Baby Snoring: Complete Guide

Key Takeaways
- Few sounds can be as alarming to new parents as the unexpected noises their baby makes during sleep. While coos and gentle breaths are reassuring, a snorting or rattling sound can quickly send parents into a spiral of worry. Studies suggest that **up to 27% of infants may experience some form of sno
Baby Snoring: Complete Guide
Few sounds can be as alarming to new parents as the unexpected noises their baby makes during sleep. While coos and gentle breaths are reassuring, a snorting or rattling sound can quickly send parents into a spiral of worry. Studies suggest that up to 27% of infants may experience some form of snoring, making it a common, yet often misunderstood, phenomenon. While occasional baby snoring can be a normal part of their developing respiratory system, it can also be a red flag for underlying health issues, including sleep-disordered breathing. Understanding the difference between benign noisy breathing and concerning symptoms is crucial for your child's immediate health and long-term development.

This comprehensive guide from SmilePedia.net will demystify baby snoring, covering everything from its common causes and potential risks to diagnosis, treatment options, and preventive strategies. We'll delve into what to watch for, when to seek professional medical advice, and how to ensure your little one breathes easily and sleeps soundly.
Key Takeaways:
- Common Occurrence: Up to 27% of infants experience snoring, often benign and due to temporary congestion or narrow airways.
- Red Flags: Persistent, loud snoring, gasping, pauses in breathing, restless sleep, mouth breathing, daytime irritability, or difficulty feeding warrant immediate medical evaluation.
- Diagnosis: A pediatrician is the first step, often followed by an ENT or pediatric sleep specialist. A pediatric sleep study (polysomnography) is the gold standard for diagnosing sleep apnea.
- Treatment Variety: Ranges from simple home remedies (humidifiers, nasal saline) to medical interventions (allergy meds) or surgical procedures (adenotonsillectomy, costing $3,000-$8,000 without insurance).
- Snoring Mouth Guards: Generally not appropriate for infants or toddlers; primarily designed for older children or adults with fully developed dentition and jaw structures.
- Untreated Risks: Chronic snoring, especially with sleep apnea, can lead to developmental delays, behavioral issues, cardiovascular problems, and poor growth.
- Insurance Coverage: Most diagnostic tests and medically necessary treatments for sleep apnea in children are covered by insurance, though deductibles and co-pays apply.
What It Is / Overview
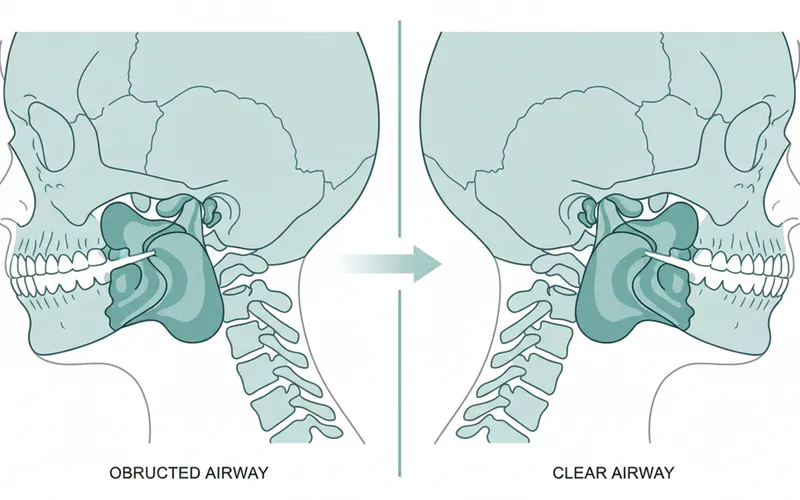
Snoring in infants, like in adults, occurs when the flow of air through the mouth and nose is partially obstructed during sleep, causing the soft tissues in the airway to vibrate. Unlike the robust, deep snores often associated with adults, newborn snoring or infant snoring might present as a softer, whistling, gurgling, or rattling sound. This noise is typically produced during inhalation, but can sometimes be heard on exhalation as well.
A baby's airway is significantly smaller and more flexible than an adult's, making it more susceptible to even minor obstructions. This sensitivity explains why relatively minor issues, such as a stuffy nose from a common cold or even certain sleep positions, can lead to noticeable snoring. It's important for parents to differentiate between occasional, light snoring that is often benign, and chronic, loud snoring accompanied by other concerning symptoms, which could indicate a more serious condition like pediatric obstructive sleep apnea (POSA).
Understanding the anatomy involved helps clarify why snoring happens. Air travels from the nostrils and mouth through the pharynx (throat) down to the larynx (voice box) and into the trachea (windpipe). Any narrowing or blockage along this path – whether due to enlarged tissues, congestion, or structural abnormalities – can disrupt smooth airflow and cause the characteristic vibrating sound.
Types / Variations of Baby Snoring
While snoring itself is a single phenomenon, it can manifest in different ways and be categorized by its underlying cause or severity. For infants, we primarily distinguish between primary snoring and snoring associated with sleep-disordered breathing.
Primary Snoring (Benign Snoring)
This refers to snoring that occurs without any significant pauses in breathing, gasping, or other signs of disrupted sleep or oxygen deprivation. It's often:
- Occasional: Happens sporadically, perhaps during a cold or when sleeping in a particular position.
- Mild to Moderate: The sound is not excessively loud or disturbing.
- No Associated Symptoms: The baby appears well-rested, grows normally, and shows no signs of daytime fatigue or irritability.
Common causes of primary snoring include temporary nasal congestion from allergies or a cold, dry air, or the natural narrowness and flexibility of an infant's airway. In these cases, the snoring is generally not a cause for alarm and often resolves on its own.
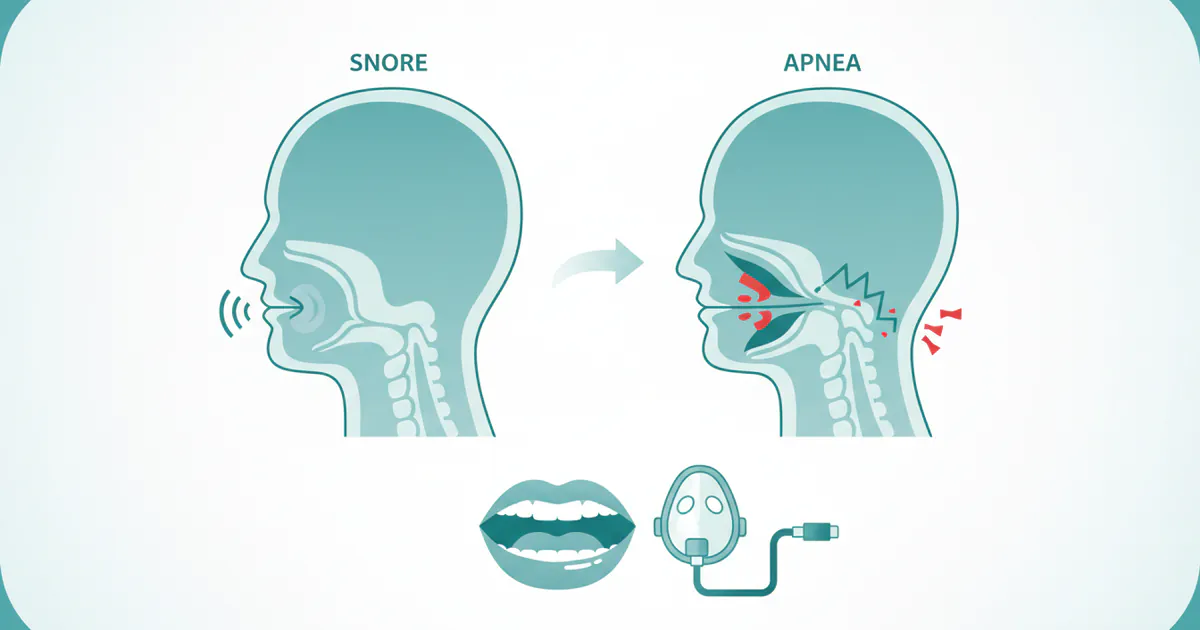
Snoring Associated with Sleep-Disordered Breathing (SDB)
This category is more concerning and includes conditions where snoring is a symptom of more significant airway obstruction or disruption to breathing during sleep. The most common and serious form of SDB in children is Obstructive Sleep Apnea Syndrome (OSAS).
- Obstructive Sleep Apnea Syndrome (OSAS): Characterized by recurrent episodes of partial or complete upper airway obstruction during sleep, leading to reduced airflow and often brief awakenings or oxygen desaturation. In infants, OSAS can be subtle but has significant health implications.
- Upper Airway Resistance Syndrome (UARS): A milder form of SDB where there's increased effort required to breathe against resistance in the upper airway, without full apnea episodes or significant oxygen drops. It can still lead to fragmented sleep and daytime symptoms.
Snoring in these cases is typically:
- Persistent and Loud: Occurs almost every night and is often quite audible.
- Accompanied by Other Symptoms: Pauses in breathing (apneas), gasping, snorting, restless sleep, mouth breathing, sweating, and daytime consequences like irritability, hyperactivity, or feeding difficulties.
- Chronic: Doesn't resolve quickly and may worsen over time if untreated.
It is critical for parents to recognize the distinction between benign primary snoring and snoring that signals SDB, as the latter requires prompt medical evaluation and intervention.
Causes / Why It Happens
The causes of baby snoring are diverse, ranging from temporary, benign factors to more serious underlying medical conditions. Understanding these causes is the first step toward appropriate management.
Common and Often Benign Causes
- Nasal Congestion: The most frequent cause of newborn snoring and infant snoring.
- Common Cold: Viral infections can cause swelling of nasal passages and increased mucus production, temporarily blocking airflow.
- Allergies: Exposure to allergens (dust mites, pet dander, pollen) can inflame nasal tissues, leading to congestion.
- Dry Air: A dry environment can irritate nasal passages, causing them to dry out and potentially swell, leading to noisy breathing.
- Small Airway Anatomy: Infants naturally have smaller, more flexible airways compared to older children and adults. This makes them more prone to partial obstruction.
- Laryngomalacia: A common congenital condition where the larynx (voice box) is softer than usual at birth. During inhalation, the soft cartilage collapses inward, partially blocking the airway. This often presents as a high-pitched "stridor" sound, but can also contribute to snoring. It usually improves as the baby matures.
- Sleep Position: Sleeping on the back is recommended to reduce SIDS risk, but sometimes certain positions can contribute to snoring. For example, the head position might slightly constrict the airway.
- Mucus and Secretions: Normal mucus buildup in the nasal passages or throat can cause a rattling or gurgling sound as air passes through.
More Significant Causes (Potentially Leading to Sleep Apnea)
- Enlarged Adenoids and Tonsils: This is the most common cause of obstructive sleep apnea in children. Adenoids are lymphoid tissues located at the back of the nasal cavity, and tonsils are at the back of the throat. When these tissues become enlarged (often due to recurrent infections or simply being naturally large), they can physically block the upper airway during sleep, particularly when muscles relax.
- Obesity: While less common in infants, childhood obesity is a growing concern and can contribute to sleep apnea in older toddlers and children. Excess fat deposits in the neck area can narrow the airway.
- Craniofacial Abnormalities: Certain birth defects affecting the jaw, palate, or skull can lead to a smaller or abnormally shaped airway, increasing the risk of obstruction. Examples include Pierre Robin sequence, Down syndrome, and Apert syndrome.
- Neuromuscular Disorders: Conditions that affect muscle tone, such as cerebral palsy, can lead to poor muscle control in the airway, making it more prone to collapse during sleep.
- Gastroesophageal Reflux Disease (GERD): Acid reflux can irritate the airways, leading to inflammation and swelling, which can contribute to snoring and breathing difficulties.
- Allergies and Asthma: Chronic allergic inflammation can lead to persistent swelling of nasal and throat tissues, contributing to chronic snoring and potentially exacerbating sleep apnea.
- Deviated Septum: A displacement of the wall between the nostrils can block airflow on one side, though this is less commonly a primary cause of significant snoring in infants unless severe.
Pro Tip: Keep a detailed log of your baby's snoring patterns, including how often it occurs, how loud it is, and any associated symptoms like pauses in breathing or restless sleep. This information will be invaluable for your pediatrician.
Signs and Symptoms
Beyond the sound of snoring itself, several other signs and symptoms can indicate whether your baby's noisy breathing is benign or points to a more serious underlying issue like sleep apnea. It's crucial for parents to observe their child closely during sleep and awake hours.
Sleep-Related Symptoms
- Loud, Persistent Snoring: If the snoring is consistently loud, occurs most nights, and doesn't resolve with simple remedies, it's a red flag.
- Pauses in Breathing (Apneas): This is perhaps the most critical symptom. You might observe your baby stopping breathing for 5-10 seconds or longer, followed by a gasp, snort, or a startled awakening.
- Gasping or Choking Sounds: These indicate the baby is struggling to overcome an airway obstruction.
- Restless Sleep: Frequent tossing and turning, unusual sleep positions (e.g., hyperextending the neck to open the airway), or waking up multiple times during the night.
- Mouth Breathing: Consistently breathing through the mouth during sleep, even when not congested, can indicate nasal obstruction.
- Excessive Sweating: Babies with sleep apnea often sweat profusely around the head and neck during sleep due to the increased effort required for breathing.
- Cyanosis: A bluish tint to the lips or skin during a breathing pause is an emergency and requires immediate medical attention.
Daytime Symptoms
- Daytime Sleepiness: Despite sleeping for adequate hours, the baby might appear excessively tired, fall asleep easily during feeds or play, or be difficult to rouse.
- Irritability and Hyperactivity: In infants and toddlers, chronic sleep deprivation can manifest as behavioral issues rather than typical tiredness. They might be unusually fussy, clingy, or paradoxically, hyperactive and difficult to calm.
- Difficulty Feeding: Problems with latching, frequent pauses during feeding, or poor coordination between sucking and swallowing can be a sign of airway issues.
- Poor Weight Gain/Failure to Thrive: The increased effort of breathing during sleep burns extra calories, and disrupted sleep can interfere with hormone regulation critical for growth.
- Nasal Speech or Chronic Congestion: Persistent nasal obstruction can lead to a "nasal" sounding voice and frequent colds or allergy-like symptoms.
- Developmental Delays: Untreated sleep apnea can have long-term impacts on cognitive development, speech, and motor skills due to chronic oxygen deprivation and sleep fragmentation.
Comparison Table: Benign vs. Concerning Baby Snoring
| Characteristic | Benign Snoring (Primary Snoring) | Concerning Snoring (Potential SDB/OSAS) |
|---|---|---|
| Frequency | Occasional, intermittent (e.g., during a cold) | Persistent, almost every night |
| Loudness | Mild to moderate, soft whistling or gurgling | Loud, often disturbing, can be heard from another room |
| Breathing Pauses | Absent | Present, often followed by gasp/snort (5-10+ seconds) |
| Sleep Quality | Appears restful, wakes refreshed | Restless, frequent awakenings, unusual positions, excessive sweating |
| Daytime Behavior | Normal, playful, alert | Irritable, fussy, hyperactive, sleepy, difficulty concentrating |
| Feeding | Normal feeding, good weight gain | Difficulty feeding, poor weight gain, slow growth |
| Associated Sounds | Occasional sniffles, quiet breathing when awake | Gasping, choking, struggling breaths, chronic mouth breathing |
| Urgency for Evaluation | Monitor, try home remedies | Prompt medical evaluation (pediatrician, ENT, sleep specialist) |
Treatment Options
Treatment for baby snoring depends entirely on its underlying cause and severity. A thorough diagnosis is essential before any treatment plan is initiated.
Conservative and Home-Based Treatments (for benign causes)
These methods are typically recommended for primary snoring due to temporary congestion or mild irritation.
- Humidifier: Using a cool-mist humidifier in the baby's room can moisten the air and help soothe irritated nasal passages, reducing congestion.
- Pros: Non-invasive, affordable (typically $30-$100), easy to implement.
- Cons: Requires regular cleaning to prevent mold growth; only effective for dryness/congestion.
- Nasal Saline Drops/Spray: Over-the-counter saline solutions can help loosen and clear mucus from the nasal passages. Follow with a nasal aspirator if needed.
- Pros: Safe for infants, effective for congestion, readily available (typically $5-$15).
- Cons: Can be uncomfortable for baby, temporary relief.
- Elevating the Head: Slightly elevating the head of the crib (NEVER use pillows or blankets under the baby's head due to SIDS risk) by placing a wedge under the mattress can sometimes help with congestion or mild reflux.
- Pros: Non-invasive, can be helpful for specific issues.
- Cons: Must be done safely (under mattress wedge only), not effective for all causes.
- Allergen Avoidance: If allergies are suspected, minimizing exposure to triggers (dust mites, pet dander, mold, pollen) through frequent cleaning, air purifiers, and hypoallergenic bedding can help.
- Pros: Addresses root cause, improves overall respiratory health.
- Cons: Can be challenging to identify and eliminate all allergens.
- Maintaining a Smoke-Free Environment: Exposure to secondhand smoke significantly increases the risk of respiratory infections and airway inflammation in infants.
- Pros: Critical for overall health, easily preventable.
- Cons: Requires commitment from all household members.
Medical Treatments (for specific conditions)
- Allergy Medications: For infants diagnosed with chronic allergies, a pediatrician or allergist might prescribe age-appropriate antihistamines or nasal corticosteroids.
- Pros: Addresses inflammatory causes, can significantly improve nasal airflow.
- Cons: Potential side effects, requires careful dosing and medical supervision.
- Acid Reflux Medications: If GERD is contributing to airway irritation, medications to reduce stomach acid (e.g., H2 blockers, proton pump inhibitors) may be prescribed.
- Pros: Reduces inflammation caused by reflux, can improve breathing.
- Cons: Potential side effects, usually for temporary use, requires medical diagnosis and prescription.
- Orthodontic Interventions / Maxillofacial Procedures: While not for infants, for older children with structural jaw or palate issues contributing to sleep apnea, orthodontic appliances (like palatal expanders) or more advanced maxillofacial surgeries might be considered to widen the airway. This is generally reserved for significant anatomical issues diagnosed by an orthodontist or oral surgeon.
- Pros: Addresses underlying skeletal issues, can provide long-term resolution.
- Cons: Invasive, costly, long treatment duration, applicable only to older children.
- Note on Snoring Mouth Guard: A snoring mouth guard (also known as a Mandibular Advancement Device or MAD) is a custom-fitted oral appliance designed to move the lower jaw and tongue forward to open the airway. It is absolutely NOT appropriate or safe for infants or toddlers due to their developing jaw structure and risk of choking. These devices are used in older children or adults with stable dentition and specific diagnoses of mild to moderate sleep apnea or primary snoring, typically prescribed by a dentist with specialized training in dental sleep medicine. For infants, alternative treatments are always prioritized.
Surgical Treatments (for significant obstruction)
- Adenotonsillectomy: The most common surgical treatment for pediatric obstructive sleep apnea caused by enlarged adenoids and tonsils. This involves the removal of these tissues.
- Pros: Highly effective in resolving OSAS in a significant majority of children.
- Cons: Invasive surgery, risks associated with anesthesia, pain during recovery, potential for recurrence of symptoms in some cases.
- Cost: Without insurance, adenotonsillectomy can range from $3,000 to $8,000, depending on the facility, surgeon's fees, and anesthesia costs. With insurance, patients typically pay deductibles and co-insurance.
- Other Airway Surgeries: In rare cases of complex craniofacial abnormalities or laryngomalacia that doesn't resolve spontaneously, more specialized surgeries may be required to reconstruct or stabilize the airway. These are highly individualized.
- Pros: Can provide life-saving airway improvement for severe conditions.
- Cons: Highly invasive, significant risks, long recovery, typically performed at specialized pediatric centers.
CPAP (Continuous Positive Airway Pressure)
While less common in infants than in adults, CPAP therapy can be used for severe pediatric sleep apnea, especially when surgery is not an option or has been unsuccessful. It involves a mask worn over the nose (or nose and mouth) that delivers continuous air pressure to keep the airway open.
- Pros: Non-invasive (no surgery), highly effective in maintaining an open airway.
- Cons: Adherence can be challenging in infants and young children, requires specialized equipment and regular monitoring, can be uncomfortable.
- Cost: A CPAP machine typically costs $500-$1,500, with masks and supplies costing $100-$300 annually. Insurance often covers a significant portion if medically necessary.
Step-by-Step Process for Diagnosis and Treatment
Navigating the diagnosis and treatment of baby snoring can feel overwhelming. Here's a typical step-by-step process you can expect:
Step 1: Initial Consultation with Your Pediatrician
- Your Role: Describe your baby's snoring, including frequency, loudness, associated symptoms (pauses in breathing, gasping, restless sleep, daytime behavior changes), and any home remedies you've tried. Bring your log of observations.
- Pediatrician's Role: Your pediatrician will conduct a physical examination, checking the nose, mouth, and throat for obvious obstructions (e.g., enlarged tonsils). They will ask detailed questions about your child's sleep, growth, and development. They may recommend initial conservative measures like humidifiers or nasal saline if benign causes are suspected.
Step 2: Referral to a Specialist (if needed)
If the pediatrician suspects an underlying medical condition or obstructive sleep apnea, they will typically refer your baby to one or more specialists:

- Pediatric Otolaryngologist (ENT): An ear, nose, and throat specialist who can further evaluate the upper airway for enlarged adenoids/tonsils, laryngomalacia, or other structural issues.
- Pediatric Sleep Specialist: A doctor trained in sleep medicine who focuses on children. They are experts in diagnosing and managing sleep disorders.
- Pulmonologist: If lung issues are suspected.
- Geneticist/Craniofacial Specialist: If craniofacial abnormalities are a concern.
Step 3: Diagnostic Testing
- Clinical Evaluation by Specialist: The specialist will conduct a more focused physical exam, possibly using a small scope to visualize the back of the nose and throat (nasopharyngoscopy).
- Polysomnography (Sleep Study): This is the gold standard for diagnosing sleep apnea in children. It's a non-invasive test usually performed overnight in a specialized sleep lab.
- What to Expect: Sensors will be gently attached to your baby's skin to monitor brain waves (EEG), eye movements, heart rate (ECG), breathing effort, oxygen levels, carbon dioxide levels, and muscle activity. Parents usually stay with their child.
- Purpose: The sleep study helps determine if there are significant breathing pauses, drops in oxygen saturation, or disruptions to sleep architecture.
- Cost: A pediatric sleep study without insurance can range from $1,500 to $5,000, depending on the facility and duration. Insurance typically covers this procedure when medically indicated.
- Imaging Studies: X-rays of the neck, MRI, or CT scans may be used in specific cases to visualize the airway structure more clearly, especially if abnormalities beyond adenotonsillar hypertrophy are suspected.
Step 4: Treatment Plan Formulation
Based on the diagnostic findings, the specialist will recommend an individualized treatment plan.
- Conservative Management: For mild cases or temporary issues.
- Medical Management: For allergies, reflux, or other conditions.
- Surgical Intervention: For significant anatomical obstructions like enlarged adenoids and tonsils.
- CPAP Therapy: For severe cases not amenable to other treatments.
Step 5: Treatment Implementation and Follow-up
- Procedure (if surgical): If surgery is recommended (e.g., adenotonsillectomy), you will receive detailed instructions for pre-operative preparation, the procedure itself, and post-operative care.
- Medication/Device Management: If medications are prescribed, follow dosing instructions carefully. If CPAP is used, you'll receive training on its proper use and maintenance.
- Follow-up Appointments: Regular follow-up appointments with the specialist are crucial to monitor treatment effectiveness, address any new concerns, and ensure your baby's breathing and development are progressing well. A repeat sleep study may be recommended several months after treatment to confirm resolution of sleep apnea.
Cost and Insurance
Understanding the financial aspect of diagnosing and treating baby snoring, particularly when sleep apnea is involved, is crucial for US families. Costs can vary significantly based on location, facility, and the specific treatments required.
Average US Price Ranges (Without Insurance)
| Service/Treatment | Average Cost Range (US Dollars) | Details |
|---|---|---|
| Pediatrician Consultation | $100 - $300 | Initial visit, often covered by routine check-up co-pay. |
| Specialist Consultation (ENT/Sleep) | $200 - $600 | Initial assessment by a pediatric ENT or sleep specialist. |
| Pediatric Polysomnography (Sleep Study) | $1,500 - $5,000 | Overnight diagnostic test, highly variable by facility. |
| Adenotonsillectomy (Surgery) | $3,000 - $8,000 | Includes surgeon's fees, anesthesia, facility charges. Outpatient procedure. |
| CPAP Machine | $500 - $1,500 | One-time purchase, often rented or leased. |
| CPAP Supplies (Masks, Tubing) | $100 - $300 (annually) | Recurring costs for replacement parts. |
| Prescription Medications (e.g., allergy) | $20 - $200 (monthly) | Varies greatly by medication type, brand vs. generic, and dosage. |
| Nasal Saline/Humidifier | $5 - $100 | Over-the-counter and one-time purchases, generally inexpensive. |
Note: These figures are estimates for uninsured patients. Actual costs can be higher or lower. Always ask for a detailed cost estimate from your provider before proceeding with tests or treatments.
Insurance Coverage Details
Most private health insurance plans in the US, as well as Medicaid and CHIP (Children's Health Insurance Program), typically cover the diagnosis and treatment of medically necessary conditions like pediatric sleep apnea.
- Deductibles: You will likely need to meet your annual deductible before insurance begins to pay for services. For families, this can range from $1,000 to $10,000+.
- Co-pays: Fixed amounts you pay at the time of service for office visits (e.g., $20-$75).
- Co-insurance: A percentage of the cost of a service you're responsible for after your deductible is met (e.g., 10-30%).
- Out-of-Pocket Maximum: A cap on how much you'll have to pay in a year for covered services. Once this limit is reached, insurance typically pays 100% of additional covered costs.
- Pre-authorization: Many diagnostic tests (like sleep studies) and surgical procedures require pre-authorization from your insurance company. Your doctor's office will usually handle this, but it's wise to confirm.
- In-Network vs. Out-of-Network: Staying with providers and facilities within your insurance network will significantly reduce your costs. Out-of-network services often result in much higher out-of-pocket expenses.
Payment Plans and Financing Options
If you face significant out-of-pocket costs, discuss these options with your provider's billing department:
- Payment Plans: Many hospitals and clinics offer interest-free payment plans, allowing you to pay your balance over several months.
- Medical Credit Cards: Services like CareCredit offer special financing for healthcare expenses, often with promotional interest-free periods if paid in full within a certain timeframe. Be cautious, as high interest rates can apply after the promotional period.
- Hospital Financial Assistance Programs: Many hospitals have programs for patients who meet certain income criteria. Inquire with their financial aid office.
- Health Savings Accounts (HSAs) or Flexible Spending Accounts (FSAs): If you have one of these accounts, you can use pre-tax dollars to cover medical expenses, including deductibles and co-pays, effectively saving money.
Pro Tip: Before any major test or procedure, contact your insurance provider directly. Ask them to verify coverage for the specific CPT codes (Current Procedural Terminology) provided by your doctor's office. This can prevent unexpected bills.
Recovery and Aftercare
Recovery and aftercare instructions vary widely depending on the chosen treatment.
For Conservative Treatments
- Humidifiers/Saline: Continue as needed. Ensure humidifiers are cleaned daily to prevent mold.
- Allergy/Reflux Management: Consistently administer prescribed medications and follow allergen avoidance strategies. Monitor for improvement.
- Monitoring: Keep observing your baby's sleep and overall health. If snoring worsens or new symptoms appear, contact your pediatrician.
After Adenotonsillectomy
Adenotonsillectomy is typically an outpatient procedure, meaning your baby can go home the same day. Full recovery usually takes 7-14 days.
- Pain Management: Pain is common after surgery. Your doctor will prescribe pain medication (e.g., acetaminophen, ibuprofen – avoid aspirin in children). Administer as directed, often alternating medications.
- Hydration and Nutrition: Encourage fluids (water, clear juices, popsicles) to prevent dehydration. Soft, cool foods like yogurt, applesauce, mashed potatoes, and scrambled eggs are best initially. Avoid crunchy, spicy, or acidic foods for at least a week to prevent irritation and bleeding.
- Activity Restrictions: Limit strenuous activity for 1-2 weeks. Quiet play is fine, but avoid activities that could cause injury or increase blood pressure.
- Observation for Complications:
- Bleeding: Small amounts of blood-tinged saliva are normal. Bright red blood, frequent swallowing (indicating hidden bleeding), or vomiting blood are emergency signs.
- Fever: A low-grade fever (under 101°F/38.3°C) is common. High fever or fever accompanied by stiff neck/rash needs immediate attention.
- Dehydration: Signs include decreased wet diapers, lethargy, dry mouth, and no tears.
- Respiratory Distress: Increased effort breathing, noisy breathing, or blue discoloration are emergencies.
- Follow-up: Attend all scheduled post-operative appointments to ensure proper healing and monitor for recurrence of sleep-disordered breathing. Often a repeat sleep study is scheduled a few months post-op.
After CPAP Initiation
- Adherence: The biggest challenge is ensuring consistent use of the CPAP mask. Work with a pediatric sleep specialist and respiratory therapist to find the most comfortable mask fit for your baby.
- Hygiene: Regular cleaning of the mask, tubing, and humidifier chamber is essential to prevent infections.
- Monitoring: Regular follow-up with the sleep specialist to monitor compliance, adjust pressure settings as needed, and address any skin irritation from the mask.
- Growth: Monitor your child's growth and development closely, as successful CPAP therapy should lead to improvements.
Prevention
While not all causes of baby snoring are preventable, especially those related to anatomy or congenital conditions, several strategies can help minimize the risk of snoring or reduce its severity.
- Maintain Good Nasal Hygiene:
- Use a humidifier in the baby's room, especially during dry seasons, to keep nasal passages moist.
- Regularly clear your baby's nose with saline drops and a nasal aspirator, especially if they have a cold or allergies.
- Create a Healthy Sleep Environment:
- Ensure the baby's room is free of dust, pet dander, and other potential allergens. Use hypoallergenic bedding and regularly clean toys and surfaces.
- Maintain an optimal room temperature (typically 68-72°F / 20-22°C) to prevent overheating or excessive dryness.
- ADA Guidelines: The American Academy of Pediatrics (AAP) and related dental/medical guidelines consistently recommend placing infants on their back to sleep to reduce the risk of SIDS. While some positions might temporarily reduce snoring, it's crucial to prioritize SIDS safety over snoring reduction.
- Reduce Exposure to Irritants:
- Absolutely avoid secondhand smoke. This is one of the most significant preventable risk factors for respiratory infections and chronic airway inflammation in infants.
- Minimize exposure to strong fumes, air fresheners, and other chemical irritants.
- Manage Allergies and Reflux: If your baby has known allergies or GERD, work with your pediatrician to manage these conditions effectively, as they can contribute to airway inflammation and snoring.
- Promote Healthy Weight: For toddlers and older children, maintaining a healthy weight is crucial, as obesity can significantly increase the risk of sleep apnea. Encourage a balanced diet and active play appropriate for their age.
- Prompt Treatment of Illnesses: Address colds, flu, and respiratory infections promptly to prevent prolonged congestion and inflammation.
Risks and Complications
While benign baby snoring usually carries no long-term risks, chronic snoring, especially when it's a symptom of obstructive sleep apnea, can lead to serious and lasting complications if left untreated.
- Developmental and Cognitive Delays: Chronic sleep deprivation and intermittent oxygen deprivation during sleep can negatively impact brain development, leading to:
- Behavioral Problems: Irritability, hyperactivity, aggression, difficulty with attention and focus (often misdiagnosed as ADHD).
- Learning Difficulties: Poor school performance in older children, difficulties with memory and problem-solving.
- Speech and Language Delays: Due to impacted cognitive development and potential changes in oral motor function.
- Cardiovascular Issues: Untreated pediatric sleep apnea is linked to:
- High Blood Pressure (Hypertension): The body's stress response to breathing difficulties can lead to elevated blood pressure.
- Heart Strain: Chronic oxygen desaturation and increased breathing effort can put a strain on the heart, potentially leading to long-term cardiac problems.
- Growth Problems (Failure to Thrive):
- The increased effort of breathing during sleep burns extra calories, which can hinder weight gain.
- Disrupted sleep interferes with the release of growth hormones, further impacting physical development.
- Metabolic Problems: There is increasing evidence linking pediatric sleep apnea to insulin resistance and an increased risk of type 2 diabetes later in life.
- Increased Risk of Accidents: Severely sleep-deprived older children or adolescents may have impaired judgment and reaction times, increasing the risk of accidents.
- Recurrence After Treatment: While adenotonsillectomy is highly effective, sleep apnea can recur in a small percentage of children, especially those with underlying conditions or significant weight gain.
These risks underscore the importance of early diagnosis and appropriate intervention for any baby snoring that is persistent, loud, or accompanied by other concerning symptoms.
Children / Pediatric Considerations
Understanding baby snoring requires specific attention to pediatric considerations, as children are not just "miniature adults" when it comes to sleep and breathing.
Age-Specific Guidance for Parents
- Newborns (0-3 months):
- Newborn snoring is quite common and often due to tiny nasal passages, transient congestion, or even remnants of amniotic fluid.
- Focus: Observe closely. Most newborn noisy breathing is benign. However, if accompanied by struggling to breathe, pauses, or poor feeding, seek immediate medical advice. Laryngomalacia is relatively common in this age group and often improves spontaneously.
- Infants (4-12 months):
- As babies grow, enlarged adenoids and tonsils become a more frequent cause of snoring. Teething can also temporarily increase congestion.
- Focus: Look for consistency of snoring, presence of breathing pauses, and impact on sleep quality and daytime behavior (e.g., irritability, frequent night wakings). This is a critical period for growth and development, making undisturbed sleep vital.
- Toddlers (1-3 years) and Preschoolers (3-5 years):
- This is the age group where obstructive sleep apnea due to enlarged tonsils and adenoids peaks. Behavioral issues (hyperactivity, inattention) due to sleep deprivation become more apparent.
- Focus: Persistent snoring, mouth breathing, and signs of restless sleep are strong indicators for specialist referral. Early intervention can prevent long-term developmental and health consequences.
Why Children are Different
- Anatomy: Children have proportionally smaller airways, more flexible cartilage, and often larger tonsils/adenoids relative to their airway size compared to adults.
- Symptoms: While adults often report excessive daytime sleepiness, children with sleep apnea may paradoxically present with hyperactivity, aggression, or attention problems.
- Developmental Impact: Untreated sleep apnea can profoundly impact a child's brain development, growth, and learning abilities, unlike in adults where the primary risks are often cardiovascular.
- Treatment: While surgery (adenotonsillectomy) is the first-line treatment for most children with OSAS, CPAP can be challenging to implement due to compliance issues. Snoring mouth guards are generally not suitable for this age group due to developing dentition and compliance challenges.
Pro Tip: Never assume your child will "grow out of" concerning snoring, especially if it's accompanied by breathing pauses or other symptoms. Always consult a pediatrician, as early intervention is key.
Cost Breakdown
As covered in the "Cost and Insurance" section, medical expenses related to baby snoring can be substantial. Here's a summary of the average costs for common scenarios:

Average US Costs (Without Insurance)
- Low-Level Concern (Pediatrician Visit + Home Remedies):
- Pediatrician visit: $100 - $300
- Saline/Humidifier: $5 - $100
- Total: $105 - $400
- Mid-Level Concern (Specialist Consult + Sleep Study):
- Specialist consultation: $200 - $600
- Pediatric Sleep Study: $1,500 - $5,000
- Total: $1,700 - $5,600
- High-Level Concern (Surgery for OSAS):
- Specialist consultation, Sleep Study (if not already done)
- Adenotonsillectomy: $3,000 - $8,000
- Post-op follow-ups: $100 - $300 per visit
- Total: $3,000 - $8,000+ (on top of diagnostic costs)
With vs. Without Insurance
- With Insurance: You will typically pay your co-pay for doctor visits (e.g., $20-$75). For sleep studies and surgery, you'll pay your deductible (ranging from $1,000-$10,000+), followed by co-insurance (e.g., 10-30% of the cost until your out-of-pocket maximum is met).
- Without Insurance: You are responsible for 100% of the billed charges. This is why discussing payment plans and financial assistance programs directly with the provider is crucial.
Payment Plans and Financing Options
As mentioned, hospitals and clinics often provide interest-free payment plans. Medical credit cards (e.g., CareCredit) can also be an option for managing costs, but be mindful of interest rates. Always inquire about financial assistance programs available through the hospital or healthcare system.
Cost-Saving Tips
- Verify Insurance Coverage: Always call your insurance company before appointments, tests, or procedures to understand what's covered, what your out-of-pocket costs will be, and if pre-authorization is required.
- Stay In-Network: Use providers and facilities that are part of your insurance network to avoid higher out-of-network costs.
- Request Itemized Bills: After services, request an itemized bill to check for accuracy and identify any potential billing errors.
- Generic Medications: If medications are prescribed, ask your doctor if a generic version is available, as it's typically much cheaper.
- Shop Around (for non-urgent services): For diagnostic tests like sleep studies, if multiple accredited sleep labs are available, compare their self-pay or insurance-negotiated rates.
Frequently Asked Questions
Is baby snoring always serious?
No, baby snoring is not always serious. Many infants snore occasionally due to temporary nasal congestion from a cold, allergies, or simply having small airways. However, persistent, loud snoring accompanied by other symptoms like breathing pauses, gasping, or restless sleep can indicate a more serious condition like obstructive sleep apnea and warrants medical evaluation.
What causes a newborn to snore?
Newborn snoring is often caused by very narrow nasal passages, normal mucus production, or temporary congestion from a mild cold or dry air. Sometimes, a condition called laryngomalacia (softness of the voice box cartilage) can cause noisy breathing that sounds like snoring, but this often improves as the baby matures.
Can a snoring mouth guard be used for babies?
No, a snoring mouth guard is generally NOT appropriate or safe for infants or toddlers. Snoring mouth guards are custom oral appliances designed to reposition the jaw and tongue in older children (with fully developed dentition) or adults. Their use in babies presents a significant choking hazard and could interfere with proper jaw and dental development.
When should I worry about my baby snoring?
You should worry if your baby's snoring is consistently loud, occurs most nights, or is accompanied by pauses in breathing, gasping for air, restless sleep, excessive sweating, mouth breathing during sleep, or daytime symptoms like irritability, poor feeding, or slow weight gain. These are signs that medical evaluation is needed.
Can baby snoring affect their development?
Yes, if baby snoring is a symptom of untreated obstructive sleep apnea, it can significantly affect development. Chronic sleep deprivation and intermittent oxygen drops can impair brain development, leading to behavioral issues (like hyperactivity), learning difficulties, and potential delays in growth and cognitive skills.
How is baby snoring diagnosed?
The diagnostic process typically starts with your pediatrician. If they suspect a serious issue, they may refer you to a pediatric ENT or sleep specialist. The gold standard for diagnosing sleep apnea is an overnight pediatric polysomnography (sleep study), which monitors breathing, oxygen levels, and sleep patterns.
What are the treatment options for baby snoring?
Treatment options depend on the cause. For benign snoring, home remedies like humidifiers or nasal saline may suffice. If allergies or reflux are culprits, specific medications can help. For obstructive sleep apnea, the most common treatment is adenotonsillectomy (surgical removal of enlarged adenoids and tonsils). In some severe cases, CPAP therapy might be considered.
Is surgery always necessary if my baby snores?
No, surgery is not always necessary. It is typically reserved for cases where an anatomical obstruction, such as significantly enlarged tonsils and adenoids, is definitively causing obstructive sleep apnea. Many babies snore for temporary or benign reasons that resolve with conservative measures or as they grow.
How much does it cost to treat baby snoring?
Costs vary widely. A pediatrician visit might be $100-$300. A diagnostic sleep study can range from $1,500-$5,000. If surgery like an adenotonsillectomy is required, costs can be $3,000-$8,000 without insurance. Insurance typically covers medically necessary treatments, but deductibles and co-pays apply.
Can baby snoring be prevented?
While not all causes are preventable, you can reduce the risk. Maintaining good nasal hygiene, using a humidifier, creating a dust-free sleep environment, avoiding secondhand smoke, and promptly treating illnesses like colds and allergies can help prevent or reduce snoring.
When to See a Dentist or Doctor
It's vital for parents to know when to seek professional medical advice regarding their baby's snoring. While some noisy breathing is normal, certain signs warrant immediate attention.
Clear Warning Signs That Need Immediate Attention:
- Pauses in Breathing: If you observe your baby stopping breathing for 5-10 seconds or longer, followed by a gasp, snort, or sudden awakening, this is a critical red flag.
- Bluish Discoloration: If your baby's lips or skin turn blue during a breathing pause, this is a medical emergency.
- Struggling to Breathe: Visible effort to breathe (e.g., chest retractions, flaring nostrils), especially with sucking in around the neck or ribs, is a serious sign.
- Loud Gasping or Choking: Sounds indicating your baby is struggling to get air are concerning.
- Excessive Lethargy: If your baby is unusually tired, difficult to wake, or less responsive than normal.
Red Flags vs. Routine Care Guidance:
See your pediatrician promptly (within a few days to a week) if:
- Loud, Persistent Snoring: Your baby snores loudly almost every night, and it doesn't improve with simple home remedies (like saline or a humidifier).
- Restless Sleep: Your baby frequently tosses and turns, adopts unusual sleep positions, or wakes up often during the night.
- Mouth Breathing: Your baby consistently breathes through their mouth during sleep, even when not congested.
- Excessive Sweating: Your baby sweats profusely around the head and neck during sleep.
- Daytime Behavioral Changes: Unexplained irritability, hyperactivity, difficulty feeding, or signs of chronic fatigue.
- Poor Growth: If your baby is not gaining weight appropriately or showing signs of developmental delays.
- Nasal Voice: A persistent "nasal" quality to your baby's cries or babbling, indicating chronic nasal obstruction.
Routine Care/Monitoring is appropriate if:
- Your baby snores only occasionally, such as during a cold or when experiencing mild allergies.
- The snoring is soft, mild, and not accompanied by any of the red flag symptoms listed above.
- Your baby appears well-rested, is feeding well, and growing normally.
Always err on the side of caution. If you have any concerns about your baby's breathing or sleep, discussing it with your pediatrician is always the best first step. They can provide an initial assessment and guide you on whether further evaluation by a specialist is necessary.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Difference Between Snoring and Sleep Apnea: Complete Guide
More than 80 million Americans regularly snore, and while often dismissed as a mere nuisance, loud and persistent snoring can be a critical indicator of a much more serious underlying health condition: sleep apnea. The difference between snoring and sleep apnea is profound, impacting not just yo
February 23, 2026
Mouth Taping for Snoring: Complete Guide
Snoring. It's the nocturnal soundtrack for millions of Americans, often a source of frustration for bed partners and a potential indicator of underlying health issues for the snorer themselves. Roughly 45% of adults snore occasionally, and 25% are habitual snorers, impacting sleep quality, relat
February 23, 2026

Is All Snoring Sleep Apnea
Many individuals, perhaps even you or a loved one, have been told they snore loudly. It's often dismissed as a harmless, albeit annoying, nocturnal habit. However, what if that nightly rumble is more than just noise? What if it's a critical indicator of an underlying health condition that significan
February 23, 2026
Cpap Dry Mouth Even With Humidifier: Complete Guide
Experiencing dry mouth while using a CPAP machine, even with a humidifier, is a common and incredibly frustrating issue for millions of Americans. It can disrupt sleep, diminish the effectiveness of your sleep apnea treatment, and significantly impact your oral health. Imagine waking up every mornin
February 23, 2026