Infant Snoring: Complete Guide

Key Takeaways
- Hearing your infant snore can be a concerning sound for any parent. While occasional, soft snoring might seem harmless, a significant percentage of babies experience chronic infant snoring, which can sometimes be a red flag for underlying health issues, including sleep-disordered breathing. In f
Infant Snoring: Complete Guide
Hearing your infant snore can be a concerning sound for any parent. While occasional, soft snoring might seem harmless, a significant percentage of babies experience chronic infant snoring, which can sometimes be a red flag for underlying health issues, including sleep-disordered breathing. In fact, studies suggest that habitual snoring affects between 10% and 30% of children, with a notable portion of these being infants. Understanding the difference between normal baby noises and potentially problematic snoring is crucial for your child's immediate health and long-term development. This comprehensive guide from SmilePedia.net aims to empower you with medically accurate information, exploring the causes, symptoms, diagnostic processes, and treatment options for infant snoring, ensuring you can make informed decisions for your little one's well-being. We will delve into everything from the anatomical reasons behind noisy breathing to the role of pediatric dental health and when it's time to consult a specialist.
Key Takeaways:
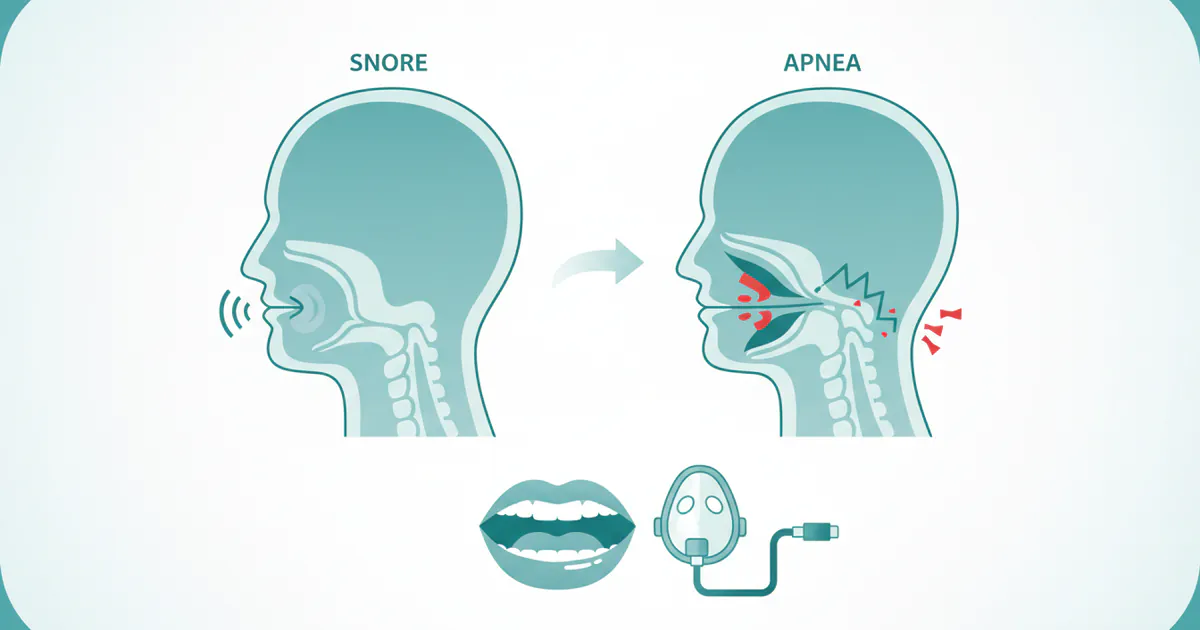
- Infant Snoring vs. Sleep Apnea: While occasional infant snoring can be normal, persistent, loud snoring, especially when accompanied by breathing pauses, gasping, or restless sleep, may indicate obstructive sleep apnea (OSA).
- Common Causes: Enlarged tonsils and adenoids are the leading culprits in older infants and toddlers, but nasal congestion, anatomical differences, reflux, and certain medical conditions can also contribute.
- Diagnosis is Key: Diagnosis typically involves a pediatrician visit, referral to a pediatric ENT specialist or sleep physician, and often a polysomnography (sleep study) in a specialized lab.
- Treatment Varies: Mild cases might improve with conservative measures (humidifiers, positional changes). More significant issues may require medical management (nasal steroids for allergies) or surgical intervention (adenotonsillectomy).
- Cost & Coverage: A sleep study can range from $1,000 to $5,000 without insurance. Adenotonsillectomy costs typically fall between $3,000 and $8,000. Most insurance plans cover diagnostic tests and medically necessary treatments for infant sleep apnea, but co-pays and deductibles apply.
- Long-Term Impact: Untreated infant sleep apnea can lead to developmental delays, behavioral problems, cardiovascular issues, and failure to thrive, underscoring the importance of early diagnosis and intervention.
- Adult Anti-Snoring Devices: Oral appliances like anti snoring mouth guards and CPAP machines are generally not used for infants. Pediatric treatments are highly specialized and age-appropriate.
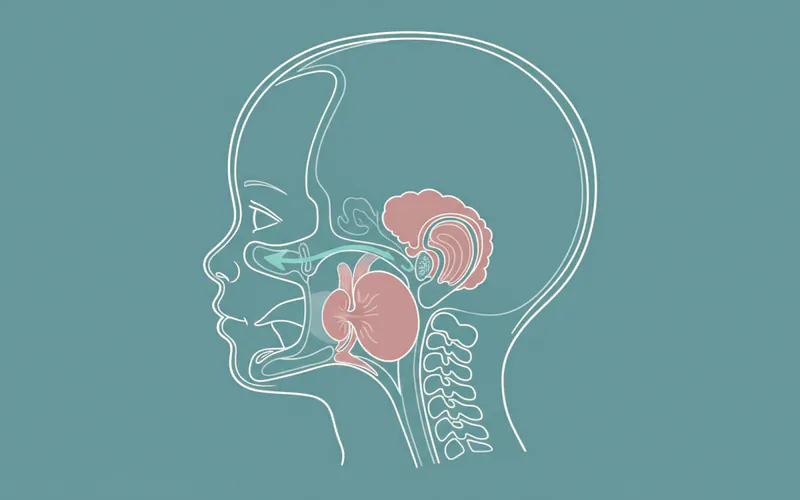
What Is Infant Snoring? An Overview
Infant snoring refers to the noisy breathing that occurs during sleep when an infant's airway is partially obstructed. The sounds can range from soft, gentle rumbling to loud, harsh vibrations. It's important to distinguish between "primary snoring" – snoring without significant breathing pauses or oxygen desaturation – and snoring that is a symptom of more serious conditions like Upper Airway Resistance Syndrome (UARS) or Obstructive Sleep Apnea (OSA).
A baby's respiratory system is inherently smaller and more pliable than an adult's, making it more susceptible to partial obstruction. Factors like nasal congestion from a cold, minor anatomical variations, or even sleeping position can cause transient snoring. However, when snoring is persistent, loud, or accompanied by other concerning symptoms, it warrants medical evaluation. It's estimated that up to 10% of infants experience habitual snoring, and a subset of these will have pediatric sleep apnea. The key is to assess the quality and consistency of the snoring, along with any associated distress or physiological changes.
Types of Infant Snoring and Related Conditions
Understanding the different categories of snoring is vital for proper diagnosis and treatment.
Primary Snoring
This is the simplest form of snoring, characterized by noisy breathing during sleep without significant disruptions to breathing, oxygen levels, or sleep architecture. It's often intermittent and may be caused by temporary factors like mild congestion or specific sleep positions. While generally considered benign, primary snoring should still be monitored, as it can sometimes progress to more severe conditions.
Upper Airway Resistance Syndrome (UARS)
UARS is a condition where the upper airway narrows during sleep, leading to increased effort to breathe. This increased effort causes micro-arousals from sleep, which disturb sleep quality without necessarily causing significant oxygen desaturation or complete breathing pauses (apneas). Infants with UARS may snore, breathe loudly, or be restless during sleep, and often experience daytime symptoms like irritability, difficulty focusing, or excessive sleepiness, even if oxygen levels appear normal.
Obstructive Sleep Apnea (OSA)
This is the most severe form of sleep-disordered breathing. In infants with OSA, the upper airway repeatedly collapses during sleep, leading to partial or complete blockage of airflow. These blockages, called apneas (complete cessation of breathing) or hypopneas (partial cessation with reduced airflow), result in drops in oxygen levels and brief awakenings (arousals) that fragment sleep. OSA in infants can have serious long-term consequences if left untreated.
Central Sleep Apnea (CSA)
Less common in typically developing infants, Central Sleep Apnea occurs when the brain fails to send the proper signals to the muscles that control breathing, leading to a pause in breathing. Unlike OSA, there is no physical obstruction of the airway. CSA is more often seen in premature infants, those with neurological conditions, or certain genetic syndromes. While it can cause snoring-like sounds (due to compensatory breathing after an apnea), its mechanism is fundamentally different from obstructive issues.
Causes: Why Infant Snoring Happens
Multiple factors can contribute to infant snoring, ranging from benign and temporary to chronic and medically significant.
Anatomical Factors
- Small Airway Size: Infants naturally have smaller, more compliant airways than adults, making them more prone to collapse or partial obstruction.
- Enlarged Tonsils and Adenoids: This is the most common cause of habitual snoring and OSA in children beyond the newborn stage. Tonsils are lymphoid tissues at the back of the throat, and adenoids are similar tissues located behind the nose. When enlarged, they can significantly block airflow during sleep.
- Nasal Obstruction:
- Allergies: Environmental allergens (dust mites, pet dander, pollen) can cause inflammation and swelling of the nasal passages, leading to congestion.
- Colds and Infections: Viral upper respiratory infections are a common, temporary cause of nasal congestion and snoring.
- Deviated Septum: Although less common as a primary cause in infants, structural issues in the nasal septum (the wall dividing the nostrils) can restrict airflow.
- Craniofacial Abnormalities: Certain conditions present at birth, such as Pierre Robin sequence, Down syndrome, or Treacher Collins syndrome, can involve structural differences in the jaw, palate, or tongue that predispose infants to airway obstruction.
- Laryngomalacia: A common congenital condition where the cartilage of the larynx (voice box) is soft and collapses inward during inhalation, causing noisy breathing (stridor) that can sometimes be mistaken for or coexist with snoring.
Medical Conditions
- Gastroesophageal Reflux Disease (GERD): Acid reflux can irritate the airway, leading to inflammation and swelling that contributes to snoring and even apnea.
- Asthma: Inflammation of the airways associated with asthma can impact breathing patterns during sleep.
- Hypotonia: Reduced muscle tone, often associated with neurological conditions, can make the upper airway muscles more prone to collapse.
- Obesity: While less common in very young infants, increasing rates of childhood obesity can contribute to sleep-disordered breathing by increasing fat deposits around the neck and pharynx.
Other Factors
- Sleep Position: Sleeping on the back is generally recommended for SIDS prevention, but in some infants, it can slightly increase the likelihood of snoring if there's mild congestion. However, changing sleep position for snoring is never recommended if it goes against safe sleep guidelines.
- Exposure to Irritants: Secondhand smoke or other airborne irritants can inflame respiratory passages, contributing to congestion and snoring.
Pro Tip: Always maintain a smoke-free environment for your infant. Exposure to secondhand smoke significantly increases the risk of respiratory infections and sleep-disordered breathing.
Signs and Symptoms of Concerning Infant Snoring
While occasional soft snoring might be benign, certain signs and symptoms, especially when persistent, should prompt a medical evaluation. It's not just the sound, but the quality of breathing and the impact on the infant.
During Sleep:
- Loud, Habitual Snoring: Snoring that occurs most nights (3 or more nights a week) and is loud enough to be heard from another room.
- Breathing Pauses: Visible pauses in breathing, lasting for several seconds (often >10 seconds, but shorter pauses can be significant in infants). These are often followed by gasping, snorting, or choking sounds.
- Labored Breathing: Visible effort to breathe, such as chest retractions (skin pulling in around the ribs), flaring nostrils, or abdominal breathing.
- Restless Sleep: Frequent awakenings, tossing and turning, or unusual sleep positions (e.g., hyperextending the neck).
- Sweating Excessively: Waking up drenched in sweat, particularly around the head and neck, due to the increased effort of breathing.
- Cyanosis: A bluish tint to the lips or skin, indicating dangerously low oxygen levels. This is a medical emergency.
- Mouth Breathing: Persistent mouth breathing during sleep, often due to nasal obstruction.
During Waking Hours:
- Difficulty Waking: Struggling to wake up, appearing drowsy or irritable.
- Daytime Sleepiness: Falling asleep easily during the day, even in stimulating environments.
- Irritability and Behavioral Issues: Increased fussiness, hyperactivity, or difficulty regulating emotions, often mistaken for typical toddler behavior.
- Difficulty Feeding or Swallowing: Infants with significant obstruction may struggle to coordinate breathing and feeding.
- Failure to Thrive: Poor weight gain or slow growth, as the body expends excessive energy on breathing rather than growth.
- Nasal Congestion or Runny Nose: Chronic symptoms of upper respiratory irritation.
- Chronic Ear Infections or Sinusitis: Enlarged adenoids can contribute to recurrent infections.

Pro Tip: If you record your infant sleeping and notice any breathing pauses or excessive effort, show this recording to your pediatrician. Visual evidence can be very helpful for diagnosis.
Treatment Options for Infant Snoring
Treatment for infant snoring depends entirely on the underlying cause and severity. A comprehensive evaluation by a pediatrician, often followed by a pediatric otolaryngologist (ENT) or sleep specialist, is essential to determine the most appropriate course of action.
Conservative and Lifestyle Approaches
These options are generally considered for mild, intermittent snoring or as initial steps before more invasive treatments.
- Nasal Saline Sprays/Drops: For congestion due to colds or allergies, saline can help clear nasal passages.
- Pros: Non-invasive, widely available, safe.
- Cons: Temporary relief, doesn't address structural issues.
- Humidifiers: A cool-mist humidifier in the infant's room can help moisturize airways, particularly in dry environments, reducing congestion.
- Pros: Safe, simple, can improve comfort.
- Cons: Requires regular cleaning to prevent mold growth; limited effectiveness for structural issues.
- Positional Changes: While infants should always be placed on their back for sleep to reduce SIDS risk, a doctor might suggest slightly elevating the head of the crib (e.g., by placing blocks under the crib legs) for specific conditions like reflux, under strict medical guidance. Never use pillows or wedges inside the crib.
- Pros: Can sometimes alleviate mild snoring.
- Cons: Must adhere to safe sleep guidelines; not a solution for significant obstruction.
- Allergy Management: If allergies are contributing to nasal congestion, identifying and minimizing exposure to allergens (dust mite covers, pet-free zones) can help. Antihistamines or nasal steroid sprays might be prescribed by a doctor for older infants, but caution is advised.
- Pros: Addresses a root cause.
- Cons: Requires diligent environmental control; medication side effects.
Medical Interventions
- Nasal Steroid Sprays: For infants with significant nasal inflammation due to allergies or chronic rhinitis, a low-dose nasal corticosteroid spray might be prescribed by a specialist.
- Pros: Reduces inflammation, can be very effective for allergy-related obstruction.
- Cons: Requires consistent use, potential for mild local side effects, not for all ages.
- Acid Reflux Medication: If GERD is suspected to be irritating the airway, medications to reduce stomach acid (e.g., H2 blockers or proton pump inhibitors) may be prescribed.
- Pros: Addresses underlying reflux, can reduce airway inflammation.
- Cons: Potential side effects, requires careful dosing.
- Weight Management: For older infants or toddlers who are overweight, dietary and lifestyle changes recommended by a pediatrician can help reduce the severity of sleep apnea.
- Pros: Holistic health benefits.
- Cons: Requires significant family commitment, can be challenging.
Surgical Interventions
These are often considered when conservative or medical treatments are ineffective, or when OSA is severe.
- Adenotonsillectomy (T&A): This is the most common and often highly effective surgical treatment for pediatric OSA caused by enlarged tonsils and adenoids.
- Pros: High success rate in resolving OSA symptoms (up to 80-90% in some populations).
- Cons: General anesthesia risks, post-operative pain and recovery (typically 7-14 days), potential for recurrence of sleep apnea.
- Lingual Frenectomy: If a "tongue tie" (ankyloglossia) is contributing to airway issues or feeding problems that indirectly impact breathing, a frenectomy (clipping the lingual frenulum) might be performed.
- Pros: Minimally invasive, quick recovery.
- Cons: Only effective if tongue tie is a primary contributing factor.
- Turbinate Reduction: Surgical reduction of enlarged nasal turbinates (structures inside the nose) can improve nasal airflow.
- Pros: Can significantly improve nasal breathing.
- Cons: Less common in infants, potential for crusting or bleeding.
- Palatal Expansion: In some cases of narrow upper jaw (maxillary constriction), an orthodontist or pediatric dentist may recommend a palatal expander for older children. While not typically for infants, early assessment of craniofacial development can be relevant. The American Dental Association (ADA) recognizes the importance of early intervention for craniofacial development and its link to airway health.
- Pros: Addresses skeletal issues, long-term airway benefit.
- Cons: Requires cooperation, multi-stage treatment.
- Other Craniofacial Surgeries: For severe craniofacial abnormalities, more complex surgeries (e.g., mandibular distraction osteogenesis) may be necessary to improve airway patency.
- Pros: Life-changing for severe cases.
- Cons: Major surgery, significant recovery, specialized centers needed.
Important Note on Oral Appliances for Infants: It's critical to understand that common adult anti snoring mouth guard devices and oral appliances, such as mandibular advancement devices (MADs), are not designed or recommended for infants. Their oral anatomy is vastly different, and their jaw structures are still developing. While sleep apnea mouth guard reviews might be useful for adults, these products are entirely inappropriate for pediatric use. Infant sleep apnea requires specialized medical or surgical intervention, never off-the-shelf adult oral appliances. In rare cases, custom-made oral appliances might be considered for older children with very specific anatomical issues and under strict supervision by a pediatric sleep dentist, but this is extremely uncommon for infants.
Step-by-Step Process: Diagnosing and Treating Infant Snoring
The journey from noticing your infant's snoring to effective treatment is typically a multi-stage process involving several healthcare professionals.
Step 1: Initial Consultation with Your Pediatrician
- What to Expect: You'll discuss your concerns, describe the snoring (loudness, frequency, associated gasping/pauses), and list any daytime symptoms (irritability, feeding issues, excessive sleepiness). The pediatrician will review your infant's medical history, perform a physical examination (checking for enlarged tonsils/adenoids, nasal congestion, weight gain), and may ask about family history of snoring or sleep apnea.
- Initial Recommendations: For mild cases, the pediatrician might suggest conservative measures like humidifiers, nasal saline, or monitoring for a few weeks. If symptoms are more concerning, they will likely recommend a referral.
Step 2: Referral to a Specialist
- Pediatric ENT (Otolaryngologist): Often the first specialist consulted, especially if enlarged tonsils or adenoids are suspected. The ENT will perform a detailed examination of the airway, sometimes using a small, flexible scope to visualize the adenoids and larynx.
- Pediatric Sleep Specialist/Pulmonologist: If the ENT finds no obvious structural issues, or if the symptoms strongly suggest sleep apnea despite ambiguous physical exam findings, a sleep specialist will be involved.
Step 3: Diagnostic Testing – Polysomnography (Sleep Study)
- Purpose: The gold standard for diagnosing sleep apnea in infants and children. It provides a comprehensive assessment of sleep, breathing, and oxygen levels.
- What to Expect: Your infant will spend a night at a specialized pediatric sleep lab. Technicians will attach small, painless sensors to monitor:
- Brain activity (EEG) to determine sleep stages.
- Eye movements (EOG).
- Muscle activity (EMG).
- Heart rate (ECG).
- Breathing effort (chest and abdominal belts).
- Airflow through the nose and mouth.
- Oxygen levels in the blood (pulse oximetry).
- Carbon dioxide levels (transcutaneous CO2 monitor).
- Video and audio recording.
- Results and Interpretation: A sleep specialist will interpret the data, looking for apneas, hypopneas, oxygen desaturations, and sleep disruptions. The Apnea-Hypopnea Index (AHI) is a key metric, indicating the number of apneas and hypopneas per hour of sleep. An AHI greater than 1-2 in infants is often considered abnormal.
Step 4: Treatment Implementation
- Based on Diagnosis: The specialist will develop a treatment plan tailored to your infant's specific diagnosis and severity. This could range from:
- Medical management: Prescribing nasal steroids, reflux medications, or allergy treatments.
- Surgical intervention: Scheduling an adenotonsillectomy if enlarged tissues are the cause.
- CPAP (Continuous Positive Airway Pressure): In severe cases, especially for infants with craniofacial anomalies or who are not candidates for surgery, a customized CPAP mask may be used. This involves a machine that delivers a continuous stream of air to keep the airway open during sleep. It requires careful fitting and ongoing monitoring by a sleep team.
Step 5: Follow-up and Monitoring
- Post-Treatment Assessment: After treatment (especially surgery), follow-up appointments are crucial. Sometimes, a repeat sleep study may be recommended a few months after surgery to ensure resolution of OSA.
- Ongoing Monitoring: Even after successful treatment, continued monitoring for recurrence or new symptoms is important, as children grow and their airways change.
Cost and Insurance Considerations for Infant Snoring Treatment
Navigating the costs associated with diagnosing and treating infant snoring can be complex. Prices vary significantly based on location, facility, and insurance coverage.
Average US Costs (Without Insurance)
| Service/Treatment | Low Range (USD) | Mid Range (USD) | High Range (USD) |
|---|---|---|---|
| Pediatrician Visit | $100 | $250 | $500 |
| Specialist Consultation (ENT/Sleep) | $200 | $400 | $800 |
| Polysomnography (Sleep Study) | $1,000 | $3,000 | $5,000 |
| Nasal Steroid Spray (monthly) | $20 | $50 | $100 |
| Adenotonsillectomy | $3,000 | $5,500 | $8,000 |
| CPAP Machine (initial setup) | $1,000 | $2,500 | $4,000 |
These are approximate cash prices and can vary widely.
Insurance Coverage Details
Most major health insurance plans in the US, including employer-sponsored plans, Affordable Care Act (ACA) marketplace plans, and government programs like Medicaid and CHIP (Children's Health Insurance Program), typically cover the diagnosis and treatment of medically necessary conditions like infant sleep apnea.
- Diagnostic Tests: Polysomnography (sleep study) is almost always covered when deemed medically necessary by a physician. You will likely be responsible for your co-pay and meeting your deductible.
- Specialist Visits: Visits to pediatric ENTs, pulmonologists, and sleep specialists are usually covered, subject to co-pays.
- Medical Treatments: Prescription medications like nasal steroids or reflux inhibitors are covered under the prescription drug portion of your plan, with varying co-pays depending on the drug tier.
- Surgical Procedures: Procedures like adenotonsillectomy are generally covered. However, you will be responsible for your deductible, co-insurance (a percentage of the cost after your deductible is met), and any out-of-pocket maximums.
- CPAP Therapy: CPAP machines and supplies are typically covered as durable medical equipment (DME), often requiring a specific prescription and sometimes prior authorization. There may be separate DME deductibles or co-insurance.
Pro Tip: Always verify your specific coverage with your insurance provider before scheduling any expensive tests or procedures. Ask about prior authorization requirements, in-network vs. out-of-network costs, and what your estimated out-of-pocket expenses will be. Keep detailed records of all communications with your insurance company.
Recovery and Aftercare for Infant Snoring Treatment
Recovery and aftercare will vary significantly depending on the treatment method.

After Conservative/Medical Treatment
- Monitoring: Continue to monitor your infant's snoring and breathing patterns. Note any improvements or worsening of symptoms.
- Medication Adherence: If prescribed, administer medications consistently as directed by your doctor.
- Environmental Control: Maintain a clean, allergen-free environment, use humidifiers, and ensure no exposure to secondhand smoke.
- Follow-up: Attend all scheduled follow-up appointments with your pediatrician or specialist to assess effectiveness and make adjustments.
After Adenotonsillectomy
This is the most common surgical intervention for infant OSA, and it requires careful post-operative care.
- Immediate Post-Op: Your infant will be monitored in a recovery room for several hours, then typically discharged home the same day or kept overnight depending on age and medical status. Pain management will begin.
- Pain Management: Pain is common, especially a sore throat. Your doctor will prescribe pain relievers (e.g., ibuprofen, acetaminophen) specifically formulated for infants. Administer these as directed. Avoid aspirin due to Reye's syndrome risk.
- Hydration and Nutrition:
- Offer clear, cool liquids (water, diluted apple juice, popsicles) frequently in small amounts.
- Progress to soft, bland foods (yogurt, mashed potatoes, applesauce) as tolerated.
- Avoid acidic, spicy, crunchy, or hot foods for at least 1-2 weeks, as these can irritate the surgical site and increase bleeding risk.
- Activity Restriction: Keep your infant quiet and avoid strenuous activity for 1-2 weeks. This includes limiting vigorous play that could cause bleeding.
- Observe for Complications:
- Bleeding: Small amounts of blood-tinged saliva are normal. Bright red bleeding, frequent swallowing (indicating hidden bleeding), or vomiting blood requires immediate medical attention.
- Fever: A low-grade fever (under 101°F or 38.3°C) is common. High fever should be reported to your doctor.
- Dehydration: Signs include decreased urination, dry mouth, and lethargy.
- Return of Snoring: Some snoring may occur initially due to swelling, but it should improve over time. If severe snoring returns after swelling subsides, inform your doctor.
- Follow-up: A follow-up appointment with the ENT is typically scheduled 1-2 weeks post-surgery. Your doctor may recommend a repeat sleep study several months later to confirm resolution of OSA.
After CPAP Therapy
- Consistent Use: CPAP therapy is only effective if used consistently every night, for the entire duration of sleep. This can be challenging with infants but is crucial.
- Mask Fit and Hygiene: Ensure the mask fits correctly to prevent leaks and skin irritation. Clean the mask and tubing regularly as instructed by the DME provider to prevent infections.
- Monitoring: Regular follow-ups with the sleep specialist are necessary to adjust pressure settings, monitor compliance, and address any issues.
Prevention of Infant Snoring
While some causes of infant snoring are unavoidable (e.g., genetic craniofacial differences), several strategies can help reduce the risk or severity of sleep-disordered breathing.
- Promote Healthy Weight: For infants and toddlers, maintaining a healthy weight through appropriate nutrition and activity levels can reduce the risk of obesity-related sleep apnea. Consult your pediatrician for guidance on infant feeding and growth.
- Manage Allergies and Asthma: Work with your pediatrician to diagnose and manage any allergies or asthma your infant may have. Controlling these conditions reduces inflammation in the airways.
- Avoid Environmental Irritants:
- Secondhand Smoke: Strictly avoid exposing your infant to tobacco smoke, which is a major irritant and risk factor for respiratory infections and sleep apnea.
- Pollutants: Minimize exposure to indoor air pollutants and strong fumes.
- Practice Good Sleep Hygiene:
- Safe Sleep Environment: Always place your infant on their back to sleep on a firm, flat surface without loose bedding, bumpers, or toys. This is primarily for SIDS prevention but also promotes clear airways.
- Consistent Sleep Schedule: Establishing a regular bedtime and wake-up time, even for infants, can support better sleep quality.
- Optimal Room Conditions: Maintain a cool, dark, and quiet sleep environment. A humidifier can be beneficial in dry climates.
- Address Reflux: If your infant has GERD, work with your pediatrician to manage it through feeding techniques, thickened feeds, or medication, as reflux can contribute to airway inflammation.
- Early Intervention for Oral Health: Regular pediatric dental check-ups, as recommended by the ADA, can help identify early signs of craniofacial developmental issues that might impact airway health. A pediatric dentist can assess oral structures and provide guidance.
Risks and Complications of Untreated Infant Snoring and OSA
Ignoring persistent or severe infant snoring, particularly when it indicates Obstructive Sleep Apnea, carries significant risks for your child's health and development.
Developmental and Cognitive Delays
- Brain Development: Fragmented sleep and intermittent oxygen deprivation can impair brain development, leading to long-term cognitive deficits.
- Learning and Behavior: Children with untreated OSA are at a higher risk for attention deficit hyperactivity disorder (ADHD)-like symptoms, learning difficulties, poor academic performance, irritability, and aggression.
- Speech and Language: Chronic mouth breathing and altered facial growth can sometimes contribute to speech articulation problems.
Cardiovascular Complications
- High Blood Pressure: Repeated drops in oxygen and surges in adrenaline during apneic events can lead to systemic hypertension (high blood pressure) later in childhood or adulthood.
- Heart Strain: Over time, the increased effort to breathe against an obstructed airway can put a strain on the heart, potentially leading to cardiac enlargement or dysfunction.
Growth and Metabolic Issues
- Failure to Thrive: The increased metabolic demand of struggling to breathe can divert energy away from growth, leading to poor weight gain and delayed physical development.
- Insulin Resistance: Chronic sleep deprivation and stress responses can contribute to insulin resistance, increasing the risk of type 2 diabetes later in life.
Other Complications
- Chronic Mouth Breathing: Leads to poor facial development, dental issues (e.g., malocclusion, gingivitis), and increased susceptibility to respiratory infections.
- Recurrent Infections: Enlarged adenoids contributing to OSA can also obstruct the Eustachian tubes, leading to recurrent ear infections (otitis media) and hearing problems.
- Increased Risk of Accidents: Daytime sleepiness can increase the risk of accidents in older children.
Comparison Tables
Table 1: Normal Snoring vs. Obstructive Sleep Apnea in Infants
| Feature | Normal Infant Snoring | Obstructive Sleep Apnea (OSA) in Infants |
|---|---|---|
| Sound | Soft, gentle, intermittent | Loud, habitual, often accompanied by gasps, snorts, choking |
| Frequency | Occasional (e.g., with a cold) | Most nights (≥3 nights/week), persistent, loud |
| Breathing Pauses | Rare or very brief, not clinically significant | Frequent, visible pauses in breathing (>5-10 seconds), followed by gasp |
| Effort to Breathe | Minimal to none | Visible chest retractions, nasal flaring, abdominal breathing |
| Oxygen Levels | Stable, no significant drops | Repeated drops in oxygen saturation |
| Sleep Quality | Generally undisturbed, restful sleep | Restless sleep, frequent awakenings, unusual positions |
| Daytime Symptoms | Alert, happy, normal development | Irritability, difficulty waking, daytime sleepiness, poor feeding/growth |
| Long-term Risk | Low, typically benign | High for developmental, cardiovascular, metabolic issues |
| Intervention | Monitor, conservative measures | Medical evaluation, sleep study, specialized treatment (e.g., surgery, CPAP) |
Table 2: Common Treatment Options for Infant Snoring/OSA
| Treatment Option | Target Condition/Cause | Effectiveness for OSA | Typical Cost Range (USD, without insurance) | Recovery/Timeline | Pros | Cons |
|---|---|---|---|---|---|---|
| Nasal Saline/Humidifier | Mild congestion, dry airways | Low | $10-$50 | Immediate; ongoing as needed | Non-invasive, safe, improves comfort | Temporary relief, not for structural issues |
| Allergy Management (e.g., Nasal Steroids) | Allergic rhinitis, inflammation | Moderate | $20-$100/month | Weeks to see full effect; ongoing | Addresses root cause, non-surgical | Requires consistent use, potential mild side effects |
| Adenotonsillectomy | Enlarged tonsils/adenoids (most common) | High | $3,000-$8,000 (including facility, anesthesia) | 1-2 weeks significant pain, full recovery 2-3 weeks | Highly effective for appropriate cases, often curative | Surgical risks, anesthesia, post-op pain, recurrence possible |
| CPAP Therapy | Severe OSA, anatomical issues, non-surgical candidates | High | $1,000-$4,000 (initial setup); $50-$200/month (supplies) | Immediate effect; ongoing nightly | Non-invasive (no surgery), highly effective | Requires consistent adherence, mask fit issues, maintenance |
| Craniofacial Surgery | Severe craniofacial abnormalities | Varies (high for specific cases) | $10,000-$50,000+ (highly variable) | Months to years for full recovery | Life-changing for severe structural issues | Major surgery, significant risks, long recovery |
Children / Pediatric Considerations
The entire article focuses on infants, but it's important to specifically highlight how infant snoring and OSA differ from adult conditions and why a specialized pediatric approach is paramount.
Infants and young children are not simply "mini-adults" when it comes to sleep-disordered breathing. Their anatomy, physiology, and developmental stage present unique challenges and considerations:
- Airway Anatomy: Infants have proportionally larger tongues, softer airways, and smaller mandibles compared to adults, making them more vulnerable to collapse.
- Rapid Development: The rapid growth and development of the brain and body in infancy mean that untreated sleep apnea can have a more profound and lasting impact on neurological and physical growth.
- Symptoms Presentation: Infants cannot verbalize their symptoms. Daytime sleepiness might manifest as irritability or hyperactivity rather than overt drowsiness. Feeding difficulties or poor weight gain are critical clues.
- Diagnosis Challenges: Polysomnography in infants requires specialized pediatric sleep labs with staff experienced in monitoring and comforting babies. Normal AHI thresholds are lower for infants.
- Treatment Limitations: As discussed, adult anti snoring mouth guard devices are completely inappropriate. CPAP therapy for infants requires highly specialized masks and extensive parental training and support. Surgical decisions (like adenotonsillectomy) are made after careful consideration of age, severity, and potential impact.
- Dental and Craniofacial Development: Pediatric dentists play a crucial role, especially as the infant grows into a toddler and child. They can identify early signs of malocclusion or jaw development issues that might contribute to airway obstruction. Collaboration between pediatricians, ENTs, sleep specialists, and pediatric dentists is often necessary for comprehensive care. The ADA emphasizes the importance of early oral health assessment in overall pediatric health.
Cost Breakdown for Infant Snoring Diagnosis & Treatment
While general ranges were provided, a more detailed breakdown helps parents budget and understand potential financial obligations.

Average US Costs
- Initial Pediatrician Visit: $100 - $500
- Specialist Consultations (ENT, Sleep Physician): $200 - $800 per visit
- Polysomnography (Sleep Study):
- Low: $1,000 (outpatient, less complex)
- Mid: $2,500 - $3,500 (standard pediatric sleep lab)
- High: $4,000 - $5,000+ (complex cases, university hospitals)
- Adenotonsillectomy:
- Surgeon's Fee: $1,000 - $3,000
- Anesthesia Fee: $500 - $2,000
- Facility Fee (Hospital/Surgical Center): $1,500 - $3,000
- Total Average: $3,000 - $8,000
- CPAP Therapy (initial setup):
- Machine: $500 - $2,000
- Mask and Tubing: $100 - $500
- Initial Consultation/Fitting: $200 - $500
- Total Average: $1,000 - $4,000
With vs. Without Insurance
- Without Insurance: You are responsible for 100% of these costs. Facilities may offer prompt-pay discounts or charity care options.
- With Insurance:
- Deductible: This is the amount you must pay out-of-pocket before your insurance begins to cover costs. Family deductibles often range from $1,000 to $10,000+.
- Co-pay: A fixed amount you pay for a doctor's visit or prescription (e.g., $30-$75).
- Co-insurance: Once your deductible is met, your insurance typically covers a percentage of costs (e.g., 80%), and you pay the remaining percentage (e.g., 20%).
- Out-of-Pocket Maximum: A cap on the total amount you will pay in a plan year for covered medical expenses. Once this is reached, insurance covers 100% of covered costs. Family maximums often range from $5,000 to $15,000+.
Example: If your family deductible is $3,000 and an adenotonsillectomy costs $5,000:
- You pay the first $3,000 (your deductible).
- The remaining $2,000 is subject to co-insurance. If your co-insurance is 20%, you pay $400, and your insurance pays $1,600.
- Your total out-of-pocket for the surgery would be $3,400 (plus any specialist co-pays leading up to it).
Payment Plans and Financing Options
- Hospital Payment Plans: Many hospitals offer interest-free payment plans for medical bills. Inquire with the billing department.
- CareCredit and Other Medical Credit Cards: These offer deferred interest or low-interest financing for healthcare expenses. Be aware of the terms and conditions.
- Health Savings Accounts (HSAs) and Flexible Spending Accounts (FSAs): These tax-advantaged accounts allow you to save money specifically for medical expenses. They can significantly reduce your out-of-pocket burden.
Cost-Saving Tips
- Verify In-Network Providers: Always ensure all providers (surgeon, anesthesiologist, facility) are in-network with your insurance plan to avoid higher out-of-network costs.
- Obtain Prior Authorizations: For sleep studies, surgeries, or CPAP equipment, your insurance often requires prior authorization. Ensure your doctor's office handles this promptly.
- Negotiate Cash Prices: If you are uninsured or have a high deductible, ask for prompt-pay discounts for upfront payment.
- Review Your Bill: Carefully review all itemized bills for accuracy and question any charges you don't understand.
Frequently Asked Questions
What sounds are normal for a baby sleeping?
Infants often make various sounds during sleep, including grunts, sighs, snorts, and soft gurgles, due to their small, developing airways and often rapid, irregular breathing patterns. Occasional soft snoring, especially with a cold or in certain positions, can also be normal. However, consistently loud snoring, pauses in breathing, or gasping sounds are not normal and warrant medical evaluation.
How can I tell if my infant's snoring is serious?
Serious infant snoring is typically loud, happens most nights, and is accompanied by other symptoms such as visible breathing pauses, gasping for air, restless sleep, waking up tired or irritable, excessive daytime sleepiness, or difficulty feeding. If you notice any of these signs, particularly breathing pauses or gasping, consult your pediatrician promptly.
Is infant snoring linked to SIDS?
While sleep-disordered breathing and OSA are not the same as Sudden Infant Death Syndrome (SIDS), studies indicate that infants with OSA may have an increased risk of SIDS. The exact relationship is complex, but both conditions are associated with sleep disturbances and respiratory control issues. Proper diagnosis and treatment of OSA are crucial for reducing health risks, including those potentially related to SIDS.
At what age can an infant have a sleep study?
Infants of any age, including newborns and premature babies, can undergo a polysomnography (sleep study). Specialized pediatric sleep labs are equipped to handle even the youngest patients, with trained staff who understand the unique needs and physiological characteristics of infants.
Are anti-snoring mouth guards effective for infants?
No, anti snoring mouth guards and similar oral appliances designed for adults are absolutely not suitable or effective for infants. Infant oral anatomy is vastly different, and their jaws are still developing. Pediatric sleep apnea requires specialized medical or surgical interventions, not adult oral appliances.
Where can I find sleep apnea mouth guard reviews for children?
You will not find reliable or appropriate sleep apnea mouth guard reviews for infants because these devices are not used for this age group. If you are looking for information on oral appliances for older children or adolescents, always consult a pediatric sleep dentist or orthodontist specializing in airway issues, as custom-fitted appliances may be considered in specific cases, but never for infants.
What is adenotonsillectomy, and is it safe for babies?
Adenotonsillectomy is a surgical procedure to remove the tonsils and adenoids. It is a common and generally safe procedure for infants and children with obstructive sleep apnea caused by enlarged tissues. The decision for surgery is made carefully by a pediatric ENT specialist after a thorough evaluation and sleep study, considering the child's age and overall health. Risks, though rare, include bleeding, infection, and anesthesia complications.
How long does recovery from adenotonsillectomy take for an infant?
Recovery from an adenotonsillectomy typically takes about 7 to 14 days. During this time, infants will experience a sore throat, may have difficulty eating, and require close monitoring for pain and potential complications like bleeding. Most discomfort subsides within the first week, but full recovery of normal eating and activity may take a bit longer.
Can allergies cause infant snoring?
Yes, allergies can cause inflammation and swelling in the nasal passages and throat, leading to congestion and contributing to infant snoring. Managing allergies through environmental controls and, if necessary, prescribed medications (under a doctor's guidance), can significantly improve snoring related to allergic rhinitis.
Will my infant outgrow snoring?
Some infants may outgrow mild, temporary snoring, especially if it's related to occasional congestion or minor anatomical factors that resolve with growth. However, if snoring is habitual, loud, and especially if it's due to enlarged tonsils/adenoids or other significant medical conditions, it is unlikely to be outgrown without intervention. It's crucial to have it evaluated rather than waiting for them to "grow out of it."
When to See a Dentist for Infant Snoring
While your pediatrician or a pediatric ENT will be your primary contacts for infant snoring, a pediatric dentist plays an important, albeit sometimes secondary, role, especially regarding the development of the oral and craniofacial structures that impact the airway.
You should consult a pediatric dentist in the following situations:
- Referral from Pediatrician/Specialist: If your pediatrician or an ENT suspects that issues with oral development, jaw structure, or tongue tie (ankyloglossia) might be contributing to your infant's snoring or feeding difficulties that indirectly affect breathing.
- Visible Oral/Craniofacial Anomalies: If you notice any obvious structural differences in your infant's mouth, jaw, or palate that could affect their airway, such as a very recessed chin, a high arched palate, or a significant tongue tie.
- Concerns about Tongue Tie or Lip Tie: While controversial in some aspects, severe tongue or lip ties can sometimes impact proper feeding, potentially leading to compensatory mouth breathing and indirectly influencing airway patency. A pediatric dentist can assess the severity and discuss potential interventions like a frenectomy.
- Chronic Mouth Breathing: Persistent mouth breathing, even without obvious snoring, can impact facial growth and dental development. A pediatric dentist can monitor these aspects and discuss strategies to encourage nasal breathing as your child grows.
- Early Assessment of Craniofacial Development: The American Dental Association (ADA) recommends a first dental visit by age one. This visit allows the pediatric dentist to assess overall oral health and identify any early developmental patterns that might predispose a child to future airway issues, offering anticipatory guidance.
Red Flags that Need Immediate Attention (Call 911 or go to ER):
- Bluish discoloration of the lips, face, or chest (cyanosis).
- Severe difficulty breathing, gasping, or struggling for air.
- Periods of apnea lasting longer than 15-20 seconds, especially if the infant goes limp or unresponsive.
- Loud, high-pitched squeaking noises (stridor) during inhalation, indicating severe upper airway obstruction.
For less urgent but concerning symptoms (loud habitual snoring, frequent breathing pauses, restless sleep, daytime irritability), schedule an appointment with your pediatrician as soon as possible. Do not delay, as early diagnosis and intervention are critical for an infant's developing health.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Difference Between Snoring and Sleep Apnea: Complete Guide
More than 80 million Americans regularly snore, and while often dismissed as a mere nuisance, loud and persistent snoring can be a critical indicator of a much more serious underlying health condition: sleep apnea. The difference between snoring and sleep apnea is profound, impacting not just yo
February 23, 2026
Mouth Taping for Snoring: Complete Guide
Snoring. It's the nocturnal soundtrack for millions of Americans, often a source of frustration for bed partners and a potential indicator of underlying health issues for the snorer themselves. Roughly 45% of adults snore occasionally, and 25% are habitual snorers, impacting sleep quality, relat
February 23, 2026

Is All Snoring Sleep Apnea
Many individuals, perhaps even you or a loved one, have been told they snore loudly. It's often dismissed as a harmless, albeit annoying, nocturnal habit. However, what if that nightly rumble is more than just noise? What if it's a critical indicator of an underlying health condition that significan
February 23, 2026
Cpap Dry Mouth Even With Humidifier: Complete Guide
Experiencing dry mouth while using a CPAP machine, even with a humidifier, is a common and incredibly frustrating issue for millions of Americans. It can disrupt sleep, diminish the effectiveness of your sleep apnea treatment, and significantly impact your oral health. Imagine waking up every mornin
February 23, 2026