Baby Snoring Normal: Complete Guide
Key Takeaways
- Waking up to the gentle sounds of your baby sleeping can be one of life's greatest joys, but what if those sounds include a soft snore? As many as 10-12% of infants snore regularly, a figure that often leaves parents wondering: is baby snoring normal, or is it a sign of something more seriou
Baby Snoring Normal: Complete Guide
Waking up to the gentle sounds of your baby sleeping can be one of life's greatest joys, but what if those sounds include a soft snore? As many as 10-12% of infants snore regularly, a figure that often leaves parents wondering: is baby snoring normal, or is it a sign of something more serious? This concern is entirely valid, as distinguishing between innocent, occasional baby snoring and a red flag for a condition like sleep apnea is crucial for your child's health and development. Understanding the nuances of your baby's breathing patterns can help you know when to simply cherish their slumber and when to seek professional advice.

This comprehensive guide from SmilePedia.net aims to provide you with all the information you need regarding baby snoring. We'll delve into the various causes, explain how to differentiate between normal snoring and sleep apnea, explore available treatment options, discuss costs, and empower you with the knowledge to ensure your little one breathes easy and sleeps soundly.
Key Takeaways:
- Occasional, soft baby snoring can be normal, especially due to temporary nasal congestion.
- Persistent, loud snoring accompanied by gasping, pauses in breathing, or struggling warrants immediate medical evaluation.
- Pediatric obstructive sleep apnea (OSA) affects 1-5% of children and can have serious developmental and health consequences if untreated.
- Diagnosis typically involves a pediatric sleep specialist and a sleep study (polysomnography), which can cost anywhere from $1,000 to $5,000+ without insurance.
- Primary treatments for pediatric OSA often include adenotonsillectomy, costing $3,000 to $8,000+ (before insurance), or, less commonly in infants, positive airway pressure (PAP) therapy.
- Oral appliances (like mouth guards for sleep apnea) are generally not suitable for infants and young children; they are typically prescribed for older children and adults with mild to moderate OSA.
- Early intervention is key: Consult a pediatrician if you have any concerns about your baby's snoring or breathing during sleep.
What Is Baby Snoring? An Overview
Snoring, at its core, is the sound produced when air flows past relaxed tissues in the throat, causing them to vibrate. In babies, this mechanism is similar, but their smaller, more delicate airways make them particularly susceptible to airflow disturbances. The sound can range from a soft, barely audible rumble to a louder, more noticeable rasp.
Understanding the anatomy involved is key. A baby's airway consists of the nasal passages, the pharynx (throat), and the larynx (voice box) leading to the trachea (windpipe) and lungs. Any obstruction or narrowing in these upper airway structures can impede smooth airflow, leading to snoring. Factors such as a baby's rapid growth, the position they sleep in, and even the presence of temporary mucus can influence whether they snore. While adult snoring is often linked to lifestyle factors like diet or alcohol, baby snoring is almost exclusively an anatomical or physiological issue.
The Spectrum of Baby Breathing Sounds
It's important for parents to recognize the wide range of sounds a baby makes during sleep. These can include:
- Soft snorts or grunts: Often due to nasal passages clearing or mucus moving.
- Whistling: Typically from minor nasal blockage.
- Congested breathing: Sounds wet or rattling, especially when a baby has a cold.
- Occasional, soft snoring: The focus of this article, often harmless.
- Loud, persistent snoring: A potential red flag.
- Gasping, choking, or pauses in breathing: Immediate concern, indicative of sleep apnea.
Types of Snoring in Babies: Normal vs. Problematic
Not all snoring is created equal. Differentiating between benign, normal snoring and snoring that signals a health concern is the most critical aspect for parents.
Normal (Primary) Snoring
This refers to snoring that occurs without any associated breathing difficulties or interruptions during sleep. It's often:
- Intermittent: Happens occasionally, not every night.
- Soft and quiet: Not excessively loud or disruptive.
- Not accompanied by other symptoms: The baby seems well-rested, alert during the day, and feeding/growing normally.
- Often linked to temporary factors: Like a stuffy nose from a cold, allergies, or sleeping position.
Many babies, especially newborns, are obligate nasal breathers, meaning they primarily breathe through their noses. Even minor congestion can lead to snoring. Their nasal passages are tiny and easily blocked.
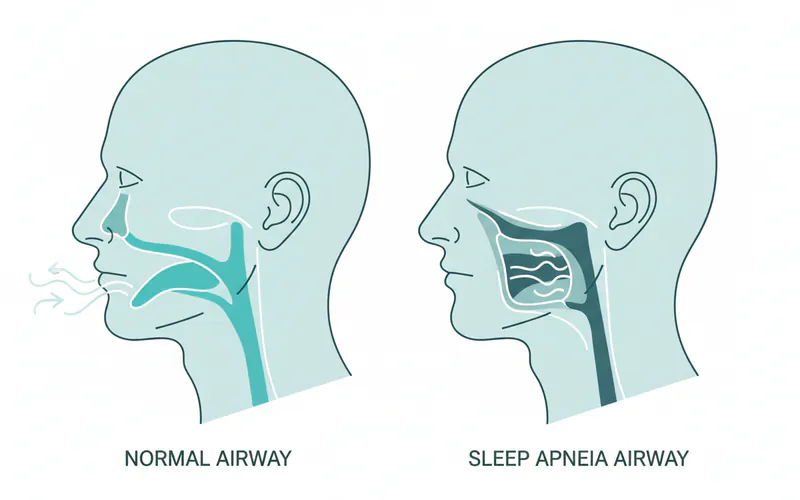
Problematic Snoring and Obstructive Sleep Apnea (OSA)
This is where snoring vs sleep apnea becomes the key distinction. Problematic snoring is often a symptom of pediatric obstructive sleep apnea (OSA), a condition where the upper airway repeatedly becomes partially or completely blocked during sleep, leading to reduced or absent airflow despite efforts to breathe. This can cause oxygen levels to drop and sleep to be fragmented.
Signs that snoring might be problematic and indicative of OSA include:
- Loud, persistent snoring: Happens nightly and is very noticeable.
- Snoring with gasps, chokes, or pauses in breathing: These apneic events can last for several seconds.
- Struggling to breathe: Chest retraction (the skin pulling in around the ribs or collarbone), flaring nostrils.
- Cyanosis: A bluish tint to the lips or skin, indicating low oxygen (a medical emergency).
- Restless sleep: Frequent awakenings, unusual sleep positions (e.g., neck hyperextended).
- Excessive daytime sleepiness: Though in babies and young children, this can manifest as hyperactivity, irritability, or difficulty concentrating (paradoxical effect).
- Poor feeding and weight gain: Due to increased effort of breathing during sleep and poor sleep quality.
- Developmental delays or learning difficulties: In older infants and children.
Pediatric OSA affects approximately 1-5% of children, with peak incidence between 2 and 8 years of age, often coinciding with the growth of tonsils and adenoids. However, it can occur in infants as well.
Causes of Baby Snoring
Understanding why a baby snores is the first step in determining if it's benign or a cause for concern.
Common, Benign Causes:
- Nasal Congestion: The most frequent cause. Babies have very small nasal passages, and even a small amount of mucus from a cold, allergies, or dry air can cause obstruction and snoring.
- Pro Tip: Use a cool-mist humidifier in the baby's room and saline nasal drops to help loosen mucus.
- Sleeping Position: Babies often snore more when sleeping on their back, as gravity can cause the tongue and soft palate to relax and fall slightly backward, narrowing the airway.
- Pro Tip: While back sleeping is recommended to reduce SIDS risk, ensure their head is not excessively flexed forward. If snoring persists, discuss sleeping position with your pediatrician.
- Anatomical Variations (Minor): Some babies naturally have slightly narrower airways, smaller nostrils, or a more flexible larynx (laryngomalacia), which can cause noisy breathing that is often outgrown.
- Dry Air: A dry environment can irritate nasal passages and make mucus thicker, contributing to congestion and snoring.
Causes of Problematic Snoring / Obstructive Sleep Apnea (OSA):
- Enlarged Tonsils and Adenoids: This is the number one cause of pediatric OSA. The tonsils are located at the back of the throat, and the adenoids are higher up behind the nose. When these lymphoid tissues become enlarged (often due to recurrent infections or simply being large for the child's airway), they can block the airway during sleep.
- Obesity: While less common in infants, obesity in older children can contribute to OSA by increasing soft tissue around the neck and airway.
- Craniofacial Anomalies: Certain genetic syndromes or birth defects that affect the structure of the jaw, face, or airway can predispose a baby to OSA. Examples include Down syndrome, Pierre Robin sequence, or Treacher Collins syndrome.
- Neuromuscular Disorders: Conditions that affect muscle tone can lead to airway collapse during sleep.
- Allergies and Asthma: Chronic inflammation and swelling of the nasal passages and throat due to allergies can contribute to airway obstruction. Asthma can also lead to increased respiratory effort.
- Gastroesophageal Reflux Disease (GERD): Acid reflux can irritate and swell the throat tissues, potentially contributing to snoring and apnea.
- Hypotonia (Low Muscle Tone): Babies with conditions causing low muscle tone may have a weaker airway that is more prone to collapse during sleep.
Signs and Symptoms: When to Watch Closely
Observing your baby during sleep is vital. Here’s a detailed list of signs and symptoms to look for:
During Sleep:
- Loud, consistent snoring: Not just occasional, but every night or most nights.
- Gasping or choking sounds: The baby suddenly makes a loud noise as if struggling for air.
- Pauses in breathing (apnea): You notice your baby stops breathing for several seconds, followed by a gasp or snort. Note that brief pauses (up to 5-10 seconds) are common in newborns (periodic breathing) but should be distinguished from longer, more frequent, or effortful pauses.
- Retractions: The skin pulling in noticeably around the ribs or collarbone with each breath, indicating increased effort to breathe.
- Nostril flaring: Widening of the nostrils with each breath, another sign of increased respiratory effort.
- Restless sleep: Tossing and turning, unusual sleeping positions, sweating excessively during sleep.
- Bluish tint to lips or skin (Cyanosis): A serious sign of low oxygen. Seek immediate medical attention.
While Awake:
- Daytime sleepiness: Your baby may seem excessively tired, lethargic, or fall asleep easily during feeds or playtime. In toddlers and older children, this can paradoxically manifest as hyperactivity, aggression, or difficulty paying attention.
- Difficulty feeding: Babies with OSA may struggle to coordinate breathing and sucking, leading to poor intake and weight gain.
- Irritability or behavioral issues: Due to chronic sleep deprivation.
- Mouth breathing: Consistently breathing through the mouth, especially when awake, can be a sign of chronic nasal obstruction.
- Speech delays or nasal voice: Chronic nasal obstruction can affect speech development.
- Poor weight gain or failure to thrive: In infants, this is a significant indicator.
Diagnosis of Pediatric Obstructive Sleep Apnea
If you observe any concerning signs, the first step is to consult your pediatrician. They will perform a physical examination and may refer you to a specialist.
-
Pediatrician Visit: The pediatrician will take a detailed medical history, including your observations of your baby's sleep, feeding, and development. They will examine your baby's throat, nose, and jaw.
-
ENT Specialist Referral (Otolaryngologist): Often, if enlarged tonsils or adenoids are suspected, a referral to an Ear, Nose, and Throat (ENT) specialist is made. The ENT can examine these tissues more closely, sometimes using a small camera (nasal endoscope).
-
Sleep Study (Polysomnography - PSG): This is the gold standard for diagnosing sleep apnea in children. It's a non-invasive overnight study conducted in a specialized sleep lab. During the study, various parameters are monitored:
- Brain activity (EEG)
- Eye movements (EOG)
- Muscle activity (EMG)
- Heart rate (ECG)
- Breathing effort
- Airflow through the nose and mouth
- Blood oxygen levels (oximetry)
- Carbon dioxide levels (capnography)
- Snoring and body position
The sleep study helps determine the severity of apnea-hypopnea events and their impact on oxygen levels and sleep architecture.
Treatment Options for Problematic Snoring and OSA
Treatment depends entirely on the underlying cause and severity of the condition. For simple, benign snoring, conservative measures are often sufficient. For diagnosed OSA, more specific interventions are needed.
Conservative and Non-Surgical Treatments:
- Nasal Saline and Humidifiers: For snoring due to congestion, saline nasal drops can thin mucus, and a cool-mist humidifier can moisten nasal passages.
- Addressing Allergies: If allergies are contributing, identifying and avoiding allergens, along with pediatrician-prescribed antihistamines or nasal steroid sprays, can help.
- Positional Therapy: Ensuring the baby sleeps on their back (as per SIDS guidelines) but ensuring the neck is not excessively flexed. For older children, sleeping on their side might reduce snoring, but this is not recommended for infants.
- Weight Management: For older children with obesity-related OSA, lifestyle changes and weight loss are crucial.
- CPAP (Continuous Positive Airway Pressure): While typically associated with adults, CPAP can be used in children and even infants with severe OSA, especially when other treatments aren't suitable or effective (e.g., in children with craniofacial anomalies or neuromuscular disorders). A small mask is worn over the nose (or nose and mouth) to deliver pressurized air, keeping the airway open.
- Oral Appliances / Mouth Guards for Sleep Apnea: It's important to clarify: oral appliances and mouth guards for sleep apnea are almost exclusively used for older children (often adolescents) and adults with mild to moderate OSA. These custom-fitted devices work by repositioning the jaw and/or tongue to keep the airway open. They are not suitable or safe for infants and very young children due to their developing dental structures and potential for airway obstruction. If you hear about mouth guards for sleep apnea, understand this generally applies to a different age group and clinical scenario than infant snoring.
Surgical Treatment:
- Adenotonsillectomy: This is the most common and often most effective treatment for pediatric OSA caused by enlarged tonsils and adenoids. The surgical removal of these tissues opens up the airway.
- Pros: High success rate in resolving OSA symptoms (around 80-90% for uncomplicated cases).
- Cons: General anesthesia risks, post-operative pain and recovery period, risk of bleeding or infection, and potential for residual OSA in some cases.
- Other Airway Surgeries: In cases of severe craniofacial anomalies, other surgeries such as palate expansion or jaw advancement may be considered, often performed by a specialized craniofacial surgeon.
Step-by-Step Process: What to Expect During Treatment
The journey from suspicion to resolution for problematic baby snoring often follows a clear path:
- Initial Consultation with Pediatrician: Share your observations and concerns. The pediatrician will conduct an initial assessment.
- Referral to Specialist (ENT or Sleep Specialist): If concerns persist, a referral will be made.
- Diagnostic Testing:
- ENT Exam: The ENT specialist will visually inspect the tonsils and might perform a flexible nasopharyngoscopy to visualize the adenoids and other airway structures.
- Sleep Study (PSG): If OSA is suspected, an overnight sleep study will be scheduled. This involves a night in a pediatric sleep lab, where your baby's vital signs and sleep patterns are monitored. Parents usually stay with the child.
- Diagnosis and Treatment Plan Development: Based on the sleep study results and specialist examinations, a definitive diagnosis will be made. The specialist will discuss treatment options tailored to your child's specific condition.
- Implementation of Treatment:
- Adenotonsillectomy: If surgery is chosen, you'll meet with the surgical team (surgeon, anesthesiologist). The procedure is typically outpatient or involves a short hospital stay.
- CPAP: If CPAP is recommended, you'll work with a respiratory therapist to find the right mask and pressure settings, and learn how to use and maintain the equipment at home.
- Conservative Measures: If the cause is benign, the pediatrician will guide you on home remedies and monitoring.
- Follow-up Care: Regular follow-up appointments with the specialist are crucial to monitor progress, assess the effectiveness of treatment, and address any lingering issues. A repeat sleep study may be recommended several months after surgery or starting CPAP to confirm resolution or improvement.

Cost and Insurance Considerations in the US
The cost of diagnosing and treating problematic baby snoring, particularly pediatric OSA, can be substantial in the US. Prices vary widely based on location, facility, and insurance coverage.
Diagnostic Costs:
| Service | Average Cost (Without Insurance) | Insurance Coverage | Notes |
|---|---|---|---|
| Pediatrician Visit | $100 - $300 | Usually good | Covered by most plans; often a co-pay. |
| ENT Specialist Visit | $200 - $500 | Varies | May require a referral; specialist co-pay. |
| Overnight Sleep Study (PSG) | $1,000 - $5,000+ | Varies widely | Often requires prior authorization. Hospital-based studies are more expensive than independent labs. Fees include facility, physician interpretation. |
| Nasal Endoscopy | $300 - $800 | Varies | If performed in-office, may be bundled with specialist visit. |
Treatment Costs:
| Service | Average Cost (Without Insurance) | Insurance Coverage | Notes |
|---|---|---|---|
| Adenotonsillectomy | $3,000 - $8,000+ | Usually good | Includes surgeon's fee, anesthesia, facility fees. Most commonly covered when medically necessary. Deductibles and co-insurance apply. |
| CPAP Machine & Supplies | Machine: $500 - $3,000+ (one-time) | Varies | Many plans cover CPAP as durable medical equipment (DME), often with rental-to-own agreements. Masks and tubing (monthly/quarterly): $50-$200. |
| Oral Appliances (for older children/adults) | $1,800 - $3,500+ | Limited | Less common for pediatric use. May be covered by medical or dental insurance, but often considered elective or out-of-network. |
| Allergy Medications/Sprays | $10 - $100+ (monthly) | Varies | Over-the-counter options are cheaper. Prescription drugs are usually covered with a co-pay. |
Insurance Coverage:
- Most commercial insurance plans and Medicaid/CHIP programs cover medically necessary diagnostic tests (like sleep studies) and treatments (like adenotonsillectomy) for pediatric OSA.
- Prior authorization is almost always required for sleep studies, CPAP machines, and surgical procedures. Failure to obtain this can lead to significant out-of-pocket costs.
- Be aware of your plan's deductible, co-pay, and co-insurance amounts. You'll likely be responsible for these.
- Out-of-network providers can significantly increase costs. Always confirm that all providers involved (e.g., surgeon, anesthesiologist, facility) are in-network.
Payment Plans and Financing Options:
- Many hospitals and clinics offer payment plans to spread costs over several months.
- Healthcare credit cards (e.g., CareCredit) offer deferred interest periods, but high interest rates if not paid off on time.
- Health Savings Accounts (HSAs) and Flexible Spending Accounts (FSAs) allow you to use pre-tax dollars for medical expenses, significantly reducing your out-of-pocket burden.
Recovery and Aftercare for Pediatric OSA Treatment
Recovery specifics depend on the treatment method.
After Adenotonsillectomy:
- Pain Management: Pain is common, especially throat pain, and will be managed with prescribed pain relievers (e.g., acetaminophen, ibuprofen).
- Diet: A soft diet is recommended for 7-10 days to avoid irritating the surgical site. Cold liquids and soft foods like popsicles, yogurt, and mashed potatoes are good choices. Avoid hot, spicy, or sharp foods.
- Hydration: Crucial to prevent dehydration. Offer small, frequent sips of liquids.
- Activity: Limit strenuous activity for 1-2 weeks. Quiet play is generally fine.
- Bleeding Risk: The highest risk of bleeding is within the first 24 hours and around 7-10 days post-op (when scabs typically fall off). Watch for bright red blood in spit-up or vomiting.
- Follow-up: A post-operative check-up is usually scheduled within 1-2 weeks. A repeat sleep study may be performed 3-6 months later to confirm resolution of OSA.
After Starting CPAP:
- Adaptation Period: It can take time for a baby or child to get used to wearing the mask. Patience and positive reinforcement are key.
- Mask Fit: Ensuring a proper mask fit is crucial to prevent leaks and skin irritation. Regular adjustments may be needed as the child grows.
- Cleaning: Regular cleaning of the mask, tubing, and humidifier chamber is essential to prevent infections.
- Troubleshooting: You'll learn how to troubleshoot common issues like mask leaks, dry mouth, or discomfort.
- Ongoing Monitoring: Regular follow-ups with the sleep specialist and respiratory therapist are important to monitor progress, adjust settings, and address any challenges.
Prevention: Minimizing the Risk of Problematic Snoring
While some causes of snoring (like anatomical anomalies) aren't preventable, you can take steps to reduce the likelihood of problematic snoring and OSA:
- Breastfeeding: Some studies suggest that breastfeeding, especially exclusive breastfeeding, may be protective against OSA in early childhood, possibly due to promoting optimal craniofacial development.
- Manage Allergies: If your baby has allergies, work with your pediatrician to manage them effectively to reduce nasal and throat inflammation.
- Maintain a Healthy Weight: For older infants and children, ensuring they maintain a healthy weight reduces the risk of obesity-related OSA.
- Clear Nasal Passages: Use saline drops and a nasal aspirator (bulb syringe or electric aspirator) as needed to keep nasal passages clear, especially during colds. A humidifier can also help.
- Smoke-Free Environment: Exposure to secondhand smoke is a significant risk factor for respiratory issues, including enlarged tonsils and adenoids, and respiratory infections, all of which contribute to snoring and OSA.
- Address GERD: If your baby has GERD, working with your pediatrician to manage it can reduce airway irritation.
Risks and Complications of Untreated Pediatric OSA
Leaving pediatric OSA untreated can have significant, long-term consequences for a child's health and development:
- Developmental and Cognitive Impairment: Chronic sleep deprivation and intermittent oxygen deprivation can affect brain development, leading to learning difficulties, poor academic performance, attention deficit hyperactivity disorder (ADHD)-like symptoms, and behavioral problems (irritability, aggression).
- Cardiovascular Problems: Long-term untreated OSA can strain the heart, leading to high blood pressure (hypertension), pulmonary hypertension, and, in severe cases, right-sided heart failure.
- Growth Delays: Poor sleep and the increased metabolic effort of breathing can interfere with growth hormone release and overall growth, leading to poor weight gain or failure to thrive in infants.
- Metabolic Issues: OSA has been linked to insulin resistance and an increased risk of type 2 diabetes later in life.
- Quality of Life: The child's and family's quality of life can be significantly impacted by fragmented sleep, daytime fatigue, and behavioral challenges.
- Increased Risk of Accidents: For older children, daytime sleepiness can increase the risk of accidents.
Children / Pediatric Considerations
Children are not just miniature adults when it comes to sleep and dental health. Their rapidly developing bodies and unique physiology require specialized consideration.
- Anatomical Differences: Infants and young children have smaller, more flexible airways, larger tongues in proportion to their mouths, and often relatively larger tonsils and adenoids, making them more prone to airway obstruction.
- Symptoms Presentation: As mentioned, daytime sleepiness in children often presents as hyperactivity, aggression, or difficulty concentrating, rather than overt fatigue. This can lead to misdiagnosis as behavioral problems or ADHD.
- Diagnosis Challenges: Sleep studies can be more challenging to conduct and interpret in very young children. The parameters for diagnosing OSA are also age-adjusted.
- Treatment Limitations: While adenotonsillectomy is highly effective for many children, CPAP compliance can be difficult for young ones. Oral appliances are generally not an option until permanent teeth have erupted and facial growth is nearing completion (typically adolescence).
- Impact on Development: The critical period of brain development in early childhood means that untreated sleep apnea can have profound and lasting effects on cognitive function, behavior, and physical growth.
Pro Tip: Always seek evaluation from a pediatric sleep specialist or a pediatric ENT when dealing with concerns about your baby's snoring or sleep breathing. General practitioners may not have the specialized knowledge required for optimal pediatric care in this area.
Cost Breakdown: Understanding the Financial Picture
To reiterate the cost aspects, here's a more detailed look, emphasizing the financial planning involved.
| Cost Category | Low Estimate (USD) | Mid Estimate (USD) | High Estimate (USD) | Notes |
|---|---|---|---|---|
| Initial Consults | ||||
| Pediatrician | $100 | $200 | $300 | Co-pays often apply. |
| ENT Specialist | $200 | $350 | $500 | May vary if procedures (like endoscopy) are done during the visit. |
| Diagnostic Tests | ||||
| Overnight Sleep Study (PSG) | $1,000 | $3,000 | $5,000+ | Varies by facility type (hospital vs. standalone lab) and region. |
| Treatment (Surgical) | ||||
| Adenotonsillectomy | $3,000 | $5,500 | $8,000+ | Includes surgeon, anesthesia, facility fees. Complications increase cost. |
| Treatment (Non-Surgical) | ||||
| CPAP Machine | $500 | $1,500 | $3,000+ | Costs can be spread out via rental-to-own agreements. |
| CPAP Supplies (annual) | $600 | $1,200 | $2,400+ | Masks, tubing, filters – ongoing expense. |
| Oral Appliance (for older children/adults) | $1,800 | $2,500 | $3,500+ | Custom-made; less common in pediatric OSA management. |
With vs. Without Insurance:
- With Insurance: You will typically be responsible for your deductible (which can range from $500 to $5,000+ for family plans) and co-insurance (e.g., 10-30% of the allowed charges after the deductible is met), up to your annual out-of-pocket maximum. Co-pays apply to individual visits.
- Without Insurance: You will be responsible for 100% of all charges. Negotiating cash prices directly with providers may be possible, but costs can still be prohibitive.
Cost-Saving Tips:
- Verify Insurance Coverage: Before any appointment or procedure, call your insurance company to understand your benefits, deductibles, co-pays, co-insurance, and out-of-pocket maximums. Inquire about specific procedure codes (e.g., for adenotonsillectomy or a sleep study).
- Prior Authorization: Always ensure prior authorization is obtained for costly tests and treatments.
- In-Network Providers: Confirm that all providers (doctors, anesthesiologists, labs) are in-network to avoid surprise bills.
- Generic Medications: Opt for generic versions of prescription medications if available.
- HSAs/FSAs: Utilize pre-tax health savings or flexible spending accounts to cover medical expenses.
- Hospital Financial Assistance: Many hospitals offer financial assistance programs or charity care for families meeting certain income criteria. Inquire with the billing department.
- Shop Around (when possible): For non-urgent procedures or equipment, compare prices between different facilities or DME suppliers if your insurance allows.
Frequently Asked Questions
Is all baby snoring bad?
No, not all baby snoring is bad. Occasional, soft snoring, especially when your baby has a stuffy nose or during certain sleep positions, can be quite normal and benign. The concern arises when snoring is loud, persistent, and accompanied by other symptoms like gasping, pauses in breathing, or daytime behavioral changes.
How can I tell the difference between normal snoring and sleep apnea in my baby?
Normal snoring is typically quiet, infrequent, and your baby appears well-rested. Sleep apnea, however, involves loud, regular snoring with gasps, chokes, or visible pauses in breathing that last several seconds. Babies with sleep apnea may also struggle to breathe, have restless sleep, or show signs of chronic tiredness (like hyperactivity or poor feeding) during the day.
What are the main causes of baby snoring?
The most common benign causes are nasal congestion from colds, allergies, or dry air, and certain sleep positions. Problematic snoring, indicative of sleep apnea, is most frequently caused by enlarged tonsils and adenoids, but can also be due to obesity, craniofacial anomalies, or neuromuscular disorders.
Can a mouth guard for sleep apnea be used for my baby?
No, oral appliances or mouth guards for sleep apnea are generally not suitable for infants or very young children. These devices are custom-fitted for older children (typically adolescents) and adults whose dental and facial structures are more developed. For infants, treatment focuses on addressing underlying causes like enlarged tonsils/adenoids or, in severe cases, CPAP therapy.
What is a sleep study (polysomnography) for a baby like?
A sleep study for a baby involves an overnight stay in a specialized pediatric sleep lab, usually with a parent present. Sensors are painlessly attached to monitor brain activity, breathing, heart rate, oxygen levels, and muscle movements. The baby sleeps as naturally as possible while data is collected, providing a comprehensive picture of their sleep and breathing patterns.
How much does an adenotonsillectomy cost for a baby in the US?
Without insurance, an adenotonsillectomy can cost anywhere from $3,000 to over $8,000 in the US, depending on the facility, surgeon's fees, and anesthesia costs. With insurance, you would typically pay your deductible and co-insurance, up to your annual out-of-pocket maximum. Most insurance plans cover this procedure when it's medically necessary.
How long does it take for a baby to recover from adenotonsillectomy?
Recovery from adenotonsillectomy typically takes 7 to 14 days. During this time, pain management is crucial, and a soft diet is recommended. Limiting strenuous activity for 1-2 weeks helps prevent complications like bleeding. Follow-up appointments are essential to monitor healing and assess the improvement in breathing.
Are there any natural remedies for baby snoring?
For benign snoring due to congestion, natural remedies include using a cool-mist humidifier in the baby's room, using saline nasal drops to loosen mucus, and ensuring a smoke-free environment. However, these are not treatments for obstructive sleep apnea. Always consult your pediatrician for persistent or concerning snoring.
What are the long-term effects if my baby's sleep apnea goes untreated?
Untreated pediatric sleep apnea can lead to serious long-term complications including developmental and cognitive delays, behavioral problems (such as hyperactivity), cardiovascular issues (like high blood pressure), growth problems, and an increased risk of metabolic disorders. Early diagnosis and treatment are crucial to prevent these consequences.
Can allergies cause my baby to snore?
Yes, allergies can certainly contribute to baby snoring. Allergic reactions can cause inflammation and swelling in the nasal passages and throat, leading to congestion and obstruction that impede smooth airflow during sleep. Managing your baby's allergies with your pediatrician's guidance can often reduce snoring caused by this issue.
When to See a Dentist or Medical Professional
It’s crucial to know when to escalate your concerns beyond general observation.
See your pediatrician promptly if you notice any of the following:
- Loud, consistent snoring every night.
- Snoring accompanied by gasps, choking, or visible pauses in breathing.
- Your baby struggles to breathe during sleep (e.g., chest retractions, flaring nostrils).
- Bluish discoloration of the lips or skin (this is a medical emergency; seek immediate care).
- Excessive daytime sleepiness, lethargy, or, conversely, hyperactivity and irritability.
- Difficulty feeding or poor weight gain.
- Unusual sleep positions (e.g., hyper-extending the neck).
- Any concerns about your baby's breathing during sleep that worry you. Trust your parental instincts.
When to consult a dental professional (specifically a pediatric dentist or orthodontist):
While a general dentist is usually not the first point of contact for infant snoring, they may become involved if:
- Your child is older (toddler, preschooler, or school-aged) and presents with chronic mouth breathing, malocclusion (bad bite), or a narrow palate, which can contribute to airway issues. A pediatric dentist can assess oral structures and possibly suggest orthodontic interventions like palatal expanders if deemed appropriate by an ENT or sleep specialist.
- A sleep specialist recommends an oral appliance for an older child/adolescent. In this case, a dentist specializing in sleep medicine would custom-fit the device. Again, this is not applicable for infants.
The American Dental Association (ADA) emphasizes a collaborative approach between dentists and medical professionals for comprehensive care, especially concerning sleep-disordered breathing. Your pediatric dentist can be a valuable part of a multidisciplinary team to assess craniofacial development and its impact on the airway in older children.
Don't hesitate to seek professional medical advice. Early intervention is paramount for ensuring your baby's healthy growth, development, and overall well-being.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Difference Between Snoring and Sleep Apnea: Complete Guide
More than 80 million Americans regularly snore, and while often dismissed as a mere nuisance, loud and persistent snoring can be a critical indicator of a much more serious underlying health condition: sleep apnea. The difference between snoring and sleep apnea is profound, impacting not just yo
February 23, 2026
Mouth Taping for Snoring: Complete Guide
Snoring. It's the nocturnal soundtrack for millions of Americans, often a source of frustration for bed partners and a potential indicator of underlying health issues for the snorer themselves. Roughly 45% of adults snore occasionally, and 25% are habitual snorers, impacting sleep quality, relat
February 23, 2026

Is All Snoring Sleep Apnea
Many individuals, perhaps even you or a loved one, have been told they snore loudly. It's often dismissed as a harmless, albeit annoying, nocturnal habit. However, what if that nightly rumble is more than just noise? What if it's a critical indicator of an underlying health condition that significan
February 23, 2026
Cpap Dry Mouth Even With Humidifier: Complete Guide
Experiencing dry mouth while using a CPAP machine, even with a humidifier, is a common and incredibly frustrating issue for millions of Americans. It can disrupt sleep, diminish the effectiveness of your sleep apnea treatment, and significantly impact your oral health. Imagine waking up every mornin
February 23, 2026