PDL acts as a shock absorber during chewing, transmits sensory information, and plays a role in bone and cementum formation and resorption.
Together, these structures form a dynamic system that allows teeth to function effectively and withstand the rigors of daily use.
Types of Teeth: A Specialized Workforce
Humans typically have two sets of teeth during their lifetime: primary (deciduous or "baby") teeth and permanent (succedaneous or "adult") teeth. Each set consists of different types of teeth, each adapted for specific tasks.
Primary Dentition (20 Teeth)
Children usually have 20 primary teeth, 10 in the upper jaw and 10 in the lower jaw. These teeth are crucial for chewing, speech development, and maintaining space for the permanent teeth to erupt correctly. They are generally smaller, whiter, and have thinner enamel and dentin than permanent teeth.
- Incisors (8): Four central and four lateral incisors, for biting and cutting.
- Canines (4): For tearing food.
- Molars (8): For grinding food (note: no premolars in primary dentition).
Permanent Dentition (32 Teeth)
Adults typically have 32 permanent teeth, 16 in the upper jaw and 16 in the lower jaw. These teeth are designed to last a lifetime and perform the full range of masticatory functions.
- Incisors (8): Same function as primary incisors.
- Canines (4): Same function as primary canines.
- Premolars (Bicuspids) (8): Located between canines and molars, they help crush and grind food. These replace the primary molars.
- Molars (12): Divided into first, second, and third molars (wisdom teeth). They are the largest teeth, designed for heavy grinding. Wisdom teeth often erupt last, typically between ages 17-25, and may require extraction if impacted or causing problems.
Pro Tip: Understanding which teeth are where can help you communicate more effectively with your dentist about specific pain points or concerns. For example, "the upper right first molar" is much more precise than "a back tooth."
Children / Pediatric Considerations: The Eruption Journey
The development and eruption of teeth are critical milestones in a child's growth. Primary teeth lay the groundwork for permanent teeth and proper oral development.
Pediatric Tooth Eruption Chart
Primary teeth begin to erupt around 6-10 months of age, with the full set usually present by 2-3 years. The order of eruption is generally symmetrical and predictable.
| Tooth Type | Average Eruption Age (Months) | Average Shedding Age (Years) |
|---|---|---|
| Lower Central Incisors | 6-10 | 6-7 |
| Upper Central Incisors | 8-12 | 6-7 |
| Upper Lateral Incisors | 9-13 | 7-8 |
| Lower Lateral Incisors | 10-16 | 7-8 |
| Upper First Molars | 13-19 | 9-11 |
| Lower First Molars | 14-18 | 9-11 |
| Upper Canines | 16-22 | 10-12 |
| Lower Canines | 17-23 | 9-12 |
| Lower Second Molars | 23-31 | 10-12 |
| Upper Second Molars | 25-33 | 10-12 |
Important Note: These are average ages, and there can be significant individual variation. If you have concerns about your child's tooth development, consult a pediatric dentist.
Permanent Tooth Eruption Chart
Permanent teeth begin to replace primary teeth around age 6 and continue to erupt into early adulthood.
| Tooth Type | Average Eruption Age (Years) |
|---|---|
| First Molars | 6-7 |
| Central Incisors | 6-8 |
| Lateral Incisors | 7-9 |
| Canines (Lower) | 9-10 |
| First Premolars | 9-11 |
| Second Premolars | 10-12 |
| Canines (Upper) | 11-12 |
| Second Molars | 11-13 |
| Third Molars (Wisdom) | 17-25 |
ADA Recommendation: The American Dental Association recommends a child's first dental visit by their first birthday or within six months of the first tooth's eruption. Early dental care helps establish good habits and allows for early detection of any developmental issues.
Causes / Why Anatomical Issues Happen
While the basic tooth anatomy is a fixed biological structure, various factors can compromise its integrity and lead to dental problems. Understanding these "causes" helps in prevention and targeted treatment.
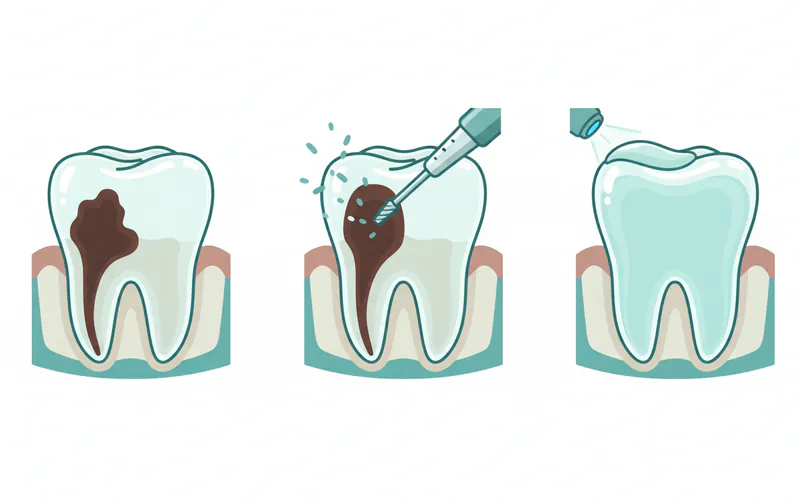
Dental Caries (Cavities)
This is the most common reason for anatomical damage. Bacteria in the mouth feed on sugars and produce acids that demineralize enamel. If left untreated, this erosion progresses through the enamel into the dentin, creating a cavity. Once decay reaches the tooth pulp chamber, it can lead to infection, severe pain, and potentially an abscess.
Erosion
Acidic foods, drinks, or medical conditions (e.g., acid reflux, bulimia) can directly dissolve tooth enamel and dentin without bacterial involvement. This "acid erosion" thins the protective layers, making teeth sensitive and vulnerable to further damage.
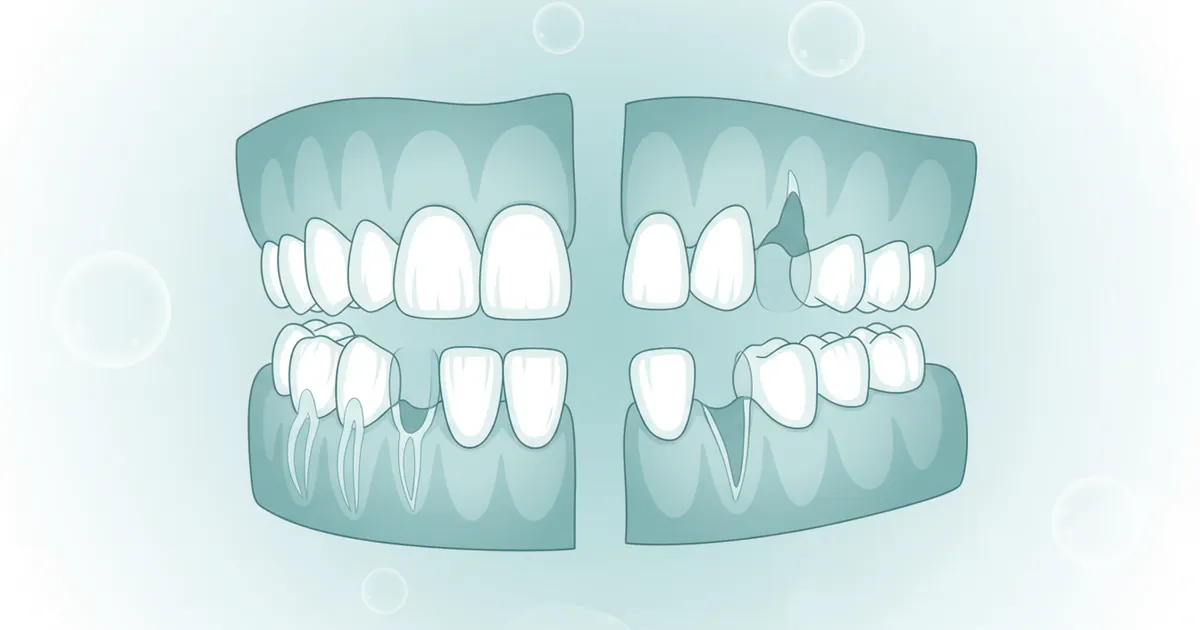
Trauma
Physical impact to the face can fracture or chip tooth enamel, dentin, or even the root. Trauma can also dislodge a tooth or damage its internal pulp, even if the external structure appears intact.
Abrasion and Attrition
- Abrasion: Wear of tooth structure caused by external forces, such as aggressive brushing with a hard-bristled toothbrush or using abrasive toothpastes.
- Attrition: Wear caused by tooth-to-tooth contact, often due to clenching, grinding (bruxism), or malocclusion. This can flatten biting surfaces and expose underlying dentin.
Gum Recession
Loss of gum tissue and underlying bone can expose the root surface, which is covered by softer cementum. Exposed roots are more sensitive to hot, cold, and touch, and are more prone to decay and abrasion.
Developmental Anomalies
Sometimes, teeth don't form correctly. Examples include:
- Amelogenesis Imperfecta: Enamel doesn't form properly, leading to soft, easily damaged teeth.
- Dentinogenesis Imperfecta: Dentin doesn't form properly, leading to brittle teeth.
- Hypoplasia: Patches of thin or missing enamel due to disturbances during tooth development.
Signs and Symptoms of Anatomical Damage
Recognizing the signs of compromised tooth anatomy is crucial for early intervention and preventing more severe issues.
- Sensitivity: Pain or discomfort when consuming hot, cold, sweet, or acidic foods and drinks. This often indicates exposed dentin due to decay, erosion, gum recession, or enamel cracks.
- Toothache: Persistent or throbbing pain, especially when biting or at night. This is a strong indicator that decay has reached the tooth pulp chamber, causing inflammation or infection.
- Visible Holes or Pits: A clear sign of a cavity, indicating enamel and dentin breakdown.
- Discoloration: Dark spots on the tooth surface can indicate decay. White spots can be an early sign of demineralization.
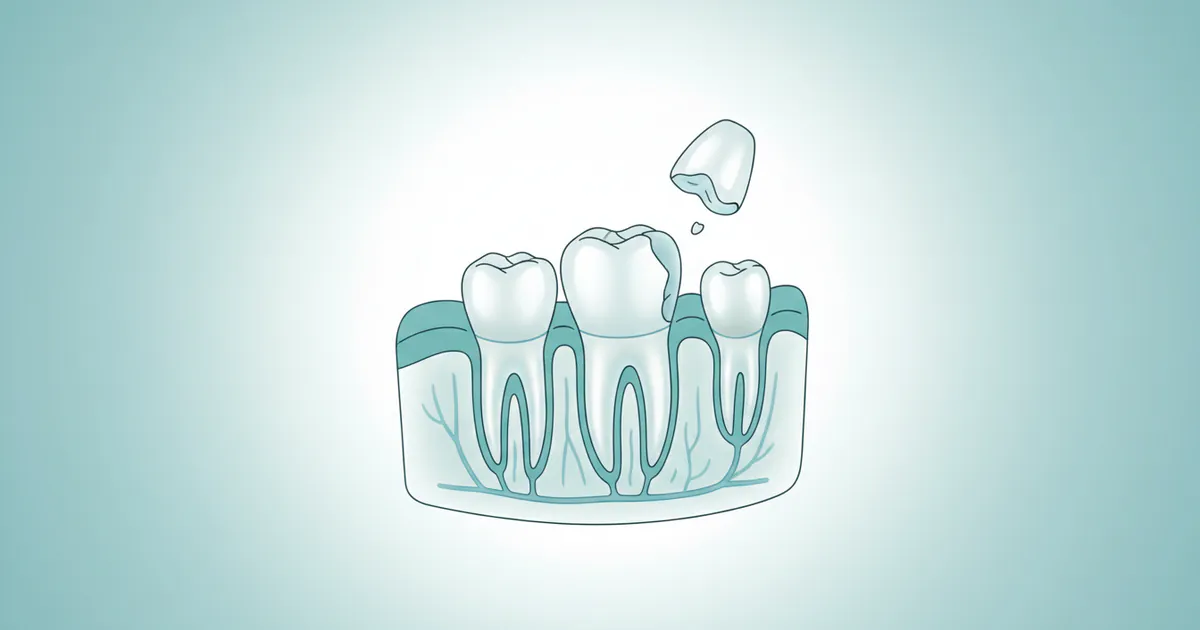
- Chipped or Fractured Tooth: Visible breaks in the enamel or dentin, often from trauma or biting on something hard.
- Swelling or Redness around the Gums: Can indicate an abscess stemming from an infected pulp or gum disease affecting supporting structures.
- Bad Breath (Halitosis): Can be a symptom of severe decay or gum disease.
- Loose Tooth: Indicates significant damage to the periodontal ligament or alveolar bone, often due to advanced gum disease or trauma.
Treatment Options for Compromised Anatomy
Treatment focuses on restoring the tooth's structure, function, and aesthetics, as well as addressing any underlying infection.
1. Fillings
- Purpose: To repair small to moderate cavities that affect enamel and dentin.
- Process: The dentist removes decayed tooth structure and fills the cavity with a restorative material.
- Materials:
- Amalgam (Silver) Fillings: Durable, cost-effective, but not aesthetically pleasing.
- Composite (Tooth-Colored) Fillings: Esthetically pleasing, bond directly to the tooth, but may be less durable for very large restorations.
- Glass Ionomer Fillings: Release fluoride, good for small cavities or temporary restorations, less durable.
- Pros: Restores tooth function, prevents further decay, relatively quick procedure.
- Cons: Not suitable for large defects, potential for sensitivity post-procedure.
2. Dental Crowns
- Purpose: To restore extensively damaged teeth, protecting them from further fracture, or for aesthetic improvement. Often used after a root canal to strengthen the tooth.
- Process: The tooth is reshaped, an impression is taken, and a custom-made cap (crown) is fabricated and permanently cemented over the entire visible portion of the tooth.
- Materials: Porcelain, ceramic, metal alloys (gold, silver), porcelain-fused-to-metal (PFM), zirconia.
- Pros: Restores strength, function, and appearance; protects weakened teeth.
- Cons: Requires removal of healthy tooth structure, can be costly, multiple appointments usually needed.
3. Root Canal Treatment (Endodontic Therapy)
- Purpose: To save a tooth when the tooth pulp chamber or root canals are infected or severely inflamed.
- Process: The infected pulp is removed from the pulp chamber and root canals, the canals are cleaned, shaped, and then filled with a biocompatible material (gutta-percha). The tooth is then sealed, usually with a crown.
- Pros: Saves the natural tooth, prevents extraction, eliminates pain and infection.
- Cons: Can be multiple appointments, tooth may become brittle and require a crown, potential for re-infection (rare).
4. Extractions
- Purpose: Removal of a tooth that is beyond repair due to severe decay, trauma, infection, or overcrowding (e.g., problematic wisdom teeth).
- Process: The tooth is carefully loosened from its socket and removed.
- Pros: Eliminates source of infection/pain.
- Cons: Creates a gap that can lead to shifting teeth, bone loss, and functional issues; often requires subsequent treatment like implants or bridges.
5. Veneers and Bonding
- Purpose: Primarily aesthetic solutions for chipped, discolored, or slightly misaligned front teeth, affecting the enamel layer.
- Veneers: Thin, custom-made shells (porcelain or composite) bonded to the front surface of teeth.
- Bonding: A tooth-colored resin applied and shaped directly to the tooth, then hardened with a special light.
- Pros: Greatly improves appearance, can address minor anatomical imperfections.
- Cons: Veneers are irreversible and costly; bonding is less durable than veneers.
Comparison Table: Common Restorative Procedures
| Procedure | Primary Indication | Average US Cost (Without Insurance) | Duration of Treatment | Longevity |
|---|---|---|---|---|
| Composite Filling | Small to moderate cavities | $100 - $400 | 1 appointment | 5-10 years |
| Amalgam Filling | Moderate to large posterior cavities | $100 - $300 | 1 appointment | 10-15 years |
| Dental Crown | Extensive damage, post-root canal | $800 - $3,000 | 2-3 appointments | 10-15+ years |
| Root Canal | Infected pulp (pulp chamber/canals) | $700 - $1,500 (front) | 1-2 appointments | Lifelong (with crown) |
| $1,000 - $2,000 (back) | ||||
| Extraction | Non-restorable tooth | $75 - $200 (simple) | 1 appointment | Permanent |
| $200 - $600 (surgical) |
Step-by-Step Process: What to Expect During a Filling
Let's walk through a common procedure like a composite filling to understand how anatomical issues are addressed.
- Diagnosis: Your dentist uses X-rays and a visual exam to identify decay in the enamel or dentin.
- Anesthesia: A local anesthetic is administered to numb the tooth and surrounding area, ensuring a pain-free experience.
- Decay Removal: The dentist uses a high-speed dental drill to carefully remove all decayed and weakened tooth structure. This step is critical to prevent the decay from progressing further towards the tooth pulp chamber.
- Cavity Preparation: The prepared cavity is shaped to receive the filling material and ensure a strong bond.
- Etching and Bonding (for Composite): For composite fillings, an etching gel is applied to microscopically roughen the enamel and dentin surface, followed by a bonding agent. This creates a strong adhesive surface for the composite resin.
- Filling Application: The tooth-colored composite resin is applied in layers, with each layer cured (hardened) by a special blue light. This allows the dentist to sculpt the material to match the tooth's natural contours.
- Shaping and Polishing: Once all layers are applied and hardened, the dentist meticulously shapes the filling to ensure proper bite alignment and smooth margins. The filling is then polished to a natural luster.
- Final Check: Your bite is checked, and any necessary adjustments are made. The entire process for a simple filling typically takes 30-60 minutes.
Cost and Insurance
The cost of dental treatments to restore or manage compromised tooth anatomy varies widely based on several factors:
- Type of Procedure: As seen in the table above, simple fillings are far less expensive than root canals or crowns.
- Material Used: Porcelain crowns are more expensive than metal crowns; composite fillings generally cost more than amalgam.
- Location: Costs can vary significantly by state, city, and even neighborhood. Dental care in metropolitan areas tends to be higher.
- Dentist's Fees: Specialist dentists (e.g., endodontists for root canals) may charge more than general dentists.
- Complexity: A simple filling in an easily accessible tooth is cheaper than a complex restoration on a molar with multiple root canals.
Average US Cost Ranges (Without Insurance)
- Composite Fillings: $100 - $400 per tooth
- Amalgam Fillings: $100 - $300 per tooth
- Dental Crowns: $800 - $3,000 per tooth (can be higher for specialized materials)
- Root Canal (front tooth): $700 - $1,500
- Root Canal (molar): $1,000 - $2,000
- Simple Extraction: $75 - $200
- Surgical Extraction: $200 - $600
- Dental Veneers (composite): $250 - $1,500 per tooth
- Dental Veneers (porcelain): $900 - $2,500 per tooth
Insurance Coverage Details
Most US dental insurance plans categorize services into:
- Preventive Care (e.g., check-ups, cleanings, X-rays): Typically covered at 80-100%.
- Basic Procedures (e.g., fillings, simple extractions): Usually covered at 50-80% after a deductible.
- Major Procedures (e.g., crowns, root canals, bridges, dentures): Often covered at 0-50% after a deductible, and may have waiting periods (e.g., 6-12 months before major work is covered).
Key Points on Insurance:
- Deductible: An amount you must pay out-of-pocket before your insurance begins to cover costs.
- Annual Maximum: The maximum amount your insurance will pay for dental care in a plan year. This often ranges from $1,000 to $2,000.
- In-network vs. Out-of-network: You'll typically pay less for services from dentists within your insurance company's network.
Pro Tip: Always call your insurance provider directly or check their online portal to understand your specific plan benefits, deductibles, annual maximums, and coverage percentages for different procedures before starting treatment.
Payment Plans and Financing Options
For significant out-of-pocket costs, many dental offices offer:
- In-house Payment Plans: Installment plans directly with the dental office.
- Third-Party Financing (e.g., CareCredit, LendingClub): Healthcare-specific credit cards or loans that often offer interest-free periods if paid in full within a certain timeframe.
- Dental Schools: Can offer lower-cost treatment provided by students under faculty supervision.
- Community Dental Clinics: May provide care on a sliding scale based on income.
Recovery and Aftercare
Recovery and aftercare depend entirely on the type of procedure performed to address the anatomical issue.
- Fillings:
- Recovery: Numbness usually wears off within 1-3 hours. Avoid chewing on the filled tooth until the numbness subsides to prevent accidental biting of the cheek or tongue.
- Aftercare: Some sensitivity to hot/cold for a few days is normal. Maintain regular oral hygiene. If sensitivity persists or worsens, contact your dentist.
- Crowns:
- Recovery: Temporary crown may be placed initially. Avoid sticky or hard foods on the temporary crown. Sensitivity is common until the permanent crown is placed.
- Aftercare: Once the permanent crown is cemented, treat it like a natural tooth. Brush and floss daily, paying special attention to the gum line around the crown. Regular dental check-ups are vital to monitor the crown's integrity and surrounding gum health.
- Root Canal Treatment:
- Recovery: Some soreness or mild pain for a few days, managed with over-the-counter pain relievers.
- Aftercare: Avoid chewing on the treated tooth until a permanent restoration (usually a crown) is placed to prevent fracture. Maintain excellent oral hygiene.
- Extractions:
- Recovery: Bleeding control (bite on gauze), pain management (prescribed or OTC pain relievers), swelling reduction (ice packs), and prevention of "dry socket" (avoid spitting, straws, smoking for 24-48 hours).
- Aftercare: Soft diet for a few days, gentle brushing around the site, warm salt water rinses after 24 hours. Follow all post-operative instructions carefully.
General Aftercare Principles:
- Maintain Excellent Oral Hygiene: Brush twice daily with fluoride toothpaste, floss once daily.
- Avoid Habits that Damage Teeth: Limit sugary snacks and acidic drinks, avoid chewing ice, pens, or using teeth as tools.
- Regular Dental Check-ups: Visit your dentist every six months for professional cleanings and examinations to detect issues early.
Prevention: Protecting Your Tooth Anatomy
Preventing damage to your tooth anatomy is the cornerstone of good oral health.
- Brush Twice Daily: Use a soft-bristled toothbrush and fluoride toothpaste for two minutes each time. The ADA Seal of Acceptance ensures products meet safety and efficacy standards.
- Floss Daily: Flossing removes plaque and food particles from between teeth and under the gum line, areas your toothbrush can't reach, preventing decay and gum disease that can compromise supporting structures.
- Use Fluoride: Fluoride strengthens enamel, making it more resistant to acid attacks. Most tap water in the US is fluoridated. Your dentist may also recommend fluoride rinses or professional fluoride treatments.
- Limit Sugary and Acidic Foods/Drinks: These contribute significantly to enamel demineralization and decay. If consumed, do so in moderation and rinse with water afterward.
- Regular Dental Check-ups and Cleanings: Professional cleanings remove hardened plaque (tartar) that brushing can't. Dentists can identify early signs of decay, gum disease, or other issues before they become severe.
- Dental Sealants: For children and sometimes adults, sealants can be applied to the chewing surfaces of molars and premolars. These thin, protective coatings fill in the pits and fissures of the enamel, preventing food and bacteria from getting trapped and causing cavities.
- Wear a Mouthguard: If you play contact sports or grind/clench your teeth at night (bruxism), a custom-fitted mouthguard protects your teeth from trauma and excessive wear.
- Avoid Using Teeth as Tools: Don't use your teeth to open bottles, tear packages, or cut thread, as this can lead to chips, cracks, or fractures.
Risks and Complications
Despite the best care, dental procedures and conditions affecting tooth anatomy can sometimes have risks or complications.
Complications from Untreated Anatomical Issues:
- Spread of Infection: Untreated decay or pulp infection can spread to other teeth, the jawbone, or even into the bloodstream, leading to serious systemic health issues.
- Tooth Loss: Severe decay, trauma, or gum disease can lead to irreversible damage, necessitating extraction.
- Abscess Formation: A pocket of pus at the root tip due to untreated pulp infection, causing severe pain and swelling.
- Periodontal Disease: If the supporting structures (gums, bone, PDL) are compromised, teeth can loosen and eventually fall out.
- Malocclusion/Shifting Teeth: Gaps from missing teeth or uneven wear can cause adjacent teeth to shift, affecting bite and alignment.
Risks from Dental Treatments:
- Sensitivity: Common after fillings or crowns, usually temporary but can persist.
- Nerve Damage: Rare, but can occur during extractions or root canals, leading to numbness or altered sensation.
- Re-infection: Though rare, a root canal treated tooth can sometimes become re-infected, requiring retreatment or extraction.
- Fracture: A tooth treated with a root canal can be more brittle and prone to fracture if not crowned properly. Fillings, especially large ones, can also sometimes fail or fracture.
- Allergic Reaction: To materials used (e.g., metals in fillings/crowns, latex in gloves), though modern materials are generally biocompatible.
- Dry Socket: A painful condition after tooth extraction where the blood clot fails to form or dislodges, exposing the bone.

ADA Guideline: The ADA regularly updates its recommendations and best practices to minimize risks and ensure patient safety and effective treatment outcomes. Following these guidelines is standard practice for qualified dental professionals.
Cost Breakdown: A Detailed Look
Let's summarize and expand on the cost aspects, focusing on typical US scenarios.
Average US Costs (Low, Mid, High)
Costs are highly variable. Here's a general breakdown for common procedures related to anatomical repairs:
| Procedure | Low End (USD) | Mid Range (USD) | High End (USD) |
|---|---|---|---|
| Composite Filling | $100 | $250 | $400 |
| Amalgam Filling | $100 | $200 | $300 |
| Porcelain Crown | $800 | $1,500 | $3,000 |
| Zirconia Crown | $1,000 | $2,000 | $3,500 |
| Root Canal (Anterior) | $700 | $1,000 | $1,500 |
| Root Canal (Molar) | $1,000 | $1,500 | $2,000 |
| Simple Extraction | $75 | $125 | $200 |
| Surgical Extraction | $200 | $400 | $600 |
These ranges represent costs without insurance. Geographic location is a major factor, with major cities often on the higher end.
With vs. Without Insurance
Let's consider a hypothetical scenario for a single procedure, a porcelain crown on a molar, costing $1,500.
- Without Insurance: You pay the full $1,500.
- With Insurance (example):
- Annual Deductible: $50 (you pay this first)
- Insurance Coverage (Major Procedures): 50%
- Your Out-of-Pocket Cost: $50 (deductible) + (50% of $1,450 remaining) = $50 + $725 = $775
- If you've already met your deductible, you would only pay the 50% co-insurance, so $750.
- Important: This is also subject to your annual maximum. If you've already hit your $1,500 annual maximum for the year, insurance won't pay anything further.
Payment Plans and Financing Options
- CareCredit/LendingClub: Offer special financing options, including 0% interest for 6, 12, 18, or 24 months for qualified applicants, if the balance is paid in full by the end of the promotional period. Be aware of deferred interest.
- In-Office Plans: Many practices offer customized payment schedules. Don't hesitate to ask their front office staff about options.
- Health Savings Accounts (HSAs) & Flexible Spending Accounts (FSAs): If you have one of these, you can use pre-tax dollars to pay for dental care, saving you money on taxes.
Cost-Saving Tips
- Preventive Care: The best way to save money is to prevent problems. Regular check-ups and cleanings cost very little compared to restorative work.
- Compare Plans: If you're choosing a dental insurance plan, compare premiums, deductibles, annual maximums, and coverage percentages for procedures you anticipate.
- Ask for Estimates: Always get a detailed estimate of costs from your dentist before starting treatment, including what your insurance is expected to cover.
- Community Clinics/Dental Schools: These can offer significantly lower costs, though wait times might be longer.
- Generic Drugs: If prescribed medication (e.g., antibiotics, pain relievers), ask your dentist if a generic option is available.
Frequently Asked Questions
What is the hardest part of a tooth?
The hardest part of a tooth is the enamel, which covers the crown. It is the most mineralized substance in the human body, even harder than bone, designed to withstand the immense forces of chewing and protect the inner layers.
Why is the tooth pulp chamber so important?
The tooth pulp chamber is vital because it houses the dental pulp, which contains the tooth's nerves, blood vessels, and connective tissue. It's responsible for tooth sensation (like hot, cold, and pain), provides nutrients to the surrounding dentin, and helps form new dentin throughout life.
How many teeth do children have, and when do they get their adult teeth?
Children typically have 20 primary (baby) teeth, which usually finish erupting by age 2-3. They start losing these primary teeth and gaining permanent (adult) teeth around age 6, a process that continues until early adulthood, resulting in 32 permanent teeth (including wisdom teeth).
What is the purpose of a pediatric tooth eruption chart?
A pediatric tooth eruption chart helps parents and dentists track the normal development of a child's primary and permanent teeth. It provides average timelines for when each tooth is expected to emerge, helping to identify potential delays or abnormalities that may require dental attention.
Can a damaged tooth regenerate itself?
The enamel cannot regenerate once damaged. However, the dentin, being a living tissue, can produce "secondary dentin" throughout life and "tertiary dentin" in response to irritation or mild injury, helping to protect the pulp. The pulp itself cannot regenerate if severely damaged or infected.
What are the main differences between primary and permanent teeth?
Primary teeth are smaller, whiter, and have thinner enamel and dentin compared to permanent teeth. They also have relatively larger pulp chambers. Primary teeth serve as placeholders for permanent teeth and are eventually shed, while permanent teeth are designed to last a lifetime.
How much does a root canal typically cost, and is it painful?
A root canal typically costs between $700 and $2,000 without insurance, depending on the tooth's location and complexity. The procedure itself is performed under local anesthesia, so it should not be painful. Post-procedure soreness is common and can be managed with over-the-counter pain medication.
What causes tooth sensitivity, and how can it be treated?
Tooth sensitivity is often caused by exposed dentin, which can result from enamel erosion, gum recession, decay, or cracks. It can be treated with desensitizing toothpastes, fluoride varnishes, dental bonding, gum grafts (for recession), or fillings/crowns to cover exposed areas.
What is the role of cementum, and why is it important?
Cementum is a bone-like tissue covering the root surface. Its primary role is to anchor the periodontal ligament fibers, which connect the tooth to the surrounding jawbone. This attachment system provides stability for the tooth and acts as a shock absorber during chewing.
Are wisdom teeth considered part of normal tooth anatomy?
Yes, wisdom teeth (third molars) are part of the normal human permanent dentition, making up the full count of 32 teeth. However, due to evolutionary changes in jaw size, they often don't have enough space to erupt properly and may cause issues, leading to their common extraction.
When to See a Dentist
Your teeth are remarkable structures, but they are not invincible. Knowing when to seek professional dental care is critical for preserving their anatomy and your overall health.
Red Flags (Seek Immediate Dental Attention - Emergency):
- Severe, persistent toothache: Especially if it wakes you up at night, throbs, or is accompanied by swelling. This often indicates a deep infection of the tooth pulp chamber.
- Swelling in your face, jaw, or neck: Can be a sign of a spreading dental infection or abscess.
- Knocked-out tooth (avulsed tooth): Time is critical for re-implantation.
- Sudden loosening of a tooth: Could indicate trauma or severe gum disease.
- Pain or difficulty opening your mouth: May signal infection or temporomandibular joint (TMJ) issues.
- Bleeding that won't stop after an extraction or injury.
Warning Signs (Schedule a Dental Appointment Promptly - Non-Emergency but Important):
- Increased tooth sensitivity to hot, cold, or sweets that doesn't go away.
- Visible holes or pits (cavities) in your teeth.
- Chipped, cracked, or fractured tooth: Even if not painful, it can lead to further damage or infection.
- Persistent bad breath or a bad taste in your mouth: Could indicate gum disease or decay.
- Red, swollen, or bleeding gums: Signs of gingivitis or periodontitis, which can compromise the tooth's supporting structures.
- Pain when chewing or biting down: May indicate a cracked tooth, a loose filling, or a bite problem.
- A "gummy" smile or receding gums: Indicates potential root exposure and increased sensitivity.
Routine Care (Scheduled Appointments):
- Regular dental check-ups and cleanings: Every six months, or as recommended by your dentist, is crucial for preventing issues and detecting problems early.
- Questions about oral hygiene: If you're unsure about brushing or flossing techniques.
- Concerns about cosmetic appearance: For aesthetic enhancements like veneers or bonding.
Never ignore persistent pain or unusual symptoms in your mouth. Your dental health professional is your best resource for maintaining healthy teeth and gums, ensuring the intricate tooth anatomy labeled within your mouth serves you well for a lifetime.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Tooth Eruption Order: Complete Guide
The journey of human teeth, from their initial emergence in infancy to the arrival of wisdom teeth in young adulthood, is a fascinating and crucial aspect of our overall health. Understanding the tooth eruption order is not just a matter of curiosity; it's a vital piece of knowledge that empower
February 23, 2026

Primary Tooth Eruption Sequence: Complete Guide
Did you know that by their third birthday, most children will have a full set of 20 primary teeth? The journey of these first teeth, from their initial appearance to their eventual replacement by permanent teeth, is a remarkable and often challenging milestone for both infants and parents. Understan
February 23, 2026
Canine Tooth Eruption: Complete Guide
Have you ever wondered about the complex process that brings your teeth into alignment, especially the prominent, pointed teeth known as canines? While often overshadowed by discussions of wisdom teeth or incisors, the canine tooth eruption process is a critical stage in your oral development, d
February 23, 2026

Permanent Tooth Eruption Sequence: Complete Guide
Welcome to SmilePedia.net, your trusted resource for comprehensive dental health information. The journey of your permanent teeth emerging into your mouth, known as the permanent tooth eruption sequence, is a fundamental aspect of oral development. Did you know that while primary (baby) teeth ty
February 23, 2026