Mouth Tape for Sleep Apnea: Complete Guide
Key Takeaways
- Mouth Tape for Sleep Apnea: Complete Guide
Mouth Tape for Sleep Apnea: Complete Guide
Do you wake up with a dry mouth, sore throat, or experience persistent fatigue despite a full night's sleep? You're not alone. An estimated 22 million Americans suffer from sleep apnea, a condition where breathing repeatedly stops and starts during sleep. While some individuals explore mouth tape for sleep apnea as a potential solution, it's crucial to understand its actual role, limitations, and the comprehensive array of treatments available for this serious health concern. This article will delve into what mouth taping is, explore its potential benefits and significant risks, and provide a definitive guide to effectively diagnosing and treating sleep apnea, ensuring you understand the best paths to a restful night and improved overall health. We'll cover everything from traditional treatments like CPAP therapy and oral appliances to lifestyle adjustments and when to seek professional dental and medical guidance.
Key Takeaways:
- Mouth taping is NOT a treatment for diagnosed Obstructive Sleep Apnea (OSA). It can be dangerous for individuals with moderate to severe OSA.
- Its primary (potential) benefit is for chronic mouth breathing or mild snoring without underlying sleep apnea, by promoting nasal breathing.
- The average cost of a sleep study (polysomnography) ranges from $800 to $5,000 without insurance, often covered by most plans.
- CPAP therapy, the gold standard for OSA, can cost $500 to $3,000 for the machine, with masks and supplies adding $200-$500 annually.
- Oral appliance therapy, a common alternative, ranges from $1,800 to $4,500 and is often covered by medical insurance.
- Always consult a dentist or sleep specialist before attempting mouth taping, especially if you suspect sleep apnea or chronic snoring.
- Untreated sleep apnea significantly increases risks of heart disease, stroke, diabetes, and accidents, emphasizing the need for professional diagnosis and treatment.
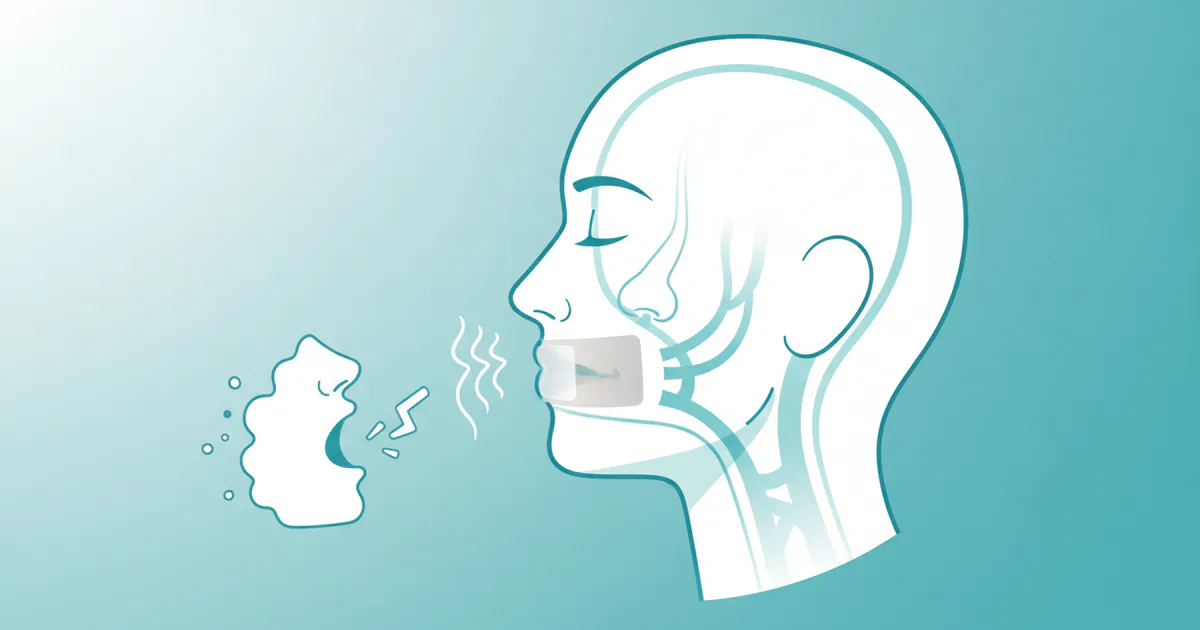
What Is Mouth Taping? An Overview
Mouth taping involves placing a small piece of specially designed adhesive tape over your lips before sleep to encourage nasal breathing throughout the night. The underlying theory is that by gently sealing the lips, you naturally train your body to breathe through your nose, which is the physiologically correct way to breathe. Chronic mouth breathing, especially during sleep, can lead to a host of problems including dry mouth, poor oral hygiene, bad breath, dental issues, and can exacerbate snoring and sleep-disordered breathing. Proponents suggest that promoting nasal breathing can improve sleep quality, reduce snoring, and support overall health.
However, it's vital to clarify that while mouth taping might help address mouth breathing and mild, uncomplicated snoring, it is not a scientifically proven treatment for obstructive sleep apnea (OSA). Sleep apnea is a complex medical condition characterized by repeated pauses in breathing due to a collapsed airway, and simply taping the mouth shut does not resolve the underlying structural or neurological issues. For individuals with diagnosed sleep apnea, relying on mouth tape instead of evidence-based treatments can be dangerous, potentially worsening oxygen deprivation during sleep.
Types of Mouth Tape and How It's Used
The market offers several variations of mouth tape, each designed with different adhesive strengths, materials, and shapes to maximize comfort and effectiveness while minimizing skin irritation.
Types of Mouth Tapes
- Standard Hypoallergenic Tapes: These are often made from medical-grade, breathable materials like surgical tape or gentle paper tape. They are usually simple strips placed horizontally across the lips.
- Perforated or "X" Shaped Tapes: Some designs feature small perforations or an "X" shape to allow for minimal airflow through the mouth if absolutely necessary, offering a slightly less restrictive approach.
- Pre-formed Lip Patches: These are ergonomically designed to fit the contours of the lips, often made with softer, more flexible materials to ensure comfort and reduce skin pull.
- Anti-Snoring Chin Straps: While not technically "mouth tape," these devices work on a similar principle by gently holding the jaw closed to prevent mouth breathing and keep the airway open. They are often used in conjunction with other therapies or as a standalone for simple snoring.
How to Use Mouth Tape (with extreme caution)
For individuals considering mouth taping for mouth breathing without diagnosed sleep apnea, the process typically involves:
- Preparation: Ensure your lips and the surrounding skin are clean, dry, and free of any lotions or oils.
- Application: Take a small strip of mouth tape (typically 1-2 inches long for standard tapes). Gently press it horizontally across the center of your lips, ensuring your lips are lightly closed but not strained. Some people prefer to fold a small edge of the tape over itself on one side to create a tab for easier removal.
- Removal: In the morning, gently peel the tape off. If it's too sticky, a warm, damp cloth can help loosen the adhesive.
Pro Tip: Always do a patch test on a small area of skin (like your forearm) for a few hours before applying mouth tape to your lips for the entire night, to check for any allergic reactions or skin irritation.
Understanding the Causes: Mouth Breathing, Snoring, and Sleep Apnea
To properly evaluate the role of mouth taping, it's essential to understand the distinctions and connections between mouth breathing, snoring, and sleep apnea.
Why Mouth Breathing Happens
Chronic mouth breathing, especially during sleep, can stem from several factors:
- Nasal Obstruction: This is the most common cause. Blockages can include allergies, chronic sinusitis, deviated septum, nasal polyps, enlarged turbinates, or even common colds. When nasal passages are obstructed, the body instinctively switches to mouth breathing to get enough air.
- Anatomical Factors: A narrow upper jaw, receding chin, or an underdeveloped midface can contribute to a smaller airway, making nasal breathing more challenging.
- Poor Oral Posture: A low resting tongue position, where the tongue doesn't rest against the roof of the mouth, can encourage mouth breathing and contribute to a collapsed airway during sleep.
- Habit: Sometimes, mouth breathing becomes a habit formed in childhood due to prolonged allergies or adenoid/tonsil issues, even after the initial cause is resolved.
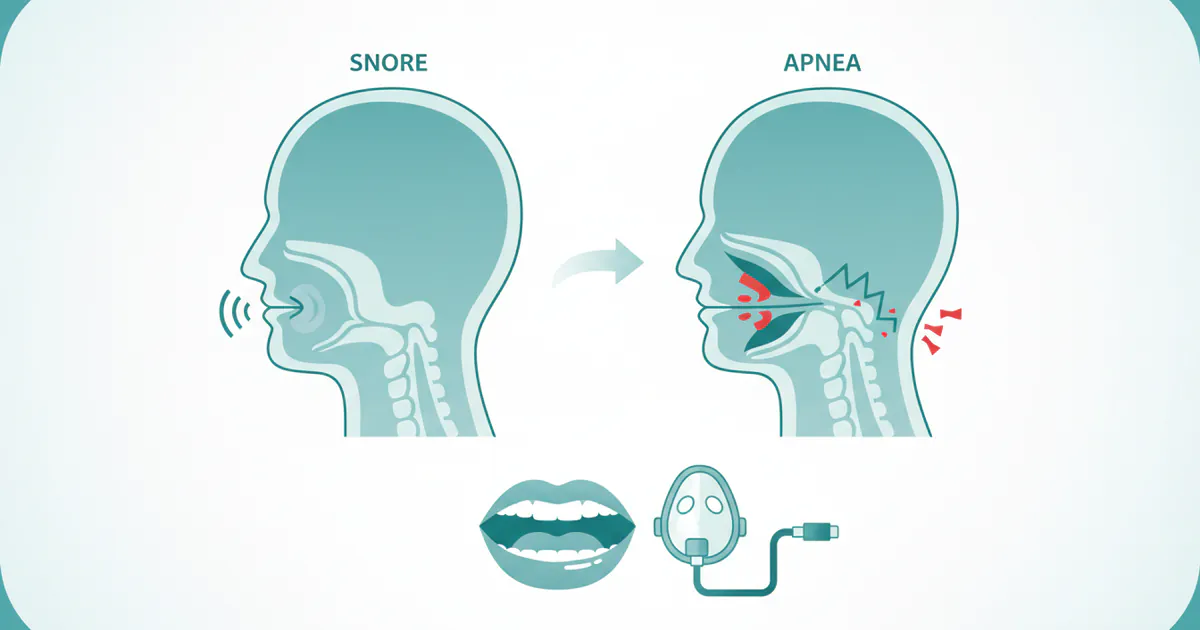
Is Snoring Sleep Apnea?
Snoring is the vibrating sound produced by obstructed air movement during sleep. It occurs when air flows past relaxed tissues in the throat, causing them to vibrate as you breathe. While often considered benign, snoring is a key symptom of sleep-disordered breathing, and it can be a significant indicator of obstructive sleep apnea (OSA). However, not all snoring indicates sleep apnea.
- Primary Snoring (Simple Snoring): This is snoring that isn't associated with sleep apnea or other medical conditions. It's often linked to lifestyle factors like alcohol consumption, certain medications, or sleeping on your back.
- Snoring with Obstructive Sleep Apnea (OSA): If your snoring is very loud, often interrupted by gasps, snorts, or silences (where breathing stops), and is accompanied by daytime fatigue, then it's highly likely to be a symptom of OSA.
Obstructive Sleep Apnea (OSA): The Core Issue
OSA is a serious medical condition where the airway repeatedly collapses or becomes blocked during sleep, causing breathing to stop for 10 seconds or more (an "apnea") or to become very shallow (a "hypopnea"). These events can happen dozens or even hundreds of times per night. Each event causes a drop in blood oxygen levels and briefly wakes the brain (though you might not remember it), disrupting the restorative sleep cycle.
Causes of OSA: The primary cause of OSA is the relaxation of muscles in the back of the throat during sleep, which allows the soft tissue (like the soft palate, uvula, and tongue) to collapse and block the airway. Contributing factors include:
- Obesity: Excess weight around the neck can narrow the airway.
- Enlarged Tonsils or Adenoids: More common in children, but can affect adults too.
- Anatomical Features: A naturally narrow throat, a thick neck circumference, a recessed jaw, or a large tongue can predispose individuals to OSA.
- Age: The risk of OSA increases with age.
- Gender: Men are more likely to have OSA than women, though the risk for women increases after menopause.
- Alcohol and Sedatives: These relax throat muscles, worsening airway collapse.
- Smoking: Can increase inflammation and fluid retention in the upper airway.
- Family History: A genetic predisposition can exist.
Signs and Symptoms: When to Be Concerned
Recognizing the signs and symptoms of sleep-disordered breathing is the first step toward diagnosis and treatment.
Symptoms of Chronic Mouth Breathing
- Dry mouth and sore throat upon waking
- Cracked lips
- Bad breath (halitosis)
- Increased cavities (due to lack of saliva production)
- Gum inflammation (gingivitis)
- Hoarseness
- Daytime fatigue and difficulty concentrating (can overlap with sleep apnea)
- Snoring
Signs and Symptoms of Obstructive Sleep Apnea
The symptoms of OSA often go unnoticed by the individual, frequently reported by a bed partner.
- Loud, chronic snoring: Often punctuated by pauses in breathing, gasps, or choking sounds (witnessed apneas).
- Daytime sleepiness or fatigue: Even after what seems like a full night's sleep.
- Morning headaches: Due to fluctuating oxygen and carbon dioxide levels.
- Dry mouth or sore throat upon waking: Common if mouth breathing occurs due to obstructed nasal passages or while struggling for air during apneas.
- Irritability or mood changes: Resulting from chronic sleep deprivation.
- Difficulty concentrating or memory problems.
- Frequent night awakenings to urinate (nocturia).
- High blood pressure (hypertension): OSA is a significant risk factor.
- Reduced libido.
If you or your bed partner notice several of these symptoms, especially witnessed pauses in breathing, it's crucial to seek professional medical evaluation.
Comprehensive Treatment Options for Sleep Apnea and Mouth Breathing
Addressing sleep apnea requires a multi-faceted approach, often involving a team of healthcare professionals including sleep physicians, dentists specializing in sleep medicine, and sometimes ENTs. Mouth taping is NOT a primary or standalone treatment for diagnosed sleep apnea and should not be used as such. It may have a very limited role for mild snoring or habitual mouth breathing, but only under professional guidance and after ruling out underlying OSA.
1. Continuous Positive Airway Pressure (CPAP) Therapy
What it is: CPAP is the gold standard and most effective treatment for moderate to severe OSA. A CPAP machine delivers a continuous stream of filtered, pressurized air through a mask worn over the nose or nose and mouth, keeping the airway open during sleep.
Pros:
- Highly effective in eliminating apneas and hypopneas.
- Significantly improves sleep quality and reduces daytime fatigue.
- Reduces the risk of long-term health complications associated with OSA (heart disease, stroke).
- Variety of masks available for comfort.
Cons:
- Can be uncomfortable or claustrophobic for some users.
- Requires consistent use every night to be effective.
- Mask leaks, dry mouth, and skin irritation are common side effects.
- Noise from the machine (though modern machines are very quiet).
- Maintenance and cleaning of equipment required.
Best CPAP Mask for Mouth Breathers: For individuals who breathe through their mouth, even with CPAP, a full-face mask that covers both the nose and mouth is often recommended. This ensures that air pressure is delivered effectively regardless of whether the mouth is open or closed. Some mouth breathers can also succeed with a nasal mask or nasal pillows combined with a chin strap to keep the mouth closed. Your sleep specialist can help you determine the best fit and style.
2. Oral Appliance Therapy (OAT)
What it is: Custom-made dental devices, similar to a mouthguard, worn only during sleep. The most common type is a Mandibular Advancement Device (MAD), which gently repositions the lower jaw and tongue forward to keep the airway open.
Pros:
- Less invasive and often more comfortable than CPAP for many users.
- Highly portable and discreet.
- Effective for mild to moderate OSA, and for those who cannot tolerate CPAP.
- Prescribed and fitted by a qualified sleep dentist, like those recommended by the American Dental Association (ADA) for OAT.
Cons:
- May not be as effective as CPAP for severe OSA.
- Potential side effects include jaw discomfort, tooth movement, or changes in bite, though these are often minor and reversible.
- Requires regular follow-up with the sleep dentist.
3. Myofunctional Therapy
What it is: A series of exercises for the tongue and facial muscles that aim to improve muscle tone, resting tongue posture, and overall oral-facial function. It focuses on strengthening the muscles that keep the airway open.
Pros:
- Non-invasive and drug-free.
- Can be an effective adjunct to other treatments for OSA or even a standalone therapy for mild cases and chronic mouth breathing.
- Can improve nasal breathing, swallowing, and speech.
Cons:
- Requires consistent effort and commitment to exercises over several months.
- Results can vary among individuals.
4. Lifestyle Modifications
What it is: Changes to daily habits that can significantly reduce OSA severity or alleviate symptoms.
Pros:
- Cost-effective and generally beneficial for overall health.
- Can improve the effectiveness of other treatments.
Cons:
- Requires significant personal discipline and commitment.
Specific modifications:
- Weight Loss: Even a modest amount of weight loss can reduce the severity of OSA.
- Positional Therapy: Sleeping on your side rather than your back can prevent the tongue and soft palate from collapsing into the airway. Special pillows or devices can help maintain side-sleeping.
- Avoid Alcohol and Sedatives: Especially before bed, as they relax throat muscles.
- Quit Smoking: Smoking irritates and inflames the airway.
- Nasal Decongestants/Saline Sprays: Can help clear nasal passages for better nasal breathing, but aren't a direct OSA treatment.
5. Surgical Interventions
What it is: Various surgical procedures are available for OSA, typically considered when other non-invasive treatments have failed or are not tolerated, and specific anatomical obstructions are identified.
Pros:
- Can offer a permanent solution for some individuals.
- Eliminates the need for daily devices.
Cons:
- Invasive, with associated risks (pain, infection, bleeding, altered sensation).
- Success rates vary depending on the procedure and individual anatomy.
- Recovery time can be significant.
Types of surgeries:
- Uvulopalatopharyngoplasty (UPPP): Removes excess tissue from the back of the throat (uvula, soft palate, tonsils).
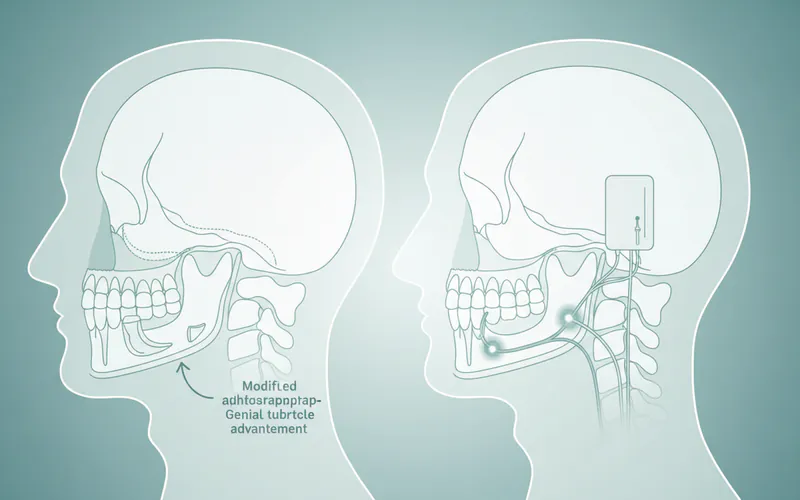
- Maxillomandibular Advancement (MMA): A more extensive surgery that moves the upper and lower jaws forward, significantly expanding the airway.
- Genioglossus Advancement (GA): Tightens the tendon that attaches the tongue to the lower jaw, preventing the tongue from falling back.
- Hypoglossal Nerve Stimulation: Implants a device that stimulates the nerve controlling tongue movement, keeping the airway open.
- Nasal Surgery: Procedures to correct a deviated septum or remove polyps can improve nasal breathing but don't typically cure OSA on their own.
6. Mouth Taping (A Note of Extreme Caution)
What it is: As discussed, placing tape over the mouth to encourage nasal breathing.
Pros (limited and conditional):
- Extremely low cost.
- May help some individuals with chronic mouth breathing (without OSA) or very mild, simple snoring to establish nasal breathing habits.
Cons (significant):
- DANGEROUS if you have undiagnosed or diagnosed sleep apnea. It prevents emergency mouth breathing, potentially leading to dangerous drops in blood oxygen.
- Does not address the underlying causes of airway collapse in OSA.
- Can cause skin irritation or allergic reactions.
- Can cause anxiety or panic if unable to breathe through the nose.
- No scientific evidence supports its effectiveness for treating OSA.
Pro Tip: Never attempt mouth taping if you have a history of nasal obstruction, severe allergies, asthma, or any respiratory condition without explicit medical approval. It's especially dangerous for children.
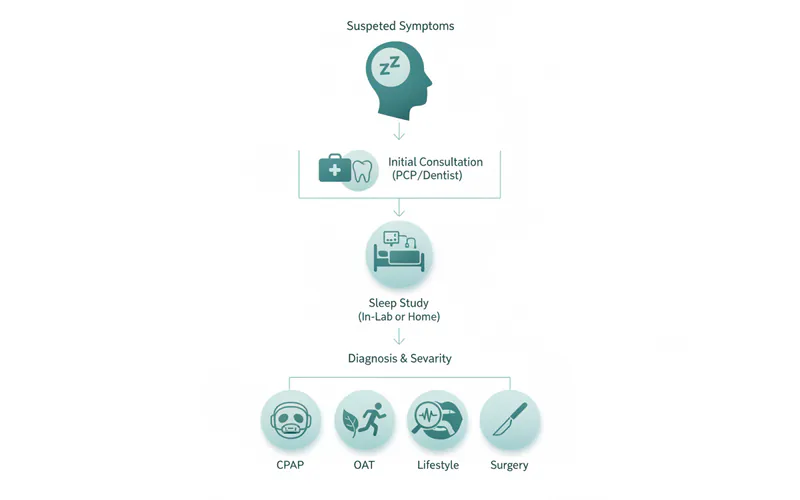
Step-by-Step Process for Diagnosing and Treating Sleep Apnea
The journey from suspected sleep apnea to effective treatment typically follows a structured path.
1. Initial Consultation
- Your Primary Care Physician (PCP) or Dentist: Start by discussing your symptoms (snoring, fatigue, dry mouth) with your doctor or a dentist specializing in sleep medicine. They will review your medical history, perform a physical exam, and assess your risk factors for OSA.
- Sleep Questionnaire: You'll likely complete questionnaires (e.g., Epworth Sleepiness Scale) to evaluate your level of daytime sleepiness.
2. Sleep Study (Polysomnography)
- Referral: If OSA is suspected, your doctor will refer you for a sleep study. This is the definitive diagnostic tool.
- Types of Sleep Studies:
- In-Lab Polysomnography (PSG): The gold standard. You spend a night at a sleep center where various physiological parameters are monitored (brain waves, heart rate, breathing effort, airflow, blood oxygen levels, leg movements).
- Home Sleep Apnea Test (HSAT): A simpler, less expensive test done in your own bed. It monitors fewer parameters but is effective for diagnosing moderate to severe OSA.
3. Diagnosis and Severity Assessment
- A sleep physician interprets the results of your sleep study.
- The Apnea-Hypopnea Index (AHI) is calculated: the average number of apneas and hypopneas per hour of sleep.
- Normal: AHI < 5
- Mild OSA: AHI 5-15
- Moderate OSA: AHI 15-30
- Severe OSA: AHI > 30
4. Treatment Planning
- Based on your diagnosis, severity, and personal preferences, your sleep physician will recommend the most appropriate treatment plan.
- This might involve CPAP, an oral appliance, lifestyle changes, or a combination.
- If an oral appliance is chosen, you'll be referred to a qualified sleep dentist for custom fitting and follow-up.
5. Follow-up and Adjustment
- Treatment for sleep apnea is often ongoing. Regular follow-ups with your sleep physician and/or sleep dentist are essential to monitor effectiveness, address any issues, and make adjustments to your therapy.
- For CPAP users, data from the machine can be reviewed remotely or in person.
- For oral appliance users, adjustments may be made to optimize jaw position.
Cost and Insurance: Understanding the Financial Aspect
The cost of diagnosing and treating sleep apnea in the US can vary significantly based on your insurance coverage, location, and the specific treatments chosen. Mouth tape, on the other hand, is a minimal expense.
Diagnostic Costs
- Initial Consultation (PCP/Sleep Specialist):
- With Insurance: Typically covered after co-pay ($20-$100) or deductible.
- Without Insurance: $100-$300.
- Sleep Study (Polysomnography - PSG):
- With Insurance: Often covered, but you may pay a co-insurance (e.g., 10-30% after deductible). Out-of-pocket costs can range from $500-$1,500.
- Without Insurance: $800-$5,000, with major metropolitan areas typically on the higher end.
- Home Sleep Apnea Test (HSAT):
- With Insurance: Generally covered with lower co-pay/co-insurance than in-lab PSG. Out-of-pocket $100-$500.
- Without Insurance: $200-$1,000.
Treatment Costs
- Mouth Tape:
- Cost: $5-$30 for a pack of 30-100 strips.
- Insurance: Not covered.
- CPAP Machine:
- Cost (Machine only): $500-$3,000 for a new device, depending on features (auto-CPAP, humidification). Refurbished models are cheaper.
- Masks and Supplies: $200-$500 annually for replacement masks, tubing, filters, and humidifier chambers.
- Insurance: Most medical insurance plans cover CPAP therapy, usually with durable medical equipment (DME) coverage. You may have a co-pay, co-insurance, or be subject to your deductible. Often, insurance companies will rent the machine to you for a period before you own it.
- Oral Appliance Therapy (OAT):
- Cost: $1,800-$4,500 for a custom-fitted device, including consultations, impressions, fabrication, and follow-up adjustments.
- Insurance: Often covered by medical insurance (not dental insurance) if medically necessary for OSA, typically under DME. Coverage varies, and you'll likely have co-insurance and a deductible.
- Myofunctional Therapy:
- Cost: $100-$250 per session, with a full course often requiring 10-20 sessions, totaling $1,000-$5,000.
- Insurance: Coverage is rare for these services, often considered elective.
- Surgical Interventions:
- Cost: Highly variable, from $2,000-$15,000+ depending on the complexity of the procedure (e.g., UPPP is less expensive than MMA).
- Insurance: Generally covered by medical insurance if deemed medically necessary for OSA, subject to deductibles, co-pays, and co-insurance. Pre-authorization is almost always required.
Payment Plans and Financing Options
Many sleep centers, dental practices, and DME providers offer:
- In-house payment plans: Spreading payments over several months.
- Healthcare credit cards: Such as CareCredit, which offers promotional financing options.
- Flexible Spending Accounts (FSAs) and Health Savings Accounts (HSAs): These tax-advantaged accounts can be used to pay for qualified medical expenses, including sleep studies, CPAP equipment, and oral appliances.
Pro Tip: Always verify your specific insurance coverage for sleep studies and treatments before proceeding. Ask for CPT codes and pre-authorization numbers to avoid unexpected costs.
Recovery and Aftercare for Sleep Apnea Treatments
Effective management of sleep apnea is an ongoing process that extends beyond initial diagnosis and treatment.
CPAP Therapy Aftercare
- Adherence is Key: Consistent nightly use is crucial for the benefits of CPAP. Your sleep specialist will monitor your usage data.
- Maintenance: Regularly clean your mask, tubing, and humidifier water chamber to prevent bacteria and mold growth. Replace filters, masks, and tubing as recommended by the manufacturer (typically every 3-6 months for masks, 6-12 months for tubing).
- Troubleshooting: Address common issues like mask leaks, dry mouth (humidifier settings), or skin irritation (different mask types, liners) with your DME provider or sleep specialist.
- Follow-ups: Schedule periodic follow-up appointments to discuss progress, address concerns, and ensure the pressure settings are optimal.
Oral Appliance Therapy Aftercare
- Cleaning: Clean your oral appliance daily with a toothbrush and mild soap or a denture cleaner. Store it in a protective case when not in use.
- Regular Adjustments: Initial follow-up appointments (typically weekly for the first month, then quarterly) are necessary to fine-tune the appliance for maximum effectiveness and comfort.
- Monitoring Side Effects: Your sleep dentist will monitor for potential side effects like jaw discomfort, changes in bite, or tooth sensitivity. These are usually mild and manageable.
- Dental Check-ups: Continue routine dental check-ups, as the appliance fits over your teeth.
- Appliance Lifespan: Oral appliances typically last 3-5 years but may need replacement sooner if wear and tear occur or if significant dental changes happen.
Surgical Recovery
- Recovery varies significantly depending on the type and invasiveness of the surgery.
- UPPP: Expect a sore throat for several weeks, with pain managed by medication. Diet will likely be soft for a period.
- More Extensive Surgeries (e.g., MMA): Involve longer hospital stays, significant pain management, and extended recovery periods (months).
- Follow-up Sleep Study: A post-surgical sleep study is often recommended 3-6 months after healing to assess the effectiveness of the procedure.
Prevention: Reducing Your Risk of Sleep Apnea and Mouth Breathing
While not all causes of sleep apnea are preventable (e.g., genetics, age), several strategies can significantly reduce your risk and improve overall sleep health.
- Maintain a Healthy Weight: Losing even a small amount of weight can reduce fatty tissue in the throat and improve airflow.
- Adopt Healthy Sleep Habits:
- Stick to a consistent sleep schedule, even on weekends.
- Ensure your bedroom is dark, quiet, and cool.
- Avoid large meals, caffeine, and alcohol close to bedtime.
- Quit Smoking: Smoking causes inflammation and fluid retention in the upper airway, exacerbating snoring and OSA.
- Limit Alcohol and Sedatives: Especially in the evening, as they relax the muscles in your throat.
- Sleep on Your Side: Positional therapy can prevent the tongue and soft palate from collapsing.
- Address Nasal Congestion: Treat allergies, colds, or chronic sinus issues to promote nasal breathing. Saline rinses, decongestants (short-term), or corticosteroid nasal sprays (long-term for allergies) can help.
- Consider Myofunctional Therapy: Especially if you have a history of mouth breathing or tongue thrust, these exercises can strengthen oral-facial muscles and improve resting tongue posture.
- Early Intervention for Children: Address mouth breathing and enlarged tonsils/adenoids in children promptly to prevent developmental issues and reduce OSA risk.
Risks and Complications: What Can Go Wrong
Understanding the risks of both untreated sleep apnea and inappropriate treatments like mouth taping is crucial.
Risks of Untreated Obstructive Sleep Apnea
The long-term consequences of untreated OSA are severe and impact multiple body systems:
- Cardiovascular Problems: Increased risk of high blood pressure, heart attack, stroke, irregular heartbeats (arrhythmias), and heart failure. The repeated drops in blood oxygen and surge in blood pressure during apneas put significant strain on the cardiovascular system.
- Type 2 Diabetes: OSA can lead to insulin resistance, increasing the risk of developing or worsening diabetes.
- Metabolic Syndrome: A cluster of conditions including high blood pressure, high blood sugar, excess body fat around the waist, and abnormal cholesterol levels, which collectively increase the risk of heart disease, stroke, and diabetes.
- Daytime Fatigue and Accidents: Chronic sleep deprivation severely impairs concentration, reaction time, and decision-making, significantly increasing the risk of motor vehicle accidents and workplace errors.
- Mental Health Issues: Increased risk of depression, anxiety, and irritability due to chronic sleep disruption.
- Complications with Medications and Surgery: People with OSA may have more complications with general anesthesia and certain medications.
- Sexual Dysfunction: Reduced libido and erectile dysfunction are common.
Risks and Dangers of Mouth Taping (Especially for Sleep Apnea)
While mouth taping is often marketed as a simple "hack," its risks can be significant, particularly if used inappropriately.
- Dangerous for Undiagnosed/Treated OSA: If you have moderate to severe sleep apnea, mouth taping can prevent you from opening your mouth to gasp for air when your airway collapses. This can lead to dangerously low blood oxygen levels, severe carbon dioxide retention, and potentially life-threatening complications.
- Panic and Anxiety: Waking up unable to breathe through your nose with your mouth taped shut can cause intense panic attacks and a feeling of suffocation.
- Skin Irritation/Allergic Reactions: Adhesives can cause redness, itching, rashes, or allergic reactions on sensitive skin around the lips.
- No Resolution of Underlying Cause: Mouth taping does not address the anatomical or physiological issues that cause sleep apnea. It's a superficial "fix" that masks a potentially severe problem.
- Exacerbation of Nasal Issues: If you have chronic nasal congestion or blockages, mouth taping can make it impossible to breathe, leading to extreme discomfort and potentially compromising your breathing during sleep.
Children / Pediatric Considerations
Sleep-disordered breathing and mouth breathing are significant concerns in children, impacting their development, behavior, and overall health.
- Causes in Children: Enlarged tonsils and adenoids are the most common cause of OSA in children. Other factors include allergies, obesity, and craniofacial abnormalities.
- Signs in Children: Unlike adults, children with OSA may not always be sleepy during the day. Instead, they might exhibit hyperactivity, behavioral problems (misdiagnosis of ADHD is common), difficulty concentrating, slow growth, bedwetting, and aggressive snoring. Chronic mouth breathing can also lead to characteristic "adenoid facies" (long, narrow face; drooping eyes; open-mouth posture).
- Diagnosis: Similar to adults, a sleep study is the diagnostic gold standard.
- Treatment:
- Adenotonsillectomy: Removal of tonsils and adenoids is often the first-line treatment for children with OSA due to enlarged lymphatic tissue.
- Orthodontic Expansion: Palatal expanders can widen a narrow upper jaw, improving nasal breathing and airway space.
- Myofunctional Therapy: Can be very effective in teaching proper tongue posture and nasal breathing.
- CPAP: Used in children with severe OSA, especially if surgery is not effective or appropriate.
- Mouth Taping in Children: Mouth taping is strongly discouraged for children. Their airways are smaller and more vulnerable. Restricting their breathing, especially if they have underlying nasal congestion or developing OSA, can be extremely dangerous. Always consult a pediatric ENT or sleep specialist for any concerns about a child's breathing or sleep.
Comparison of Sleep Apnea Treatments
To provide a clear perspective on the available options, here's a comparison of the most common and effective treatments for sleep apnea, including where mouth taping fits (or doesn't fit).
| Feature | CPAP Therapy | Oral Appliance Therapy (OAT) | Myofunctional Therapy | Lifestyle Modifications | Surgery (e.g., UPPP) | Mouth Taping (Caution!) |
|---|---|---|---|---|---|---|
| Effectiveness | High (moderate to severe OSA) | Moderate to High (mild to moderate OSA, snoring) | Low to Moderate (mild OSA, adjunct therapy) | Variable (mild OSA, risk reduction) | Variable (depending on procedure and patient) | Negligible for OSA, maybe for simple mouth breathing |
| Invasiveness | Non-invasive (external device) | Non-invasive (internal dental device) | Non-invasive (exercises) | Non-invasive | Highly Invasive | Non-invasive (external tape) |
| Comfort | Can be challenging initially, mask fit issues | Generally good, some jaw discomfort | Generally good | Easy to implement, requires discipline | Significant pain during recovery | Can be uncomfortable, risk of panic |
| Cost (Annual) | $500-$3,000 (machine) + $200-$500 (supplies) | $1,800-$4,500 (device, multi-year) | $1,000-$5,000 (full course, often self-pay) | Low (gym membership, healthy food) | $2,000-$15,000+ (one-time, may need revision) | $5-$30 (tape) |
| Insurance | Usually covered (medical DME) | Often covered (medical DME) | Rarely covered | Not covered directly | Usually covered (medical) | Not covered |
| Primary Use | Moderate to severe OSA | Mild to moderate OSA, snoring | Adjunct for OSA, mouth breathing, swallowing | OSA prevention, mild snoring | Specific anatomical obstructions in OSA | Mouth breathing, not OSA |
| Risks | Mask discomfort, dry mouth, compliance issues | Jaw discomfort, bite changes, tooth movement | Requires consistent effort | Requires long-term commitment | Pain, infection, bleeding, altered sensation, recurrence | DANGEROUS for OSA, skin irritation, anxiety |
| Recommended By | Sleep physicians, dentists, ENT | Sleep dentists, sleep physicians | Myofunctional therapists, some dentists/ENIs | PCP, sleep specialists | ENT surgeons, oral surgeons | Not recommended for OSA by medical professionals |
Frequently Asked Questions
H3: Can mouth tape cure sleep apnea?
No, mouth tape cannot cure sleep apnea. It does not address the underlying causes of airway collapse. While it might help individuals who primarily mouth breathe or snore mildly, it is not an effective or safe treatment for diagnosed obstructive sleep apnea and can be dangerous by preventing emergency mouth breathing.
H3: Is mouth taping safe if I have sleep apnea?
Mouth taping is generally considered unsafe for individuals with diagnosed or suspected sleep apnea. It can prevent you from gasping for air when your airway collapses, leading to dangerous drops in blood oxygen levels. Always consult a sleep specialist before considering mouth taping, especially if you have any respiratory issues or symptoms of sleep apnea.
H3: What is the best alternative to mouth tape for mouth breathers?
For chronic mouth breathing, the best alternative is to address the root cause. This often involves nasal congestion treatment (allergies, deviated septum), myofunctional therapy to improve tongue posture, or, if sleep apnea is present, standard treatments like CPAP or oral appliances that promote nasal breathing by keeping the airway open.
H3: How is sleep apnea diagnosed, and how long does it take?
Sleep apnea is definitively diagnosed with a sleep study (polysomnography), either in a sleep lab or at home. The diagnostic process typically involves an initial consultation, followed by the sleep study overnight, and then an interpretation of results which usually takes 1-2 weeks. From first appointment to diagnosis can take 2-4 weeks.
H3: How much does sleep apnea treatment cost in the US?
Costs vary widely depending on the treatment. A sleep study can range from $200-$5,000. A CPAP machine is $500-$3,000, plus $200-$500 annually for supplies. An oral appliance is $1,800-$4,500. Surgical options can range from $2,000-$15,000+. Most medical insurance plans cover diagnostics and primary treatments like CPAP and oral appliances, subject to deductibles and co-pays.
H3: Will my insurance cover an oral appliance for sleep apnea?
Many medical insurance plans (not dental plans) will cover oral appliance therapy for mild to moderate obstructive sleep apnea when prescribed by a sleep physician and fabricated by a qualified sleep dentist. Coverage is typically under durable medical equipment (DME) benefits, requiring pre-authorization and often subject to deductibles and co-insurance.
H3: What is the recovery period for sleep apnea treatments?
For CPAP and oral appliances, there isn't a "recovery" period in the traditional sense, but rather an adjustment period to using the device nightly, which can take a few weeks to a few months. Surgical recovery can range from several weeks (for UPPP) to several months (for more extensive jaw surgeries), involving pain management and diet restrictions.
H3: Besides mouth tape, are there other ways to stop snoring?
Yes, many effective ways to reduce or stop snoring exist. These include lifestyle changes like weight loss, avoiding alcohol before bed, and sleeping on your side. Nasal strips or dilators can improve nasal airflow, and oral appliances are highly effective for snoring, especially if it's related to mild to moderate sleep apnea. Addressing allergies and nasal congestion can also help significantly.
H3: Can a dentist help with sleep apnea?
Absolutely. Dentists specializing in sleep medicine play a crucial role in managing sleep apnea, particularly with oral appliance therapy. They custom-fit devices to keep the airway open during sleep. Many general dentists are also trained to screen for sleep apnea symptoms and can refer you to a sleep specialist for diagnosis. The American Dental Association (ADA) recognizes the role of qualified dentists in the management of sleep-related breathing disorders.
H3: What happens if sleep apnea is left untreated?
Untreated sleep apnea carries severe health risks, including a significantly increased likelihood of high blood pressure, heart attack, stroke, type 2 diabetes, and metabolic syndrome. It also causes chronic daytime fatigue, increasing the risk of accidents, and can lead to mood disorders like depression and anxiety.
When to See a Dentist
Given the nuanced relationship between mouth breathing, snoring, and sleep apnea, knowing when to seek professional dental or medical advice is paramount.
- You frequently wake with a dry mouth or sore throat: This is a strong indicator of chronic mouth breathing, which a dentist can assess for underlying causes.
- Your bed partner reports loud, chronic snoring, especially if it's interrupted by gasps, snorts, or pauses in breathing: These are classic signs of obstructive sleep apnea, warranting immediate evaluation by a sleep specialist or a dentist specializing in sleep medicine.
- You experience persistent daytime fatigue, even after adequate sleep: This is a hallmark symptom of sleep apnea that requires professional diagnosis.
- You have high blood pressure, diabetes, or other cardiovascular issues, and also snore or feel tired: Your dentist or physician should screen you for sleep apnea, as it's a significant risk factor for these conditions.
- You're considering mouth taping: Always consult your dentist or a sleep physician first. They can help determine if mouth taping is safe for your specific situation (i.e., ruling out sleep apnea) and discuss more effective, evidence-based treatments for mouth breathing or snoring.
- Your child exhibits snoring, mouth breathing, or behavioral issues: A pediatric dentist or ENT should evaluate your child promptly to rule out enlarged tonsils/adenoids or other airway issues that could impact their development and health.
Don't ignore the signs of sleep-disordered breathing. Taking proactive steps to get a professional diagnosis and appropriate treatment can profoundly improve your health, energy levels, and overall quality of life.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles
Difference Between Snoring and Sleep Apnea: Complete Guide
More than 80 million Americans regularly snore, and while often dismissed as a mere nuisance, loud and persistent snoring can be a critical indicator of a much more serious underlying health condition: sleep apnea. The difference between snoring and sleep apnea is profound, impacting not just yo
February 23, 2026
Mouth Taping for Snoring: Complete Guide
Snoring. It's the nocturnal soundtrack for millions of Americans, often a source of frustration for bed partners and a potential indicator of underlying health issues for the snorer themselves. Roughly 45% of adults snore occasionally, and 25% are habitual snorers, impacting sleep quality, relat
February 23, 2026

Is All Snoring Sleep Apnea
Many individuals, perhaps even you or a loved one, have been told they snore loudly. It's often dismissed as a harmless, albeit annoying, nocturnal habit. However, what if that nightly rumble is more than just noise? What if it's a critical indicator of an underlying health condition that significan
February 23, 2026
Cpap Dry Mouth Even With Humidifier: Complete Guide
Experiencing dry mouth while using a CPAP machine, even with a humidifier, is a common and incredibly frustrating issue for millions of Americans. It can disrupt sleep, diminish the effectiveness of your sleep apnea treatment, and significantly impact your oral health. Imagine waking up every mornin
February 23, 2026