Knocked Out Teeth: Complete Guide

Key Takeaways
- Experiencing a knocked out tooth, medically termed dental avulsion, can be a startling and distressing event. Every year, an estimated five million Americans experience dental trauma, with a significant percentage involving teeth being completely dislodged from their socket. While the immediate
Knocked Out Teeth: Complete Guide
Experiencing a knocked out tooth, medically termed dental avulsion, can be a startling and distressing event. Every year, an estimated five million Americans experience dental trauma, with a significant percentage involving teeth being completely dislodged from their socket. While the immediate shock can be overwhelming, knowing precisely what to do in these critical moments can be the difference between losing a tooth permanently and successfully replanting it. This guide from SmilePedia.net aims to provide a comprehensive, medically accurate roadmap for understanding, treating, and preventing knocked out teeth. We'll delve into the immediate first aid steps, professional treatment options, potential costs, and crucial long-term care to help you navigate this dental emergency effectively and preserve your oral health.
Key Takeaways:
- Time is Critical: For permanent teeth, immediate action within 5-30 minutes significantly increases the chances of successful replantation. Success rates drop rapidly after 30 minutes and are very low after 60 minutes.
- Proper Handling: Always pick up a knocked out tooth by its crown, never by the root, to avoid damaging critical cells.
- Storage Medium: Transport the tooth in a suitable medium like cold milk, Hank's Balanced Salt Solution (HBSS), saliva, or water (as a last resort) to keep root cells viable.
- Professional Care: An emergency dental visit is mandatory for any knocked out permanent tooth. A dentist will clean, replant, and splint the tooth, and may prescribe antibiotics.
- Cost Variation: Emergency replantation, splinting, and follow-up root canal treatment can range from $1,500 to $4,000+ without insurance. Restorative options like dental implants or bridges are substantially more, ranging from $3,000 to $8,000+ per tooth.
- Long-Term Outlook: Even with successful replantation, root canal treatment is often necessary, and long-term monitoring for complications like root resorption is crucial.
- Prevention: Wearing a custom-fitted mouthguard during sports is the most effective way to prevent knocked out teeth.
What It Is / Overview
A knocked out tooth, or dental avulsion, occurs when a tooth is completely dislodged from its socket in the jawbone. This is a severe form of dental trauma that severs the blood vessels, nerves, and periodontal ligament fibers connecting the tooth root to the bone. The periodontal ligament (PDL) is a specialized connective tissue that acts as a shock absorber and plays a vital role in tooth support and regeneration. When a tooth is avulsed, these delicate PDL cells on the root surface are damaged or die if not kept moist and viable.
Unlike a broken bone that can heal naturally, an avulsed tooth requires immediate and specific intervention to maximize the chances of successful reattachment and long-term survival. The primary goal in treating a knocked out permanent tooth is replantation – carefully placing the tooth back into its original socket. This allows the remaining viable PDL cells to reattach to the bone, ideally restoring the tooth's function and vitality. Without prompt action, the tooth will not naturally reinsert itself and will be lost.
Types / Variations
While "knocked out tooth" typically refers to a complete avulsion, it's important to distinguish between primary (baby) teeth and permanent teeth, as the treatment approach differs significantly.
Permanent Teeth Avulsion
This is the most critical type, demanding immediate attention. When a permanent tooth is fully knocked out, the objective is always to attempt replantation, provided the tooth can be found, is relatively intact, and appropriate first aid steps are followed. The long-term prognosis depends heavily on the time elapsed out of the socket and the storage medium used.
Primary (Baby) Teeth Avulsion
If a primary tooth is knocked out, the approach is generally different. The American Academy of Pediatric Dentistry (AAPD) and the American Dental Association (ADA) typically recommend against replanting primary teeth. The primary concern is potential damage to the developing permanent tooth bud located beneath the primary tooth. Replanting a primary tooth can introduce infection, cause ankylosis (fusion of the root to the bone), or lead to developmental disturbances in the succedaneous (erupting permanent) tooth. Instead, the focus is on managing the space, preventing infection, and ensuring proper development of the permanent tooth.
Causes / Why It Happens
Knocked out teeth are almost always the result of traumatic injury. These incidents can range from everyday accidents to high-impact events. Understanding the common causes can help in implementing preventative measures.
- Sports-Related Injuries: This is one of the most common causes, particularly in contact sports like football, basketball, hockey, and soccer. Even non-contact sports can pose a risk due to falls or accidental collisions. Studies show that athletes are 60 times more likely to suffer dental trauma if they don't wear a mouthguard.
- Falls: Accidental falls, especially in children, the elderly, or individuals with balance issues, can lead to facial impact and tooth avulsion. This includes falls from bikes, skateboards, or simple slips.
- Motor Vehicle Accidents: Car crashes, motorcycle accidents, and pedestrian accidents often result in significant facial trauma, including avulsed teeth, due to the force of impact.
- Fights and Assaults: Direct blows to the face during altercations can easily dislodge teeth.
- Other Accidents: Incidents such as hitting a hard surface unexpectedly, using teeth as tools (e.g., opening bottles), or industrial accidents can also cause severe dental trauma.
- Risk Factors: Certain factors can increase the likelihood of avulsion:
- Protruding Upper Incisors: Teeth that stick out are more exposed and vulnerable to trauma.
- Lack of Mouthguard: Not wearing a protective mouthguard during high-risk activities.
- Oral Piercings: Can sometimes snag or cause trauma in an impact.
- Malocclusion: Certain bite issues can make teeth more susceptible to injury.
Signs and Symptoms
The signs and symptoms of a knocked out tooth are usually very evident and require immediate attention.
- Missing Tooth: The most obvious sign is the complete absence of a tooth from its socket.
- Empty Socket: You will see a visible hole in the gum line where the tooth used to be.
- Bleeding: There will likely be bleeding from the tooth socket due as blood vessels are severed. The amount of bleeding can vary but typically subsides with pressure.
- Pain: While the initial shock might mask it, there may be pain, especially if other facial injuries (e.g., fractured jaw, lip lacerations) are present. The socket itself may be tender.
- Swelling: The gum tissue around the empty socket or surrounding facial areas may start to swell soon after the injury.
- Visible Tooth: The avulsed tooth will be somewhere nearby, often on the ground or stuck in clothing, usually covered in debris or blood.

Treatment Options
The treatment for a knocked out tooth depends critically on whether it's a permanent or primary tooth, and how quickly care is sought. For permanent teeth, the primary goal is replantation. If replantation is not possible or unsuccessful, restorative options are considered.
1. Immediate First Aid and Replantation (Permanent Teeth)
This is the gold standard for saving a permanent knocked out tooth. The success rate is highly dependent on swift action.
Pros:
- Preserves natural tooth structure and function.
- Maintains the natural bite and aesthetics.
- Potentially avoids more extensive and costly restorative procedures later.
- Maintains bone density in the jaw.
Cons:
- Requires extremely fast action from the patient or bystander.
- Risk of complications like root resorption, ankylosis, or infection.
- Often requires subsequent root canal treatment.
- Not always successful; the tooth may still be lost long-term.
Pro Tip: The first 5-30 minutes are crucial. If you can get the tooth back into its socket within this timeframe, the chances of successful reattachment are highest.
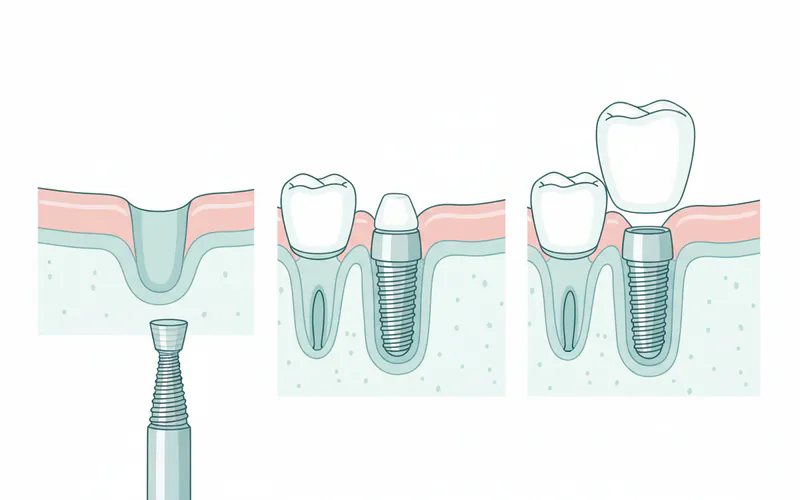
2. Dental Implants (If Replantation Fails or is Not Possible)
If replantation is unsuccessful, or if the tooth is lost due to delays or damage, a dental implant is often the preferred long-term solution for replacing a single permanent tooth.
Pros:
- Highly durable and long-lasting: Can last for decades, often a lifetime, with proper care.
- Mimics natural tooth: Looks, feels, and functions like a natural tooth.
- Preserves bone density: The implant post stimulates the jawbone, preventing bone loss.
- Doesn't affect adjacent teeth: No need to alter healthy neighboring teeth, unlike a bridge.
- High success rate: Generally over 95%.
Cons:
- High cost: Typically the most expensive single-tooth replacement option.
- Surgical procedure: Involves minor surgery, with associated recovery time.
- Long treatment timeline: Can take several months (3-9 months) from extraction to final crown placement, as bone healing around the implant is required.
- Not suitable for everyone: Requires sufficient bone density and good general health.
- Risk of complications: Though rare, can include infection, nerve damage, or implant failure.
3. Fixed Dental Bridge (If Implants are Not Suitable)
A dental bridge is a prosthetic device that fills the gap created by a missing tooth by using the adjacent teeth as anchors.
Pros:
- Faster treatment timeline: Can be completed in a few weeks compared to months for implants.
- Lower upfront cost: Generally less expensive than a single dental implant.
- Esthetically pleasing: Can blend well with natural teeth.
- Does not require surgery: Non-invasive compared to implant placement.
Cons:
- Requires alteration of healthy adjacent teeth: The teeth on either side of the gap must be prepped (filed down) to support the crowns of the bridge, even if they are perfectly healthy.
- Does not prevent bone loss: The absence of a tooth root means the jawbone beneath the bridge can still resorb over time.
- Shorter lifespan than implants: Typically lasts 5-15 years before needing replacement.
- More difficult to clean: Requires special flossers to clean under the bridge, increasing the risk of decay in the anchor teeth.
- Potential for strain on anchor teeth: The supporting teeth bear extra load.
4. Removable Partial Denture (Least Preferred Long-Term)
A removable partial denture is a prosthetic device that replaces one or more missing teeth and is held in place by clasps attached to remaining natural teeth. It can be taken out for cleaning.
Pros:
- Most affordable option: Significantly less expensive than implants or fixed bridges.
- Non-invasive: No alteration to existing teeth or surgery required.
- Can be made relatively quickly: Production time is often faster than other options.
Cons:
- Less stable and comfortable: Can feel bulky and move during eating or speaking.
- Impacts taste and sensation: Can cover parts of the palate or gums, reducing sensory feedback.
- Requires daily removal for cleaning: Can be inconvenient.
- Does not prevent bone loss: Similar to bridges, bone resorption can occur.
- Can affect speech: May require an adjustment period.
- Less natural appearance: Clasps may be visible.

Step-by-Step Process for a Knocked Out Permanent Tooth
Immediate action is paramount. Here's what to do and what to expect at the dental office:
First Aid: What YOU Need to Do IMMEDIATELY
- Stay Calm: While stressful, panicking can hinder effective action.
- Locate the Tooth: Find the tooth if it's nearby.
- Handle with Care: Pick up the tooth only by its crown (the white chewing surface). Avoid touching the root at all costs, as the delicate periodontal ligament cells are vital for reattachment.
- Clean the Tooth (Gently): If the tooth is dirty, gently rinse it with cold milk or saline solution (e.g., contact lens solution) for no more than 10 seconds. DO NOT scrub, brush, or use soap/chemicals. Do not remove any tissue fragments attached to the root.
- Replant the Tooth (If Possible and Appropriate):
- If the injured person is conscious, cooperative, and able to do so, gently attempt to reinsert the tooth into its socket.
- Push it slowly and firmly back into place.
- Once in, have the person bite down gently on a piece of gauze, a clean cloth, or even their own tongue to hold the tooth in position.
- Pro Tip: If you can replant the tooth yourself immediately, this offers the highest chance of success.
- Store the Tooth (If Replantation Isn't Possible):
- If you cannot replant the tooth immediately, or if the person is unconscious/uncooperative (especially with children), store the tooth in a suitable medium for transport to the dentist. The goal is to keep the root cells moist and viable.
- Best options (in order of preference):
- Hank's Balanced Salt Solution (HBSS): Special kits (e.g., Save-a-Tooth) contain this, but it's rarely immediately available.
- Cold Milk: The most commonly available and effective medium.
- Saliva (inside the mouth): If the person is old enough not to swallow the tooth, they can hold it in their cheek pouch.
- Saline solution: (e.g., contact lens solution)
- Water: Only as a last resort and for very short periods, as it can damage root cells due to osmotic differences.
- DO NOT store in tap water for extended periods, dry cloth, or alcohol.
- Seek Immediate Dental Care: Call your dentist or an emergency dental clinic right away. Explain the situation and head there immediately. The faster you get professional care, the better the prognosis.
At the Dentist's Office: Professional Treatment
Upon arrival at the dental office, the team will spring into action:
- Assessment: The dentist will evaluate the tooth, the socket, and the patient's overall condition. They will ask about the incident, how long the tooth was out, and how it was stored. X-rays will be taken to check for bone fractures or other hidden injuries.
- Cleaning and Preparation: The tooth and socket will be thoroughly irrigated with saline solution to remove debris and bacteria. The root surface will be inspected.
- Replantation: If the tooth was not replanted on-site, the dentist will gently reinsert it into the socket. Local anesthetic may be used to ensure comfort.
- Stabilization (Splinting): Once replanted, the tooth needs to be stabilized to allow the periodontal ligament to heal. The dentist will use a flexible splint (often a wire and composite resin) to bond the avulsed tooth to its adjacent healthy teeth. This splint is typically left in place for 1-2 weeks.
- Antibiotics and Pain Management: The dentist may prescribe oral antibiotics to prevent infection and anti-inflammatory pain relievers.
- Tetanus Booster: If the injury occurred in a dirty environment and the patient's tetanus vaccination status is unclear or outdated, a tetanus booster may be recommended.
- Root Canal Consideration: For most replanted permanent teeth (especially in adults), the pulp inside the tooth will eventually die due to the severed blood supply. Therefore, a root canal treatment is often necessary. This is typically performed 7-14 days after replantation to allow initial PDL healing but before replacement resorption (where the root gets replaced by bone) begins. The goal is to remove the dead pulp tissue to prevent infection and further complications.
Cost and Insurance
The cost of treating a knocked out tooth can vary significantly depending on the type of treatment needed, geographic location, and whether the patient has dental insurance.
Emergency Replantation and Follow-up Care
If a tooth can be replanted, the initial emergency visit, splinting, and follow-up care will involve several components:

- Emergency Office Visit: $150 - $400 (initial assessment, X-rays).
- Replantation Procedure: $300 - $800.
- Splinting: $200 - $500.
- Root Canal Treatment (if needed): $800 - $2,000 per tooth (varies by tooth type, e.g., incisor vs. molar).
- Follow-up Appointments (multiple): $50 - $150 per visit.
- Antibiotics/Pain Meds: $30 - $100.
Total Estimated Cost for Successful Replantation (without insurance): $1,500 - $4,000+
Restorative Options (If Replantation Fails or is Not Possible)
If replantation is not successful or not an option, the costs escalate significantly for permanent replacement options.
- Dental Implant:
- Implant Placement (surgical phase): $1,500 - $3,000.
- Abutment: $500 - $1,500.
- Crown: $800 - $2,500.
- Bone Graft (if needed): $300 - $2,000.
- Total Estimated Cost for Single Implant (without insurance): $3,000 - $8,000+
- Fixed Dental Bridge:
- Cost per unit (a three-unit bridge replaces one missing tooth and crowns two adjacent teeth): $800 - $2,000 per unit.
- Total Estimated Cost for a 3-Unit Bridge (without insurance): $2,400 - $6,000+
- Removable Partial Denture:
- Total Estimated Cost (without insurance): $600 - $2,000+
Insurance Coverage
- Dental Insurance: Most standard dental insurance plans offer some coverage for emergency dental procedures and restorative work.
- Emergency Care: Often covered at a higher percentage (e.g., 70-80%) after a deductible. This typically includes the initial visit, X-rays, replantation, and splinting.
- Root Canal Treatment: Usually considered a "major procedure" and covered at 50-80% after deductible.
- Restorative Options: Implants are often considered elective and may have limited or no coverage, or be covered under a "major" category at 50% up to the plan's annual maximum (which is often $1,000-$2,000). Bridges and partial dentures are usually covered under "major" at 50-80%.
- Waiting Periods: Be aware that some plans have waiting periods for major procedures.
- Medical Insurance: If the knocked out tooth is part of a larger injury (e.g., car accident, severe fall) and is managed in an emergency room, some aspects might be covered by medical insurance, especially the initial hospital visit or if surgical intervention for other facial trauma is required. However, the direct dental work itself is typically not covered by medical insurance.
Cost Comparison Table
| Treatment Option | Primary Goal | Average US Cost Range (without insurance) | Timeframe to Completion | Longevity | Insurance Coverage (Typical) |
|---|---|---|---|---|---|
| Emergency Replantation | Save natural tooth | $1,500 - $4,000 | Weeks (splint removal, root canal) | Varies (months to years), high risk of long-term issues | Often 70-80% for emergency |
| Dental Implant | Permanent tooth replacement | $3,000 - $8,000 | 3-9 months | 15-25+ years (often lifetime) | Limited/50% (Major), often with max limits |
| Fixed Dental Bridge | Permanent tooth replacement | $2,400 - $6,000 (3-unit) | 2-4 weeks | 5-15 years | Often 50-80% (Major) |
| Removable Partial Denture | Temporary/affordable replacement | $600 - $2,000 | 2-6 weeks | 3-8 years | Often 50-80% (Major) |
Note: Costs are estimates and can vary by region (e.g., major metropolitan areas may have higher costs).
Recovery and Aftercare
Successful replantation is only the first step. Proper aftercare is crucial for long-term prognosis and minimizing complications.
Immediate Post-Replantation Care (First 1-2 Weeks)
- Soft Diet: Stick to soft foods that require minimal chewing. Avoid biting into hard or crunchy foods directly with the splinted tooth.
- Oral Hygiene: Maintain excellent oral hygiene, but be gentle around the splint.
- Brush carefully with a soft-bristled toothbrush.
- Use an antiseptic mouthwash (e.g., chlorhexidine gluconate, prescribed by your dentist) twice daily to control bacterial plaque and prevent infection around the splint.
- Floss around the other teeth, avoiding the splinted area.
- Avoid Trauma: Protect the area from any further bumps or impacts. Avoid sports during this healing period.
- Pain Management: Take prescribed pain relievers or over-the-counter anti-inflammatories (like ibuprofen) as directed.
- Monitor for Complications: Watch for signs of infection (fever, increased swelling, pus), persistent severe pain, or loosening of the splint.
After Splint Removal (Post 2 Weeks)
- Root Canal Treatment: As mentioned, a root canal is almost always necessary for replanted permanent teeth (especially in adults) to prevent infection and internal resorption. This is typically done within 7-14 days of replantation.
- Continued Soft Diet: Continue with a soft diet for a few more weeks, gradually introducing firmer foods as comfort allows.
- Regular Dental Check-ups: Frequent follow-up appointments are essential. Your dentist will monitor the tooth with X-rays for signs of healing or complications (e.g., root resorption, ankylosis). These checks may be every 1-3 months initially, then annually.
- Mouthguard Use: If the injury was sports-related, a custom-fitted mouthguard is strongly recommended before returning to activity.
Long-Term Monitoring
A replanted tooth, even if initially successful, requires long-term vigilance. Complications can arise months or even years later. Your dentist will monitor for:
- Root Resorption: The most common long-term complication, where the body's immune system mistakenly attacks and resorbs the tooth's root structure.
- Ankylosis: The root fuses directly to the jawbone, preventing normal tooth movement and potentially leading to the tooth sinking into the bone over time (infraocclusion).
- Discoloration: The tooth may darken over time, indicating pulp necrosis or internal resorption.
- Infection: Despite root canal treatment, infection can sometimes recur.
Pro Tip: Even if the replanted tooth feels fine, adhere strictly to all follow-up appointments and X-rays. Early detection of complications can often lead to more successful intervention.
Prevention
Preventing knocked out teeth is far better than treating them. Most avulsions are preventable through simple, effective measures.
- Wear a Custom-Fitted Mouthguard During Sports: This is by far the most effective preventative measure.
- Custom-fitted mouthguards (fabricated by a dentist): Offer the best protection, comfort, and fit. They absorb shock more effectively than over-the-counter options.
- Boil-and-bite mouthguards: Offer better protection than stock mouthguards but are less effective than custom ones.
- Stock mouthguards: Offer the least protection and comfort.
- The ADA strongly recommends mouthguards for any sport involving potential facial impact, including basketball, soccer, baseball, martial arts, and skateboarding.
- Use Seatbelts and Child Safety Seats: In motor vehicle accidents, proper restraint can significantly reduce facial trauma.
- Improve Home Safety:
- Eliminate tripping hazards.
- Install handrails on stairs.
- Ensure adequate lighting.
- Use safety gates for young children.
- Avoid Using Teeth as Tools: Never use your teeth to open bottles, tear packages, or hold items. Use appropriate tools.
- Avoid Risky Behaviors: Refrain from aggressive activities that could lead to facial trauma.
- Manage Oral Piercings: If you have oral piercings, be aware of the increased risk of tooth chipping or trauma.
- Address Protruding Teeth: For children with significantly protruding front teeth (malocclusion), orthodontic treatment might reduce their vulnerability to trauma.
Risks and Complications
Despite best efforts, replanted teeth carry various risks and potential complications.
- Root Resorption:
- Inflammatory Resorption: Occurs when necrotic (dead) pulp tissue inside the tooth and bacterial infection stimulate inflammation in the periodontal ligament, leading to progressive destruction of the root surface. This is why root canal treatment is crucial after replantation.
- Replacement Resorption (Ankylosis): This happens when the damaged root surface directly fuses with the alveolar bone. The tooth loses its natural mobility and feels "stiff." Over time, the tooth may appear to "sink" into the bone, especially in growing children, leading to an uneven gum line and bite problems. It's irreversible.
- External Cervical Resorption: Less common, but involves resorption starting from the outside of the root near the gum line.
- Pulp Necrosis and Infection: The blood supply to the tooth's pulp is almost always severed during avulsion. The pulp tissue dies, making the tooth susceptible to bacterial infection if a root canal is not performed. This can lead to pain, swelling, and how to get rid of gum swelling in this context would involve draining the infection and root canal treatment.
- Ankylosis: As described under replacement resorption, this fusion can prevent orthodontic movement if needed later and can lead to aesthetic issues in growing patients.
- Discoloration: The tooth may darken (grey, yellow, or pink) due to pulp necrosis, internal bleeding, or subsequent root canal filling materials.
- Loss of Tooth/Failed Replantation: Despite immediate action, some teeth simply do not reattach or develop severe complications, ultimately leading to loss. This risk increases significantly if the tooth was out for a long time, stored improperly, or heavily contaminated.
- Damage to Adjacent Teeth/Structures: The initial trauma might also have caused damage to neighboring teeth (e.g., fractures, luxations) or the jawbone, which might be discovered during follow-up.
- Cyst Formation: In rare cases, residual infection or inflammation can lead to the formation of a cyst around the apex of the root.
When does gum swelling occur, and how to get rid of it?
Gum swelling, in the context of a knocked out tooth, can occur for several reasons:
- Immediate Trauma: The initial injury itself will cause inflammation and swelling of the gum tissue around the socket. This is a normal part of the body's immediate response to injury.
- Infection: If the replanted tooth's pulp becomes necrotic and infected (especially if a root canal is delayed or incomplete), or if the socket becomes infected, bacteria can cause significant gum swelling, pus formation, and pain.
- Root Resorption Complications: Some forms of root resorption can lead to inflammation and localized gum swelling.
How to get rid of gum swelling related to a knocked out tooth:
- Immediate Post-Trauma Swelling:
- Cold Compress: Apply a cold compress or ice pack to the outside of the face near the affected area for 15-20 minutes on, 15-20 minutes off, during the first 24-48 hours. This helps reduce immediate inflammation and swelling.
- Over-the-Counter Anti-Inflammatories: Medications like ibuprofen (Advil, Motrin) can help manage pain and reduce swelling.
- Gentle Oral Hygiene: Continue gentle brushing and use an antiseptic mouthwash (if prescribed) to keep the area clean.
- Swelling Due to Infection:
- Immediate Dental Intervention: This type of swelling is a red flag for infection and requires prompt dental care. The dentist will need to diagnose the source of the infection.
- Root Canal Treatment: If the infection is from the pulp of a replanted tooth, a root canal will remove the infected tissue and sterilize the root canal system.
- Antibiotics: The dentist may prescribe antibiotics to help fight the bacterial infection.
- Drainage: In cases of severe swelling and pus accumulation (abscess), the dentist may need to drain the pus to relieve pressure and facilitate healing.
- Professional Cleaning: Sometimes, localized infection around the gum requires targeted cleaning by the dentist.
Pro Tip: Any persistent or worsening gum swelling after a dental trauma, especially if accompanied by pain or fever, warrants an immediate call to your dentist. Self-treating an infection can lead to more serious systemic health issues.
Children / Pediatric Considerations
Knocked out teeth are common in children, but the approach for primary (baby) teeth differs significantly from permanent teeth.
Primary (Baby) Teeth Avulsion
If a baby tooth is knocked out:
- DO NOT Replant: As per ADA and AAPD guidelines, primary teeth should generally not be replanted. Replanting a primary tooth can damage the developing permanent tooth bud underneath, leading to potential issues like enamel defects, root malformation, or even delayed eruption of the permanent tooth.
- Find the Tooth (for identification): While not for replantation, try to find the tooth so the dentist can confirm it's a primary tooth and distinguish it from a permanent one.
- Seek Dental Care: Even if not replanting, it's crucial to see a pediatric dentist immediately.
- The dentist will examine the empty socket to ensure no fragments of the tooth remain.
- They will check for other injuries to adjacent teeth, gums, or the jawbone.
- They will assess the condition of the underlying permanent tooth bud using X-rays.
- They will advise on keeping the area clean and monitoring the child.
- Space Management: If a primary molar is lost prematurely, the dentist may recommend a space maintainer to prevent adjacent teeth from drifting into the gap, which could cause crowding and eruption problems for the permanent tooth. For front teeth, space maintainers are less critical functionally but may be used for aesthetic or speech development reasons.
Permanent Teeth Avulsion in Children
If a child's permanent tooth is knocked out:
- Treat Exactly Like an Adult's Permanent Tooth: Follow all the immediate first aid steps discussed earlier, including finding the tooth, handling it by the crown, cleaning it gently, and attempting immediate replantation.
- Time Sensitivity: The urgency is even greater for children's permanent teeth as their root development may not be complete (open apex). Replantation in teeth with open apices has a higher chance of pulp revascularization (the blood supply returning), potentially avoiding the need for a root canal.
- Pediatric Dentist: Take the child to a pediatric dentist or an emergency dentist trained in pediatric dental trauma immediately.
- Splinting: The tooth will be splinted, usually for 1-2 weeks.
- Follow-up: Close monitoring is essential due to the potential for complications like root resorption and ankylosis, which can significantly impact facial growth and development.
Pro Tip for Parents: Educate yourself and your child's caregivers (teachers, coaches) on immediate first aid for dental injuries. Keep your dentist's emergency contact information readily available.
Cost Breakdown
To reiterate and expand on the financial aspects, here's a detailed cost breakdown for knocked out teeth treatment in the US, considering different scenarios.
Scenario 1: Successful Replantation of a Permanent Tooth
This is the best-case scenario for saving the tooth.
- Emergency Exam & X-rays: $150 - $400
- Replantation & Splinting: $500 - $1,300 (includes the procedure itself and materials)
- Root Canal Treatment (usually 1-2 weeks later): $800 - $2,000 (for an anterior tooth, posterior teeth might be more)
- Post-Operative Meds (antibiotics, pain relievers): $30 - $100
- Follow-up Visits (1-2 years of monitoring): $50 - $150 per visit (could be 4-6 visits initially, then annual)
- Total Low-End (without insurance): ~$1,500 - $2,500
- Total Mid-Range (without insurance): ~$2,500 - $4,000
- Total High-End (without insurance): ~$4,000 - $5,500+
Scenario 2: Failed Replantation or Tooth Not Found/Salvageable (Requires Replacement)
If replantation is not possible or fails, a permanent replacement is needed.
- Dental Implant (Single Tooth):
- Implant Placement Surgery: $1,500 - $3,000
- Abutment (connector): $500 - $1,500
- Crown (restoration): $800 - $2,500
- Bone Grafting (if needed): $300 - $2,000 (often required if bone is lost after avulsion)
- Total Low-End: ~$3,100 - $5,000
- Total Mid-Range: ~$5,000 - $6,500
- Total High-End: ~$6,500 - $8,000+
- Fixed Dental Bridge (3-Unit):
- Preparation & Impression: $100 - $300
- Each Unit (3 total): $800 - $2,000 per unit
- Total Low-End: ~$2,500 - $3,500
- Total Mid-Range: ~$3,500 - $5,000
- Total High-End: ~$5,000 - $6,000+
- Removable Partial Denture:
- Impression & Fabrication: $600 - $2,000
- Total Low-End: ~$600 - $1,000
- Total Mid-Range: ~$1,000 - $1,500
- Total High-End: ~$1,500 - $2,000+
With vs. Without Insurance
- With Insurance: As previously detailed, emergency procedures and root canals typically have higher coverage (50-80%), while implants often have limited or no coverage, or are subject to annual maximums (e.g., $1,000-$2,000). A bridge might be covered at 50-80% but will still exhaust a significant portion of an annual maximum.
- Without Insurance: You will be responsible for the full cost. Many dental offices offer discounts for cash payments or specific financing options.
Payment Plans and Financing Options
- In-Office Payment Plans: Some dental practices offer interest-free payment plans for a portion of the cost, usually for shorter terms.
- Third-Party Financing (e.g., CareCredit): These companies specialize in healthcare financing, offering low-interest or interest-free plans for a set period (e.g., 6, 12, 18 months), often with approval based on credit history.
- Dental School Clinics: Dental schools often provide services at a reduced cost compared to private practices, as procedures are performed by students under the supervision of experienced faculty. This can be a more affordable option for major restorative work, though it may involve longer appointments.
- Personal Loan: Banks or credit unions may offer personal loans for larger expenses.
Cost-Saving Tips
- Act FAST for Replantation: The most significant cost-saving measure is successfully replanting the original tooth. This avoids the much higher costs of implants or bridges.
- Understand Your Insurance: Before treatment, know exactly what your dental insurance covers, including deductibles, co-pays, annual maximums, and waiting periods.
- Get a Detailed Estimate: Request a written treatment plan with a clear breakdown of all costs before proceeding with elective restorative work.
- Discuss Alternatives: Talk to your dentist about all viable replacement options, considering both your budget and long-term oral health goals.
- Preventative Care: Investing in a custom mouthguard can cost a few hundred dollars but can save thousands in emergency treatment and tooth replacement.
Frequently Asked Questions
### Q1: Can a knocked out tooth always be saved?
A knocked out permanent tooth can often be saved, but success depends heavily on immediate action, proper handling, and the time elapsed. The sooner the tooth is replanted (ideally within 5-30 minutes), the higher the chances of success. Factors like the tooth's condition, storage medium, and individual healing capacity also play a role. However, not all knocked out teeth can be saved, especially if there's significant damage or prolonged dryness.
### Q2: How long do I have to save a knocked out tooth?
The critical window for successful replantation of a permanent tooth is within 5 to 30 minutes of the injury. After 30 minutes, the delicate cells on the root surface begin to die, significantly decreasing the chances of reattachment. Beyond 60 minutes, the prognosis is generally poor, though replantation may still be attempted by a dentist if no other option is available.
### Q3: What's the best liquid to store a knocked out tooth in for transport?
The ideal storage medium for a knocked out tooth is Hank's Balanced Salt Solution (HBSS), found in specific tooth-saving kits. If that's unavailable, cold milk is the next best option, followed by saliva (inside the cheek). As a last resort, contact lens saline solution or water can be used for very short periods, but avoid tap water for extended storage as it can damage root cells.
### Q4: Is it painful to replant a tooth?
Attempting to replant the tooth yourself immediately after the injury might cause some discomfort, but the adrenaline from the incident can sometimes numb the sensation. At the dental office, the dentist will typically use a local anesthetic to numb the area around the socket, making the professional replantation and splinting process much more comfortable. Any lingering pain after the procedure can be managed with over-the-counter pain relievers or prescribed medication.
### Q5: What if I accidentally swallow a knocked out tooth?
If you accidentally swallow a knocked out permanent tooth, it usually isn't a medical emergency, as the tooth will typically pass through your digestive system without harm. However, it means the tooth cannot be replanted. You should still see a dentist immediately to assess the empty socket for any bone fractures or other injuries and discuss replacement options.
### Q6: What are the long-term prospects for a replanted tooth?
The long-term prospects for a replanted tooth vary greatly. While initial replantation can be successful, many replanted permanent teeth (especially in adults) will require a root canal within 1-2 weeks. Complications like root resorption (where the body slowly breaks down the root) or ankylosis (fusion of the root to the bone) can occur months or even years later. Regular follow-up appointments and X-rays with your dentist are crucial for monitoring its health.
### Q7: How much does it cost if my insurance doesn't cover replantation?
Without insurance, the cost for emergency replantation, splinting, and subsequent root canal treatment for a permanent tooth can range from approximately $1,500 to $4,000 or more. If replantation fails or isn't possible, replacement options like dental implants or bridges are significantly more expensive, ranging from $3,000 to $8,000+ for an implant or $2,400 to $6,000+ for a bridge.
### Q8: What if the knocked out tooth is dirty?
If a knocked out tooth is dirty, gently rinse it with cold milk or saline solution (like contact lens solution) for no more than 10 seconds. DO NOT scrub, brush, or use soap or harsh chemicals, as this can damage the vital cells on the root surface. The goal is to remove gross debris without causing further trauma to the root.
### Q9: Can a knocked out baby tooth be replanted?
No, a knocked out primary (baby) tooth should not be replanted. Replanting a baby tooth can cause serious damage to the developing permanent tooth bud underneath, potentially leading to issues like enamel defects, root malformation, or altered eruption patterns for the permanent tooth. If a baby tooth is knocked out, see a pediatric dentist immediately for evaluation and space management if needed.
### Q10: How to get rid of gum swelling after a knocked out tooth?
Immediate gum swelling after a knocked out tooth is normal trauma response and can be reduced with a cold compress applied to the outside of the face and over-the-counter anti-inflammatories. If the swelling is persistent, worsens, or is accompanied by severe pain, fever, or pus, it's a sign of potential infection (e.g., from pulp necrosis) and requires immediate dental attention. The dentist may perform a root canal, prescribe antibiotics, or drain an abscess to eliminate the infection and reduce swelling.
When to See a Dentist
A knocked out permanent tooth is one of the most urgent dental emergencies. You should see a dentist IMMEDIATELY, ideally within 30 minutes of the incident. Every minute counts in saving the tooth.
Red Flags Indicating Immediate Emergency Care:
- Any knocked out permanent tooth: Regardless of whether you were able to replant it or not.
- Any knocked out primary (baby) tooth: While not for replantation, the socket needs to be evaluated to ensure no fragments remain and to check for damage to the underlying permanent tooth bud.
- Significant bleeding from the tooth socket or gums: That doesn't subside with firm pressure after 10-15 minutes.
- Signs of a fractured jaw or other facial bones: (e.g., inability to close mouth, severe pain, facial asymmetry).
- Concomitant injuries: Such as severe cuts to the lips, tongue, or cheeks.
- Signs of infection post-replantation: Persistent or worsening pain, swelling (especially if accompanied by pus or fever), or a foul taste in the mouth.
Routine Care vs. Emergency:
- Emergency: A knocked out permanent tooth always falls into the "emergency" category. Do not wait for a scheduled appointment. Contact your dentist's emergency line or head to an emergency dental clinic or hospital emergency room if your dentist is unavailable.
- Scheduled Appointment: If the tooth has already been replanted and splinted, or if it was a primary tooth and initial care was provided, subsequent root canal treatment and follow-up monitoring will be scheduled appointments. However, any new symptoms or complications (e.g., increased pain, swelling, splint loosening) require prompt, unscheduled attention.
Always err on the side of caution when it comes to dental trauma. Swift and appropriate action can preserve your natural smile and prevent more complex and costly problems down the line.
Frequently Asked Questions
Medically Reviewed Content
This article was written by our dental health editorial team and reviewed for medical accuracy. Our content follows strict editorial guidelines for reliability and trustworthiness.
Medical Disclaimer
This article is for informational purposes only and does not constitute medical advice. Always consult with a qualified dental professional for diagnosis and treatment. Do not delay seeking professional advice because of something you read on this website.
Related Articles

How to Relieve Gum Swelling
When your gums are swollen, it can be an alarming and uncomfortable experience, often signaling an underlying issue that requires attention. Statistics from the Centers for Disease Control and Prevention (CDC) reveal that **nearly half of adults aged 30 or older in the United States have some form o
February 23, 2026

Teeth Swelling: Complete Guide
When you experience teeth swelling, it's more than just a minor discomfort; it's a clear signal from your body that something is amiss within your oral cavity, often indicating an underlying infection or inflammation that requires prompt attention. A recent survey revealed that **over 25% of adu
February 23, 2026

Submandibular Salivary Gland Swelling: Complete Guide
When you notice a peculiar lump or uncomfortable fullness beneath your jaw, it can be an alarming experience. This sensation, often accompanied by pain and difficulty swallowing, could indicate submandibular salivary gland swelling. Affecting an estimated 1 in 10,000 adults annually, conditi
February 23, 2026

What Helps With Gum Swelling
Gum swelling, medically known as gingival swelling or gingivitis, is a common yet often underestimated dental issue affecting millions of Americans. Have you ever woken up with sore, puffy gums that bleed easily when you brush? You're not alone. Research indicates that nearly **half of all a
February 23, 2026