How to Handle Knocked Out Tooth
Key Takeaways
- A sudden impact, a sporting accident, or an unexpected fall – in a fraction of a second, your world can shift when you realize you've lost a tooth. A knocked out tooth, medically known as an avulsed tooth, is one of the most severe dental emergencies, and knowing **how to handle a knocked out to
A sudden impact, a sporting accident, or an unexpected fall – in a fraction of a second, your world can shift when you realize you've lost a tooth. A knocked out tooth, medically known as an avulsed tooth, is one of the most severe dental emergencies, and knowing how to handle a knocked out tooth immediately can be the difference between saving and losing it permanently. Approximately 5 million teeth are knocked out each year in children and adults, according to the American Association of Endodontists (AAE), highlighting the commonality and urgency of this situation. When a tooth is completely dislodged from its socket, the clock starts ticking for successful reimplantation. The immediate actions you take within minutes can critically influence the outcome, often determining if the tooth can be successfully reinserted and functional for years to come.
This comprehensive guide from SmilePedia.net will equip you with the essential knowledge and step-by-step instructions to manage a knocked-out tooth. We'll delve into what constitutes a dental avulsion, explore its common causes, and provide detailed guidance on the critical first aid measures. Furthermore, we’ll cover professional treatment options, discuss recovery and aftercare, outline potential risks, and provide practical advice on prevention. You'll also find insights into cost considerations, insurance navigation, and specific advice for pediatric cases, ensuring you're prepared for this time-sensitive emergency.
Key Takeaways:
- Time is Critical: For a permanent tooth, successful reimplantation significantly decreases after 60 minutes out of the mouth; ideal time is within 5-10 minutes.
- Handle With Care: Hold the tooth only by the crown (the chewing part), never touch the root.
- Keep it Moist: If possible, gently rinse the tooth (no scrubbing!) and reinsert it into the socket. If not, store it in milk, an emergency tooth preservation kit, or saliva (in the mouth next to the cheek). Avoid tap water for storage.
- Seek Immediate Dental Care: An emergency dental visit is crucial within the hour. Call your dentist or an emergency dental clinic immediately.
- Cost Variation: Reimplantation and follow-up root canal treatment can range from $1,500 to $4,000. Alternative solutions like dental implants range from $3,000 to $6,000 per tooth.
- Pediatric Note: Primary (baby) teeth are typically not reimplanted to avoid damage to developing permanent teeth.
- Prevention: Wearing a custom-fitted mouthguard during sports can prevent up to 90% of dental injuries, including knocked-out teeth.
What It Is: Understanding a Knocked Out Tooth (Dental Avulsion)
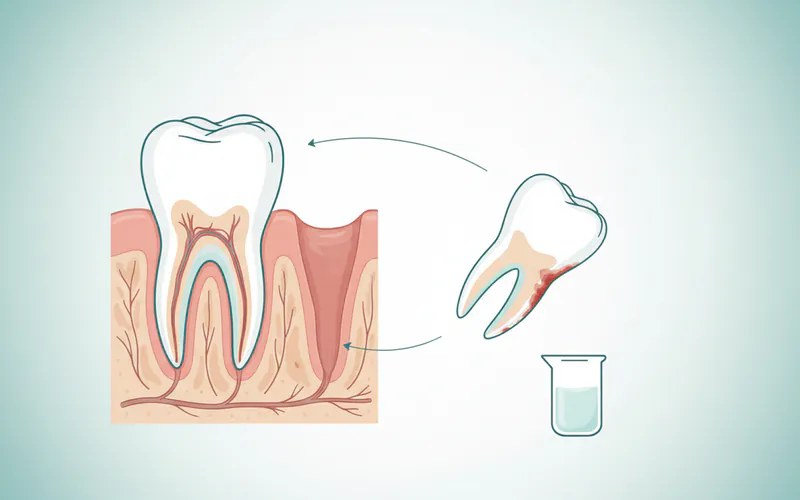
A knocked-out tooth, or dental avulsion, refers to the complete displacement of a tooth from its socket in the alveolar bone. This is a severe form of dental trauma where the tooth's root, periodontal ligament (PDL), and the surrounding bone are all impacted. The periodontal ligament is a specialized tissue that connects the tooth's root to the bone, containing vital cells necessary for the tooth to reattach and heal after reimplantation. When a tooth is avulsed, these cells can dry out and die quickly, which is why immediate action is paramount.
Unlike a chipped or fractured tooth, an avulsed tooth is entirely separated from the mouth. It's a true emergency because the viability of the tooth hinges on the survival of these PDL cells. The faster the tooth is reinserted into the socket and supported by professional dental care, the higher the chances of these cells surviving and the tooth successfully re-establishing its connection to the bone.
Why Time is the Ultimate Factor
The viability of an avulsed tooth is directly proportional to the "extra-alveolar dry time"—the time the tooth spends outside the mouth without proper storage.
- Optimal Window: Ideally, a tooth should be reimplanted within 5-10 minutes of avulsion. Within this timeframe, the chances of successful reattachment and long-term survival are highest.
- Critical Threshold: After 60 minutes of dry time, the prognosis for successful reimplantation drops significantly. The periodontal ligament cells begin to die, making reattachment much more challenging and increasing the risk of complications like root resorption or ankylosis (the tooth fusing directly to the bone).
- Beyond 2 Hours: While reimplantation can still be attempted after two hours, the likelihood of complications is very high, and the long-term prognosis is often poor.
Understanding this critical timeline emphasizes the urgency of knowing exactly what to do immediately after a tooth is knocked out.
Types of Tooth Avulsion
While "knocked out tooth" generally refers to a complete avulsion, there are variations in dental trauma that might seem similar but require different approaches.
1. Complete Avulsion (Knocked Out Tooth)
This is the scenario we are primarily discussing: the entire tooth, including its root, is fully dislodged from the socket.
2. Partial Avulsion (Extrusion)
In this case, the tooth is still in its socket but has been partially dislodged, appearing longer than adjacent teeth. It's still attached but loose and displaced. This also requires immediate dental attention, but the first aid steps differ as the tooth is not completely out of the mouth.
3. Lateral Luxation
The tooth is displaced sideways, either forward, backward, or to the side, but remains in the socket. It is usually firm and often fractured.
4. Intrusive Luxation
The tooth is pushed deeper into the socket, making it appear shorter than adjacent teeth. This is a severe injury as it can damage the developing permanent tooth if it's a primary tooth.
For the purpose of this article, we will focus on complete avulsion of permanent teeth, which demands the most critical immediate response. Children's primary teeth are a special consideration discussed later.
Causes: Why a Tooth Gets Knocked Out
Dental avulsion is almost always the result of significant trauma or impact to the face and mouth. Understanding the common causes can help in prevention.
- Sports Injuries: This is a leading cause, particularly in contact sports like football, hockey, basketball, and soccer. Any sport involving potential falls, collisions, or impacts to the face carries a risk. Studies show that around 39% of dental injuries are sports-related.
- Accidents:
- Falls: Tripping, slipping, or falling from a height can lead to direct impact on the mouth. This is common in both young children and older adults.
- Bicycle Accidents: Falling off a bike, especially without a helmet or face protection, frequently results in dental trauma.
- Motor Vehicle Accidents (MVAs): Car accidents, particularly those involving facial impact with the steering wheel, dashboard, or airbag, can cause severe dental injuries including avulsion.
- Fights/Assaults: Direct blows to the face during altercations.
- Workplace Accidents: Industries where there's a risk of falling objects or machinery impact.
- Other Traumas: Less common causes can include recreational activities like skateboarding accidents or even impacts from playground equipment.
Signs and Symptoms
The signs of a knocked-out tooth are usually unmistakable:
- Missing Tooth: The most obvious sign is the complete absence of a tooth from its normal position in the dental arch.
- Visible Socket: An empty space where the tooth once was. You might see a blood clot in the socket.
- Bleeding: Significant bleeding from the empty tooth socket and surrounding gum tissue is common.
- Pain: There will likely be immediate and intense pain in the area of the avulsion and potentially surrounding teeth or jaw.
- Swelling: The gum tissue and possibly the lip or cheek around the area may swell rapidly.
- Associated Injuries: Depending on the cause, there may be other facial injuries, such as cuts to the lips, tongue, or cheek, or even jaw fractures. In severe cases of trauma, you might also experience signs like a swollen face or even TMJ swelling face, indicating potential injury to the temporomandibular joint, which connects your jaw to your skull. This often requires additional medical assessment.
Step-by-Step Process: What to Do Immediately When a Tooth is Knocked Out
This is the most critical section for anyone encountering a knocked-out permanent tooth. Your actions in the first few minutes can save the tooth.
Immediate First Aid (The First Few Minutes)
- Stay Calm and Locate the Tooth: While easier said than done, panicking wastes precious time. Find the tooth quickly.
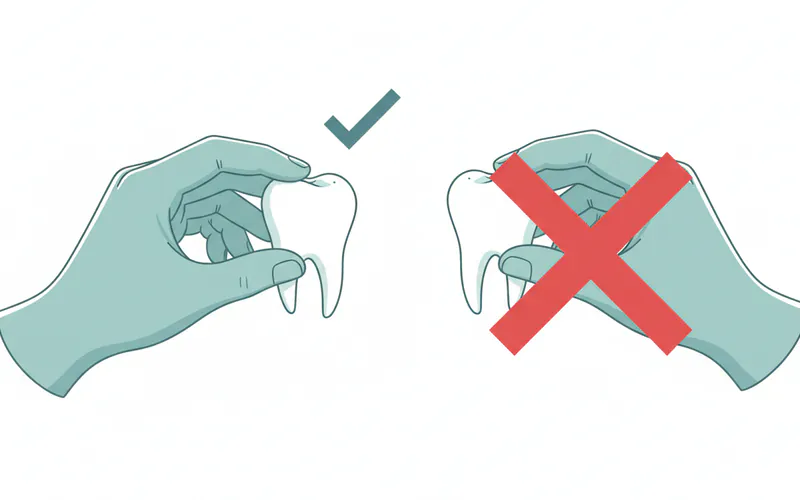
- Handle the Tooth Properly:
- Hold it by the crown ONLY. The crown is the visible, chewing part of the tooth.
- NEVER touch the root. The root surface contains delicate cells of the periodontal ligament (PDL) that are vital for successful reattachment. Touching or scrubbing the root can damage these cells.
- Clean the Tooth (If Necessary, Gently):
- If the tooth is dirty (e.g., fell on the ground), gently rinse it with cold running water or saline solution for no more than 10 seconds.
- DO NOT scrub, scrape, or wipe the tooth. Do not use soap, alcohol, or any harsh chemicals. The goal is to remove visible debris without harming the root surface.
- Reinsert the Tooth (If Possible and Safe):
- This is the best option if you can do it quickly and correctly.
- Gently push the tooth back into its socket. Ensure it's facing the correct way (the same orientation it was before).
- Apply gentle but firm pressure with your fingers.
- Once reinserted, bite down on a piece of gauze, a clean cloth, or even your finger to hold the tooth in place. This also helps control bleeding.
- Pro Tip: If you're unsure which way the tooth goes, try gently fitting it; it should only fit comfortably one way. Do not force it.
- If Reinsertion Isn't Possible or Safe, Store It Correctly:
- Best Storage Mediums (in order of preference):
- Hanks' Balanced Salt Solution (HBSS) / Emergency Tooth Preservation Kit: If available (e.g., Save-A-Tooth kit), this is ideal as it provides nutrients to the PDL cells.
- Milk (whole milk is preferred): Easily accessible and has an osmolarity and pH that is somewhat compatible with PDL cells, keeping them viable for a few hours.
- Saliva (in the mouth): The injured person (if conscious and able to cooperate) can hold the tooth in their mouth, between the cheek and gums, or under the tongue. This keeps it moist in a physiological environment. Caution: Only do this if there is no risk of swallowing the tooth, especially with small children or unconscious individuals.
- Saline Solution: A less ideal but acceptable option if others aren't available.
- NEVER store a knocked-out tooth in tap water. Tap water contains chemicals and has an osmotic pressure that can cause the PDL cells to swell and burst, killing them rapidly.

- Best Storage Mediums (in order of preference):
- Control Bleeding:
- Bite down on a clean piece of gauze or cloth placed over the empty socket. Maintain pressure to help stop the bleeding.
- If there's significant pain or swelling, a cold compress applied to the outside of the face can help.
Seek Immediate Professional Dental Care
Once the initial first aid is administered, the next critical step is to get to a dentist or emergency dental clinic immediately.
- Call Ahead: Contact your dentist or an emergency dental service on your way. Explain the situation – a permanent tooth has been knocked out and what steps you've taken (reinserted/storage). This allows them to prepare for your arrival.
- Transport Carefully: If the tooth is reinserted, ensure the patient keeps biting down gently. If stored, transport the tooth with the patient, carefully ensuring it remains in the proper storage medium.
- Emergency Room vs. Dentist: For an isolated knocked-out tooth without other severe injuries (e.g., head trauma, broken bones), an emergency dentist or oral surgeon is preferable as they are best equipped to handle dental avulsions. If there are other serious injuries, go to the nearest emergency room first.
Professional Treatment Options and What to Expect at the Dentist
Upon arrival at the dental office, the dentist will assess the situation and proceed with treatment.
1. Reimplantation and Splinting (If the Tooth Was Saved)
- Assessment: The dentist will first assess the tooth, the socket, and the surrounding tissues. X-rays will be taken to check for other dental injuries, root fractures, or foreign bodies in the socket.
- Cleaning and Preparation: The socket will be gently rinsed to remove any clots or debris. The tooth may be further cleaned, if necessary.
- Reimplantation: If the tooth was not reinserted by you, the dentist will gently place it back into the socket.
- Splinting: Once in place, the tooth will be stabilized with a flexible splint. This is typically a thin wire or composite resin bonded to the avulsed tooth and its adjacent, healthy teeth. The splint holds the tooth in position while the periodontal ligament heals.
- Duration: The splint is usually kept in place for 1-2 weeks for uncomplicated avulsions. If there was associated bone injury, it might remain for 3-4 weeks.
- Antibiotics & Pain Management: The dentist may prescribe antibiotics to prevent infection and recommend over-the-counter pain relievers or prescribe stronger medication if needed.
- Tetanus Shot: If the injury occurred outdoors and the patient's tetanus vaccination status is unclear or outdated, a tetanus booster may be recommended.
- Root Canal Treatment: In most cases of avulsion where the tooth's nerve has been damaged or severed, a root canal will be necessary after reimplantation, typically 7-14 days later. This prevents future infection and discoloration of the tooth. It's usually performed once the tooth has stabilized in the socket, but before the splint is removed.
2. Alternative Treatment Options (If Reimplantation Isn't Possible)
If the tooth cannot be reimplanted (e.g., too much dry time, severe root damage, primary tooth), or if reimplantation fails, other options are available to restore the missing tooth.
a. Dental Implant
- What it is: A titanium post surgically placed into the jawbone, acting as an artificial tooth root. After healing, a crown is attached to the implant.
- Pros: Highly durable, aesthetically pleasing, functions like a natural tooth, preserves jawbone, does not affect adjacent teeth.
- Cons: Surgical procedure, higher initial cost, requires sufficient bone density, can take several months for full completion (healing period), not suitable for growing jaws (typically placed after jaw development is complete, late teens/early 20s).
- Cost: Ranges from $3,000 to $6,000 per tooth (including implant, abutment, and crown).
b. Dental Bridge (Fixed Partial Denture)
- What it is: One or more artificial teeth (pontics) are held in place by dental crowns cemented onto the natural teeth adjacent to the gap.
- Pros: Permanent, aesthetically good, quicker to place than implants, generally less invasive than implant surgery.
- Cons: Requires grinding down healthy adjacent teeth to place crowns, can put stress on supporting teeth, more difficult to clean, may need replacement after 5-15 years.
- Cost: Ranges from $2,000 to $5,000 for a three-unit bridge (replacing one tooth).
c. Removable Partial Denture
- What it is: A removable appliance with artificial teeth attached to a metal or acrylic framework, which clasps onto existing natural teeth.
- Pros: Least invasive, most affordable, easily removable for cleaning.
- Cons: Not as stable or comfortable as fixed options, can affect speech or eating, needs to be removed daily, less aesthetic than implants or bridges, can accelerate bone loss over time.
- Cost: Ranges from $600 to $2,500.
Comparison Table: Tooth Replacement Options
| Feature | Reimplantation (Successful) | Dental Implant | Dental Bridge | Removable Partial Denture |
|---|---|---|---|---|
| Preserves Original Tooth | Yes | No (replaces) | No (replaces) | No (replaces) |
| Esthetics | Excellent (natural tooth) | Excellent | Very Good | Good |
| Function | Excellent (natural tooth) | Excellent (like natural) | Good | Fair (can shift) |
| Longevity | Variable (2-20+ years, often needs root canal later) | 15-25+ years | 5-15 years | 5-10 years (with adjustments) |
| Invasiveness | Moderate (splinting, root canal) | Surgical | Requires reduction of adjacent teeth | Non-invasive (no tooth alteration) |
| Cost Range (US) | $1,500 - $4,000 (incl. root canal) | $3,000 - $6,000 per tooth | $2,000 - $5,000 (3-unit) | $600 - $2,500 |
| Timeframe | Immediate + 1-2 weeks splint + root canal | Months (healing & crown placement) | Weeks | Weeks |
| Bone Preservation | Yes | Excellent | Poor (can lead to bone loss under bridge) | Poor (can lead to bone loss) |
Cost and Insurance Considerations in the US
The cost of handling a knocked-out tooth can vary significantly based on whether the tooth is successfully reimplanted and the subsequent treatments required, or if an alternative replacement is chosen. Location, the complexity of the case, and the dental professional's fees also play a role.
Average US Price Ranges:
- Emergency Dental Visit (Initial Assessment & Reimplantation/Splinting):
- Without insurance: $200 - $600 (This often includes examination, X-rays, and the initial procedure).
- With insurance: You'll typically pay your co-pay (e.g., $50-$100) and a percentage of the remaining cost after your deductible.
- Root Canal Treatment (if needed after reimplantation):
- Front tooth: $700 - $1,500
- Back tooth: $1,000 - $2,000+
- Total for Reimplantation + Root Canal: $1,500 - $4,000
- Dental Implant (including surgical placement, abutment, and crown):
- $3,000 - $6,000 per tooth
- Dental Bridge (3-unit):
- $2,000 - $5,000
- Removable Partial Denture:
- $600 - $2,500
Insurance Coverage Details:
- Dental Insurance: Most comprehensive dental insurance plans will cover a portion of emergency dental care, including reimplantation and subsequent root canal treatment.
- Deductibles: You will likely need to meet your annual deductible (e.g., $50-$150) before your insurance starts paying.
- Co-insurance: After the deductible, plans typically cover 50% to 80% of major procedures like root canals, and 80% to 100% of preventive/basic care.
- Annual Maximums: Be aware of your plan's annual maximums (often $1,000 - $2,000). A knocked-out tooth requiring multiple procedures can quickly hit this limit.
- Medical Insurance: In cases of severe trauma, especially if it's part of a larger injury (e.g., a car accident, fall with other facial trauma), medical insurance might cover some aspects of the initial emergency visit and diagnostics, especially if seen in an emergency room first. However, long-term dental restoration is rarely covered by medical insurance.
- Workers' Compensation: If the injury occurred on the job, workers' compensation should cover all related dental and medical costs.
Payment Plans and Financing Options:
- Dental Office Payment Plans: Many dental offices offer in-house payment plans, allowing you to pay in installments.
- Third-Party Financing (e.g., CareCredit): These medical credit cards offer special financing options, including interest-free periods if paid within a certain timeframe.
- Personal Loans: Banks and credit unions offer personal loans that can be used for significant medical expenses.
- Health Savings Accounts (HSAs) / Flexible Spending Accounts (FSAs): If you have an HSA or FSA, you can use these tax-advantaged accounts to pay for qualified dental expenses.
Recovery and Aftercare
The recovery process after a knocked-out tooth depends heavily on whether the tooth was reimplanted or if an alternative replacement was chosen.
After Successful Reimplantation:
- Diet: Stick to a soft diet for several weeks to avoid putting stress on the healing tooth. Avoid biting into hard or chewy foods.
- Oral Hygiene: Maintain excellent oral hygiene, but be extremely gentle around the injured tooth.
- Use a very soft toothbrush and brush gently.
- Rinse with an antimicrobial mouthwash (like chlorhexidine, if prescribed by your dentist) or warm salt water (1/2 teaspoon salt in 8 oz warm water) 2-3 times a day to reduce bacteria and promote healing.
- Avoid flossing directly around the splinted teeth.
- Medication: Take prescribed antibiotics as directed to prevent infection. Use pain relievers (over-the-counter or prescription) as needed.
- Follow-Up Appointments: Attend all scheduled follow-up appointments.
- The splint will typically be removed after 1-4 weeks.
- Regular check-ups and X-rays will be necessary for months, and sometimes years, to monitor the tooth for complications like root resorption or ankylosis.
- Root canal treatment will be necessary in most cases, typically within 7-14 days after reimplantation, once the tooth is stable.
- Avoid Trauma: Be extra cautious to avoid any further trauma to the face and mouth during the healing period.
After Dental Implant Placement:
- Initial Healing: Soft diet, pain management, and meticulous oral hygiene are crucial during the initial healing phase (osseointegration), which can take 3-6 months.
- Follow-ups: Regular check-ups to monitor implant healing.
- Crown Placement: Once the implant has integrated with the bone, the abutment and custom crown will be placed.
- Long-Term Care: Implants require the same diligent brushing, flossing, and regular dental check-ups as natural teeth to prevent peri-implantitis (gum disease around the implant).
After Dental Bridge Placement:
- Initial Adjustment: You may experience some sensitivity to hot/cold, and it may take a few days to adjust to the feel of the new bridge.
- Oral Hygiene: Special attention to cleaning under the bridge with floss threaders or interdental brushes is necessary to prevent plaque buildup and gum disease.
- Diet: Avoid extremely hard or sticky foods that could dislodge or damage the bridge.
- Regular Check-ups: Routine dental visits are essential to monitor the health of the supporting teeth and the bridge itself.
After Removable Partial Denture:
- Adjustment: It will take time to get used to wearing and speaking with the denture.
- Cleaning: Remove the denture daily for thorough cleaning and soak it in a denture cleaning solution.
- Nightly Removal: Typically, removable partial dentures should be removed at night to allow gum tissues to rest.
- Diet: Avoid very sticky or hard foods that could dislodge or damage the denture.
- Regular Check-ups: To monitor fit and adjust as needed.
Prevention: Avoiding a Knocked Out Tooth
Prevention is always better than cure, especially when it comes to saving your natural teeth.
- Wear a Mouthguard for Sports: This is the single most effective preventive measure.
- Custom-fitted mouthguards provided by your dentist offer the best protection, comfort, and fit. They cost more (e.g., $150-$400) but are superior to boil-and-bite or stock mouthguards.
- Any sport with a risk of facial impact (contact sports, basketball, soccer, skateboarding, cycling, even gymnastics) warrants a mouthguard.
- Pro Tip: For children and teens involved in sports, discuss mouthguard options with your dentist. They can prevent costly and painful dental emergencies.
- Use Seatbelts and Child Safety Seats: In vehicles, proper restraint significantly reduces the risk of facial trauma during accidents.
- Wear Helmets: Helmets for cycling, skateboarding, and other activities protect not just the head but also can help mitigate facial impact.
- Childproofing Homes: For young children, ensure safe environments: use gates at stairs, cushion sharp furniture edges, and supervise play closely.
- Avoid Risky Behaviors: Avoid using teeth as tools (opening bottles, tearing packages) and be mindful of your surroundings to prevent falls.
- Address "TMJ swelling face" and "how to get gum swelling down" as related issues: While not direct causes of avulsion, if you experience significant facial swelling, especially around the jaw joint (TMJ) or persistent gum swelling (perhaps from a minor impact or dental infection), seek prompt dental evaluation. Unaddressed issues can weaken oral structures or indicate underlying problems that might make future trauma more severe.
Risks and Complications
Despite immediate and appropriate care, reimplanted teeth are still prone to certain complications.
- Root Resorption: This is the most common and serious complication. The body's immune system mistakenly identifies the tooth root as a foreign body and starts to dissolve it.
- External Resorption: Occurs on the outer surface of the root.
- Internal Resorption: Occurs within the root canal space.
- Replacement Resorption (Ankylosis): The root surface resorbs and is replaced by bone, causing the tooth to fuse directly to the jawbone. This prevents the tooth from moving naturally and can lead to it sinking below the level of adjacent teeth, especially in children.
- Infection: Despite antibiotics, bacterial infection can occur, particularly if the tooth was contaminated or if the root canal was delayed or unsuccessful.
- Ankylosis: As described above, the tooth fuses to the bone. This often leads to infraocclusion (the tooth appearing shorter) and requires extraction in the long term, especially in growing individuals.
- Pulp Necrosis: The nerve and blood supply inside the tooth die, making a root canal virtually always necessary for permanent teeth.
- Discoloration: The tooth may darken over time due to internal bleeding or if a root canal is not performed.
- Loss of the Tooth: Despite best efforts, the reimplanted tooth may eventually fail and need to be extracted, necessitating one of the alternative replacement options.
- Damage to Adjacent Teeth/Structures: The impact that caused the avulsion might have also damaged nearby teeth, the jawbone, or soft tissues, potentially leading to gum swelling down from the trauma.
Children / Pediatric Considerations
A knocked-out tooth in a child requires special consideration, primarily distinguishing between primary (baby) teeth and permanent teeth.
Knocked Out Primary (Baby) Tooth
- Do NOT Reimplant: The general rule for a completely avulsed primary tooth is not to reimplant it. Reinserting a primary tooth can cause significant damage to the developing permanent tooth bud beneath it, leading to issues like enamel defects, root abnormalities, or even impaction of the permanent tooth.
- Seek Dental Care: Even though you don't reimplant it, you should still see a pediatric dentist immediately. They will:
- Check for fragments of the tooth left in the gum.
- Assess for other injuries to the gums, lips, or tongue.
- Take X-rays to ensure the permanent tooth bud is undamaged.
- Provide instructions for pain management and bleeding control.
- Discuss space maintainers if necessary, though often the space is naturally held until the permanent tooth erupts.
- Parental Guidance: Reassure the child, control bleeding, and apply a cold compress to reduce swelling.
Knocked Out Permanent Tooth in a Child/Adolescent
- Treat Exactly Like an Adult Tooth: If a permanent tooth (even a newly erupted one) is knocked out, follow all the immediate first aid steps for adults: handle by the crown, gentle rinse, attempt immediate reimplantation, or store in milk/HBSS.
- Time is Even More Critical: In young permanent teeth with incompletely formed roots (open apices), the chances of successful revascularization (re-establishing blood supply) are higher if reimplanted very quickly. A successful revascularization may reduce or even eliminate the need for a root canal.
- Pediatric Dentist: A pediatric dentist or endodontist experienced in dental trauma will be best equipped to handle these cases, considering the child's growth and development.
Cost Breakdown: Detailed US Averages
Beyond the general ranges mentioned, let's break down potential full costs for different scenarios.
Scenario 1: Successful Reimplantation with Follow-up Root Canal
| Service | Average Cost (Without Insurance) | Average Cost (With Insurance, e.g., 50% coverage after $100 deductible) |
|---|---|---|
| Emergency Exam & X-rays | $100 - $250 | $50 (deductible) + $25 (20% of remaining $125) = ~$75 |
| Reimplantation & Splinting | $400 - $800 | $200 - $400 |
| Root Canal (Anterior Tooth) | $700 - $1,500 | $350 - $750 |
| Total Estimated Cost | $1,200 - $2,550 | $625 - $1,225 (Plus potential for additional follow-up visits) |
| Note: This does not include potential crown after root canal if needed. |
Scenario 2: Dental Implant Replacement (When Reimplantation Fails or is Not Possible)
| Service | Average Cost (Without Insurance) | Average Cost (With Insurance, limited or no coverage) |
|---|---|---|
| Tooth Extraction (if necessary) | $150 - $400 | $75 - $200 |
| Bone Graft (if needed) | $400 - $1,200 | $200 - $600 |
| Implant Post Placement (Surgery) | $1,500 - $3,000 | $750 - $1,500 (Often considered 'major' with 50% or less coverage) |
| Abutment | $300 - $600 | $150 - $300 |
| Implant Crown | $1,000 - $2,000 | $500 - $1,000 (Often considered 'major' with 50% or less coverage) |
| Total Estimated Cost | $3,350 - $7,200 | $1,675 - $3,600+ (Highly variable based on plan; many plans have specific implant exclusions or lower maximums) |
| Note: Implants are often not fully covered by basic dental insurance plans. |
Cost-Saving Tips:
- Act Fast: The single biggest cost-saving measure is successfully reimplanting your own tooth. This avoids the much higher costs of implants or bridges.
- Utilize Insurance Benefits: Understand your dental insurance policy, deductibles, co-pays, and annual maximums. Don't hesitate to call your provider for clarification.
- Seek Multiple Opinions for Replacement: For non-emergency replacement options like implants or bridges, get quotes from a few different dentists or specialists.
- Dental Schools: University dental schools often provide high-quality care at a reduced cost, as procedures are performed by students under the supervision of experienced faculty.
- Payment Plans: Discuss payment plans with your dental office or explore third-party financing options.
- Health Savings Accounts (HSAs) & Flexible Spending Accounts (FSAs): Maximize these tax-advantaged accounts to cover dental expenses.
Frequently Asked Questions
1. How long can a knocked-out tooth survive outside the mouth?
A permanent tooth has the best chance of survival if reimplanted within 5-10 minutes. After 60 minutes of dry time, the prognosis drops significantly, though efforts can still be made. Proper storage in milk or an emergency kit can extend this window for several hours, but immediate reimplantation is always superior.
2. Can I put a knocked-out baby tooth back in?
No, you should never reimplant a knocked-out baby (primary) tooth. Reinserting it can damage the developing permanent tooth underneath. Instead, control bleeding and seek immediate dental evaluation to ensure no other injuries have occurred and to monitor the permanent tooth bud.
3. Will a reimplanted tooth be painful?
Initial pain from the trauma is expected, but once the tooth is reimplanted and stabilized, and local anesthesia wears off, discomfort is usually manageable with over-the-counter pain relievers. Your dentist may prescribe stronger medication if needed. Root canal treatment, if performed, will be done under anesthesia.
4. What are the chances of a reimplanted tooth failing?
The success rate depends heavily on the extra-oral dry time and storage medium. If reimplanted within 5-10 minutes with proper handling, success rates can be as high as 90%. However, complications like root resorption or ankylosis can develop months or years later, leading to eventual failure in 50% or more cases, even with initial success.
5. What if the tooth broke in half when it was knocked out?
If the tooth broke in half, it is typically not suitable for reimplantation. The root structure necessary for reattachment would be compromised. In such cases, the dentist will discuss alternative replacement options like a dental implant or bridge.
6. Can a knocked-out tooth be saved if it's dirty?
Yes, but it must be cleaned correctly. Gently rinse the tooth with cold water or saline for no more than 10 seconds, holding it by the crown. Do not scrub or use harsh cleaners. The goal is to remove gross debris without damaging the delicate root surface.
7. How long will I have to wear the splint?
A flexible splint is typically worn for 1-2 weeks for an uncomplicated avulsion. If there are associated bone fractures or other complex injuries, the splint might need to stay in place for 3-4 weeks to allow for proper healing.
8. Will I need a root canal if my permanent tooth is reimplanted?
In nearly all cases of avulsed permanent teeth, the pulp (nerve and blood vessels) inside the tooth dies due to severed blood supply. Therefore, a root canal treatment is almost always necessary and is usually performed 7-14 days after reimplantation to prevent infection and discoloration.
9. What are the alternatives if the tooth cannot be saved?
If reimplantation is unsuccessful or not possible, common alternatives include a dental implant (a permanent screw-in replacement), a dental bridge (a fixed appliance using adjacent teeth for support), or a removable partial denture (a removable appliance). The best option depends on your individual situation, budget, and oral health.
10. Does insurance cover a knocked-out tooth?
Most dental insurance plans cover a portion of emergency dental services, including reimplantation and follow-up root canal treatment, usually after a deductible and with co-insurance. Coverage for dental implants or bridges varies significantly by plan, often with lower coverage percentages or specific exclusions.
When to See a Dentist
A knocked-out tooth is a definitive dental emergency requiring immediate attention.
Immediate Emergency Care (Go to the dentist or emergency room NOW):
- Permanent Tooth Avulsion: If any permanent tooth (adult tooth) has been completely knocked out, follow the first aid steps and get to a dentist or emergency dental clinic within 30-60 minutes.
- Partial Avulsion/Severe Luxation: If a permanent tooth is severely loose, displaced, or extruded (hanging out), but not completely out of the socket.
- Suspected Jaw Fracture: If you suspect your jaw is broken (e.g., difficulty opening/closing mouth, severe pain, misalignment).
- Other Severe Facial Trauma: If the knocked-out tooth is accompanied by significant lacerations, uncontrolled bleeding, signs of concussion, or other head/facial injuries, go to the nearest emergency room first.
- Persistent Bleeding: If bleeding from the socket or gums cannot be controlled with direct pressure.
- Significant Swelling: Rapidly increasing swelling in the face or mouth, particularly if affecting breathing or swallowing, is an emergency. This can be related to the trauma (e.g., gum swelling down from impact) or indicate infection.
When to Consult (Within 24-48 hours, but still urgent):
- Knocked-out Baby Tooth: While not reimplanted, a pediatric dentist should still evaluate the child to check for other injuries and ensure the permanent tooth bud is safe.
- Chipped or Fractured Tooth: If a piece of tooth is broken off but the tooth is still in place, it's urgent but not always an immediate emergency like an avulsion.
Red Flags:
- Fever or increasing pain/swelling after initial treatment, which could indicate infection.
- Any numbness or tingling in the face, which could suggest nerve damage.
- Difficulty breathing or swallowing after dental trauma.
Your immediate response to a knocked-out tooth is critical. By understanding the proper first aid and seeking prompt professional care, you significantly increase the chances of saving your natural tooth and restoring your smile. Don't hesitate – every minute counts.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

How to Relieve Gum Swelling
When your gums are swollen, it can be an alarming and uncomfortable experience, often signaling an underlying issue that requires attention. Statistics from the Centers for Disease Control and Prevention (CDC) reveal that **nearly half of adults aged 30 or older in the United States have some form o
February 23, 2026

Teeth Swelling: Complete Guide
When you experience teeth swelling, it's more than just a minor discomfort; it's a clear signal from your body that something is amiss within your oral cavity, often indicating an underlying infection or inflammation that requires prompt attention. A recent survey revealed that **over 25% of adu
February 23, 2026

Submandibular Salivary Gland Swelling: Complete Guide
When you notice a peculiar lump or uncomfortable fullness beneath your jaw, it can be an alarming experience. This sensation, often accompanied by pain and difficulty swallowing, could indicate submandibular salivary gland swelling. Affecting an estimated 1 in 10,000 adults annually, conditi
February 23, 2026

What Helps With Gum Swelling
Gum swelling, medically known as gingival swelling or gingivitis, is a common yet often underestimated dental issue affecting millions of Americans. Have you ever woken up with sore, puffy gums that bleed easily when you brush? You're not alone. Research indicates that nearly **half of all a
February 23, 2026